Reproductive A&P and Disorders
1/73
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
74 Terms
What are the hormones in female reproductive systems?
Significant hormones and hormonal changes
Estrogens
Progesterone
Androgens
Follicle-stimulating hormone (FSH) and luteinizing hormone (LH)
What is the health history to do for reproductive system?
Menstrual history and history of pregnancies
History of exposure to medications
Pain with menses or intercourse
Vaginal discharge, odor, or itching
Urinary and bowel function
Sexual history, including sexual or physical abuse
History of STDs, surgeries, or procedures
Chronic illness or disabilities that affect health and self- care
Family and genetic history
What is the sexual history done?
Assessment includes subjective and objective data
Purpose is to obtain information to picture a woman’s sexuality and sexual practices to promote sexual health
May move from less sensitive areas of general health history or assessment to more sensitive areas
Ask for permission to discuss these issues
Do not assume sexual preferences
Asking the patient to label herself as married, single, and so on may be interpreted as inappropriate; asking about current meaningful relationships may be less offensive
PLISST model
What are some considerations to keep in mind for reproductive health?
Female genital mutilation or cutting
Intimate partner violence: physical, sexual, stalking, and psychological aggression
Incest and childhood sexual abuse
Health issues in women with disability
Lesbian, gay, bisexual, transgender or queer (LGBTQ)
Gerontologic considerations
What is the physical assessment for reproductive system; pelvic examinations?
Annual breast and pelvic examinations: all women 21 years of age or older and for those who are sexually active, regardless of age
Alleviate feelings of anxiety with explanations and education
Patient is asked to empty her bladder and to provide a urine specimen if urine tests are part of the total assessment
Positioning
Inspection
Speculum examination
Inspection of cervix
Obtaining pap smears and other samples
Inspecting vagina
Bimanual palpation
Cervical, uterine, adnexal, vaginal, and rectal palpation
Breast assessment?
Anatomic and physiologic overview
Health history
Physical assessment: female breast and male breast
Inspection, palpation, lymph nodes
Adolescent, obese
Gynecomastia
Refer to Chart 52-1
Diagnostic evaluation for breast issues
Breast self-examination (BSE; “breast self- awareness”)
5 to 7 days after menses
Mammography
Annually after the age of 45 years
Digital and 3D
Contrast
Ultrasonography
MRI
Things to keep in mind with male reproductive system?
Includes conditions that affect both reproduction and sexuality and urinary elimination
Patient may experience anxiety and embarrassment
Be sensitive to cultural and emotional issues related to sexuality and the genitals to accomplish effective assessment and communication
Provide for privacy and education
What is the assessment for male reproductive system?
Urinary function and symptoms
Sexual function and manifestations of sexual dysfunction
Symptoms related to urinary obstruction
Increased urinary frequency
Decreased force of stream
“Double” or “triple” voiding
Nocturia, dysuria, hematuria, hematospermia
Presence of conditions that may affect sexual function (diabetes, cardiac disease, multiple sclerosis)
PLISSIT model & BETTER model
PLISSIT model
Permission
Limited Information
Specific Suggestions
Intensive Therapy
BETTER model includes cancer patients
Bringing up the topic, explaining, telling, timing, educate about treatment-related sexual side effects, recording
Physical assessment for male reproductive system
Digital rectal exam
Recommended annually for men >50 years old
Recommended >45 years of age for high risk; African American and men with family history
Testicular exam
Instruct on testicular self-examination (TSE)
What are some diagnostic tests to evaluate the male reproductive system?
Prostate-specific antigen (PSA)
Ultrasonography
Prostate fluid or tissue analysis
Tests of male sexual function
What are some types of menstrual disorders?
Premenstrual syndrome (PMS)
Dysmenorrhea
Amenorrhea
Excessive, irregular, or in-between/unrelated to cycles bleeding
Premenstrual Syndrome (what is it, S&S, tx)
A cluster of physical, emotional, and behavioral symptoms that are usally related to the luteal phase (2nd half) of the menstrual cycle
Very common affecting many women at some time in their lives
S&S: headache, fatigue, low back pain, painful/tender, breasts, abdominal fullness; general irritability mood swings, fear of losing control, depression, anxiety, withdrawal, anger, binge eating, and crying spells
Premenstrual dysphoric disorder (PMDD) is a severe form of PMS w/ significant severity of symptoms
Can be managed
Pharm tx: SSRIs, naproxen, antianxiety, Ca+, birth control
Dysmenorrhea (what is it, S&S, tx)
Painful menstruation with no identifiable pelvic pathology
S&S: crampy lower abdominal pain that begins before or shortly after menstrual flow and continues 48-72 hrs; n/d, dizziness, backache
Rule out endometriosis, PID, uterine fibroids
Pharm tx: NSAIDs, local heat
Amenorrhea
Absence of menstral flow; is a symptom of a variety of disorders and dysfuctions
Factors: obesity, eating disorders (anorexia and bulimia); intense exercise
Contraception
Abstinence
Long-acting reversible contraceptive (LARC)
Intrauterine device (IUD), implants
Sterilization
Hormonal contraception: oral, transdermal, vaginal, injectable
Mechanical barriers
Diaphragm, cervical cap, female condom, spermicides, male condom
Coitus interruptus or withdrawal
Fertility awareness-based methods
Emergency Contraception
Emergency contraceptive pills
Postcoital intrauterine device (IUD) insertion
Patients who use emergency contraception may be anxious, embarrassed, and lacking information about birth control. The nurse must be supportive and nonjudgmental and provide facts and appropriate patient education.
Purpose, eucation (benefits/cons)
Abortion
Interruption of pregnancy or expulsion of the product of conception before the fetus is viable
Types
Spontaneous abortion
Habitual abortion
Induced abortion
Medical and nursing management
Induced abortion
Preabortion counseling
Pelvic examination and laboratory tests
Use of RhoGAM for Rh-negative patient
Types of induced abortions
Patient education, including instruction for follow- up care and information on contraception
Psychological support
Infertility (definition, primary v secondary, factors)
A couple’s inibility to achieve a pregnancy after 1 year of unprotected intercourse
Primary infertility referf to couple that has never had a child
Secondary infertility means at least one conception has occured but the couple cannot achieve a pregnancy
Pathophysiology:
Ovarian and ovulation factors
Tubal and uterine factors
Male factors
How can infertility be managed?
Pharmacologic therapy
Potential for multiple pregnancies
Ovarian hyperstimulation syndrome (OHSS)
Artificial insemination
Assisted reproductive technologies
In vitro fertilization (IVF)
Gamete intrafallopian transfer (GIFT
Other technologies
Make sure to give psycosocial suport and stay on hormones
Ectopic Pregnancy (clinical manifestations)
A leading cause of pregnancy-related death in the first trimester
Causes include salpingitis (inflammation of the fallopian tubes), peritubal adhesions, structural abnormalities of the fallopian tube, previous ectopic pregnancy, previous tubal surgery, tumors, IUD, progestin (only contraception), and pelvic inflammatory disease (PID)
Clinical manifestations:
Delay in menses, slight bleeding, vague soreness or sharp colicky pain, GI symptoms, dizziness, lightheadedness
With tube rupture: agonizing pain, dizziness, faintness, nausea or vomiting, progression to shock
Later: generalized abdominal pain that radiates to shoulder
Assessment for patient with ectopic pregnancy?
Menstrual pattern
Pain: description and location; sharp, colicky; radiating to shoulder and neck
Vital signs, level of consciousness, nature and amount of bleeding
Coping
Potential complications
Hemorrhage
Hemorrhagic shock
Nursing Interventions for patient with ectopic pregnancy
Relieving pain
Preanesthetic medications
Postoperative analgesics administered liberally
Early ambulation
Coughing
Deep breathing
Supporting the grieving process
Listen to and support patient
Encourage patient’s partner to be a part of this process
Monitoring and managing potential complications
Continuous monitoring (VS, LOC, amount of bleeding, I&O)
Bed rest
Hct, Hgb, and blood gases should be monitored
Blood transfusions when appropriate
Self-care and continuing care
Effect of future pregnancies
Preconception counseling recommended
What is perimenopause?
The period before menopause that begins on average 4 years before the last menstrual period
Characterized by marked hormonal fluctuations and irregular menstrual cycles
Women often have varied beliefs about aging, and these must be considered when caring for and educating perimenopausal patients
What is menopause?
Permanent physiologic cessation of menses associated with declining ovarian function
Changes in menstruation
Clinical manifestations
Psychological considerations
Medical management: HRT; risks and benefits
Alternative therapy for hot flashes
What is a vulvovaginal infections?
Common problem
Vagina is normally protected by acid pH maintained, in part, by Lactobacillus acidophilus
Vaginal epithelium is responsive to estrogen, which induces glycogen formation, which breaks down into lactic acid; therefore, decreased estrogen decreases acid production
With perimenopause and menopause, decreased estrogen is related to vaginal and labial atrophy, and tissue is more susceptible to infection
Types:
Vaginitis
Candidiasis
Bacterial vaginosis: Gardnerella vaginalis
Trichomonas vaginalis
What are the risk for vulvovaginal infections?
Premenarche, perimenopause, menopause, low estrogen levels
Pregnancy or oral contraceptives
Poor hygiene
Tight garments and synthetic clothing
Frequent douching
Antibiotics
Allergies
Diabetes
Intercourse with infected partner, oral genital contact, HIV
What is the assessment of patient with a vulvovaginal infections?
Examine as soon as possible after onset of symptoms
Instruct patient not to douche before assessment
History includes
Physical and chemical factors
Psychogenic factors
Medical conditions
Use of medications
Sexual activity and history
What are the nursing interventions for patient with a vulvovaginal infection?
Sitz baths may help relieve discomfort
Explanation of the cause of symptoms and methods to help prevent infections may help reduce anxiety
Douching is usually avoided; however, therapeutic douching may be prescribed to reduce odors and remove excessive drainage
Patient education includes handwashing, proper hygiene, preventive strategies, measures to reduce risk, information regarding medications, and information regarding self-examination
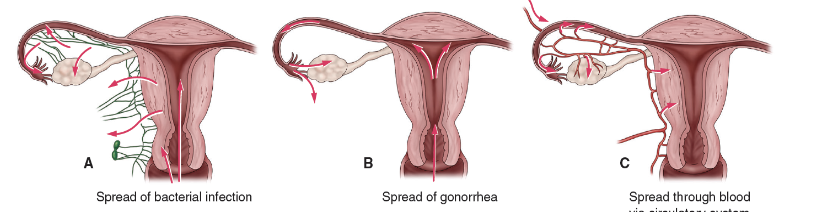
Pelvic Inflammatory Disease (PID)
Inflammatory condition of the pelvic cavity that may begin with cervicitis and involve the uterus (endometritis), fallopian tubes (salpingitis), ovaries (oophoritis), pelvic peritoneum, or pelvic vascular system
Gonorrheal and chlamydial organisms are common causes, but most cases are associated with more than one organism
Short- and long-term consequences can occur
What are the nursing assessments for PID?
Vaginal discharge
Dyspareunia
Lower abdominal pelvic pain, and tenderness that occurs after menses that may increase with voiding or with defecation
Other symptoms
Fever, general malaise, anorexia, nausea, headache, and possibly vomiting
Pelvic examination—intense tenderness may be noted on palpation of the uterus or movement of the cervix (cervical motion tenderness)
What is the treatment PID?
Broad-spectrum antibiotics; Ceftriaxone, doxycycline, methonizone
Treat sexual partner to prevent reinfection
Analgesics for pain relief
Adequate rest and nutrition
Patient education: how to prevent reinfection
HIV and AIDS
25% living with HIV are women
Counseled about safer sex and informed about the dangers of unprotected sex
Because there is a riskbof perinatal transmission, decisions to conceive or to use contraception must be based on education, accurate information, and care
Pregnant women are advised to have an HIV test. The use of antiretroviral agents by preganant
What are some structual disorders- of female anatomy?
Fistulas of the vagina
Pelvic organ prolapse
Cystocele
Rectocele
Enterocele
Treatment
Surgical
Medical: pessaries, pelvic floor muscle training
Fistua (what is goal?)
An abnormal opening between two internal hollow organs or between an internal hollow organ and the exterior of the body.
Congenital but most common in developing countries due to obstructed labor complications
Goal: eliminate the fistula and treat infection/ excoriation; surgery
Pelvic Organ Prolapse (risk factor & management)
Weakening of the vaginal walls allowing the pelvic organs to descend and protrude into the vaginal canal
Risk factors: age, parity-amount of times women have given birth to child (24 weeks & older) (particularly vaginal delivery), menopause, previous pelvic surgery, and possibly a genetic predisposition
Management: Kegel exercises, pelvic floor PT
Endometriosis
A benign lesion or lesions that contain endometrial tissue (similar to lining of uterus) found in the pelvic cavity outside the uterus
A chronic disease affecting between 7% and 10% of women of reproductive age, occurring more frequently in women who have never had children
Major cause of chronic pelvic pain and infertility
Pharmacologic therapy: analgesic, prostaglandin inhibitors, hormone therapy, oral contraception
What are some malignant disorders of the female reproductive tract?
Cervical, uterine (endometrium), vaginal, vulvar, fallopian tubes, and ovarian cancers
Early disease may not have symptoms → Lower back pain can be a early indicator
Signs and symptoms: depend on location; vaginal discharge, pain, bleeding, and systemic symptoms (weight loss and anemia)
Prevention, screening, and early detection are vital
Tx: Surgery, chemotherapy, radiation, or a combination of these
Treatment may be curative or palliative
Care of the surgical patient is similar to care of patients with other abdominal surgeries
What are some genital viral infections?
Human papillomavirus (HPV)
The most common sexually transmitted disease amongsexually active young people
Vaccine -> usally given around age 11-13
Treatment of genital warts
Associated with cervical dysplasia and cervical cancer; need annual Pap smears
Herpes type 2 infection (herpes genitalis)
A recurrent lifelong viral infection
An STD that also may be transmitted by contact and that may be transmitted when the carrier is symptomatic
Causes painful itching and burning herpetic lesions
What is hysterectomy?
Surgical removal of the uterus to treat cancer, dysfunctional uterine bleeding, endometriosis, nonmalignant growths, persistent pain, pelvic relaxation and prolapse, and previous injury to the uterus
Total hysterectomy
Radical hysterectomy
Types of approaches
Laparoscopic
Vaginal
Abdominal
Asessment + collaborative problems and potential complications of patient undergoing a hysterectomy
Assessment
History
Physical & pelvic exam
Psychosocial & emotonal response
Patient knowledge → educate on self care post op
Collaborative Problems & Potential Complications
Hemorrhage
DVT
Bladder dysfunction
Infection
Nursing Interventions for the patient undergoing a hysterectomy
Relieving anxiety
Allow patient to express feelings
Explain physical preparations and procedures
Improving body image
Listen and address concerns
Provide appropriate reassurance
Address sexual issues
Approach and evaluate each patient individually
Relieving pain
Assess intensity of pain and administer analgesia as prescribed
Manage abdominal distension
Monitoring for complications
Hemorrhage
Venous thromboembolism
Bladder dysfunction
Educate about self-care and continuing care
Surgical incision care, maintaining bowel and urinary function, resuming activities slowly, showers instead of baths, activities to avoid, symptoms to report, follow-up
Radiation Therapy (in female reproductive tract)
Used in the treatment of cervical, uterine, and less frequently in ovarian cancers
Methods
External radiation therapy
Intraoperative radiation therapy
Internal (intracavitary irradiation)
Care of the patient undergoing radiation therapy
What are some benign conditions of the breast?
Breast pain (mastalgia)
Cysts, fibrocystic breast changes
Fibroadenomas
Benign proliferative breast disease
Atypical hyperplasia
Lobular carcinoma in situ (LCIS)
Other: cystosarcoma phillodes, fat necrosis, intraductal papilloma, superficial thrombophlebitis
What are some malignant conditions of the breast?
Ductal carcinoma in situ (DCIS)
Proliferation of malignant cells inside the milk ducts without invasion into surrounding tissue
Invasive cancer
Infiltrating ductal carcinoma: most common
Infiltrating lobular carcinoma
Medullary carcinoma: women <50 yrs old
Mucinous carcinoma: postmenopausal
Tubular ductal carcinoma
Inflammatory carcinoma
Breast Cancer
Breast cancer is a major health problem in the United States. At present, there is no cure
Over an entire lifetime, a woman’s risk of developing breast cancer is about 12% or one in eight
Approximately 268,600 new cases of invasive breast cancer are diagnosed in women each year
Risk of developing breast cancer increases with age
Female breast cancer incidence rates vary substantially by race and ethnicity
Non-Hispanic African American women have higher incidence of breast cancer than non-Hispanic Caucasian women before the age of 40 and are more likely to die from breast cancer at every age
Diagnosing Breast Cancer
Staging: TMN (tumor, nodes, metastasis)
Chest x-ray, CT, MRI, PET, bone scan and blood work
Prognosis
Tumor size
Spread to the lymph nodes?
Certain genes (ERBB2)
Educate on how to perform breast exam
Surgical management of breast cancer
Modified radical mastectomy
Total mastectomy
Breast conservation treatment
Sentinel node biopsy and axillary lymph node dissection
Potential complications of surgery
Lymphedema
Hematoma or seroma formation
Infection
Changes in sexual function
Preoperative Nursing Interventions for the Patient Undergoing Surgery for Breast Cancer
Review and reinforce information on treatment options
Prepare patient regarding what to expect before, during, and after surgery
Inform patient regarding surgical drain, arm and shoulder mobility, and range-of-motion exercises
Maintain open communications
Provide patient with realistic expectations
Support coping
Involve or provide information for supportive services and resources
Support patient decisions
Postoperative Nursing Interventions for the Patient Undergoing Surgery for Breast Cancer
Relieve pain and discomfort
Inform patient regarding common postoperative sensations
Promote positive body image
Maintain privacy
Temporary breast form or soft padding for bra
Provide information about home plan of care
Support coping and adjustment; counseling and referral
Monitor for potential complications
Lymphedema, hematoma or seroma, infection
Don’t use bp cuff on same side bc can lead to lyphedema
How to educate patients on self care?
Surgical site management and care of drain (drains are usually removed when the output is less than 30 mL in two consecutive 24-hour periods, approximately 7 to 10 days) → educate
Shower on second postoperative day and wash the incision or drain site with soap and water. If immediate reconstruction has been performed, showering may be contraindicated until the drain is removed
Patients are taught arm exercises on the affected side to perform three times a day for 20 minutes at a time until full range of motion is restored (generally 4 to 6 weeks)
Heavy lifting (more than 5 to 10 pounds) is avoided for about 4 to 6 weeks
How to evaluate patient undergoing surgery for breast cancer?
Exhibits knowledge about diagnosis and surgical treatment options
Verbalizes willingness to deal with anxiety and fears
Demonstrates ability to cope with diagnosis and treatment
Reports that pain has decreased and identifies postoperative sensations
Exhibits clean, dry, and intact surgical incisions
Verbalizes feelings regarding change in body image
Participates actively in self-care measures
What are the nonsurgical management of breast cancer?
Radiation therapy—external beam, brachytherapy
Chemotherapy
Hormonal therapy
Estrogen and progesterone receptor assay
Selective estrogen receptor modulators (SERMs)— tamoxifen
Aromatase inhibitors—anastrazole, letrozole, exemestane
Targeted therapy
Reconstructive procedures after mastectomy
Tissue expander followed by permanent implant
Tissue transfer procedures
Transverse rectus abdominal myocutaneous (TRAM) flap
Nipple–areola reconstruction
Prosthetics
Reconstructive breast surgery: mammoplasty
Reduction, augmentation
Mastopexy
What are some special considerations of breast cancer?
Implications of genetic testing: rapid advancement
Pregnancy and breast cancer
Breast cancer: quality of life and survivorship
Gerontologic considerations
Breast health of women with disabilities
Diseases of the male breast
Gynecomastia
Male breast cancer
Male breast cancer?
The lifetime risk of breast cancer in men is about 1 in 1000
Early detection is uncommon in male breast cancer because of the rare nature of the disease
Treatment: total mastectomy
Stigma with such diagnosis, which may cause poor adherence to treatment plans
Disorders of male sexual function
Erectile dysfunction
Psychogenic causes: anxiety, fatigue, depression, absence of desire
Organic causes: vascular, endocrine, hematologic, and neurologic disorders; trauma; alcohol; medications; and drug abuse
Medications associated with erectile dysfunction
Ejaculation problems
Premature ejaculation
Retrograde ejaculation
What is the medical management of erectile dysfunction?
Pharmacologic therapy
Oral medications—sildenafil (Viagra)
Side effects: headache, flushing, dyspepsia, diarrhea, nasal congestion, lightheadedness
Caution with retinopathy
Contraindicated with nitrate use
Injected vasoactive agents
Complications include priapism (persistent abnormal erection)
Urethral gel
Penile implants and transplants
Negative pressure devices
What is prostatitis?
Prostatitis: inflammation caused by an infectious agent
Acute bacterial: sudden onset of fever, dysuria, perineal prostatic pain
Chronic bacterial: typically asymptomatic
Chronic prostatitis/chronic pelvic pain syndrome: genitourinary symptoms with no bacteria in urine
Asymptomatic inflammatory prostatitis: diagnosed incidentally, elevated PSA
Treatment includes appropriate anti-infective agents and measures to alleviate pain and spasm
Trimethoprim-sulfamethoxazole or a fluoroquinolone (e.g., ciprofloxacin)
Alpha-adrenergic blocker therapy (e.g., tamsulosin; flomax) maybe prescribed to promote bladder and prostate relaxation
relax smooth muscle by blocking -1 receptors, reducing blood pressure, and increasing urine flow
What is BPH?
Benign prostatic hyperplasia (BPH=enlarged prostate)
Affects half of men older than 40 years of age and 50% of men older than 60 years of age
Manifestations are those of urinary obstruction, urinary retention, and urinary tract infections
Develops over a period of time; changes in urinary tract slow and insidious
Symptoms depend on severity: dysuria, hesitancy, sensation of incomplete bladder emptying
How is BPH treated?
Medical treatment
Alpha-adrenergic blockers#
5-alpha-reductase inhibitors
Measures to reduce pain and spasms
Catheter for acute condition; unable to void
Surgical treatment
Minimal invasive therapy
Transurethral microwave thermotherapy
transurethral needle ablation by radiofrequency energy and insertion of a stent
Surgical resection
Transurethral resection of the prostate (TURP)
Prostate Cancer (Manifestations, treatment)
Second most common cancer and the second most common cause of cancer death in men
Risk factors include increasing age, familial predisposition, and African American race
Manifestations:
Early disease has few or no symptoms
Symptoms of urinary obstruction, blood in urine or semen, painful ejaculation
Symptoms of metastasis may be the first manifestations
Treatment may include therapeutic vaccine, prostatectomy, radiation therapy, hormonal therapy, or chemotherapy
What is surgical approaches to prostatectomy?
Transurethral resection of the prostate (TURP)
Suprapubic prostatectomy
Perineal prostatectomy
Retropubic prostatectomy
Transuretheral incision of the prostate
Laparoscopic radical prostatectomy
Robotic-assisted laparopscopic radical prostatectomy
Pelvic lymph node dissection
What are the disorders affecting the testes and adjacent structures? * don’t focus on
Orchitis: an acute inflammation of one or both testes as a complication of systemic infection or as an extension of an associated epididymitis caused by bacterial, viral, spirochetal, or parasitic organisms.
Epididymitis: an infection of the epididymis, which usually spreads from an infected urethra, bladder, or prostate
Testicular torsion: a surgical emergency requiring immediate diagnosis to avoid loss of the testicle
Testicular cancer
Testicular cancer (manifestations)
Most common cancer in men ages 15 to 40 years
Highly treatable and curable
Risk factors: undescended testicles, positive family history, cancer of one testicle, Caucasian American race
Manifestations: painless lump or mass in the testes
Early diagnosis: monthly testicular self-exam (TSE) and annual testicular exam
Treatment: orchidectomy, retroperitoneal lymph node dissection (open or laparoscopic), radiation therapy, chemotherapy
What are some conditions affecting the penis? * don’t focus on
Phimosis: a condition in which the prepuce (foreskin) cannot be retracted over the glans in uncircumcised males
Penile cancer
Bowen disease
Priapism: a persistent penile erection that may or may not be related to sexual stimulation
Peyronie’s disease: an acquired, benign condition that involves the buildup of fibrous plaques in the sheath of the corpus cavernosum
Urethral stricture: a condition in which a section of the urethra is narrowed
Circumcision: surgical excision of the prepuce (foreskin) of the glans penis
What are some heath risks in in LGBTQ?
4.5% of U.S. population are gay
Stigmatization
Higher rate of: depression, anxiety, and suicide
Victimization: leads to emotional distress
HIV: higher rates in men who are gay or bisexual and transgender women
Define sex & gender?
Sex: physical or biologic characteristics that distinguish women and men
Chromosomes, genitals, hormones
Assigned at birth for most
Intersex: born with biologic traits not traditionally characterized as either male or female
Gender: a set of socially constructed characteristics of women and men
Voice, communication style, hairstyle, clothing, mannerisms
Taught norms and behaviors
Vary based on society; can be changed
What is inclusive language to use?
Sexual identity
Gender identity
Accurate information
Open to listening
Neutral language
Avoid assumptions
Confirm preferences
Health History & Physical Assessment
Family structure
Open-ended questions
Mirror language used by the patient
No specific assessments or diagnostic tests
Older LGBTQ patients
Gender Reassignment
Gender dysphoria
DSM criteria: Chart 54-2
Interdisciplinary health care team
Hormone therapy
Feminizing (male to female)
Masculinizing (female to male)
What is the surgical management/ criteria for gender reassignment surgery?
Criteria for gender reassignment surgery
Documented gender dysphoria
Age of consent
Need to get consent
12 months hormone therapy
12 months living in the gender role
How is patient undergoing gender reassignment surgery assessed?
Ensure the patient and their family feel welcomed and safe.
Use gender-neutral language and properly assess for gender identity and pronouns
Preoperative education and counseling
Risks and benefits, complications, postoperative outcomes, need for follow-up
Surgery-specific assessments
What are the nursing interventions done for patients undergoing gender reassignment surgery?
Ensuring human dignity
Reducing anxiety
Relieving pain
Preventing and monitoring for infection
Promoting hope
Monitoring and managing potential complications
Hemorrhage
Venous thromboembolism
Tissue necrosis
Patient education