Intro to Psych Exam 2
1/114
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
115 Terms
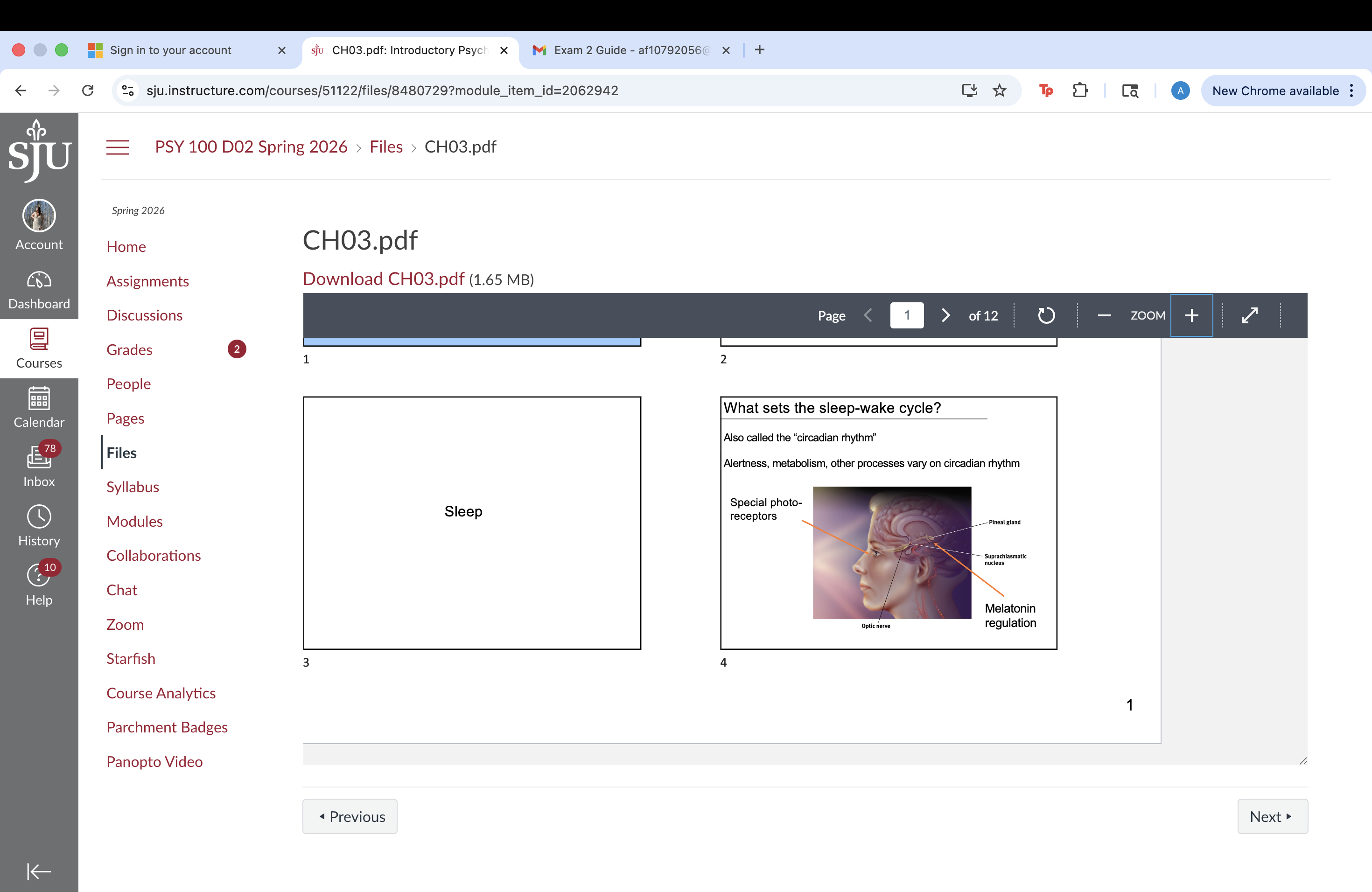
Sleep-wake Cycle
Also called the “circadian rhythm”
Alertness, metabolism, other processes vary on circadian rhythm
Sleep problems
Google trends suggest sleep problems are increasing
- Especially in the US for sleep apnea
- Everywhere for insomnia
Insomnia
Some people have a sleep cycle that is slightly too long
Why? Why are insomnia rates increasing?
Because of electric light / exposure to screens? - blue light on phone is keeping you awake
Life is more stressful?
Non-pharma treatment:
Use natural spectrum (sun) light to reset circadian rhythm each morning
Sleep Stages
If you do manage to fall asleep, your brain goes through a series of sleep “stages”
NREM1
Stage 1 sleep
Characterized by mild hallucinations
- Usually visual: geometric patterns, light flashes
- Lasts about 20 minutes
Sleep paralysis” can happen in stage NREM-1 sleep
NREM-2 sleep
Sleep Spindle
- Short duration, high frequency brain activity
- Function unclear: Believed to be related to “memory consolidation” because they are more frequent when sleeping after a lot of learning
K-Complex
- Large amplitude brain activity
- One function: processing auditory stimuli
NREM-3 sleep
10-15% of all sleep
- Characterized by large, slow delta waves
- Bedwetting (mostly in children) bc they have more of this
- Sleepwalking (mostly in children)
- “Deepest sleep”; very hard to wake up during NREM-3
Sleep paralysis
Sleep disturbed and halfway wakeup
Why do people sleepwalk?
Usually during NREM-3 sleep
Legs move, eyes open for navigation
Possible sleepwalking activities:
Common
eating
urinating
bathing
dressing
Less common
driving
homicide
REM sleep
REM(rapid eye movement) periods get longer as night progresses
Deeper sleep stages get shorter
AKA “Paradoxical Sleep”, Characterized by:
- Dreaming
- Heart rate rises
- Breathing becomes rapid and irregular
- Eyes move around (randomly, not to “watch” dreams)
- Visual / Auditory cortex is active
- 20-25% of all sleep
what is REM sleep for?
REM Deprivation during development linked to
Behavioral problems
Sleep problems later in life
Neuronal damage
REM may promote memory consolidation
May be important for recovery of some neurotransmitters
Definitely seems to be “non-optional”
REM rebound: Limit REM on night 1 → More REM on night 2
Long-term REM deprivation → Significant health issues
What are dreams for?
1) Freudian theory
“Unacceptable feelings” are expressed
Relieves internal conflicts
2) Activation-synthesis
Random activity in the brain triggers stored memories
Brain does its best to make memories into a coherent story
3) Information Processing
Byproduct of memory consolidation
Erasing of unnecessary neural associations
Rats in an MIT fMRI study dreamt about the mazes they ran
Brain processes during sleep - Can you learn while you sleep?
Yes:
- Sleepers trained on a (mild) shock - sound contingency
- Later had startle response to the sound while awake
No:
- Complex learning processes do not occur
Calculus
Foreign language
Memory consolidation
Consolidation of things you learn during the day.
Sleep Deprivation - short term vs long term
Short-term impact:
- Slowed reaction time
- Increased errors in visual judgments
Long-term impact:
- Immune system depression
- Shorter life span (esp. REM)
Why is sleep so important?
- Restoration & repair of brain tissue
- Making memories from daily experiences permanent
Hypnosis
May reflect little more than suggestibility
No evidence that hypnosis aids in recall
(Or at least “memories” are unreliable)
No evidence that people can be “controlled” by hypnosis
Demand characteristics: Subjects who are told that hypnosis reflects “gullibility” tend to stop responding
Hypnotherapy
No better than non-hypnosis positive suggestions
Drugs - Tolerance; Neuroadaption
Body is designed to maintain homeostasis
Recreational drugs act against homeostasis
e.g., increased heart rate, body temperature
After repeated exposure to a drug, tolerance may occur
When drug use happens, or is expected, brain and body attempt to counteract the drug’s effects
How does the brain know drug use is going to happen?
Time of day
Typical location where drugs are taken
Visual cues (presence of needles, etc.)
Withdrawal and Dependence
Withdrawal - symptoms associated with decrease or stoppage of drug use
Physical dependence, “physical” symptoms
(e.g., nausea)
Psychological dependence, “psychological” symptoms
(e.g., anxiety)
Dependence - taking the drug to avoid withdrawal
Addiction
Addiction is different from dependence (but they often co-occur)
Dependence is mostly associated with using the drug to avoid withdrawal symptoms
Addiction is mostly associated with a desire to get a reward from the drug (i.e., strong cravings for drug’s effects)
Addictive drugs compromise the brain’s reward system
Drug use becomes a more important goal than other, rewarding behaviors (eating, socializing, earning money)
Much information about drugs has a bias
Groups for reducing usage / harsher punishments
Groups for legalization
Psychoactive Drugs - Alcohol
Depressant (slows down CNS functions)
Slows reaction time / reduces coordination
Disrupts consolidation of memories
BUT, also reduces inhibition
Long term abuse:
Many physical problems
Psychological effects include Korsakoff syndrome:
Amnesia
Confabulation (confusing imaginations with reality)
Reduces Inhibition Experiment - alcohol
Effects interact with beliefs:
Group A: Subjects get alcohol
Group B: Subjects get realistic non-alcohol fake
1/2 in each group believe they had real alcohol
- all shown erotic movie clip -
1/2 who thought they had alcohol tended to report sexual fantasies and feeling no embarrassment
Independent of Group A / B status
Psychoactive Drugs - Cocaine
Can’t smoke powder cocaine
Blocks reuptake of dopamine, serotonin, norepinephrine
Blocking reuptake depletes neurotransmitter supplies (part of why people may feel lousy in days following use)
Addiction / tolerance with extended use
Long term use leads to brain damage
Hallucinations
Paranoia
Many physical health risks, e.g.:
Increased blood pressure
Heart attack
Stroke
Social Factors and Cocaine
Typically snorted or smoked (in “base” form, i.e. “freebasing”)
Occasionally injected (claims to deliver most intense effects)
Chewed/eaten (unrefined) by indigenous people of S. America
Method of use affects onset, duration of effects:
Crack:
Cheap form of chemically-altered cocaine
Easily smokeable
Cycle is faster (up and down)
The mechanism of cocaine
(a) Neurotransmitters carry a message from a sending neuron across a synapse to receptor sites on a receiving neuron.
(b) The sending neuron normally reabsorbs excess neurotransmitter molecules, a process called reputake.
© By binding the sites that normally reabsorb neurotransmitter molecules, cocaine blocks reuptake of dopamine, norepinephrine, and serotonin. The extra neurotransmitters molecules therefore remain in the synapse intensifying their normal mood-altering effects and producing a euphoric rush. When the cocaine level drops, the absence of those neurotransmitters produces a crash.
Psychoactive Drugs - LSD
Powerful hallucinogen
Experience interacts with person-specific characteristics
Personality
Current emotional state
Technically not “hallucinations”, because experience is caused by sensory input, but significantly altered
Synesthesia - hear sounds associated to colors
Believed to be non-toxic, non-addictive
Danger is mostly due to behavior with altered sensory input
Infrequent flashbacks in a significant minority of users
Common experiences (e.g., “breathing walls”) across users
Psychoactive Drugs - marijuana
Effects depend on:
- Person-specific characteristics
- Current emotional state
Cognitive Effects (lasting beyond usage period):
- Impaired motor skills
- Impaired perceptual skills
- Disruption of memory formation
Hard to get reliable data on long-term cognitive effects
Psychoactive Drugs - Ecstasy
Introduced as a marital therapy drug in the 70’s
Effect:
- Feelings of openness,
- Euphoria, empathy, love, etc.
Mechanism:
- Release of dopamine / serotonin
- Blocks serotonin reuptake
Dangers:
- Dehydration in short term
- Insomnia, anxiety, depression in semi-short term
- Brain structure damage (long-term use)
- Memory, attention deficits (long-term use)
Social Psych
Scientific study of…
Beliefs
Attitudes
Behaviors
…of people in the presence of others.
How do other people affect your thoughts and behaviors?
How do you affect other people’s thoughts and behaviors?
Attribution/Motivation, Personality, Situation
Attribution - Beliefs about the causes of people’s behaviors
What caused him / her to do that?
Possible interpretations:
Personality - A person’s behavior is caused by their moral character and disposition
Situation - A person’s behavior is caused by the incidental conditions of their environment
Attribution is important because it affects how you RESPOND to other people’s actions
Fundamental Attribution Error
Overemphasize Personality
Underemphasize Situation
Tendency to believe other people’s behaviors are caused by their PERSONALITY rather than their
Defense against making the fundamental attribution error:
1) Think about how you and most other people behave under the circumstances
2) Actively try to generate potential, unseen causes for a
person’s behavior
How important are situations in determining behavior?
Zimbardo “prison” study
Set up in the basement of the psych. building at Stanford
Prisoners: undergraduates
Guards: undergraduates
Prisoners, guards knew they were randomly assigned to their group
After only a few days, some “guards” began to act like “guards”
Despite the arbitrary assignment to “guard” or “prisoner”, some guards were abusive:
Types of guard:
Type 1: “Tough but fair” guards followed prison rules.
Type 2: “Good guys” did favors for prisoners, never punished them.
Type 3: Hostile / inventive in punishments / humiliation.
Problems with Zimbardo’s Experimental Design
Demand characteristics” - Prisoners were forced (as part of the experiment) to do arbitrary humiliating activities to simulate prison life
“Hawthorne effect” - Zimbardo participated as prison superintendent. How did this affect people’s behavior?
“Selection effects” - What type of people would volunteer for this study? Are they different from other people?
Other concerns: Is this experiment ethical?
Attitudes
feelings based on beliefs
Conventional Thinking:
Attitudes determine our behaviors in response to situations
But do Behaviors also affect Attitudes?
My town has mandatory recycling
Behavior: I recycle
Attitude: I should be concerned about the environment
The “Foot-in-the-Door”
Behaviors affecting attitudes:
2 signs read “drive safely”
Sign A: big and ugly
Sign B: tiny and nice
Will you put sign A in your yard? Yes: 17%
Will you put sign B in your yard? Yes: ~100%
New situation:
Show up with Sign B first
Then later on ask to put sign A in the yard? Yes: 76%
Why does this happen?
Behavior - Put tiny “drive safely” sign in yard
New Attitude - I support safe driving
Behavior - Put big “drive safely” sign in yard
Cognitive Dissonance
Feeling uncomfortable or “guilty” when our behaviors do not align with our beliefs:
An example:
You eat meat, even though you believe that the way animals are treated on large-scale factory farms is morally wrong
To resolve conflict:
- Change behavior (stop eating meat; less likely)
- Change belief (deny evidence; believe situation is less bad than it actually is, etc.; more likely
Conformity
One way animals learn: Mimic the behavior of older animals
Humans are inclined to mimic behavior as well
Tendency to behave in a manner similar to others in your group
Overt: Peer Pressure
Covert: Unconscious responses to group dynamics
Sometimes good, sometimes bad:
Positive: Following social norms at a movie / restaurant
Negative: Not standing up for an individual against a group / not voicing your opinions at appropriate times
Factors that strengthen conformity
One reason to conform: Others may be right
Conformity greatest for difficult, important judgments
Non conformity leads to feeling insecure or incompetent
Group has 3+ people
Group is unanimous
Group has high status
No prior commitments that contradict the group
Behavior is observable by others
Culture stresses social standards
Obedience
People conform:
To avoid group conflicts / maintain social harmony
Because other people may have good information to help make better decisions
People obey to please authority figures
Obedience – Attempting to meet someone’s expectations
Motivation to please people (especially powerful people)
Why is some level of obedience important for society?
Your parents
The police
Your professor
The CDC during COVID?
Why is too much bad - people can take advantage
Obedience experiment
Most subjects will give “learner” highest shock
Many subjects will “obey” even though it causes cognitive
dissonance.
Instructor is perceived as authority figure
Instructor is nearby when shocks are delivered
Authority figure is supported by a legitimate institution
Victim is not visible
No role models for defiance
Social Loafing
Typically, people working together work less per person than people working alone.
Tug of War example:
Group A: Fooled to think they were pulling with other people
Group B: Pulled alone
Subs. in Group A used 82% of the force of subs. in Group B
People clap less hard in larger groups:
Group Polarization
Members of like-minded groups tend to become MORE extreme in their viewpoints:
Groupthink
Working groups feel pressure to keep “good group dynamic”
Dissenting opinions get suppressed
Bay of Pigs ex: Recordings of debate leading up to invasion showed signs of censoring of cabinet members with dissenting opinions
Prejudice
How prejudiced are people? Less than they used to be (in some places)
Who is affected? Ethnic minorities, gay people, women, religious groups… everyone?
Are people really less racially prejudiced… … or do they just answer questions that way?
How does prejudice originate? - cognitive strategies
Cognitive Strategies?
People use categories to efficiently represent the world:
Category: Fruits
- Sweet
- Grow on trees
- Have seeds
- Has a skin
- Healthy
Now if you are given a new fruit, you can assume it probably has these properties
How does prejudice originate? - exposure bias
Unlike fruits, we don’t get to directly interact with large number of people of all types
Instead we learn about them through TV, movies, etc.
Exposure bias against Muslims:
Nearly 100% of Muslims are not terrorists
But the ones who are get a lot of attention
Category “Muslim” takes on characteristic terrorist
Stereotypes
Overgeneralization of a group
- Not entirely made up
- Can be positive, negative, or neutral
- Often a negative exaggeration
Regardless, stereotypes negatively impact group relations
Who placed a personal ad for:
“a special lady to love and cherish forever”
Slightly feminized face (b) is picked by 66% to be
more likely to have placed the personal ad
Implicit bias
stereotypes can influence our behavior even without awareness
Even people who believe they have no biases against black
people may still behave differently toward blacks vs. whites
Task: “Shoot” quickly if person has a gun
Police and civilians more likely to shoot black man carrying harmless object than white man
Aggression
Animals can be bred / evolve to be aggressive:
What is the nature vs. nurture debate here?
Twin studies indicate aggression is in part hereditary:
Aggression - environmental factors
Conditions that make people uncomfortable make them aggressive, violent:
Does role-playing violence cause violent real-life behavior?
little evidence of a causal link
Small association between violent video game use and minor aggression, like as yelling and pushing
No evidence of increase in serious violence
Social Traps
Occur in any situation where:
- Everyone benefits if everyone follows a rule
(if everyone sets their thermostat at 68 degrees in the
winter it will help the environment)
- But if you cheat (secretly set your thermostat to 75), you
benefit, as long as everyone else doesn’t cheat
(environment is still helped, and you get a cozy house, too!)
End result: Everyone cheats
Prisoners Dilemma
What makes us like each other?
Familiarity - we like things we see often
Called the “mere exposure” effect.
An experiment on physical attractiveness:
HS Students took personality and aptitude tests
Were randomly assigned to be “couples” at a dance
Appearance was Only reliable predictor of how much the couples liked one another
No difference between men and women
Mood and attraction
Men are more happy around attractive women
Women are more happy around attractive men
Men are less happy around attractive men
Women are less happy around attractive women
What is attractive?
Many individual differences, but people seem to prefer “average” features:
One reason?
Composite faces are more symmetric
Symmetry may be an evolutionary sign of good health
Altruism - when do you get involved?
When will people help out a stranger?
Being altruistic is a decision process:
You’ve got to worry about becoming a victim yourself
In some places, helping is a virtue. Other places, not so much
Altruism - the bystander effect
When you have more people around, fewer will hep. As the number of people around increase, the percentage of people who help decreases.
Emotions
Happy, fearful, angry, sad, disgust
Bored, interested, etc
Fewer than 100 distinct emotions
Basics of emotions
Physiological response - heart beat, respiration, adrenaline
Expressive behavior - facial, vocal
Have a short duration - mood lasts longer
Either positive or negative, pleasant or unpleasant
Functions of Emotions
Communication (through facial expressions)
Communicate our feelings to others
Tell us what others are feeling
Motivate appropriate actions
Anger - being prevented from doing something - remove the barrier
Fear - threat or danger - free, hide, run
Autonomic Nervous System
Sympathetic - response to arousal, threat, stress
Parasympathetic - opposite, calming response
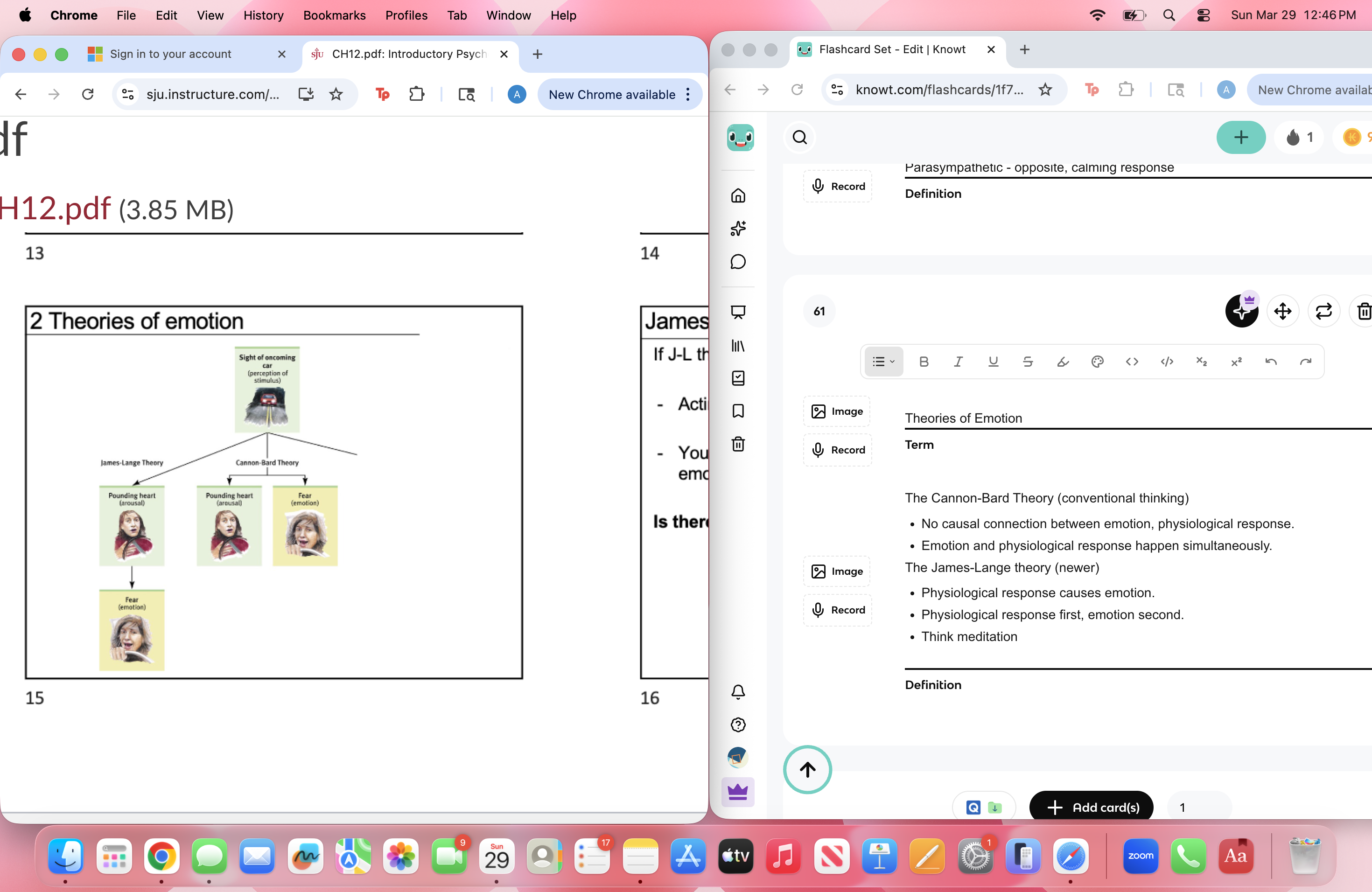
Theories of Emotion
The Cannon-Bard Theory (conventional thinking)
No causal connection between emotion, physiological response.
Emotion and physiological response happen simultaneously.
The James-Lange theory (newer)
Physiological response causes emotion.
Physiological response first, emotion second.
Think meditation
James-Lange Theory Supporting Evidence
If it’s correct:
Acting happy/sad can make you happy/sad - this doesn’t hold up
Your body needs to communicate to your brain to create emotions. - this doesn’t hold up
Higher injury (near neck) associated with decrease in emotional intensity compared to lower injury (near waist).
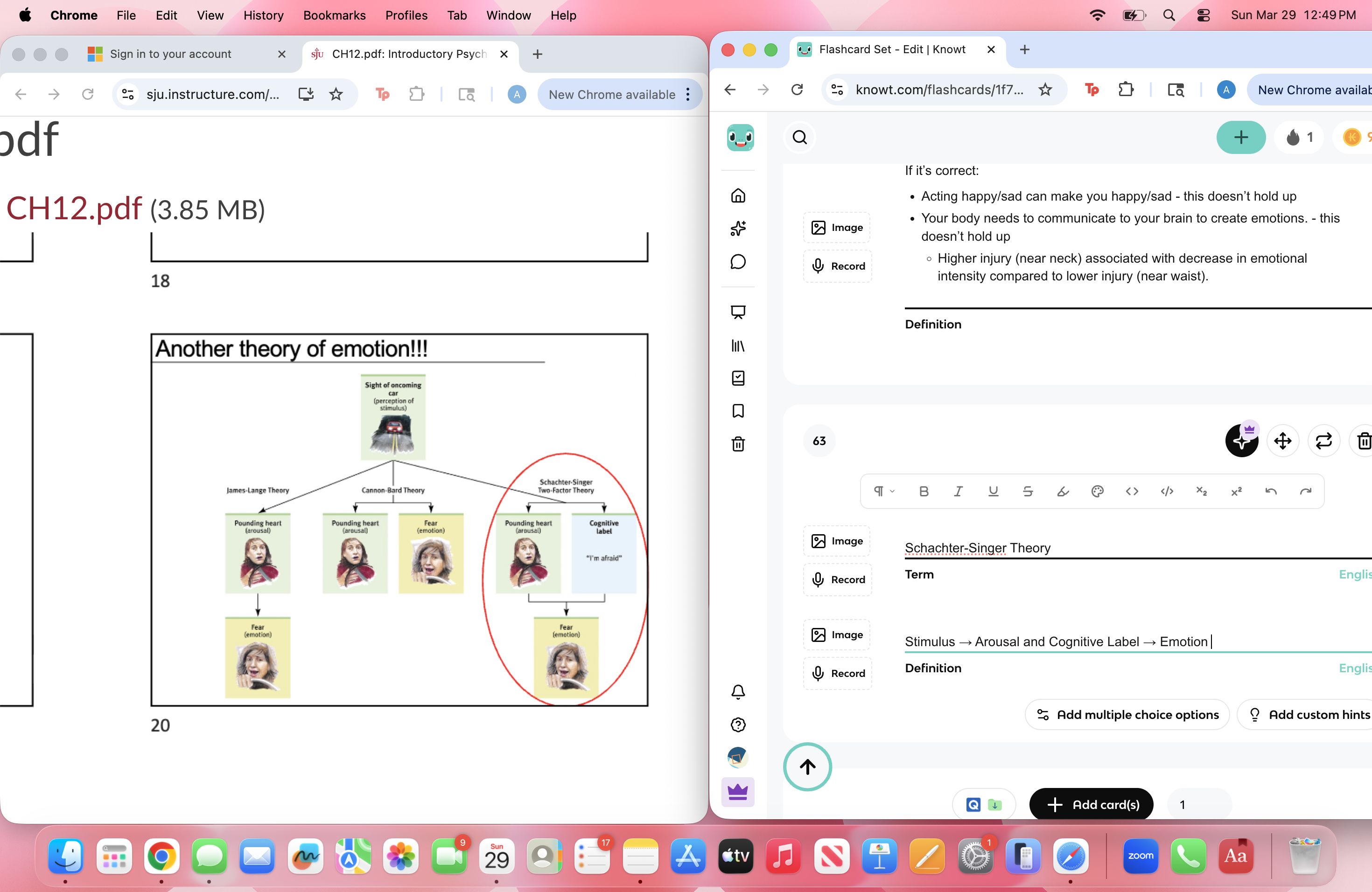
Schachter-Singer Theory
Stimulus → Arousal and Cognitive Label → Emotion
Famous Experiment:
Injected subjects with epinephrine
Sent them to a waiting room
IV 1 - Confederate in waiting room acts either
Angry
Happy
IV 2 - Participants either
Know they have been injected with epinephrine and what physio effects to expect.
Are naive(injected with epinephrine, but not told about the drugs effects).
When knowing - “i’m not angry/happy, I just feel like this because I got injected”
When naive - “why am i so amped up? I must be super angry/super happy like this guy.
Misattribution of Arousal
Capilano Bridge vs control nonscary bridge
Attractive woman/man would stop single men/women halfway across the bridge
Asked participants to tell a story about a picture
Gave participants their phone number, if they had questions about the experiment later.
Only worked for men
Scary bridge 9/18
Control 2/16
Misattributing those feelings of fear up feelings as arousal
The amygdala
Strong emotional experiences(especially fear and anger) can process emotions quickly(no cortex) or more slowly(with cortical processing)
Processing emotions very quickly may save your life. But bypassing cortex means that you may not have conscious awareness of what happened.
Complex emotions(guilt/jealousy) require the interpretative processes that happen in cortex.
Animals and amydgala
Stimulating amygdala triggers predatory behavior.
Cat just reacts; doesn’t have to think
Humans and amygdala
Functions - detecting and eliciting strong, basic, emotions
Subliminally presented fearful eyes generate different amygdala activity(fMRI) from happy eyes
Tumors in amygdala
Charles Whitman - gunman
No prior history of violence
But had a tumor near his amygdala
Non-verbal communication
People are good at detecting the emotional state of a person through facial expression
What is the major confound in his earlier research that Ekman overcomes with these studies?
Cultural learning
Many studies on this had been shows to people from industrialized societies - people were exposed to media.
Studied non-Western cultures that were exposed to no media
Participants were asked to match facial expressions to emotional stories. They consistently identified the same basic emotions.
This shows that facial expressions are universal and innate rather than learned.
Born with Emotions
Basic emotions / facial expressions seem to be innate
Are people good at detecting lies?
Generally no
60% of people lie during typical 10 min conversation
Regular people, relying on non-verbal are not good at it.
88% of police officers believe they can detect deception.
Police lie detection actually below average.
Most signs of deception son’t actually predict lying.
Gaze avoidance
Fidgeting
Restless foot and leg movements
Frequent body posture changes
Can a machine detect lying?
Polygraphs use physiological response to detect stress.
50 suspects who late confessed, 50 whose innocence was later established
Instead of asking questions, measure physiological response to pictures of crime scenes vs. similar pictures
Use brain imaging?
- Lying requires generating new content
- Answering truthfully requires memory
- These processes happen in distinct brain regions
Does money make us happy?
While American buying power has increased steadily (until recently), happiness has remained constant
“Money can’t buy happiness”
What makes us happy?
Happy people tend to:
- Have high self-esteem (in individualistic cultures)
- Be optimistic, outgoing, and agreeable
- Have close friends or a satisfying marriage (or both!)
- Enjoy their job
- Have an active religious faith
- Sleep well
- Exercise
Happiness is not related to:
- Age
- Gender
- Parenthood (choice to have children)
- Attractiveness
How does our brain gauge how happy we should feel?
The Adaptation-Level Phenomenon
Happiness is judged relative to recent experience
So positive changes are only enjoyed in the short term
When do people appreciate good health?
Relative Deprivation
We are unhappy if we judge ourselves to be worse off than our peers
When a professional baseball player gets a million-dollar contract, we don’t feel bad…
…but if your co-worker gets a big promotion and you don’t, you might have a negative reaction
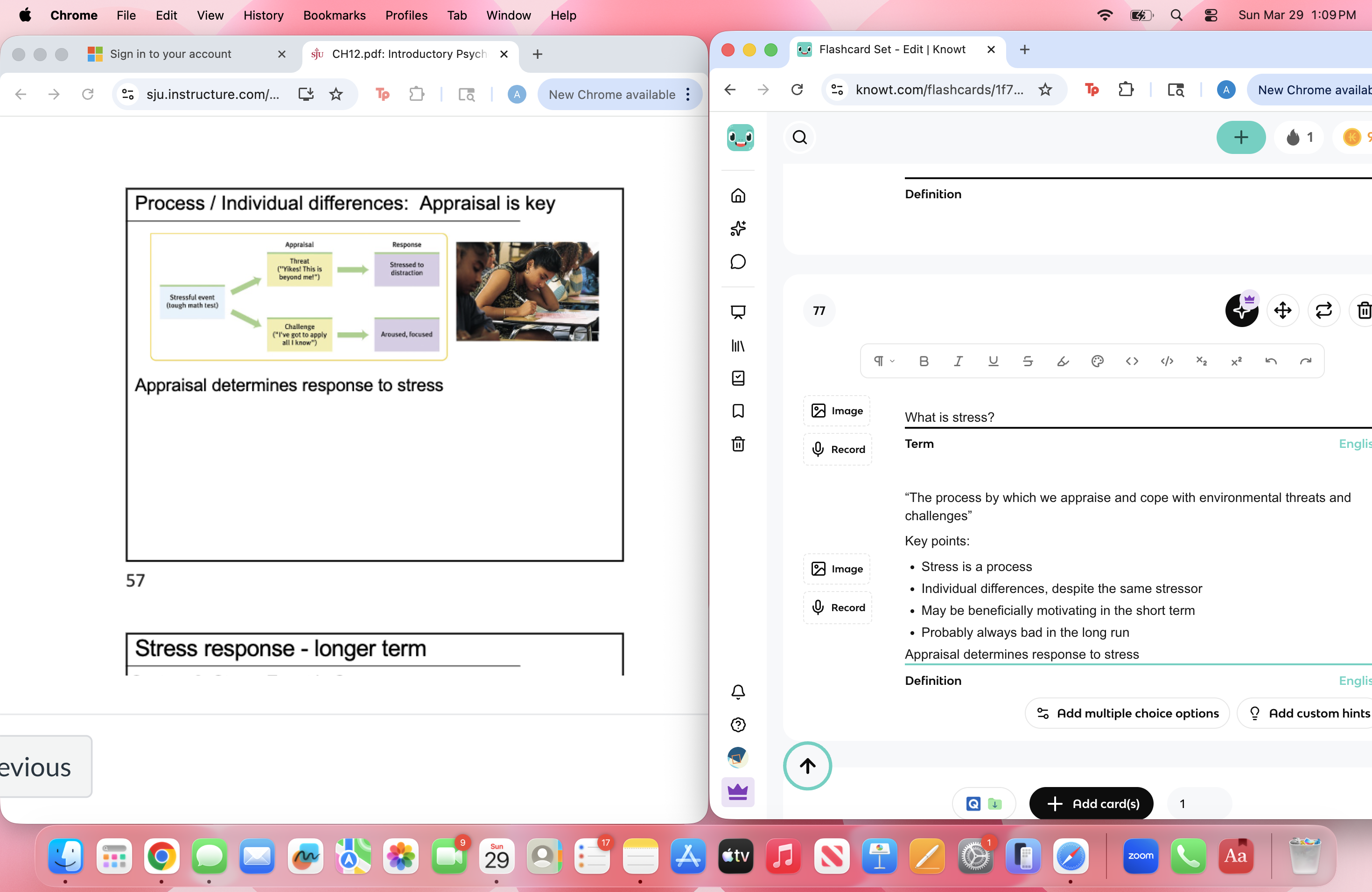
What is stress?
“The process by which we appraise and cope with environmental threats and challenges”
Key points:
Stress is a process
Individual differences, despite the same stressor
May be beneficially motivating in the short term
Probably always bad in the long run
Appraisal determines response to stress
Stress response short term
System 1 - stress event happens
Physical stressor (e.g., pain) triggers
Adrenal glands release of epinephrine, norepinephrine
ANS increases heart rate, inhibits digestion, etc.
Happens fast
Stress response longer term
System 2: Stress Event is Over
Release of hormones like cortisol
Restores homeostasis after stress
Much slower
Stress will kill you
Stress system evolved for short-term stressors
Unfortunately, many modern-stressors are VERY long term
- Will I be able to afford a house?
- Will I have enough money to retire?
- Is the country headed in the wrong direction?
Long term stress has been linked to accelerated aging
Immune response to stress
Why does stress make you sick?
Stress hormones interfere with white blood cells
Stress causes:
Wounds to heal more slowly
Top 10 most stressful events
Death of Spouse
Divorce
Marital Separation
Jail Time / Death of friend or family member
Personal Injury / Illness
Marriage
Getting Fired
Marital Reconciliation
Retirement
Pregnancy
Change in Financial State
Why are we stressed out?
Many stressors are related to “lack of control”
People, animals get stressed when they cannot actively control events in their lives
Rat with no control develops exhibits “learned helplessness”
Symptoms look a lot like clinical depression
Personality and Stress
Type A: Reactive, competitive
Type B: Relaxed, easy-going
3000 high risk subjects, 35-59 yrs. Old
257 heart attacks
69% of heart attacks were type A’s
Explanatory Style
Something goes wrong. Is it:
Internal (your fault)…..or….. external (somebody else’s)
Permanent (long lasting)…or…temporary
Universal (affecting many parts of your life)…or… specific to this incident
Stress Management
Exercise - “Treatment” = aerobic exercise, relaxation, or nothing
Alternative medicine - Herbal Medicine Magnets, Folk Remedies Mind-Body Control, Therapeutic Touch Etc.
Most have not been experimentally tested
Some experimentally shown to NOT work
Some are actually harmful (esp. herbal medicines)
Lifestyle changes - reduce stress!
Control Group: Standard advice on medication, exercise, and diet
Lifestyle Group: Same + advice to “slow down”, relax, smile, laugh, etc.
Spirtuality/Faith - Some studies suggest that belonging to a religious group
correlates with prolonged life
Hard to interpret because these people usually engage in less alcohol and drug use.
Obesity
Smoking is on the decline and obesity is on the rise
Correlates with: Heart disease, diabetes, high blood pressure, gallstones, arthritis, some types of cancer
“Relative risk” of death by BMI:
People discriminate against overweight people
Employers discriminate against overweight people
Affect is greater for women:
Lifestyle choices
many health problems are linked to behavioral choices - smoking as a big one
We don’t have a cure for cancer, heart disease, etc.
But many diseases can be prevented by modifying behavior
So, health psychologists try to modify behavior to save lives
What is abnormal?
Abnormal Psychology = Study of “Abnormal” Behavior
Deviance - “Too Different” from the average
Another Problem: Abnormal suggests “bad”
Many “abnormal” behaviors aren’t harmful
Exercising twice / day
Geniuses with abnormally high intelligence
Practically speaking - Clinical psychologists are interested in behaviors that are abnormal and harmful
How do you decide if a behavior is normal or abnormal?
Why is it better to focus on harmful behaviors?
Oneself: interferes with daily functioning
- Exercising 15 hours / day
- Avoiding social interactions
Others / society: disrupts / impairs group behaviors
- Unwarranted aggressive behavior
- Narcissism
Diagnostic Challenges
Same disorder can present differently across people
Some symptoms may be present, others absent
Disorders often come in groups
Diagnosis often relies on self report, introspection
Modern (best?) approach: Standardization
DSM
A manual of checklists for all disorders
- Tells the clinician if a person meets diagnostic criteria
- Classifies disorders:
Axis 1, Axis 2, etc. – if you’re interested in being a clinical psychologist,
Good
- Very systematic, based on lots of data
- Reliable, 2 clinicians usually reach the same diagnosis
Bad
- May categorize too many people with a mental disorder
- Influenced by non-scientific agendas
Generalized Anxiety Disorder (GAD)
Disproportionate anxiety signals a disorder
Criteria: Excessive anxiety on most days for 6 months or more
Symptoms:
Restlessness
Fatigue
Difficulty Concentrating
Irritability
Muscle Tension
Sleep Disruption
GAD is a chronic, high level of anxiety
Other anxiety disorders are more transient
Phobias
Intense, irrational fear in anticipation of or in the presence of a particular object or situation
Specific Phobia: flying, heights, spiders, blood, …
Social Phobia: performance situations, meeting people
Agoraphobia: Outdoor, wide open places, situations where escape (esp. from embarrassment) is difficult
More common fears are not more common phobias
Phobias don’t seem to be related to “normal scariness”
How do phobias develop?
Classical conditioning - one trial conditioning; through single exposure, especially in young children/
When something scary happens that thing can they just cause the fear alone.
To extinguish a conditioned response
Present CS (Bell) but no US (Food)
Eventually CS (Bell) will no longer elicit CR (Salivation)
Panic Disorder
Recurrent “Panic Attacks”
- A normal, but intense, fear response
- But without any obvious danger
Panic attacks result from a “positive feedback loop”:
- Distress about future attacks → more panic
- Worry about health effects of attacks → more panic
Panic disorder often co-occurs with
Agoraphobia - Irrational, excessive fear of outdoors, open places where escape to safety is difficult; stop going out
Social Anxiety - stop socializing; for both of these, don’t want to have a panic attack in front of others
Believe that others are observing you - self conscious
Noticing every mistake they make - paranoid
How to treat panic disorder?
Treat with cognitive methods - not likely having heart attack
Treating thoughts, not behaviors
Obsessive-Compulsive Disorder (OCD)
Obsessions: Recurrent thoughts / images that cause anxiety, interfere with patient’s life
Compulsions: Repetitive behaviors that a person must perform, to reduce anxiety caused by obsessions
Cleaning - may do something directly related
Checking
Order/Balance
Touching/Counting - ritualistic behavior to make them feel better about it
Obsessions, compulsions are NOT random
Obsessions = evolutionarily adaptive thoughts
Compulsions = evolutionarily adaptive behaviors
But… in OCD, thoughts and behaviors are excessive
In 2013 OCD was reclassified from Anxiety disorder to its own category, “Obsessive-Compulsive and Related Disorders”
Genetic, brain activity differences between OCD and other anxiety disorders suggests it is distinct
New theory suggests OCD primarily involves problems with “self- regulation”. However, OCD almost always includes anxiety.
Main point: DSM / understanding disorders is an ongoing process
PTSD
Previously an Anxiety disorder
Reclassified “Trauma & Stress-Related” disorder in 2013
Disabling response to experiencing very high stress
Symptoms:
Nightmares
Flashbacks
Excessive startle response
Anxiety
Depression
Usually lasts less than 6 months, but can last much longer
Commonly treated with talk-therapy and antidepressants
WWI - Shell Shock
Not just soldiers:
Accident / disaster survivors
Sexual Assault victims
Prostitutes
Witnesses of atrocities: