Functional Neurologic Disorder (FND)
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
FND is a group of neurological disorders caused by ___________ in the brain
Abnormal function/ signaling...how the brain and body sends and/or receives signals (i.e., NOT due to structural damage in the nervous system)
What are two analogies you could use to describe FND to your patient?
Computer analogy: "Software" problem vs. a hardware problem
Piano analogy: "Out of tune" vs. broken
FND is associated w/ ___________ levels of physical disability and distress
HIGH!!
Cause: FND
UNKNOWN!!
FND is NOT:
- a diagnosis of ___________
- a wastebasket diagnosis
- a purely ___________ condition or one that is only present w/ a ___________ comorbidity
EXCLUSION, PSYCHOSOMATIC, PSYCHIATRIC
How do we know that patients with FND are NOT malingering/ faking/ feigning symptoms?
Abnormal functioning can be demonstrated using fMRI
- hypoactivation of cortical and subcortical motor area
- accentuated limbic activity
- dysfunction in sensorimotor integration --> right parietotemporal junction (perceptual processing)
- abnormal motor planning --> supplementary motor area and prefrontal area
- other areas implicated: insula, cerebellar vermis
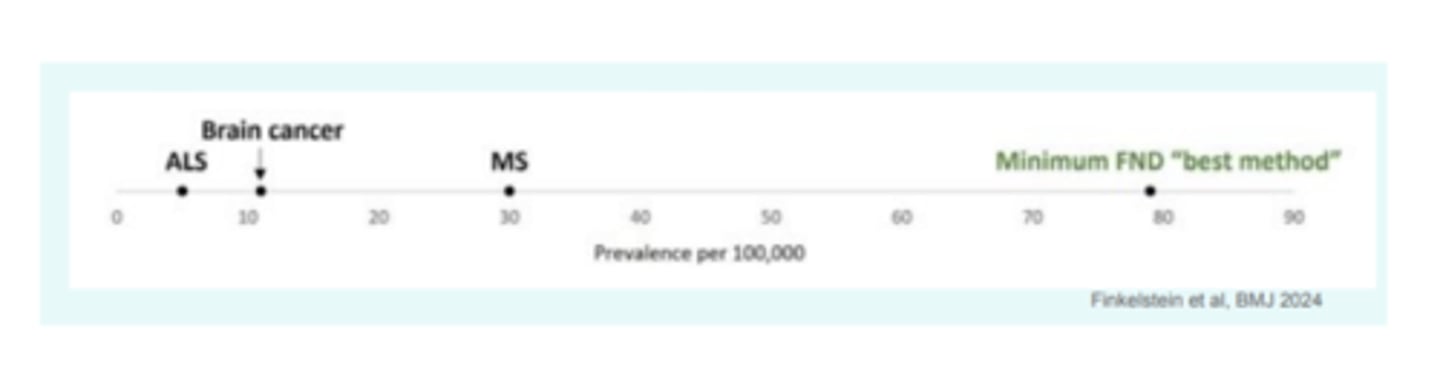
FND is the ___________ most common neurologic diagnosis in neuro clinics
2nd (HA/migraine is first)
Which disorders fall underneath the FND umbrella?
1. Functional Movement Disorder (FMD) = tremor, gait, limb weakness/ paralysis, dystonia
2. Functional seizures
3. Functional cognitive disorders
What are other conditions that share similar "software" problems related to maladaptive neuroplasticity?
Chronic pain/CRPS, persistent postural perceptual dizziness (PPPD), persistent post-concussion syndrome (PPCS), fibromyalgia, IBS
___________: involuntary but learned habitual movement pattern driven by abnormal self-directed attention due to a complex combination of physical + psychological + social influences on brain function
Functional movement disorders (FMD)
What may trigger FMD?
Physical or psychophysiological events such as injury, illness, pain, stress, and is mediated by illness beliefs and expectations
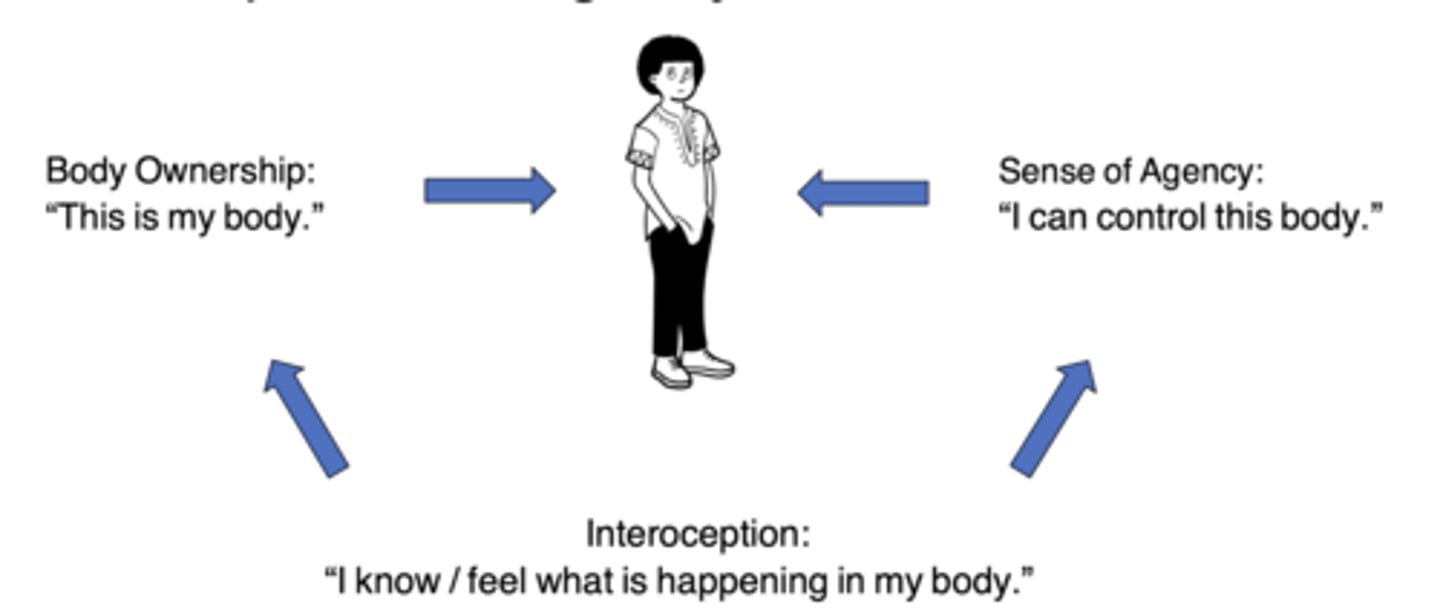
FMD is driven by impaired ___________ and ___________
Self-agency & attention
Explain the difference b/w normal and impaired self-agency.
Normal = "I am in control of my actions" (comparison of sensory feedback received from movement with what was predicted) vs. impaired = "I do not have conscious control over my abnormal movements despite evidence that normal movement can occur" (sensory feedback may be "smudged" or inaccurate)
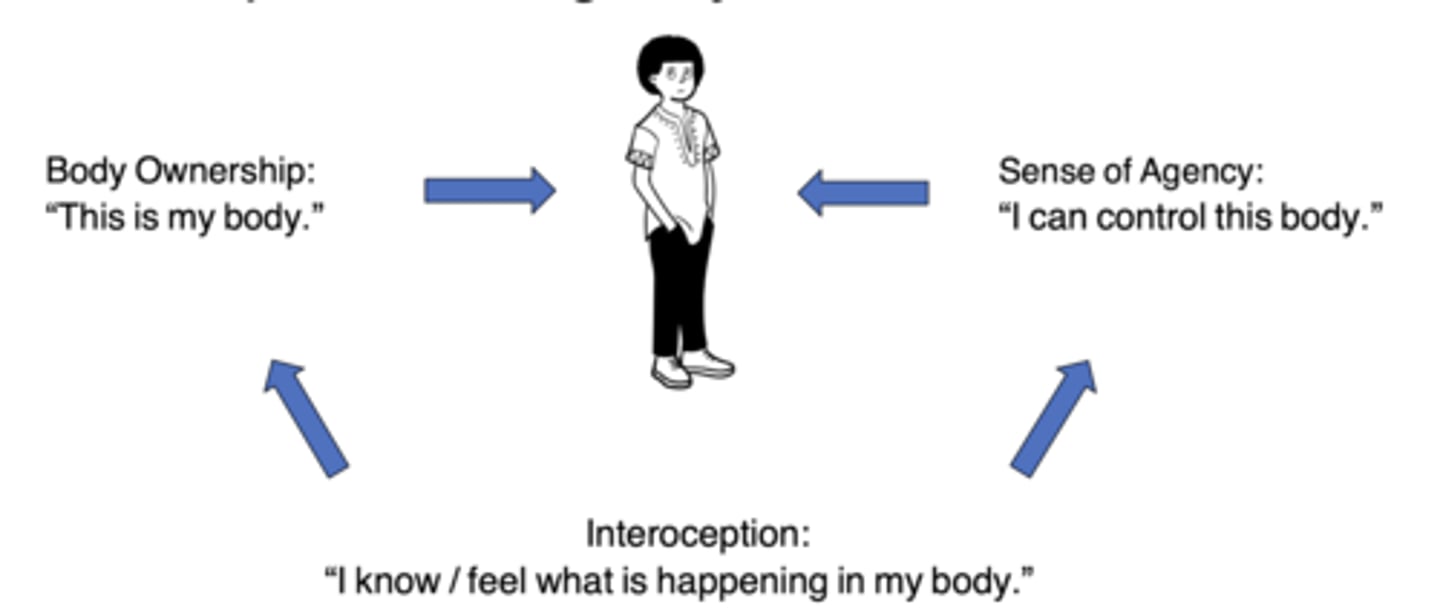
What might occur alongside impaired self-agency?
Impaired interoception (ability to sense and interpret body's own internal signals)...i.e., hunger, thirst, full bladder, anxiety, fatigue
___________: over-___________ to the symptoms/ hypervigilance --> exacerbation of abnormal movements
Attention
What are some subjective clues you may hear from patients w/ FMD?
"My body feels disconnected" "It is like my leg just isn't there" "My leg collapses or gets stuck" "My leg feels like a piece of chalk"
Predisposing factors: FND
Other neuro conditions (ex: PD), chronic pain, fatigue, or stress, recent or childhood trauma or life stress
True or false: all cases of FND are linked to mood/anxiety and symptoms
FALSE!!--not all!!
Proposed mechanism: FND
Initial event (or accumulation of predisposing factors/ triggers) + negative neuroplasticity factors (comorbidities, lifestyle factors, psychosocial factors, environmental barriers) + positive neuroplasticity factors (no comorbid health factors + fitness, brain health, diet, sleep, sense of safety, confidence/ self-efficacy, support, validation) --> adaptation vs. maladaptation to injury or event (10-20% develop chronic manifestations like FNDs, chronic pain, or PPPD)
How do the s/s of FND differ in children vs. adults?
Children = seizures, sensory loss, motor symptoms
Adults = tremor, gait disorder, dystonia, weakness, paralysis
What are characteristics of functional signs?
Variable/ inconsistencies, changes w/ attention vs. distraction, exacerbations & remissions, suppressible, sudden onset, entrainable (tremor), sensory loss in a pattern that is inconsistent w/ known causes (i.e., "split down the middle")
As an example of functional vs. NON-functional signs, explain the difference b/w a Parkinson's Tremor and Functional Tremor
PD tremor = low-freq. (3-7 Hz) w/ pill rolling pronation/ supination
Functional tremor = variable speed and amplitude, entrainable, sudden onset w/ relapses and remissions, improves w/ automatic movement
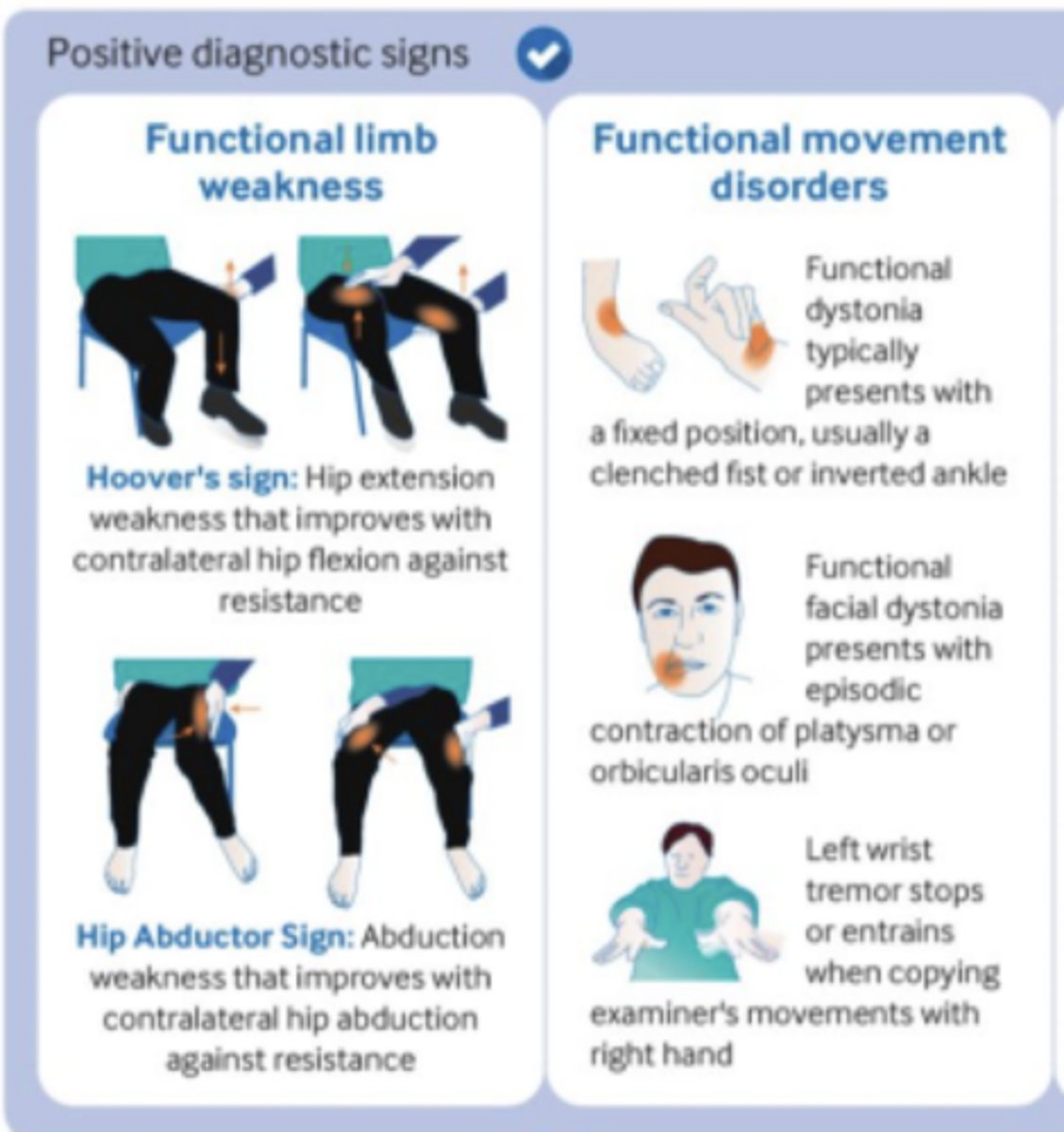
___________ (rule-in sign): hip extension weakness that improves w/ contralateral hip flexion against resistance
Hoover's sign (tests functional limb WEAKNESS)
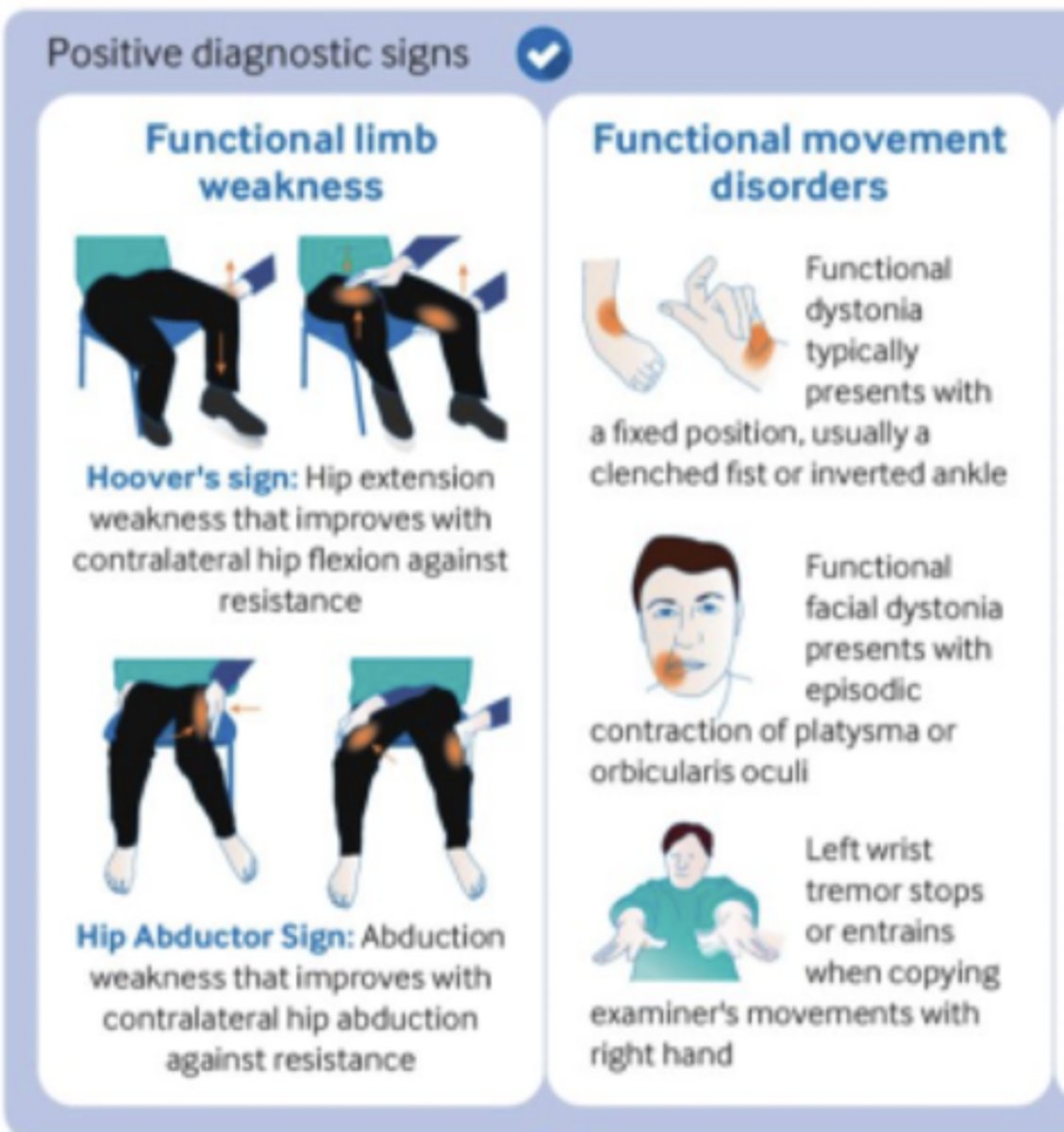
___________ (rule-in sign): abduction weakness that improves w/ contralateral hip abduction against resistance
Hip abductor sign (tests functional limb WEAKNESS)
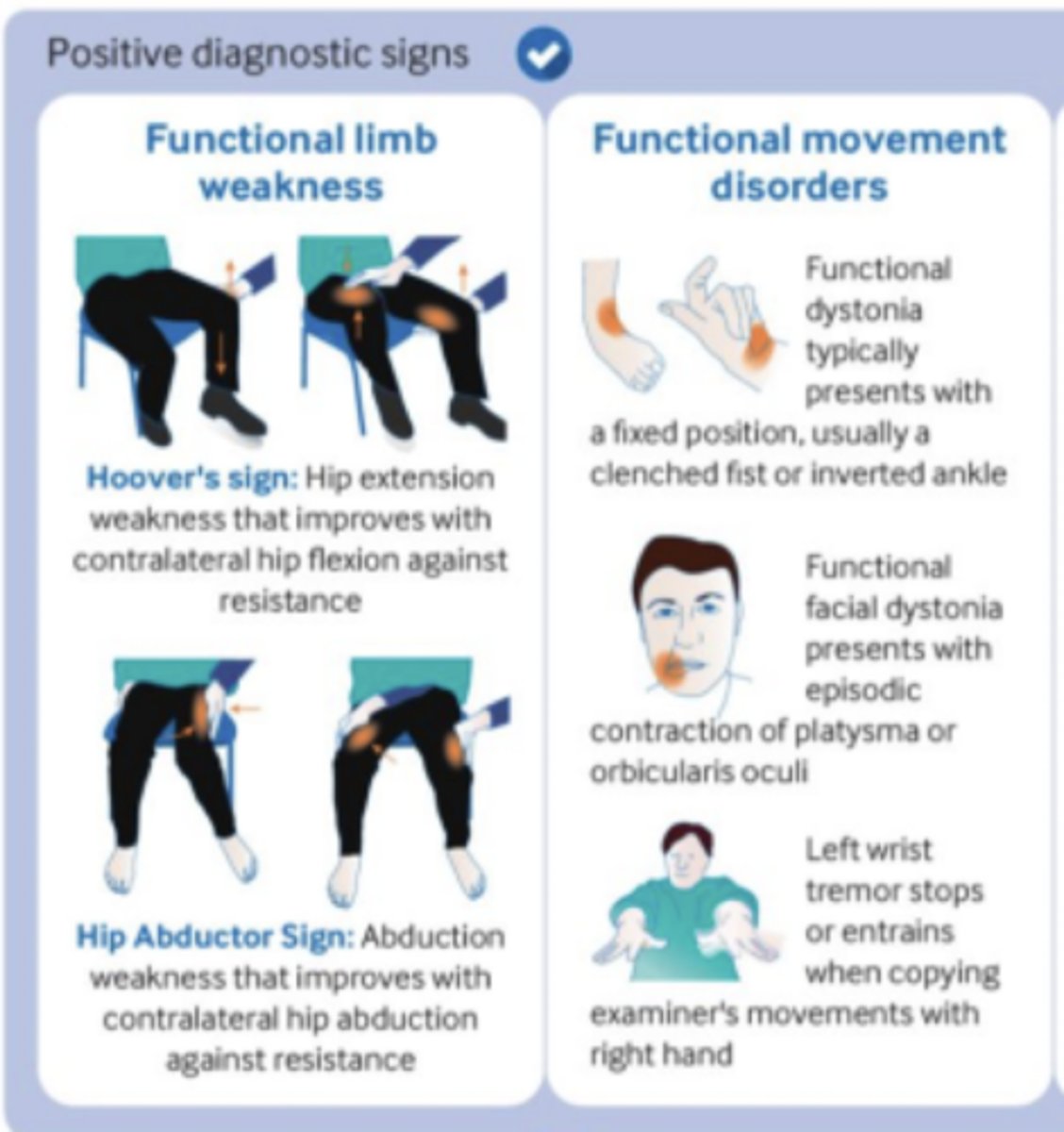
How would functional movement disorders present...functional dystonia?
Fixed position, usually w/ a clenched fist or inverted ankle
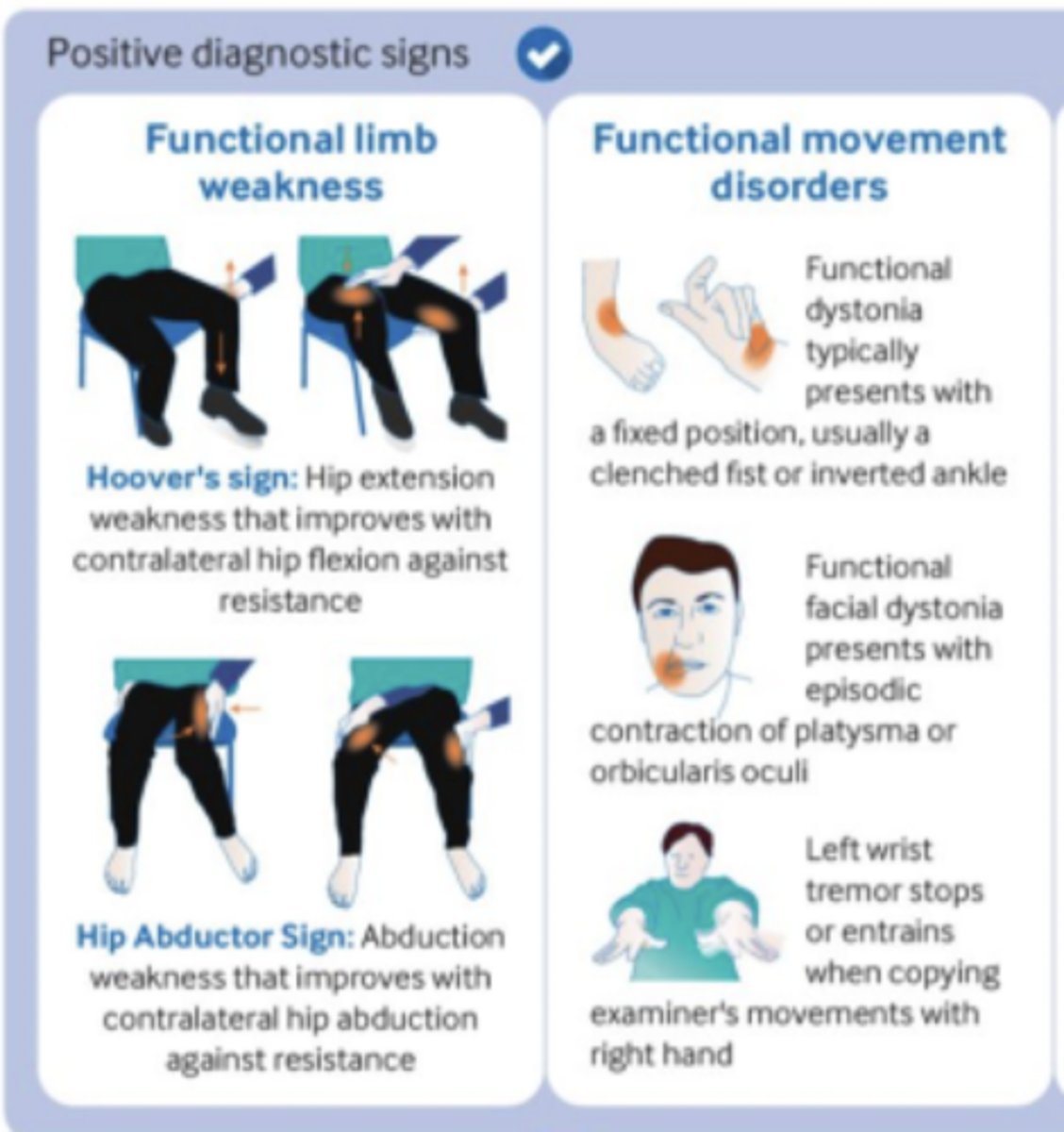
How would functional movement disorders present...functional facial dystonia?
Episodic contraction of PLATYSMA or orbicularis oculi
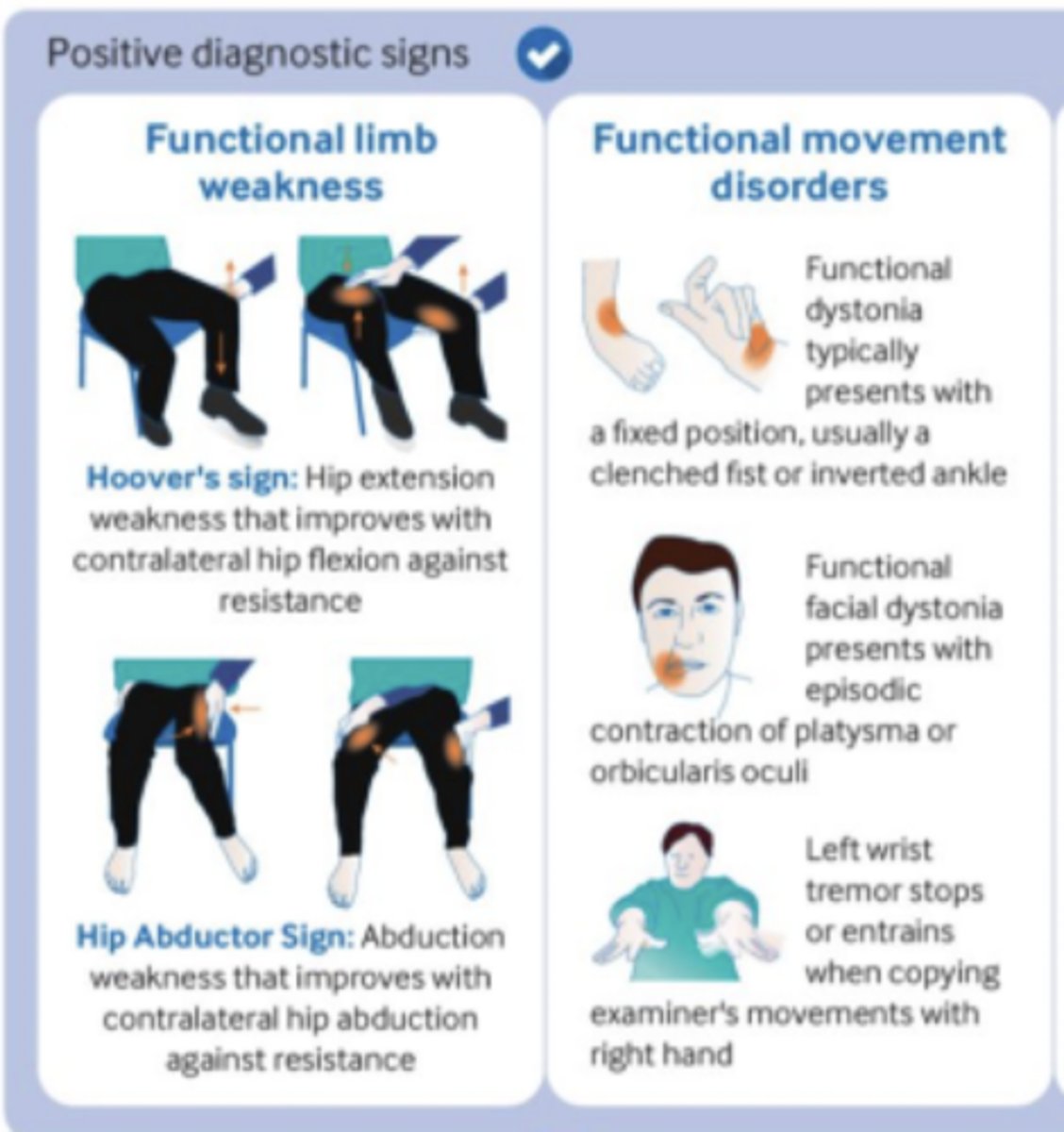
How would functional movement disorders present...tremor?
Left wrist tremor stops or entrains when copying examiner's movements w/ right hand
How should functional or dissociative seizures be diagnosed?
On the basis of finding characteristic features in the subjective account + observed description of the attacks ("eyes tightly closed, tearfulness, >5 min, side to side head shaking, hyperventilating)
Diagnosis of FND is based on careful ___________ of s/s and ___________ --> "rule ___________" based on findings
history, positive physical signs, in
What are tests and measures for positive physical signs? (note: are sensitive to non-organic neuro s/s) (hint: 6x)
1. Hoover's test/sign
2. Hip abd sign
3. Giveway weakness
4. Drift w/o pronation
5. Non-anatomical pattern of sensory loss
6. Tremor entrainment
True or false: many people w/ FND will experience spontaneous resolution of s/s after reassurance/education about their diagnosis
TRUE!! (however, FND tends to be recurrent, separated by asymptomatic periods)
List good prognostic indicators.
Stable relationships/ work history, ability to develop trusting patient-doctor/ therapist relationship and express emotion w/o incapacitating anxiety/ depression
List poor prognostic indicators.
Delayed diagnosis/ longer duration of s/s (chronicity), co-existent personality disorder
The initial diagnosis of FND should come from a ___________....why?
Physician -- sets the stage that the treating health professional accepts that the patient has a genuine problem & starts the convo that their problem has the potential for reversibility
What encompasses the medical team? Rehab team?
Medical team = initial diagnosis and clear explanation of the condition, mediation to tx comorbidities, psychotherapy for some (CBT/ cognitive analytical therapy)
Rehab team = PT, OT, and/or ST depending on the nature of the s/s and functional limitations
Which 3x criteria are recommended to ensure a patient w/ FMD is suitable for therapy?
1. Unambiguous diagnosis of FND by physician/psychologist
2. Patient has some confidence in or openness to the diagnosis of FND (i.e., does NOT believe the diagnosis is wrong)
3. Patient desires improvement and can ID treatment goals
PT eval -- FMD: subjective hx
1. Gather details of symptom onset and progression (including any potential triggers)
2. Develop comprehensive list of s/s (variability, severity, freq., aggs vs. eases)
3. Social hx
4. 24-hour routine
5. Use of adaptive aids, equipment, and home modifications
6. Activity limitations and participation restrictions
7. Explore patient's understanding and beliefs about the diagnosis
8. Goals for PT
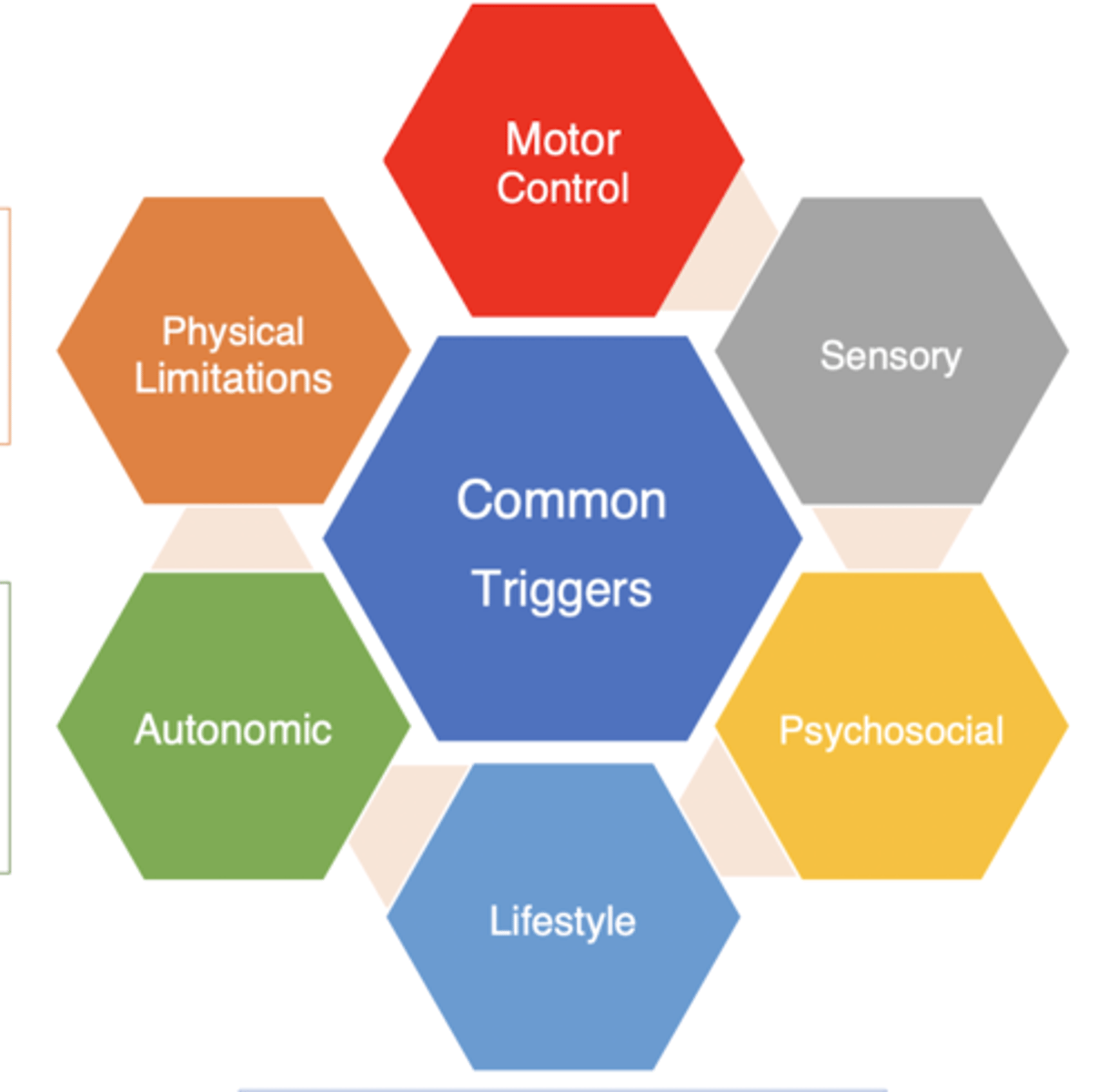
What are 6x buckets of common triggers for FMD?
1. Motor control (attention to body part/ symptom, change in environment, seeing abnormal movements in others)
2. Sensory (changing stimuli, too much vs. too little, specific stimuli, changes in temp, textures)
3. Psychosocial (ACEs, anxiety/ depression, trauma, stress, lack of control or autonomy)
4. Lifestyle (sleep, fatigue, stress, change in diet/routine, poor pacing)
5. Autonomic (fear, stress, exercise or exertion, change in position, change in vitals)
6. Physical limitations (physical injury, nerve tension, muscle tightness/soreness, pain)
PT eval -- FMD: objective exam rec.
1. Perform tests of positive physical signs (helps reinforce diagnosis as correct & demonstrate to patient that their body CAN move in a more typical way)
2. Emphasize activity/function more than individual impairments
3. Use outcome measures that have an emphasis on function -- numbers are "proof" of baseline and progress (also include EXTERNAL FOCUS)
4. Use caution in administering body-specific measures (may draw attention to the body part)
What are 6x buckets of importance for an FMD objective examination?
1. Motor control (ex: positive physical signs, movement analysis, response to external feedback/distraction)
2. Sensory (higher-order sensory testing, joint position error/ body awareness, vestibular, visual acuity)
3. Psychosocial (level of confidence w/ diagnosis, self-efficacy scale, GAD-7, PHQ, PCS)
4. Lifestyle (sleep hygiene index, insomnia severity index, daily routine/ schedule, perceived stress scale)
5. Autonomic (vitals, response to breath)
6. Physical limitations
Which 4x outcome measures encompass the "Physical Limitations" section?
1. PSFS
2. Core outcome measures
3. Agility tests/ dual-task tests
4. 9-hole peg test
Is there an optimum plan of care for patients w/ FMD?
NO!! (various models have shown effectiveness including "standard" OP 1-3x/week for 6-12 sessions; outpatient intensive; inpatient rehab intensive)
___________: component of the plan of care that outlines the exact plan for number, length, and freq. of sessions and clearly outlines the cancellation/ no-show policy
Treamtent contract
Why are tapered schedules beneficial?
Helps promote self-mgmt. b/w sessions and future ability to manage w/o PT if they have a relapse
When educating an individual w/ FMD, use the term ___________ vs. outdated terms and acknowledge s/s are REAL!!
FUNCTIONAL
When educating an individual w/ FMD, reinforce that s/s can ___________
Get better/be reversed BUT there is likelihood that there will be some ups and downs along the way
When educating an individual w/ FMD, explain how FND is diagnosed using ___________
Positive signs, which show that the nervous system is still capable of performing normal movement
When educating an individual w/ FMD, educate on the role of PT to ___________
"Retrain" the nervous system to help regain control over movement
When educating an individual w/ FMD, focus on factors that MAY be ___________
More in their control (i.e., "I can't control my movement" but "I can control my hydration...or sleep")
How do we address lifestyle factors/ triggers?
Pacing, diet, sleep, stress, mindfulness, purposeful activities
How do we address autonomic factors?
HR variability -- as biofeedback, breathwork, water and diet
General PT tx principles in FMD: build ___________ before challenging/pushing too hard --> graded exposure & project confidence that you have an understanding about FMD
Trust
General PT tx principles in FMD: create expectation of ___________
Improvement
General PT tx principles in FMD: maintain ___________ and ___________ communication b/w interdisciplinary team, patient, and family/caregivers
Open & consistent
General PT tx principles in FMD: limit ___________ treatment
"Hands-on" -- facilitate vs. support (even though their movement is unsteady, patients often will not "let themselves" fall or have "controlled fall")
General PT tx principles in FMD: encourage early ___________
WB (standing/gait)
General PT tx principles in FMD: foster ___________ and ___________ --> promote autonomy/ self-agency
Independence & self-mgmt.
General PT tx principles in FMD: focus on ___________ & ___________ vs. ___________
Function, automatic, impairments
General PT tx principles in FMD: minimize reinforcement of ___________
Maladaptive movement patterns and postures
General PT tx principles in FMD: avoid use of ___________
Splints and devices that immobilize joints
General PT tx principles in FMD: use ___________, IF necessary to maintain safety...but do NOT automatically prescribe devices
Adaptive equipment and mobility aids
General PT tx principles in FMD: recognize & challenge ___________
Unhelpful thoughts and behaviors
General PT tx principles in FMD: develop a ___________ & ___________ plan
Self-mgmt & relapse prevention
What are some FMD interventions? 1. Retrain movement w/___________________ (i.e., dual tasks, obstacle courses)
2. Emphasis on _________________________-- targets, auditory cues/ music, fast speed, automatic movements (do NOT use internal cues like "take a bigger step")
3. ________________(stationary bike, treadmill)
4. Visualization, mirror feedback, and ______________
5. ________________ to increase "sensory" cue and demonstrate that muscle is capable of movement
6. Other "sensory ___________" techniques (i.e., weighted vests, theraband straps/ body braid, "heavy work" w/ pushing/pulling, taping)
1. diverted attention
2. EXTERNAL focus
3. Non-specific graded exercise
4. video recording
5. FES, E-stim, TENS
6. Weighting
What are some FMD interventions to AVOID!!
1. Deceiving the patient through any form
2. Confining a person to a WC outside of PT
3. Surgery
Specific interventions: leg weakness (hint: 5x)
1. Early WB w/ progressively less UE support
2. Lateral weight shifting
3. Crawling in quadruped --> tall kneeling
4. Increased walking speed, may use harness/mirror
5. Backward walking
Specific interventions: UE weakness (hint: 3x)
1. Closed chain/ WB through arms
2. Use "weak" arm to functionally stabilize objects during task
3. Stimulate automatic UE postural responses by sitting on unstable surface w/ UEs resting on support surface
Specific interventions: gait (hint: 6x)
1. Change to a different speed (often faster)
2. Slide feet along floor like XX skiing
3. Walk while carrying objects/weighted vest for increased sensory input
4. Walk to metronome or music
5. Exaggerated movements (i.e., walking w/ high steps)
6. Stair negotiation
Specific interventions: tremors (hint: 2x)
1. Perform a competing movement (i.e., clapping)
2. Focus on movements of the other side of the body or bilateral, simultaneous movements