Prosthetics: Amputation Overview (via jillianmaul8)
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
Biggest driver of dysvascular amputations; encompasses arteriosclerosis, chronic venous insufficiency, and burger's disease
Peripheral vascular disease (PVD)
Most common cause of LE amputations
Dysvascular (82%)
T/F: nearly 50% with an amputation due to vascular disease die within 4 years
TRUE!!
Path to foot amputation from PVD
Foot trauma —> wound —> infection —> infection spreads to bone (osteomyelitis) —> amputation to prevent systemic infection
PVD causes ___ circulation in the limb which prevents adequate healing & immune response
DECREASED
Other cause of dysvascular amputations; leads to micro and macrovascular disease and neuropathies
Diabetes
This makes up only 16% of amputations; causes include compound fractures, blood vessel rupture, compression injuries, MVA, GSW, frostbite, severe burns; common among males and young adults
Trauma
This cause of amputation usually occurs in older (60+), diabetic, overweight, less active patients who have a slowed healing rate due to poor circulation
Dysvascular
T/F: In dysvascular amputation, 30-50% of contralateral limbs are amputated as well
TRUE!!
2 causes of dysvascular amputations
Diabetes + PVD
This cause of amputation usually occurs in younger, male, active patients who may have no past medical history and often have a faster return to activity
Traumatic
Most frequent cause of cancer amputations that mostly occurs in 11-20 y/os is ___ wherein cancer creates structural weakness or life-threatening condition
Osteosarcoma
This type of amputation occurs when an individual is born with incomplete or absent limb; unknown but risk is higher with exposure to certain chemicals
Congenital limb difference
T/F: trauma amputations may be preceded by attempts to salvage or reconstruct the limb that ends up being unsuccessful (non-healing, chronic p!, limitations)
TRUE!
This type of amputation has a faster return to activity, patient may have no PMH, more likely male and younger
Traumatic
This type of amputation has a slower healing rate and 30-50% of cases result in contralateral limb amputation as well
Dysvascular
This term is used when an amputation extends across the axis of a long bone
TRANS (ex: transtibial; transphalangeal)
Amputations between long bones or thru a joint is called a ___
Disarticulation (ex: knee disarticulation, toe disarticulation)
This term is used when a part of the foot or hand distal to the ankle or wrist is amputated
Partial
The ____ is the portion of the limb remaining after the amputation; stump is an alternate term but not preferred
Residual limb
Levels of LE amputation
- Hemi-Pelvectomy/Hip Disarticulation
- Trans-Femoral/Knee Disarticulation
- Trans-Tibial
- Ankle disarticulation (Symes)
- Partial Foot, ray, and toe
Impacts of amputation level
-fit and control of prosthesis (bony anatomy, lever arm)
-distal WBing
-contractures
-posture/balance
-gait mechanics and metabolic cost
This LE amputation is rare and involves the removal of the entire leg (hip, buttock, and pelvis); performed secondary to bone or cartilaginous tumors, trauma, or advanced infection
Hemipelvectomy
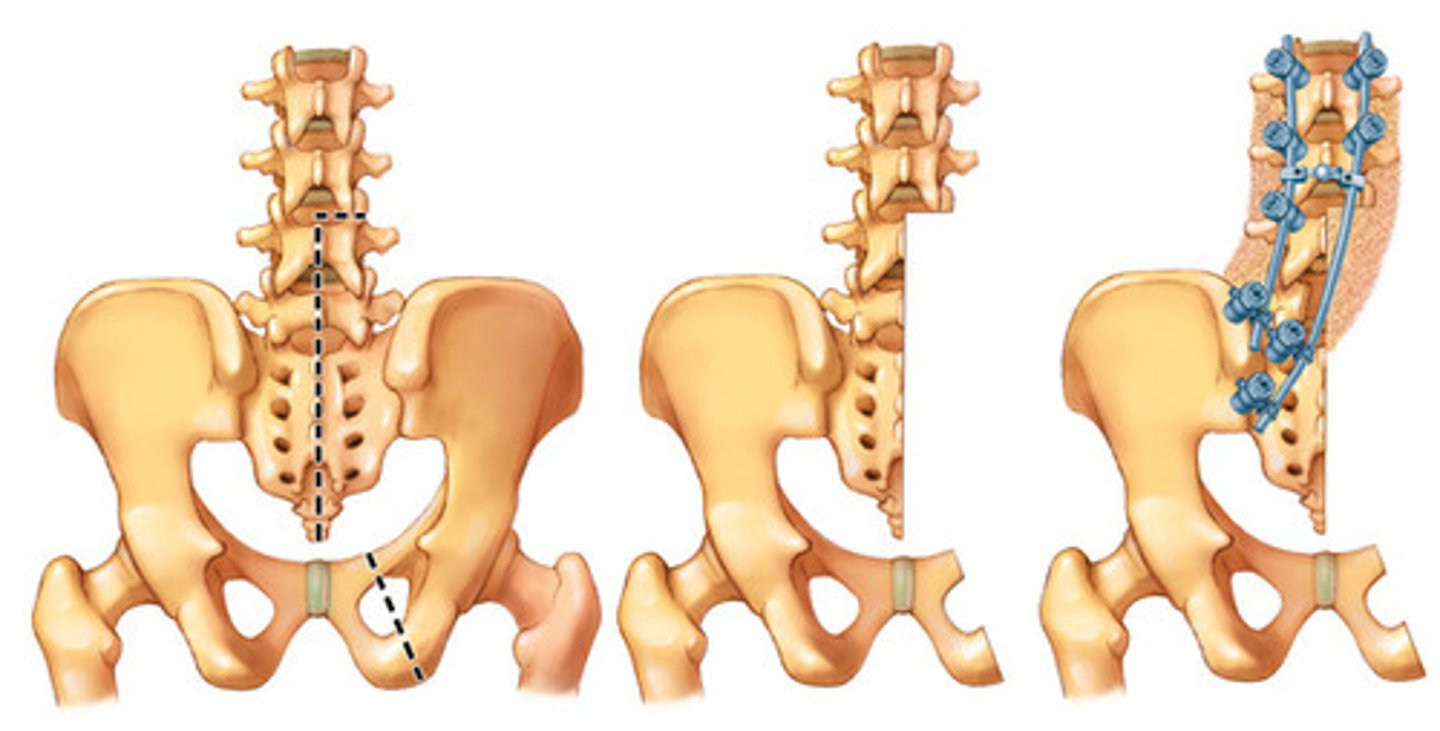
This LE amputation is rare and involves excision of LE at the hip joint; the remaining musculature is closed over the acetabulum; performed due to trauma, vascular insufficiency, and femoral sarcomas
Hip disarticulation
Considerations for hemipelvectomy and hip disarticulation
-limited bony anatomy available for control
-lacks good WBing surface
-contractures NOT an issue
-laying,sitting,standing affected
-gait slow + asymmetrical; high metabolic cost
Are contractures an issue in a hemipelvectomy/hip disarticulation?
NO!
How does a hemipelvectomy/hip disarticulation affect prosthetic use?
Less bone & less lever arm = harder to control; often not used for gait
How does a hemipelvectomy/hip disarticulation affect gait and metabolic cost?
Gait asymmetrical & slow // metabolic cost high
If not in a wheelchair, what AD would be good for hemipelvectomy/hip disarticulation?
Crutches
Balance/postures in what positions are affected by hemipelvectomy/hip disarticulation amputations? (3)
Laying, sitting, standing
T/F: patients with hemipelvectomy and hip disarticulation frequently use prosthetics for ambulation
FALSE!!!
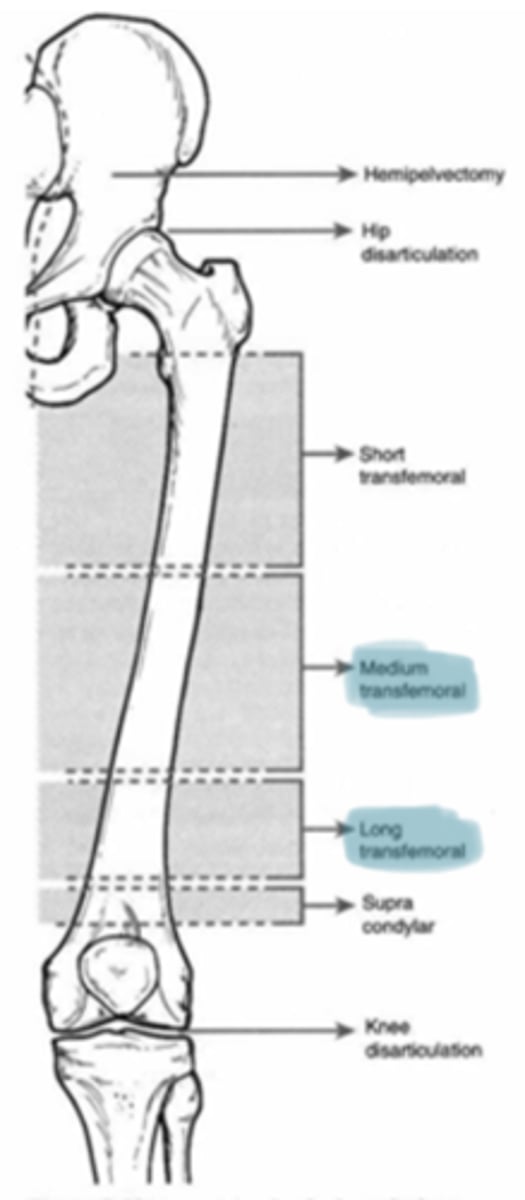
This type of LE amputation is ~25% of amputations and is also known as an above the knee amputation; performed at junction of middle and lower 1/3 of femur; provides room for prothestic knee; caused by dysvascular or trauma
Transfemoral amputation (TFA)
Considerations for transfemoral
-bony anatomy is moderate for control of prosthetic
-avoid distal end WB
-hip muscle contractures (flex, ABD, ER)
-sitting + standing affected
-gait asymmetrical and slow, metabolic cost high
Can you WB on a transfemoral amputation?
NO not on distal end
What hip muscle contractures are at risk for contractures in transfemoral amputations? (3)
Flex, ABD, EROT (limit stride length and push off in ambulation)
Balance in what positions are affected by transfermoal amputations? (2)
Sitting posture & static balance
How do transfemoral amputations affect gait and metabolic cost?
Asymmetrical + slow // increased metabolic cost
This LE amputation is rare; amputation goes through knee joint; often caused by diabetes, PVD, and trauma
Knee disarticulation

Which could you bear distal weight on: knee disarticulation or transfemoral?
Knee disarticulation (broad, horizontal distal end)
Sitting, standing, and gait in a patient with knee disarticulation are the same for what other amputation?
Transfemoral
In which amputation would the bulbous end complicate prosthetic fitting and limit space for knee mechanisms since it would be lower than contralateral anatomical knee (also may impact cosmesis) ?
Knee disarticulation
T/F: prosthetics are easy to fit for knee disarticulation
FALSE!! Bulbous end complicates it
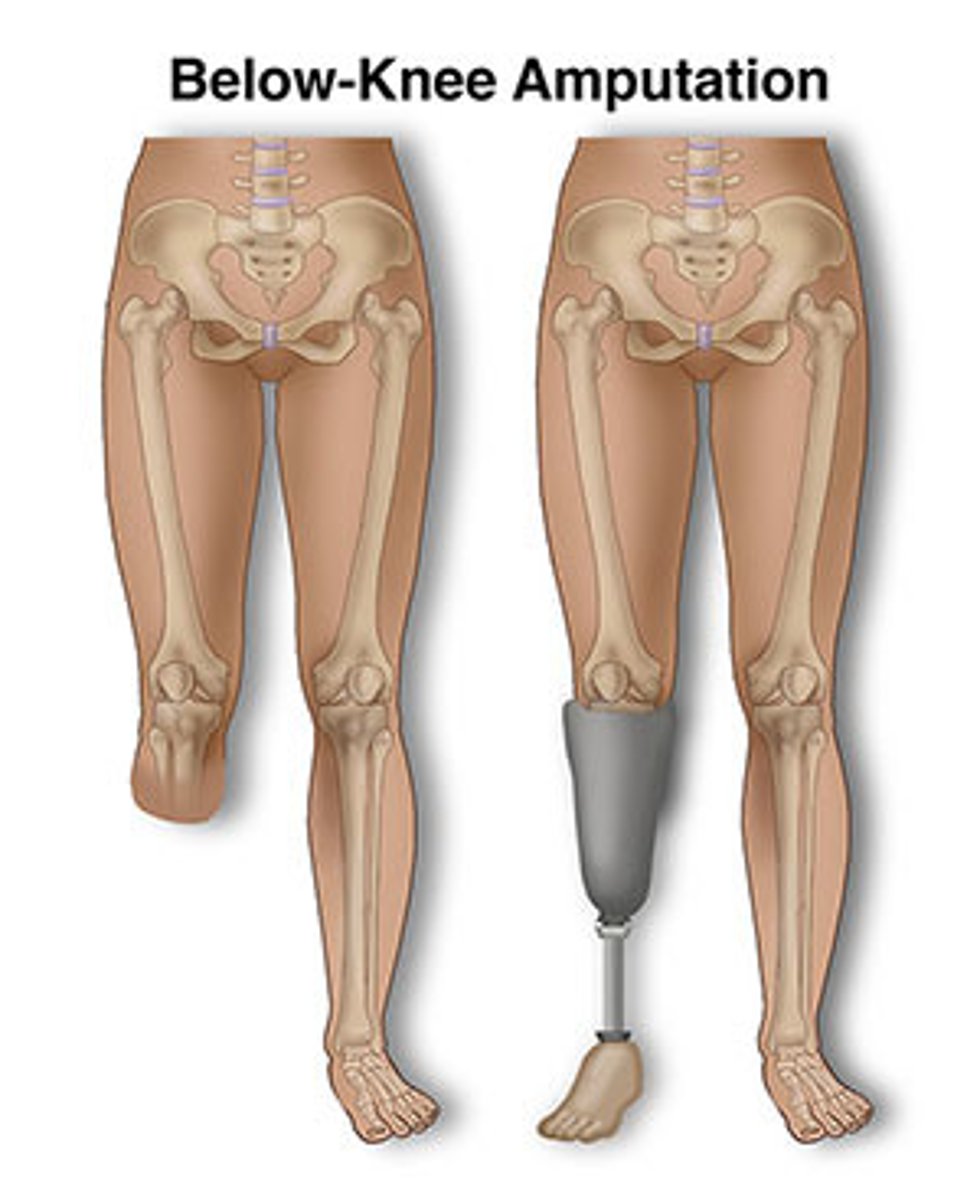
This LE amputation is ~25% of all amputations and also known as a below the knee amputation; standard length is 5-6 inches of tibia remain to provide room for prosthetic foot; caused by DM, PVD, trauma
Transtibial amputation
Considerations for transtibial
-good control of prosthesis
-a void WBing on distal end
-knee flexion contracture
-sitting affected by socket
-gait asymetric and slow
Which has better lever for control of prosthetic: transtibial or transfemoral?
Transtibial
Can you have distal WBing on a transtibial amputation?
NO!
What position would be affected by the socket of a transtibial amputation?
Sitting
What contracture would be common in a transtibial amputation?
Knee Flexion
This amputation is Disarticulation of the talocrural joint with removal of the inferior projections of the tibia and fibula; Prevents development of equinovarus deformity resulting from unopposed plantar flexors
Ankle (symes) disarticulation

In this amputation, the heel fat pad is preserved and attached to the distal tibia to allow for WBing capacity, but can also have migration of the heel pad
Ankle (symes) disarticulation
T/F: symes and distal amputations are 1/2 of all LE amputations
TRUE!!
Considerations for symes disarticulation
-good control of prothesis
-bulbous end complicates prosthetic fitting
-can ambulate short distance w/o prosthetic
-gait same as transtibial (slow, asymmetrical)
Ankle (symes) disarticulation allows a (long/short) lever arm of the tibia
LONG = good control of prosthesis!
In this amputation, Bulbus end complicates prosthetic fitting and limits space for foot mechanism and Prosthesis use can create limb length discrepancy
Ankle (symes) disarticulation
Ankle (symes) disarticulation can ambulate for (long/short) distances without a prosthesis
SHORT
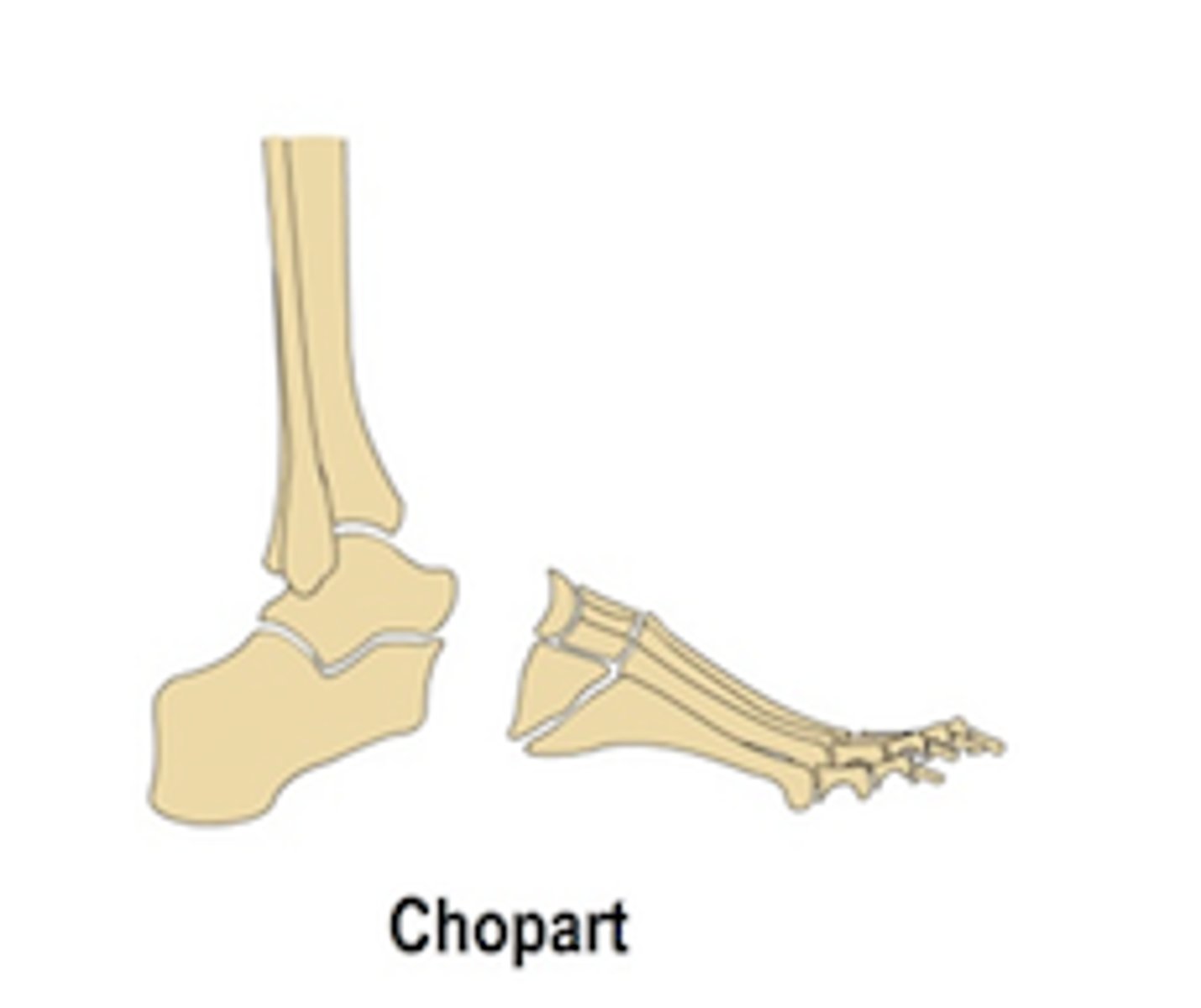
This partial foot amputation is a midtarsal joint disarticulation; preserves calcaneus and talus
Chopart
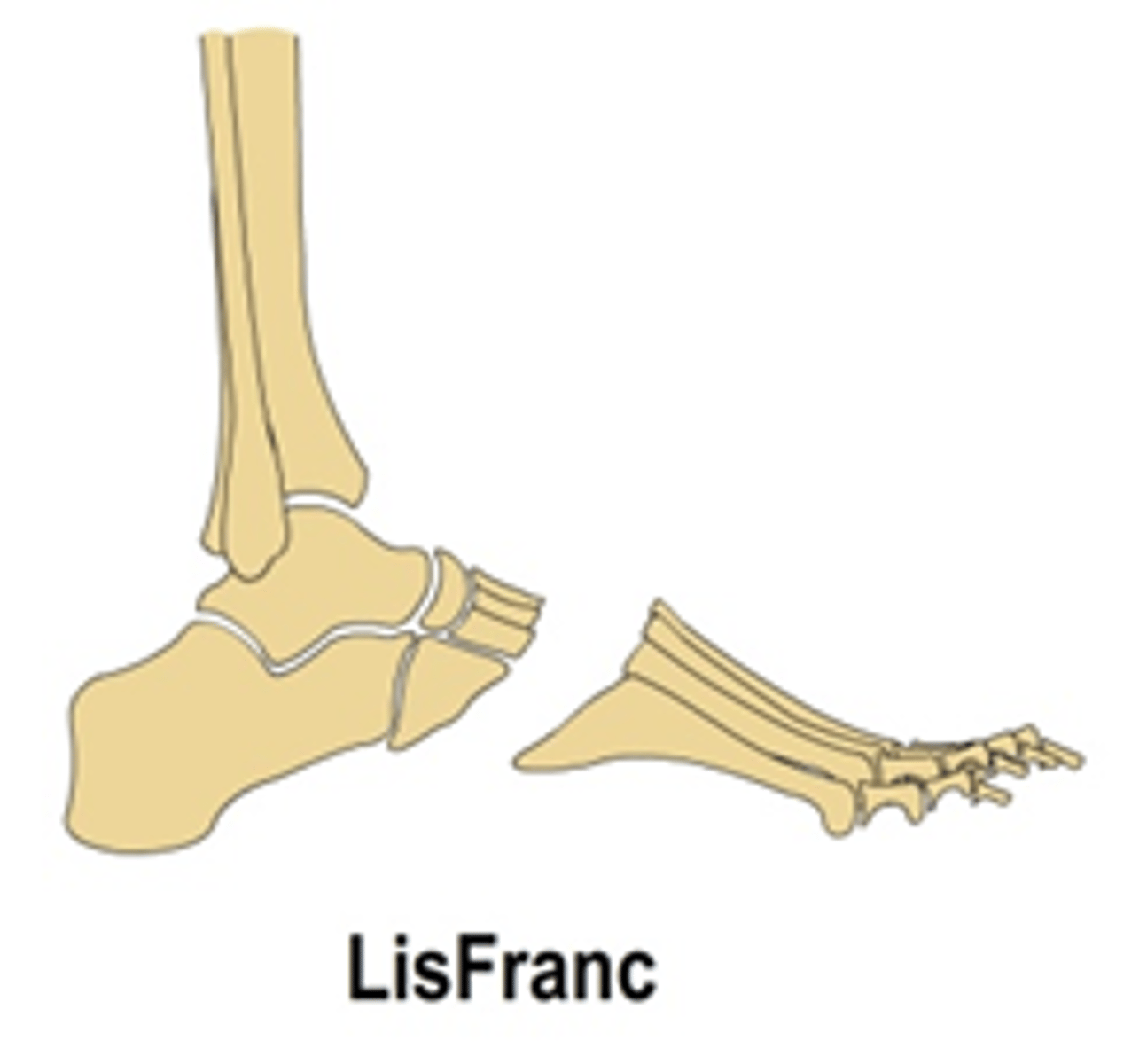
This partial foot amputation is a tarso-metatarsal joint disarticulation
Lisfranc
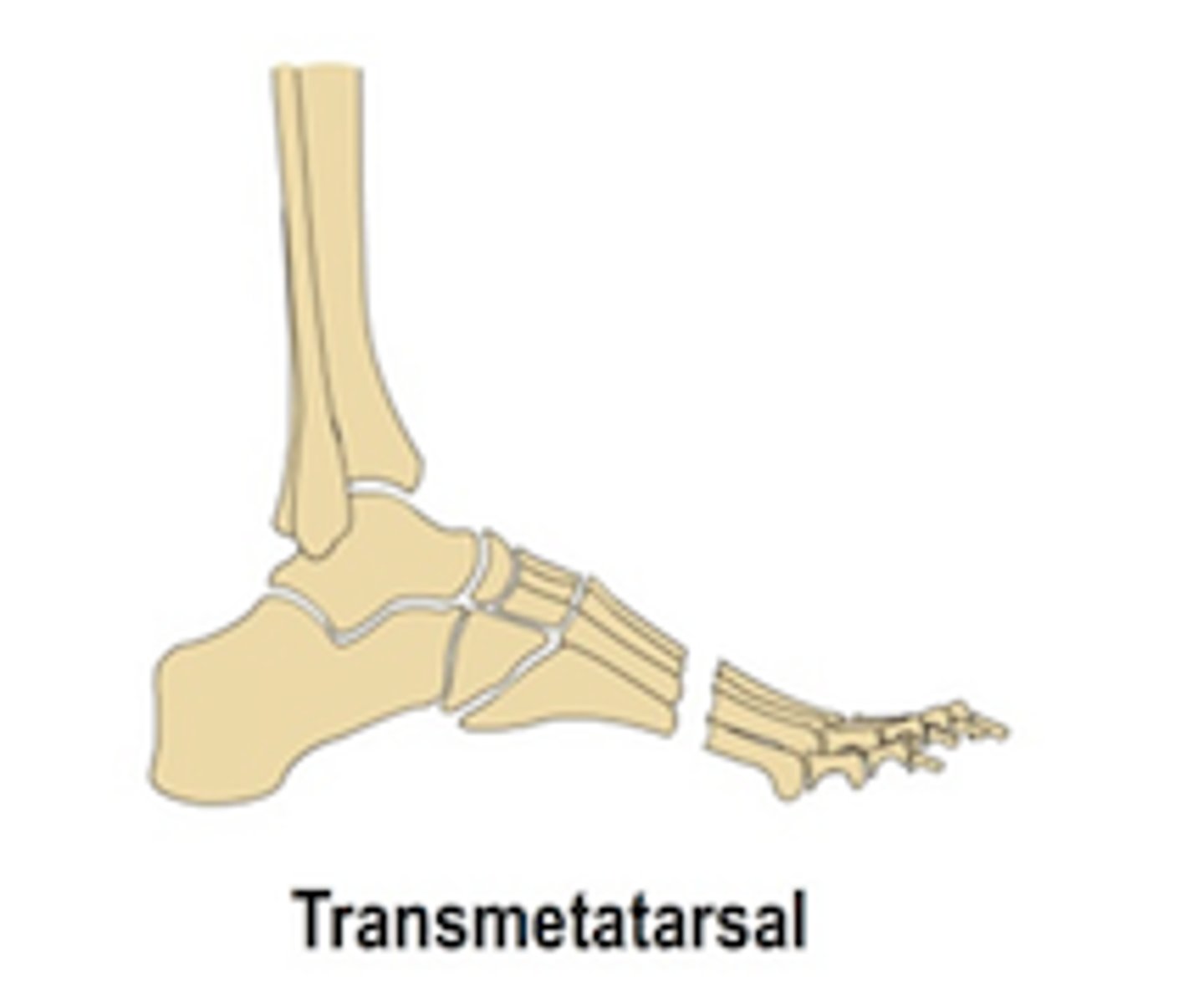
This partial foot amputation is performed thru mid-proximal metatarsal shaft
Transmetatarsal
All partial foot amputations (chopart, lisfranc) keep the ___ in tact
CALCANEUS (+ ankle!)
Reasons for toe amputations? (2)
Dysvasculatiry or trauma (frostbite, gangrene, infection)
Considerations for partial foot, ray, and transphalageal amputations
-increase risk for soft tissue breakdown
-can WB
-risk for equinovarus
-gait loss from great toe lever
T/F: for partial foot and ray amputations, normal gait is attainable with proper shoes and inserts and prosthetics are often not even prescribed
TRUE
What Is the biggest interruption to gait with partial foot and ray amputations?
Big toe push off
With partial foot, ray, and transphalangeal amputations, there is a risk for the remaining foot to be drawn into ___
Equinovarus
For partial foot, ray, and transphalageal amputation, we would want cavus support for the (high/low) arch that often results
HIGH!!
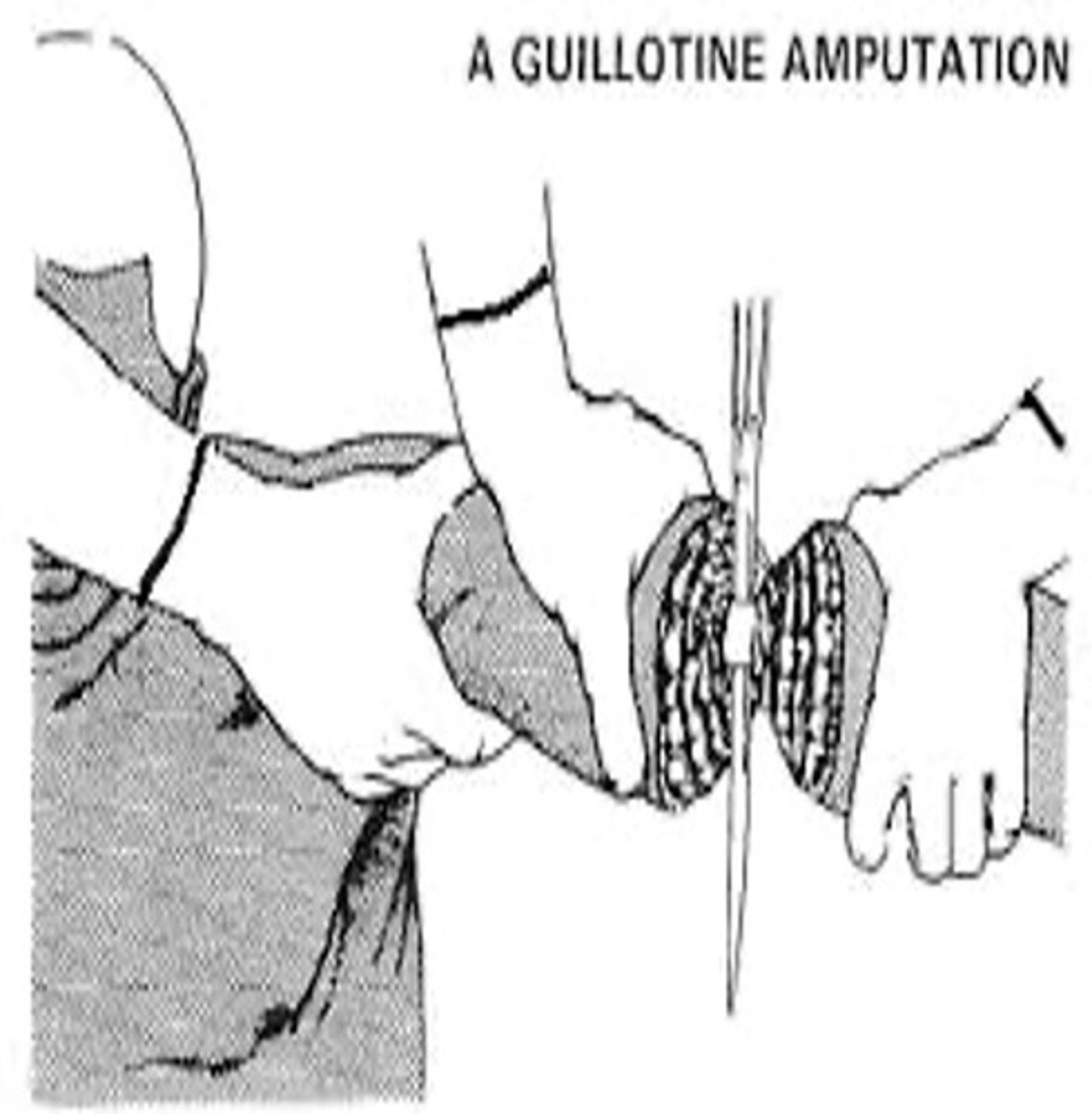
This surgical approach to amputation is just a straight cut through wherein all tissues are divided at the same level; indicated for an infection when all dead tisssue has not been removed; usually followed by a secondary procedure to revise
Guillotine (NOT COMMON)
This flap technique approach to amputation has equal skin flaps that is oriented so that incision is at distal end in either frontal or sagittal plane
Fish mouth
This flap technique approach to amputation has unequal skin flaps that is oriented so that incision is at distal end in either frontal or sagittal plane
Flap amputation
In a transfemoral amputation with a fish mouth technique, the __ flap would be a little longer than __
MEDIAL / LATERAL
In a transtibial amputation with a flap amputation, the long ___ flap is the preferred approach
POSTERIOR
What nerve would be located, cut, and retracted for TT and TF amputation operations?
Sciatic
For trans-tibial it is very important to ___ the edge of the bone
BEVEL (rounding & softening)
Soft tissue management that involves anchoring of muscle to bone
myodesis
Soft tissue management wherein a muscles are looped around end and sewn to each other; Muscle sutured to the deep fascia of the opposing group of muscles over the end of the bone
Myoplasty
Soft tissue management that involves Attaching tendon to bone
Tenodysis
This surgical technique involves an internal prosthetic implant ("abutment") protrudes through soft tissue and skin to external components (bone anchored prosthesis); option when traditional socket is NOT tolerated
Osseointegration (OI)
This procedure is a modification of a transtibial wherein the fibula is cut to same length as the tibia and bone (or metal) and a bridge is placed to allow distal end WBing; little evidence to support benefit
ERTL procedure (Still need a prosthetic but helps create a little more structure)

The ERTL procedure is good for patients who have potential to be highly (active/inactive)
ACTIVE!!
Overall goal for surgical considerations
Preserve as much length/viable tissue as possible
Considerations for surgical approaches
-lever arm
-surface area for forces
-proprioceptive feedback
-phantom pain + sensation
-energy requirements for ambulation
-vascular sufficiency
-skin integrity
-muscle stabilization