Biological Aspects of Dementia
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
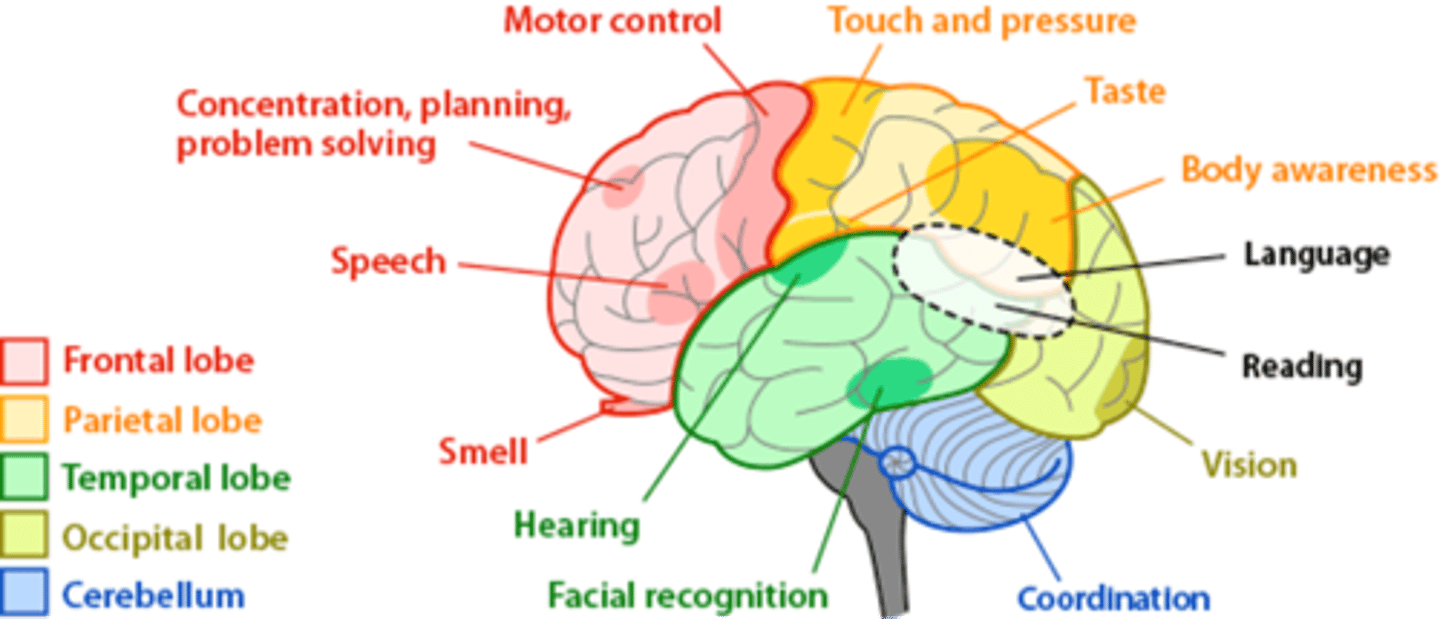
Which lobes of the brain do different dementia types correlate with? (4)
- Cerebellum is involved in most neurodegenerative processes.
- Lewy body dementia starts in brainstem and occipital lobe (so hallucinations first).
- Frontotemporal dementia involves frontal and temporal lobes (so personality changes first).
- AD starts in temporal lobes (so memory and language issues first).
Definition of Dementia -8
Based on ICD-10 criteria
Minimum six-month duration
Multidomain cognitive impairment including memory decline
Must be memory and one else = dementia
Must be severe enough to affect daily activities
Consciousness remains intact (excludes delirium)
Requires ruling out reversible causes
No brain scan , only clinical and past history
can lead to many types
Types of Dementia - 8
Key ones= underlined
Alzheimer’s Disease (AD)
Vascular Dementia (due to cerebrovascular disease)
Dementia with Lewy Bodies (DLB)
Frontotemporal Dementia (FTD)
Parkinson’s Disease Dementia
HIV-associated Dementia
Huntington’s Disease Dementia
Dementia due to Prion Diseases
Explain the neuropathology of Alzheimer's disease. (4)
Amyloid plaques (extracellular deposits of β-amyloid)
Neurofibrillary tangles (NFTs) (intracellular aggregates of hyperphosphorylated tau)
β-amyloid pathology & tauopathy (like a brick cell wall , if hyperphosphorylated → collapses → cell wall destroyed )
Synaptic dysfunction and neuronal loss
Reactive gliosis & microgliosis (like macrophages of the brian = inflammatory response)
Neuropathological changes precede clinical symptoms by decades
Weak correlation between pathology and disease severity
Which brain region is often the last to develop amyloid plaques in AD?
The cerebellum, which is the last to be affected in most dementias.
Explain the histopathology of Alzheimer's disease. (2)
1. Neuritic plaques: Extracellular β-amyloid deposits and dystrophic neutrites, activated microglia.
2. Neurofibrillary tangles: Intracellular hyperphosphorylated tau which leads to weak tau binding on microtubules, causing cells to become fragile and break.
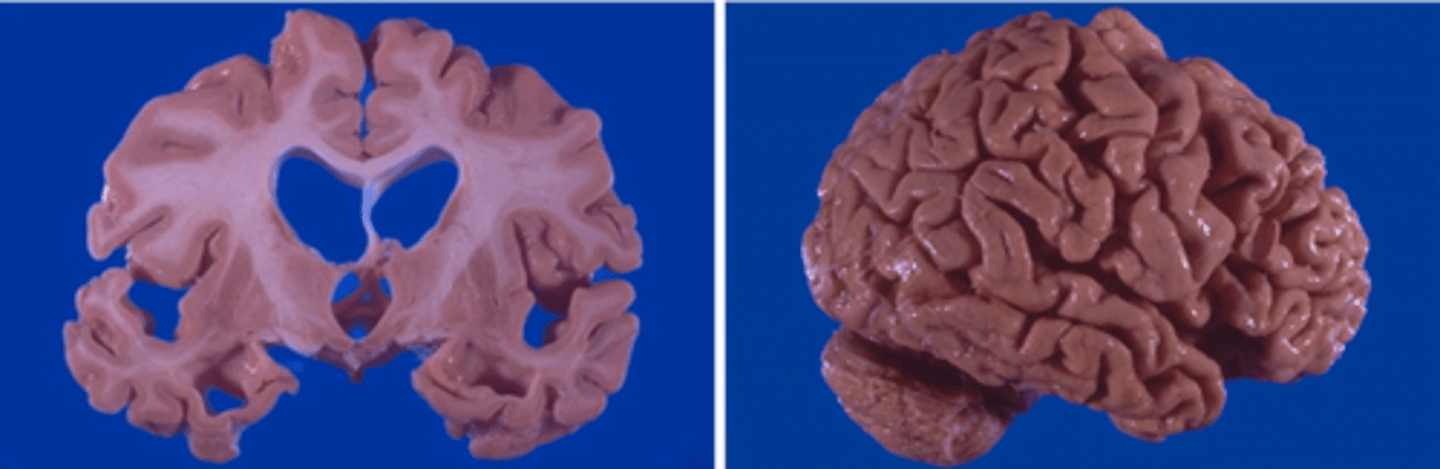
What are the structural brain changes in AD?
Atrophy in hippocampal region and enlarged ventricle sizes.
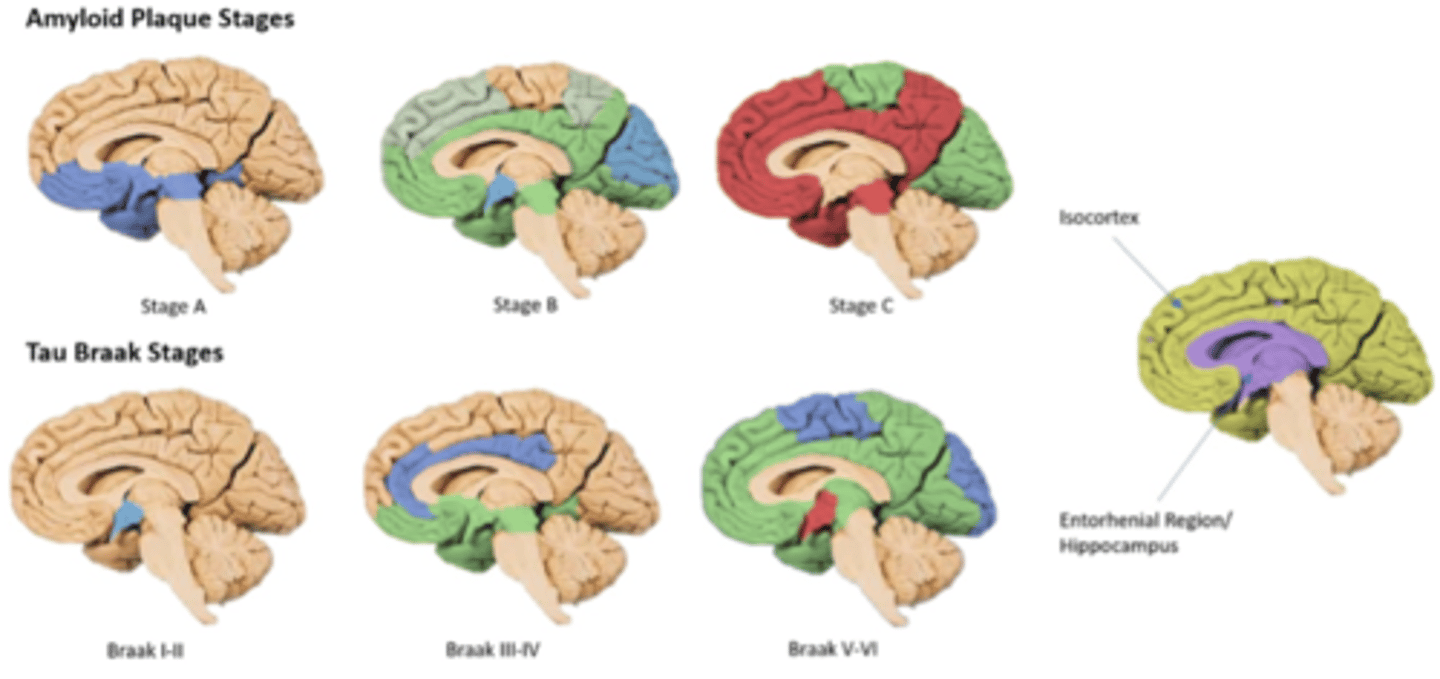
What is the neuropathological classification score of Alzheimer's? (3)
ABC score post-mortem to see severity of amyloid and tau pathology.
1. β-amyloid score - A1 starts in neocortex > A2 subcortical > A3 brainstem/cerebellum (last stage).
2. Neurofibrillary tangle (Tau) stage - B0 has no NFTs, B1 starts in transentorhinal cortex > B2 hippocampal > B3 neocortex (last stage).
3. Neuritic plaque score - C0 no plaque > C1 sparse > C2 moderate > C3 frequent.
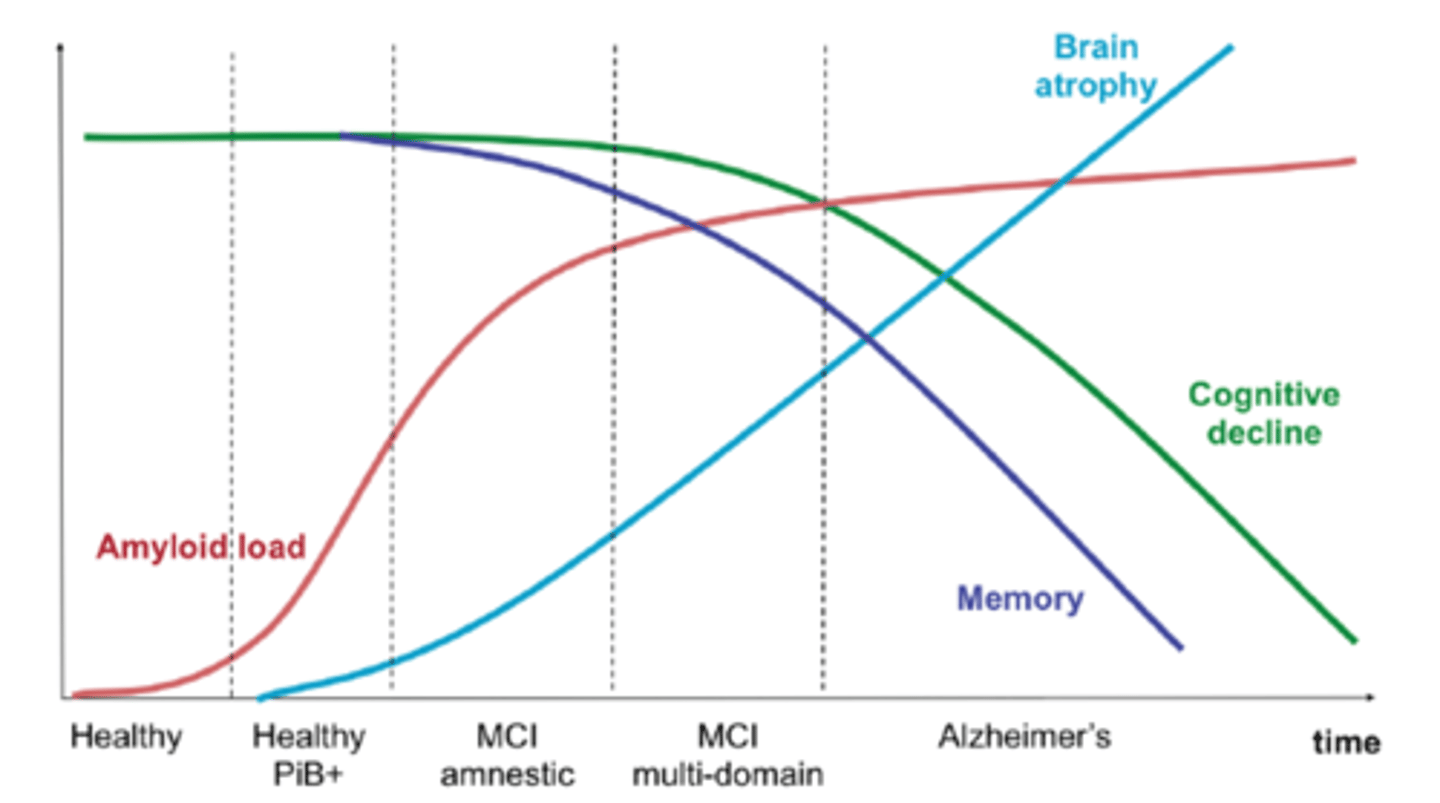
Show the evolution of AD pathology. (4)
Brain atrophy and amyloid load increase over time, memory decreases over time and cognitive decline occurs more rapidly during Alzheimer's.
1. Healthy amyloid load
2. MCI amnestic - more than 2 s.d. deficits i.e. executive function and memory but functioning independently
3. MCI multi-domain - increased amyloid levels; spread to other areas
4. Alzheimer's
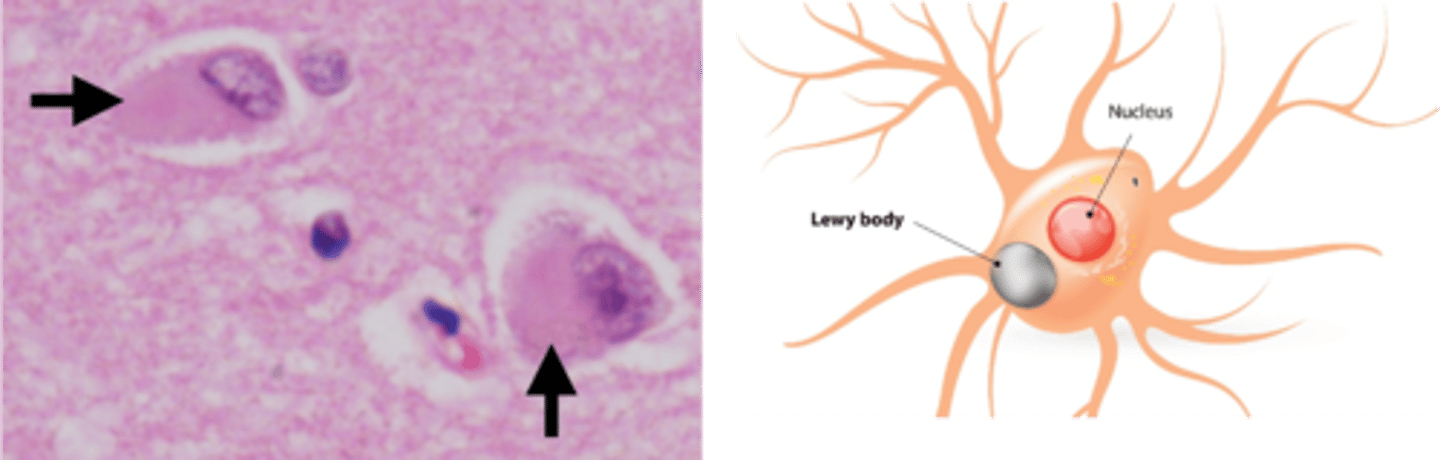
What are the features of dementia with Lewy bodies? (4)
1. Lewy bodies are eosinophilic spherical neuronal intracytoplasmic inclusions which develop inside neurons and form lewy neurites.
2. Numerous Lewy bodies occur in neocortex.
3. You have less frequent neocortical neurofibrillary tangles in DLB and varying amounts of β-amyloid plaques.
4. Faster progressing than Alzheimer's.
What are the subtypes of DLB? (4)
1. Brainstem predominant DLB - cognitive and sleep changes (ascending reticular formation) eg. muscle movements in sleep
2. Limbic DLB - emotion, comes from brainstem.
3. Neocortical or diffuse DLB - spread of dementia from brainstem
4. Cerebral DLB.
What is the clinical criteria for DLB
2 or more, o1 biomarker if there is only 1 from below
Recurrent, detailed visual hallucinations
REM sleep behaviour disorder
Spontaneous Parkinsonism
Fluctuating attention and alertness
What are the 3 molecular types of frontotemporal dementia?
Not one single disease - 3 molecular types:
FTLD-TAU (Tauopathy)
FTLD-TDP (TDP-43 pathology) = protein related, dysfunction causes DNA breaks
FTLD-FUS (Fused in Sarcoma protein) -protein misfolding
What are the 2 major clinical types of frontotemporal dementia?
1. Behavioural variant (90%) - frontal lobe is affected primarily; affects different parts
2. Primary progressive aphasia (10%) - temporal lobe; 3 types - semantic, non-fluent or logopenic.
What are the different neuroimaging techniques used in dementia and what are their 2 categories? (7)
Structural deficits:
1. CT
2. MRI
Functional - which areas have reduced blood and oxygen flow:
1. Functional MRI
2. Magnetic resonance spectroscopy (specific metabolites)
3. SPECT (differentiates between DLB and AD)
4. PET (radioactive glucose)
5. Diffusion tensor imaging
Does giving MAB (anti-amyloid monoclonal antibodies) reduce amyloid plaque?
Yes, but it does not change cognitive impairment.
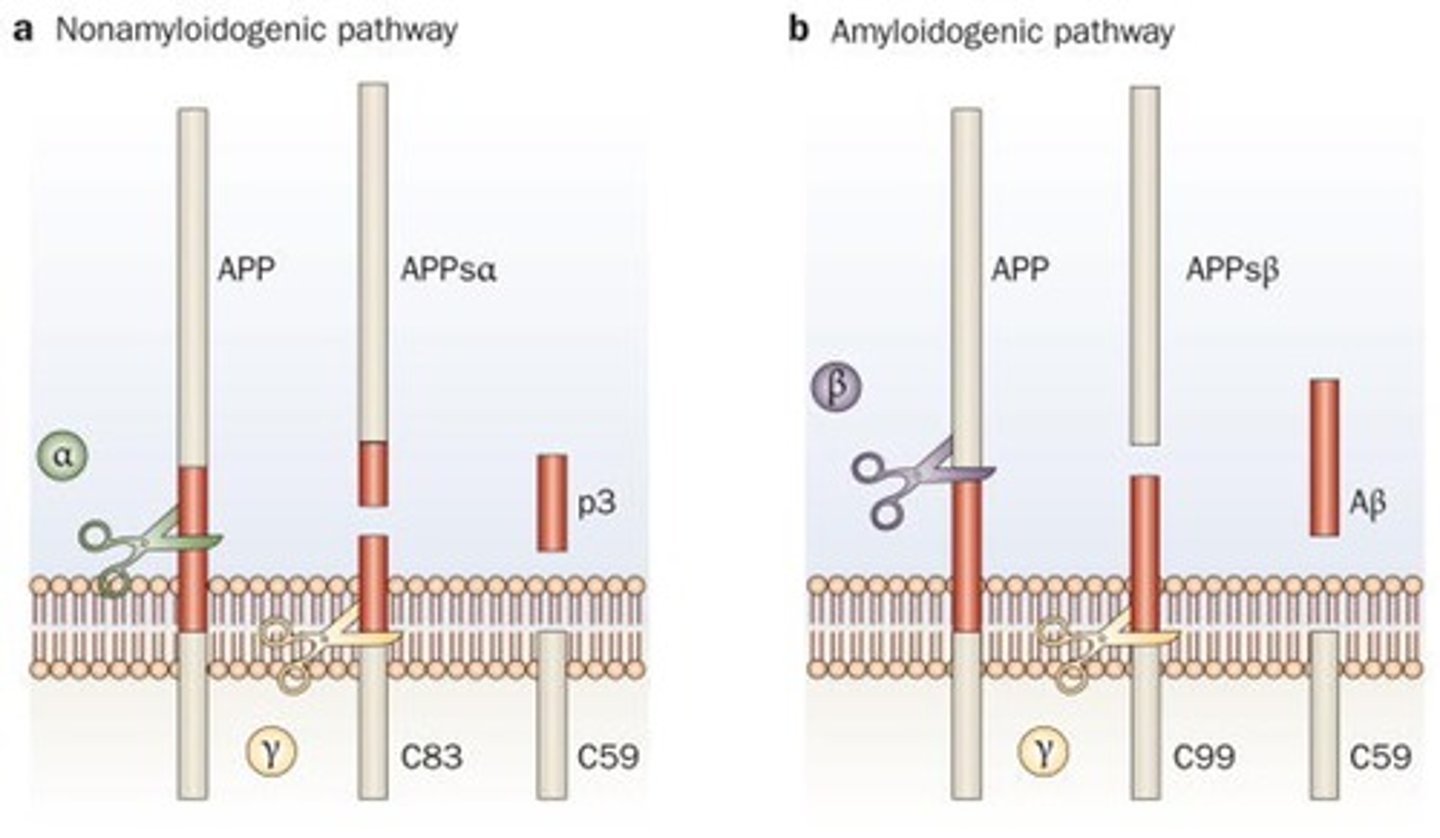
What is the precursor of amyloid and what processes this precursor?
APP - amyloid precursor protein.
Amyloid precursor protein (APP) is cleaved by β-secretase & γ-secretase.
Produces β-amyloid peptides (Aβ1-40, Aβ1-42)
Aβ1-42 is more prone to aggregation and forms plaques
Mutations in APP, PSEN1, PSEN2 increase Aβ1-42 production
List the physiological and pathological paths of APP processing.
Physiological (healthy): Nonamyloidogenic path, involving ⍺ and gamma secretases. - so the A has time to break B before t forms the plaque
Pathological (bad): Amyloidogenic path, involving β and gamma secretases. - b acts first for stays intact and forms the plaque
Outline normal and pathological APP processing. (4)
The amyloidogenic path is the pathological path.
Processed by ⍺, β and gamma secretases.
1. Normally, first cleaved by ⍺ secretase.
2. Then by gamma secretase, which makes the functional amyloid element.
Pathological:
3. But if more β secretases are expressed, then the same APP is cut into different sized fragments, one of which is amyloid-β (a product of β and gamma secretase interaction).
4. These aggregate together to form amyloid plaques - starts with monomers, then oligomers and eventually sedimentation of plaque.
People with Down's syndrome have a higher risk of AD. Which gene is most likely involved in this risk factor and why?
APP. This is because Down's syndrome is Trisomy 21, and APP is coded in Trisomy 21, so more amyloid-β generation can lead to early onset AD in those with Down's syndrome.
What are the 2 major forms of β amyloid peptides and which one is worse?
1. Aβ1-40 (40 aa long)
2. Aβ1-42.
Aβ1-42 aggregates faster, seeds plaques and is more neurotoxic.
What do most familial AD mutations increase levels of?
Aβ1-42 (which aggregates faster).
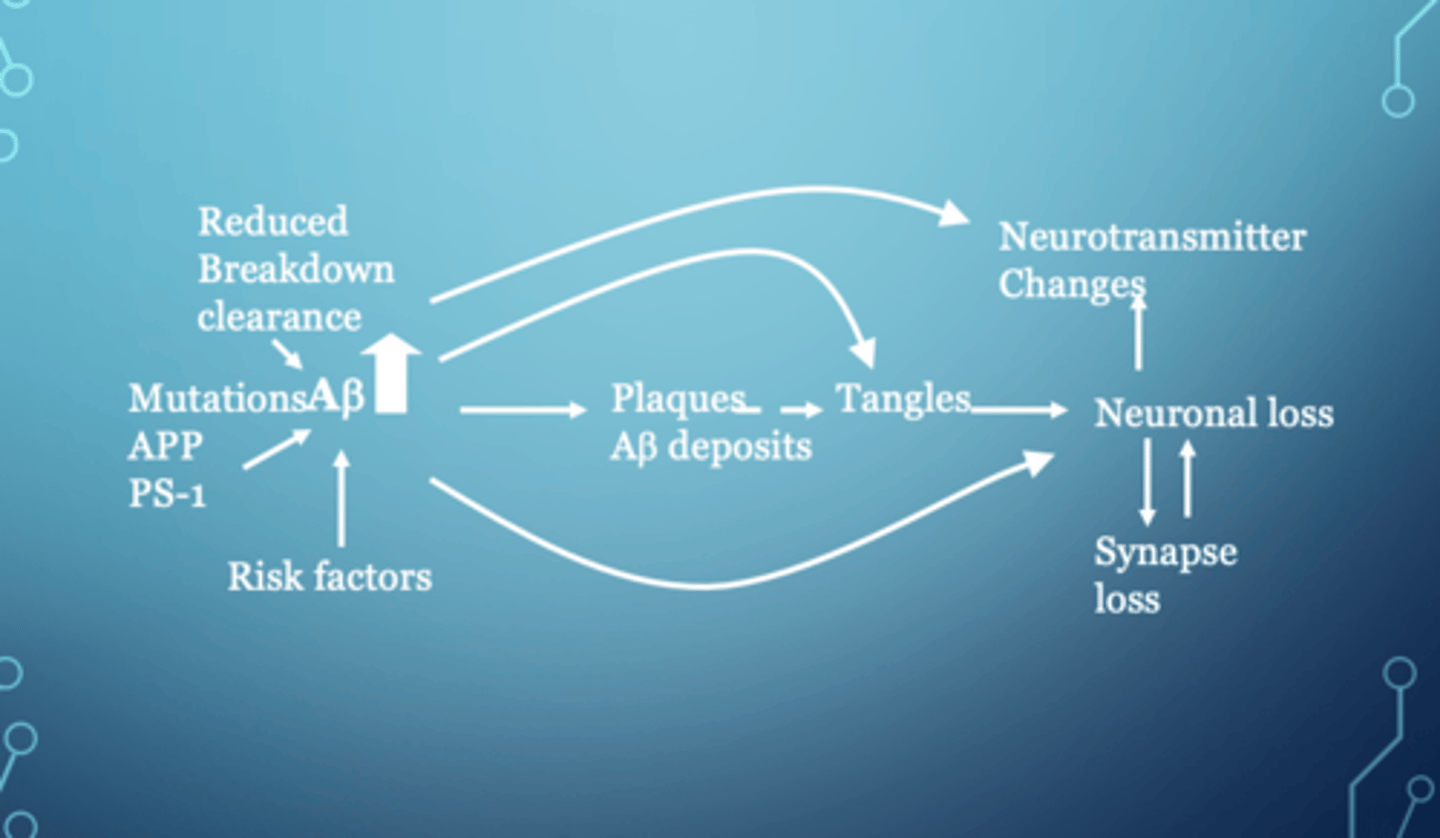
Explain the amyloid cascade hypothesis. (3)
1. Mutations increase production of amyloid-β i.e. failure of breakdown clearance or other risk factors like vascular impairment and socioeconomic factors.
2. Leads to formation of amyloid deposits.
3. Amyloid plaques increase neurofibrillary tangles and change ACh levels, causing neuronal loss and synaptic loss.
This explains why clearing the amyloid load doesn't fix the issue - there are other factors involved.
What is tau?
A low MW microtubule-associated protein coded by MAPT gene in chromosome 17.
Found mainly in axons and function to stabilise microtubules within cytoskeleton.
What happens to tau if it is phosphorylated?
Phosphorylation of tau means it binds microtubules less, leading to AD.
The insoluble, ubiquinated tau then forms filamentous inclusions in neuronal cell bodies, processes and glia and form neurofibrillary tangles.
Which type of tauopathy is involved in frontotemporal dementia?
Pick's disease.
What are the different types of tauopathies? (7)
1. AD
2. Pick's disease (frontotemporal dementia)
3. Parkinsonism
4. Progressive supranuclear palsy (PSP)
5. Corticobasal degeneration (CBD)
6. Postencephalitic parkinsonism
7. Niemann Pick's disease
What is synucleinopathy?
Key formation step of Lewy bodies (seen in DLB, PD and CBD) where ⍺-synuclein is aggregated to form neurotoxic oligomers. High extracellular amounts can transmit Lewy pathology.
Explain the neurobiology of Lewy body dementia. causes (6)
1. β-glucocerebrosidase 1 deficiency; impaired glycolipid processing in brain
2. Microglial dysfunction; makes brain vulnerable to infection + delirium, opposite to Alzheimer's which has a microglial overdrive.
3. Mitochondrial dysfunction; common to all dementia types
4. Autophagy lysosome path impairment
5. Ubiquitin protease impairment; accumulation of Lewy body formation
6. Oxidative stress
What are the 4 diagnostic criteria of DLB?
You need at least 2 present to make a DLB diagnosis.
1. Cognitive fluctuations
2. Spontaneous Parkinsonism
3. REM sleep behaviour disorder
4. Recurrent vivid visual hallucinations
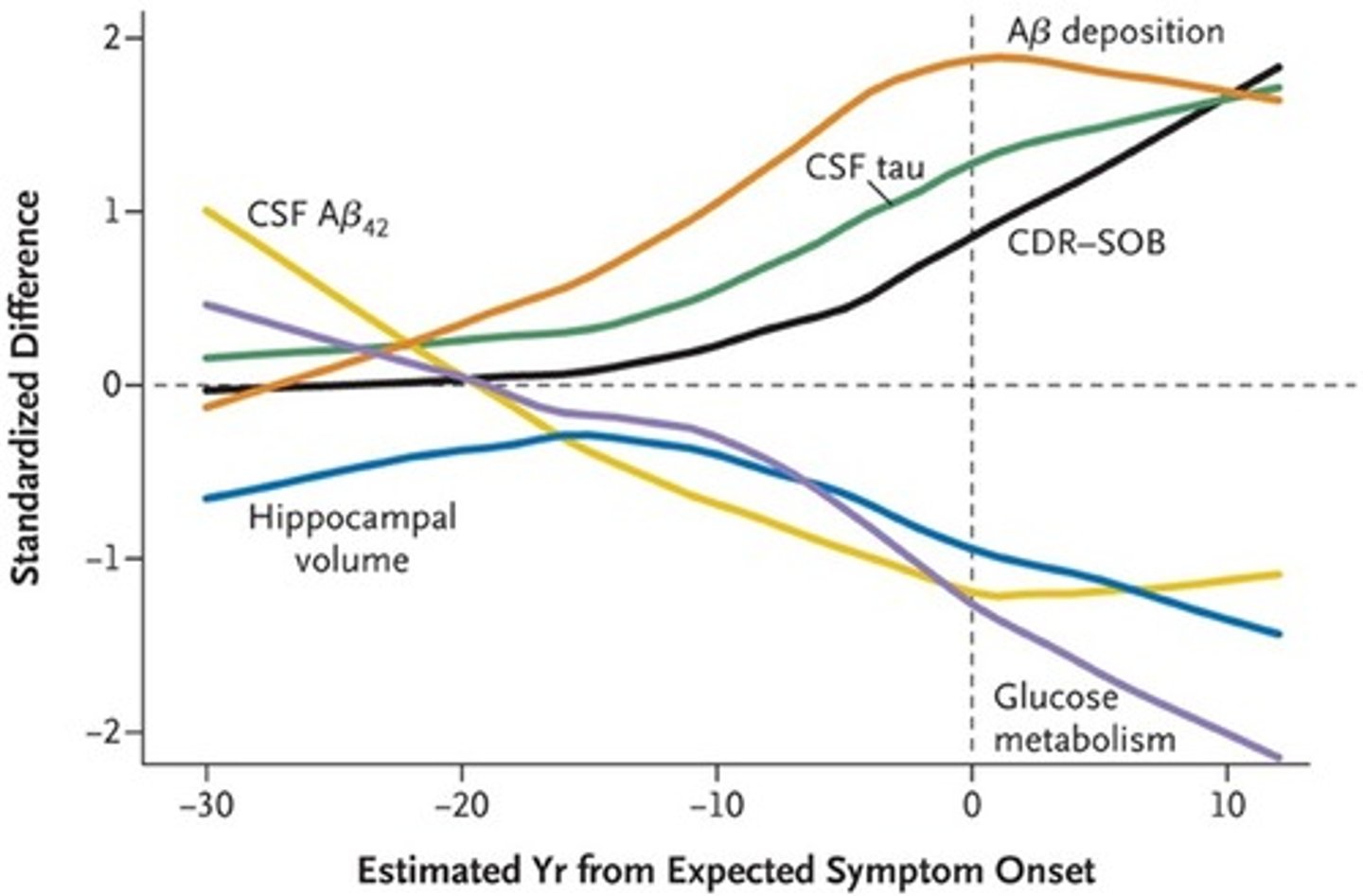
What are the biomarkers of AD? (2)
Useful in research setting to predict those with MCI who are more likely to develop dementia in the future.
1. Hippocampal vol is a poor indicator, which gradually drops over time.
2. Aβ-42 levels and tau levels can be checked in CSF.
CSF biomarkers: Increased tau, decreased Aβ42
PET imaging: Detects amyloid and tau pathology
List the different types of DLB biomarkers. (2)
Diagnosis cannot be based on biomarkers alone.
1. Indicative - diagnostic weight.
2. Supportive.
What are the indicative biomarkers of DLB? (3)
1. DaT scan - looks at reduced dopamine transport uptake in basal ganglia via PET/SPECT.
2. Myocardial scintigraphy - finds Lewy bodies in ANS.
3. Polysomnography of REM sleep with no atonia - only done in specialist sleep labs.
What are the supportive biomarkers of DLB? (3)
1. Preserved medial temporal lobe structures
2. Reduced occipital activity
3. Prominent posterior slow-wave (delta) activity with periodic fluctuations in pre-⍺/theta range.
Explain the genetic mutations and which dementias they are associated with. (7)
1. APOE4 - general dementia risk factor for all types, but more for AD.
2. APP, PSEN1, PSEN2 - associated with AD
3. MAPT - associated with tauopathy and thus AD and fronto-temporal dementia
4. TARDBP - associated with AD, frontotemporal and late dementia.
5. GBA, SNCA - associated with DLB.
6. NOTCH3 - vascular dementia
7. Extracellular vesicular miRNA - associated with sporadic? dementia? ;-;
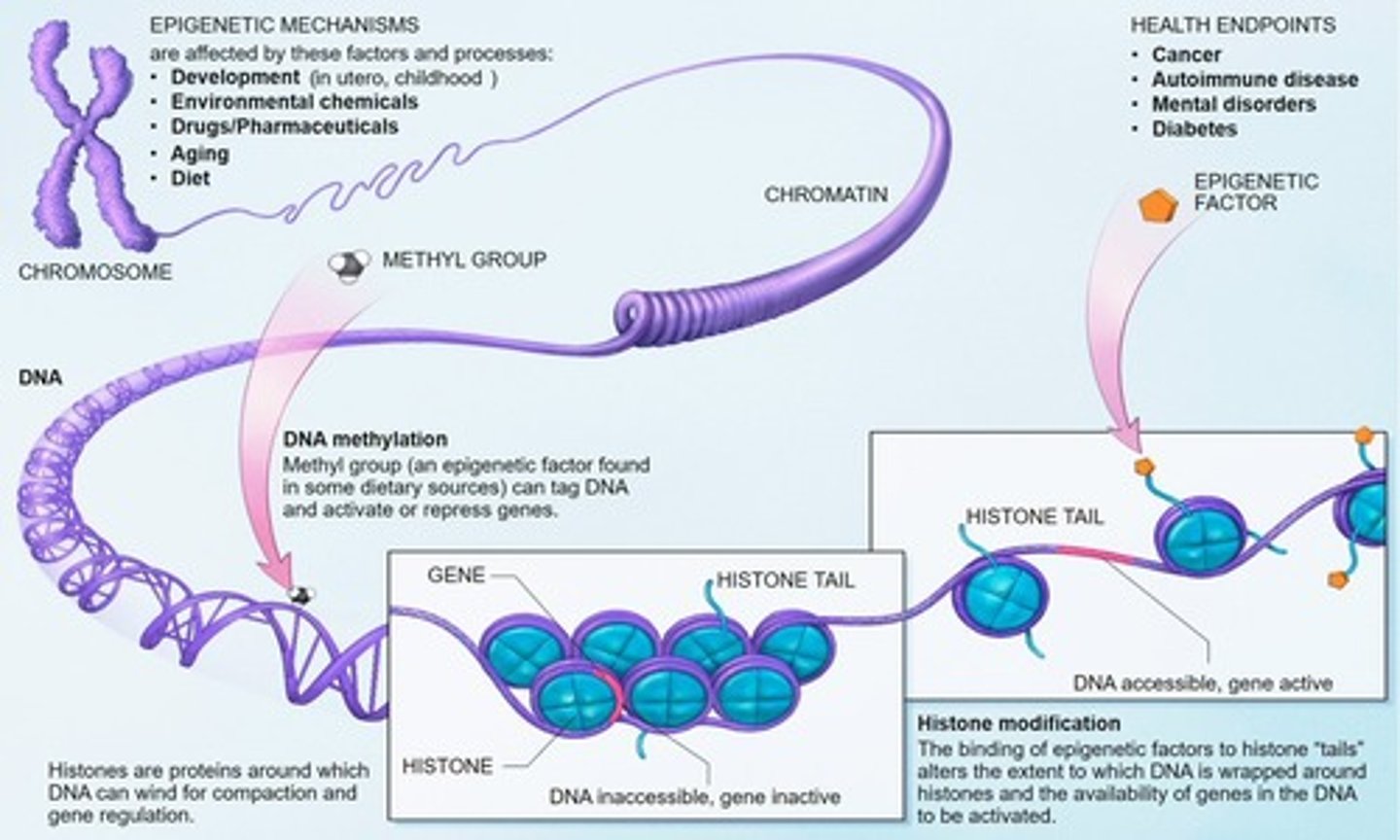
How does epigenetics play a role in dementia pathology? (4)
1. DNA methylation
2. Histone modification
3. miRNAs (influence gene expression)
4. siRNA (influence protein translation of RNA)
What are the genetic mutations associated with DLB? (4)
1. APOE
2. GBA
3. SNCA
4. MAPT
What is the significance of dementia's molecular biology? (4)
1. Understanding of molecular pathogenesis
2. Move towards biological classification
3. Find diagnostic + prognostic biomarkers that can help early diagnosis + 2º prevention
4. Identify novel drug targets.
D
m

E
X
C
X
E
X
D
X
A
X
B
X
C
D
X
C