Seronegative (RHEUM)
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
PEAR mnemonic
P - psoriatic arthritis
E - enteropathic spondyloarthropy
A - ankylosing spondylitis
R - reactive arthritis
PEAR diseases share
- RF negative
- HLA-B27 association, family associated
- Inflammatory oligioarthritis or monoarticular
- Inflammation of fascia, ligaments, tendon, bone (enthesitis)
- Extra articular involvement
Psoriatic arthritis (PsA)
Patients with psoriasis (strongest risk factors)
HIV
30-55 y/o
Joint/tendon trauma
Upper extremities and small joints in hand
Symmetric or asymmetric, gradual
PsA pathophysiology
Autoimmune (environmental trigger —> autoimmune overreaction)
T cell infiltration, angiogenesis
Chemokines/cytokines
Pencil in cup finding
Most common in psoriatic arthritis (PsA)
Erosion of DIP in pointed manner

PsA medicine
DMARD
MTX > suldasalazine, leflunomide
Anti-TNF: etanercept, adalimumab, infliximab
Ankylosing spondylitis (AS)
Males 20-30 y/o
MC seronegative spongyloarthropathy
Chronic dull low back pain and stiffness worse at night
- Improves with heat, exercise
SI - bilateral SI joint involvement
Spine - fusion in ascending manner, kyphosis, reduced mobility, "bamboo spine", question mark posture
5A's
5 A's of AS
1. Anterior uveitis
2. Aortic regurg
3. Achilles tendinitis
4. AV block
5. Amyloidosis (rare and/or late)
AS dx and tx
HLA-B27
Dx:
- Elevated ESR, CRP
- ANA neg
- Imaging of back = bamboo spine
Tx: NSAIDs >
- anti-tnfs: etancercept, infliximab
- Surgery for deformity
- Immobilization when back trauma
- PT
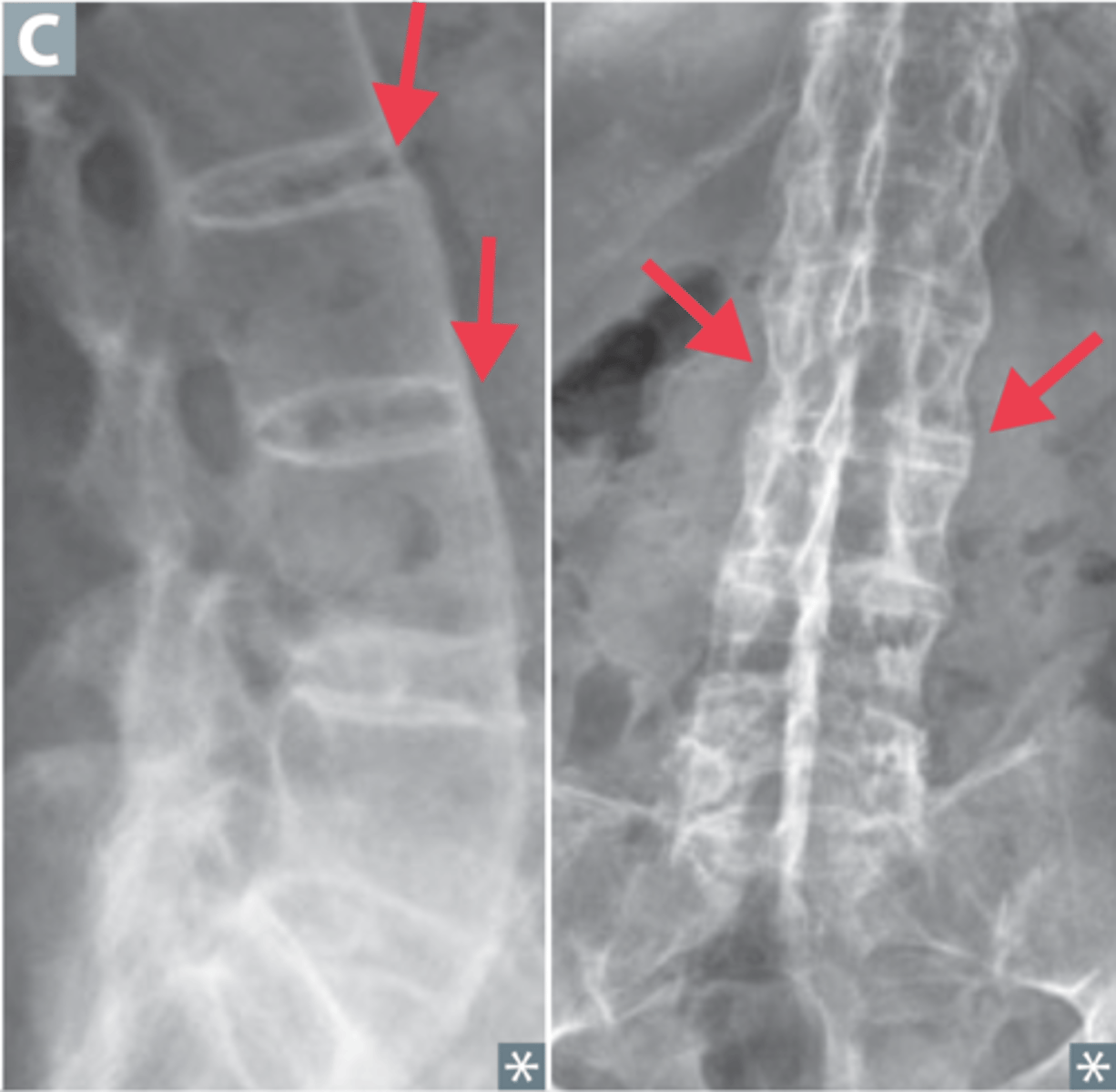
Bamboo spine
AS finding
Reactive arthritis
Reiter's syndrome
Extra articular:
- Keratoderma blennorhagicum
- Mouth ulcer
Reactive arthritis dx and tx
Dx: Joint aspiration - cloudy
- Test serum for chlamydia
Tx: NSAIDs, intra-articular steroids
- DMARDs > anti-TNF for perisistent or refractory disease
Reactive arthritis x ray findings
X ray - normal at beginning
- marginal erosion
- plantar spurs
- sacroilitis
- asymmetrical syndesmophytes
Enteropathic Arthritis
Stomach linked - IBD (crohns or ulcerative colitis) bacterial & parasitic infections, celiac, pseudomembranous colitis, whipple's disease
Peripheral arthritis, asymmetric and large joints
Enthesitis, dactylitis
Uveitis, erythema nodosum
Fistulas
Enteropathic Arthritis dx and tx
Dx: HLA-B27, CPR and ESR increased
- elevated wbc in synovial
- x-ray like AS
Tx: different for inactive vs active
Inactive enteropathic arthritis tx
NSAIDs >
- Celebrex preferred
Intra-articular steroids
DMARDs for refractory
- sulfasalazine or MTX for peripheral
- Adalimumab for axial
Active enteropathic arthritis tx
Include GI in treatment
- Celebrex if tolerated
Sulfasalazine, MTX
Large vessel vasculitis examples
Giant Cell Arteritis
Takayasu's arteritis
Medium vessel vasculitis examples
Polyarteritis nodosa
Behcet's disease
Small vessel vasculitis examples
Eosinophilic Granulomatosis with
Polyangitis
Granulomatosis with Polyangitis (GPA)
Vasculitis
Inflammatory diseases of blood vessels that lead to
vessel damage and organ dysfunction
Common presentations include systemic symptoms, skin
lesions, organ damage, and vascular occlusion
Giant cell arteritis
AKA temporal arteritis
Women > 50 y/o (with polymyalgia rheumatica)
Granulomatosis inflammation of large vessels
Temporal artery > aorta, external carotid, vertebral
Blindness and aneurism risks
Headache, scalp tenderness
Absent temporal pulses
Palpable nodules
Giant cell arteritis dx and tx
Dx: ESR > 50 mm/hr but not requires
- Biopsy of temporal artery --> multinucleated giant cells
- Ultrasound with thickened blood vessel wall = halo sign
Tx: High dose steroids prednisone >
- IMMEDIATE treatment, especially for vision loss
- Vision loss = IV steroids
- Referral to opthalm
Takayasu Arteritis
Granulomatous vasculitis of aortic arch and pulmonary arteries causing fibrosis, stenosis, and narrowing
Women > 10-40 y/o
Limb ischemia and absent pulses in upper extremities
Aortic aneurysm, stroke
Secondary HTN due to renal artery stenosis
> 10 mmHg BP difference between arms
Visual disturbances
Takayasu Arteritis dx and tx
Dx: angiography --> narrowing of aorta or primary branch
- elevated ESR and CRP
- CBC: normochronic, normocytic anemia, leukocytosis
Tx: High dose corticosteroids >
- DMARDs (MTX or azathoprine)
- Revascularization
Polyarteritis nodosa (PAN)
Middle aged men
Nervous, heart, GI, kidney system vasculitis --> necrotizing arteritis
- PMN invasion into all layers of vessel = reduced luminal area
- Ischemia, infarct, aneurysms
- Sx affecting all symptoms (abdominal pain, MI, HTN, renal failure, neuropathy, stroke)
Raised diastolic > 90 mmHg
Hep B, HIV, drug reactions
Rosary sign
Livedo reticularis rash, skin ulcers
Polyarteritis nodosa (PAN) dx and tx
Dx: microaneurisms
- Fecal occult blood test
Tx: Corticosteroids
- Graduate to cyclophosphamide if severe
Behcet disease/Syndrome
Turkish, middle eastern men
Oral, genital ulcers, erethyma nodosum
Uveitis
Mono / oligio arthritis
Neurological features
THROMBOSIS !
Behcet disease dx and tx
Dx: skin pathergy
- needle prick --> papule < 48 hrs
Tx:
- Topical steroids - ulcers, opthalmic for eye
- Sucralfate
- Colchicine, apremilast for prevention of lesions
Eosinophilic Granulomatosis with Polyangitis (EGPA)
AKA churg-strauss syndrome
(CSS)
Necrotizing granulomatous inflammation = eosinophilia
- Asthma
- Chronic rhinosinusitis
- Widespread involvement, other than respiratory; cardiac, GI, skin, renal, neurologic = skin lesions, peripheral neuroathy, heart failure, myocarditis, pericarditis, VTE, renal failure, MI
EGPA dx and tx
Dx: elevated eosinophils (BAL)
- Lung or skin biopsy
- p-ANCA
- CXR/CT opacities
- Sinus CT opacification
Tx: Prednisone, IV steroids when systemic
- Cyclophosphamide for cardio
- Rituximab if ANCA +
Granulomatosis with Polyangiitis (GPA)
c-ANCA associated, necrotizing, granulomatous affecting older adults
- Respiratory: septal perforation, saddle nose, mucosal ulceration, OM, rhinorrhea, hemoptysis, pulm nodules, tracheal hoarseness
- Renal: nephritic syndrome (blood, protein, HTN, uremia)
GPA dx and tx
Dx: + c-ANKA
- Cxy/CT nodules
- Anemia (monochronic, normocytic), thrombocytopenia, leukocytosis
- Increased Cr, urine sediment
- Skin, kidney, renal biopsy
Tx: steroids + rituximab
- Cyclophosphamide if needed (instead of rituximab)
- Renal transplant
EPGA vs GPA
Both:
- Granulomatous, necrotizing
- Affecting respiratory = opacities in CXR/CT
- ANKA associated
- Dx: skin or lung biopsy
- Tx (steroids, cyclophosphamide, rituximab)
EPGA: more involved with other organ systems / systemic
- eosinophilia
- p-ANKA
- Nasal polyps, sinus opacification
GPA: + renal only
- c-ANKA
- Nasal ulcers, more upper and lower resp sx
- Older adults
- Anemia, thrombocytopenia, leukocytosis
Thromboangiitis Obliterans (TAO)
AKA Buerger's disease
- Young male
- Heavy smoker (tobacco and/or dat green)
Upper and lower extremity ischemia, arthralgia
- Knee, wrist MC for arthralgia
- Ischemia --> ulcers --> gangrene
Gangrene: fingers and toes MC, painful, red, cyanotic
= "autoamputation"
Highly cellular and occlusive with thrombus (sparing vessel wall)
- migratory superficial throbophlebitis
- Raynauds
TAO dx and tx
Dx: positive allen test
- < 50 y/o
- Ankle-brachial index (ABI)
- Biopsy: definitive, not usually needed
- Ddx: repetitive trauma (jackhammer operator for example)
Tx: Smoking cessation only option that is curative
- ulcer debridement and dressing changes
- Vasodilators, CCB