Staph & Strep
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
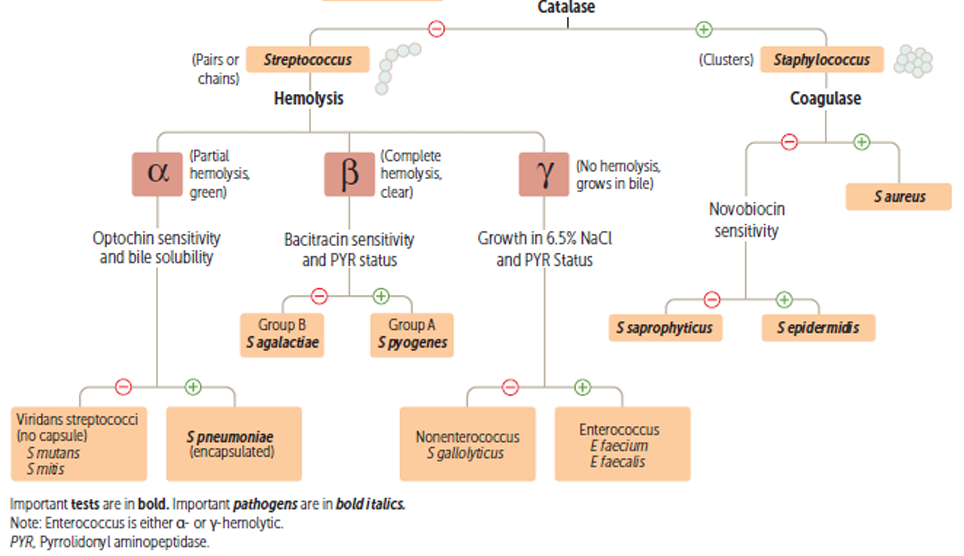
Claffification of G+ Cocci
Staphylococci habitat
Skin, mucosa of anterior nares, vagina, and inanimate objects
S. aureus habitat
Nares, ears, groin.
10-30% of healthy people carry staph
5-10% vaginal carriage (increases during menses
S. aureus Virulence factors
MSCRAMMs - Binds many ECM proteins
Clumping factors A&B (Bound Coagulase) - Bind fibrinogen and platelets → Aggregates *Important for UB
Fibronectin-binding proteins A&B (Fnbp A&B) - Helps in invasion (Attachment to exposed fibronectin in open wounds)
Collagen-binding adhesins (CNAs) → Invasion of CT, bones, joints
Teichoic acid - Promotes colonizattion
S layer - Antiphagocytic
Protein A
Coagulase
Staphylokinase
Hyaluronidase
Lipase
Nuclease
Catalse
Beta-lactamase
*Note: Staphylokinase coagulase are synthesized at different times (Invasion vs spread)
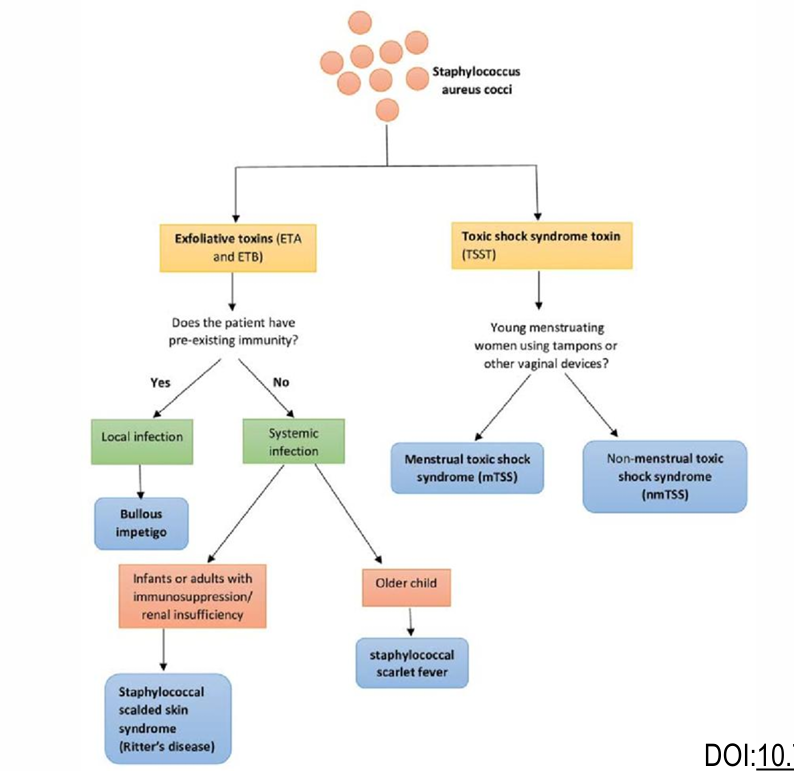
S. aureus toxins
Cytolytic axotoxins:
Alpha hemolysin → Membrane-damaging toxin → Septic shock
Beta hemolysin → Sphingomyelinase
Panton-Valentine Leucocidin (PVL) → Lyses leukocytes → Maaive inflammation (Important in MRSA)
Superantigen exotoxins:
Enterotoxins: A,B,C(1/2/3),D,E,H
TSST
Exfoliatin (SSSS)
S. aureus diseases (Everything)
Skin: Folliculitis, furuncle, carbuncle, abscess, wound infection, impetigo, paronychia, cellulitis
Soft tissue: Osteomyelitis, arthritis
RT: Bronchopneumonia, tonsillitis, pharyngitis, sinusitis, lung abscess, pneumonia
CNS: Brain abscess, meningitis, tntracranial thrombophlebitis
Endovascular: Bacteremia, septicemia, endocarditis
UT: Implants and catheters
Nosocomial infections (MRSA)
Staphylococcal food poisoning: Fast-acting, heat-resistant, preformed toxins. Mainly type A enterotoxin no more than 1 day - Sliced meat, puddings, pastries, milk, cheese
STTS: Mainly caused by TSST-1 - Vaginal tampons→ Fever, vomitting, diarrhea, rash, desquamation, shock, end-organ failure, and high AST/ALT/bilirubin
SSSS: Outer layer of the epidermis is separated from underlying tissue,
Newborns: Ritters’ Disease
Older patients: Toxic epidermal necrolysis
Milder forms: Pamphigus neonatorum/ Bullous impetigo
Kawasaki: Inflammatory disease with potential heart
S. aureus biochemistry and selective characteristics
OX -
CAT +
Coagulase + (free and bound)
Mannitol +
PYR A -
Phosphatase +
Tnase + (thormostable DNase)
Seletive stuff:
Can grow in 10-15% NaCl
Penicillin-resistant
S. aureus treatment
Drain abscess
If deep infection, need:
Advanced penicillins
Cephalosporins
Erythromycin
Clindamycin
If endocarditis:
NODs + an AG
Life-threatening → Vancomycin
Choose based on sensitivity testing
Describe S. aureus resistance
First, penicillinases, then chromosomally encoded modified PBP, and also plasmid-borne resistance to erythromycin, tetracyclines, AGs, and almost all antibiotics
Describe CAMRSA. Reservoirs/ resistance mechanism/ virulence/ treatment
Reservoir: Healthy people and people who’ve had medical procedures, specifically: damaged skin, groin, oropharynx.
Resistance: mecA gene product: PBP2a
Virulence: PVL
Treatment: Vancomycin and teicoplanin - GLYCOPEPTIDES
Coagulase-negative Staph infection risk factors
Implants
Coagulase-negative Staph lab characteristics
Similar to S. aureus but white colonies and coagulase-negative
Clinical picture of Coagulase-negative Staph
Infect prosthetic valves → Endocarditis
Contaminate blood cultures (Mainly S. epidermidis)
UTIs in pregnant women (S. Saprophyticus)
Coagulase-negative Staph treatment
Beta-lactams/ Vancomycin
S. saprophyticus treatment
TMP-SMX/ Quinolones
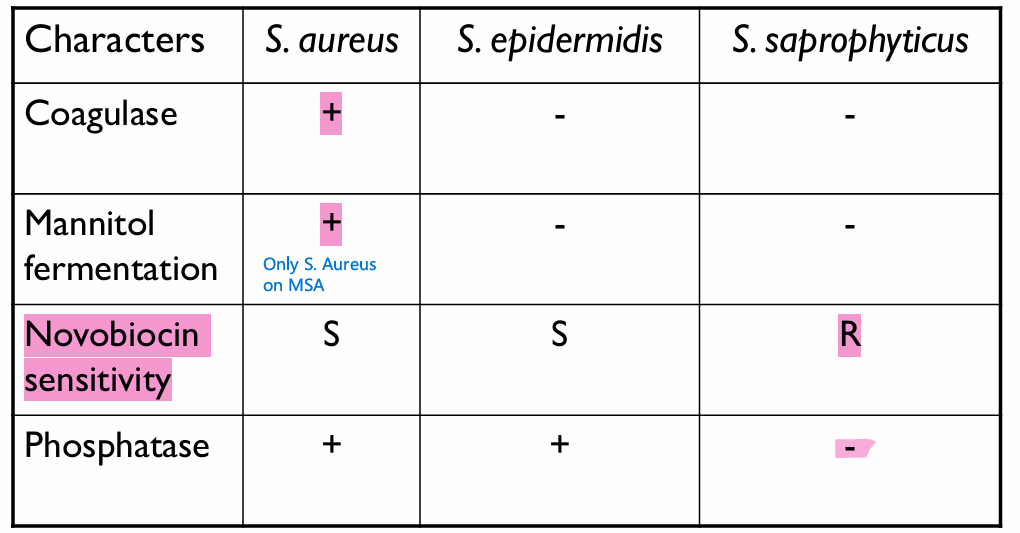
Biochem differences among Staphylococci (Coagulase / Mannitol / Phosphatase / Novobiocin sensitivity)
Treatment of Coagulase-negative staph
Bacitracin
Chlorohexidine (locally)
Vancomycin
Sreptococcus geus characteristics
G+, Non-motile, FA, fermentative metabolism of carbohydrates
Penicillin-sensitive
Commensals, parasites, saprophytes
GAS habitat
Pharynx (mainly) and skin
→ Obligate human pathogen, but it can be carried asymptomatically
S. pyogenes virulence factors and exotoxins
Virulence factors:
Streptolysin O - SLO (O2-labile) → Damages cardiac cells (Ca2+ influx)
Note: Highly antigenic: Anti-SLO (ASLO) titer is a marker for infection recency
Streptolysin S - SLS → Oxygen stable, non-antigenic
Hyaluronic acid capsule - Immune mimicry
M-like proteins: Bind IgM and IgG - STRUCTURALLY SIMILAR TO MYOSIN
LM-Protein: Adhesins and antiphagocytics
F-Protein: Adherence
Phage lysogeny → Steptococcal Pyrogenic Exotoxin
Exotoxins:
Streptococcal Pyrogenic Exotoxin (SPEs) → SCARLET FEVER
Exoenzymes: Streptokinase/ Streptodornase (DNase) → ASDOR/ Hyaluronidase
Sterptococcus pyogenes diseases
Pharyngitis & tonsilitis
If lysogenized → Scarlet fever: Sand-paper-like upper body rash + Strawberry tongue
Otitis media
Sinusitis
Pneumonia
How can you differentiate Streptococcal pharygitis from viral
In strep infection, symptoms will also include: headache, nausea, vomiting, and abdominal pain. In viral, it’s common-cold like only.
Strep: Tonsillar eudates. None in viral
Strep: Painful cervical adenopathy, in viral, adenopathy can occur but it’s painless
Streptococcus pyogenes Cutenous and soft tissue infections
Impetigo (Contagious pyoderma - honey-crusted lesions)
Erysipelas (Upper dermis + superficial lymphatics)
Cellulitis (Deep dermis and subcutaneous fat)
Necrotizing fasciitis (Subcutaneous fat + fascia → Destruction of muscle and fat)
(May or not progress from erysipelas to cellulitis to NF)
Wound infections
Lymphangitis (Inflammation of
Describe the clinical appearance of Erysipelas
You will find Erythema + Bullae (It’s only seen in Strep, not staph)
Streptococcal pyogenes systemic disease
Streptococcal toxic shock-like syndrome
Bacteremia
Sequelae of Strep infections
Acute rheumatic fever (ARF) - T2HS, Follows pharyngitis
Rheumatic heart disese (RHD) - T2HS, Follows pharyngitis
Acute glomerulonephritis (AG) - T3HS, usually follows pyoderma
S. pyogenes diagnosis
Rapid antigen test (95% Specificity, but only 70-90% sensitive)
Culture: Done in 5-10% CO2, on BA + NA → Produce B-hemolytic colonies, HOWEVER, some strains are ALPHA-HEMOLYTIC
*Note, their capsules make the colony appearances look mucoid
ASLO/ASDOR titer: Helps us to diagnose Strep complications
S. pyogenes biochemistry
Ox -
Cat -
Bacitracin S
GBS habitat
Low GIT (normal flora)
Female genital tract (Newborns at ris if females have it)
GBS pathognicity
Neonatal disease and obstetrics complications
Neonatal meningitis
Puerperal sepsis
Pneumonia
Systemic, cutenous, and urinary infections
GBS specimen and culture
Specimen: CNS, blood, vagina/rectal smears, urine
Culture: 5-10% CO2 on BA + Colistin (inhibit G- enterics)+ NA (inhibit G+ cocci)
→ Should get Beta-hemolytic colonies, but some strains are gamma-hemolytic
GBS screening
Screen pregnant women at 35-37 weeks of gestation with vaginal and rectal swabs, if + → Give prophylaxis
GBS biochemistry
Ox -
Cat -
Esculin -
Hippurate +
Bacitracin R
CAMP test +
What’s S. pneumoniae among strep, and what is its habitat
It’s an alpha-hemolytic streptococcus
Inhabitant of URT of 40-70% of people
S. pneumoniae types distribution, and. general epidemiology
Pneumococci types 1-8 → adults
Pneumococci types 6 + anything above 8 = Children
They are responsible for 60% of all bacterial pneumonias
Risk factors for S. pneumoniae pneumonia
Viral and other infections OF URT
Alcohol or drug intoxication
Circulatory system pathologies
Malnutrition
Sickle cell
Hyposplenia and asplenia (Encapsulated pathogens)
Nephrosis
Complement deficency
S. pneumoniae virulence factors
Capsule
Choline-binding protein A → Adhesin
Neuraminidases → Help invade nasopharynx
Proteases → Degrades IgG, IgM, IgA
Pneumolysin O → Cytolytic to eukaryotic cells
H2O2 → Damage host cells and competing microbiota (NHS (S here is S. aureus)
Pneumococal diseases (10)
Acute lobar pneumonia
Pneumococcal pneumonia → Rusty sputum
Bacteremia
Bacterial meningitis in children
AOM
Sinusitis
Peicarditis
Conjuctivitis
Arthritis
Peritonitis
S. pneumoniae morphological characteristics
G + diplococci
Capsulated
S. pneumoniae culture
Sputum is gold standard:
5-10% CO2
Choline
BA + NA → Alpha hemolytic colonies
Enrich with defibrinated blood
S. pneumoniae
Ox -
Cat -
Optichin S
Bile soluble
S. pneumoniae serology
Detection of pneumococcal antibodies and capsular polysaccharide Ag in urine or CSF
PCR
Note: Non-beta hemolytic strep are called: Non-lancefield Group streptococci
S. pneumoniae treatment
Based on sensitivity testing
Penicillin, 3rd gen cephalosporins, imipenem, vancomycin
S. pneumoniae vaccine
Conjugate or polysaccharide pneumococcal vaccines
Describe the Viridans
They’re normal oral/nasopharyngeal flora
Include: S .mutant/sanguis/salivarius/mitis
Common post-tooth axtraction bacteremia → They implant on damaged or prosthetic heart valves
*S. sanguis specifically is the most common cause of subacute bacterial endocaditis
Prior to tooth extraction procedure, must always give antibiotics 2 days prior
Lab diagnosis of viridans
Hemoculture
Growth on BA + NA + Colistin in 5-10% CO2
→ Alpha hemolytic, but can be gamma
Viridans biochem
Optichin R
PYRA -
Group D enterococcus and their infections
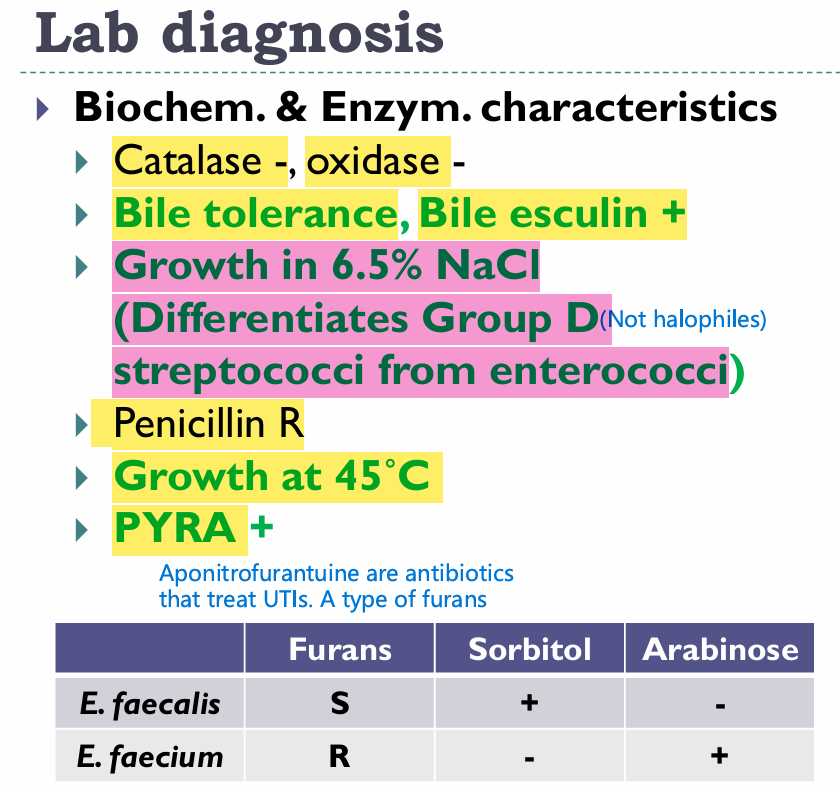
E. faecalis and E. faecium
Nosocomial infections (VREs):
UTIs/Wound infections/ bacteremia/ endocarditis/ Intrabdominal abscesses
Enterococci culture
5-10% CO2
BA + NA + Colistin → Alpha/beta/gamma (wow)
OE
BEA - Bile esculin agar (Enterococci degrade esculin in the presence of iron and give off a black coloration)
Enterococci labs
Non-enterococcus Group D strep
S. gallolyticus → Alpha-hemolytic
NOTE: Patients with S. gallolyticus endocarditis have a higher incidence of colon cancer
Group G streptococcus
S. anginosus / S. constellatus/ S. intermidius
Can cause deep pyogenic abscesses
Culture on: BA + NA + Colistin → alpha/beta/gamma
→ Caramel odor due to diacetyl metabolite