UPDATED SESATS critical care
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
What are the specifics of the Mini-Cog?
The Mini-Cog test can be used as a tool to assess cognition.
Three unrelated words are spoken to the patient to remember. The patient is then asked to draw the face of a clock with the hands on a specific time. The patient is then instructed to recall the 3 words.
For each word recalled, 1 point is given. Drawing a normal clock gets 2 points, and an abnormal clock receives 0 points.
Mini-Cog scores range from 0 (worst score) to 5 (best score). A patient with a score ≤ 3 is considered to have cognitive impairment and additional testing is warranted.
Effects of glucose control (125-200 mg/dL) compared to glucose control target of <250 mg/dL.
- lower incidence of atrial fibrillation
- decreased episodes of recurrent ischemia
- fewer recurrent wound infections
*tighter control is better but elevated is ok during these times.
General guideline for chest tube output at 1, 2, and 4 hours warranting re-exploration.
>400mL/hour for 1 hour
>300mL/hour for 2 hours
>200 mL/hour for 4 hours
When to give preoperative glucocorticoids?
Patients receiving the equivalent of 20 mg or more of prednisone per day for more than 3 weeks.
Patients taking 5-20 mg of prednisone per day and those that have discontinued the use of steroids over the previous year should undergo preoperative evaluation of the HPA axis if possible or, alternatively, should have prophylactic perioperative administration of steroids.
Topical and inhaled glucocorticoids (such as fluticasone) also have the potential to suppress the HPA axis.
Indicators for successful weaning from vent for extubation.
RSBI: When the rapid shallow breathing index (RSBI) exceeds 105 breaths/(L*min) up to 95% of the attempts to discontinue mechanical ventilation will fail.
RR: 40 breaths/min or more being an indicator of increased work of breathing.
MIP: The strength of the diaphragm and respiratory muscles can be evaluated by having a patient exhale to a residual lung volume and then inhale as forcefully as possible. This pressure generated is called a maximum inspiratory pressure (MIP) or negative inspiratory force (NIF). When this value -30 cm H20 or less the likelihood of successful extubation is great; when it is greater than -20 cm H20, it implies poor reserve and a high likelihood of reintubation.
TV: tidal volumes >5 L/min or >6 mL/kg of ideal body weight.
Total ventilation: 5-6 L/min is normal for an adult patient, and if after a spontaneous breathing trial the total ventilation remains <10 L/min, a positive outcome is more likely.
Meds contraindicated in treatment for MG crisis
Atropine, an anticholinergic medication, may be used to support patients with cholinergic crisis (eg, pyridostigmine overdose), and is contraindicated in myasthenic crisis.
Pyridostigmine bromide (Mestinon), acetylcholinesterase inhibitor is usually ineffective during a crisis because the acetylcholinesterase is already maximally inhibited by ongoing (preoperative) use. Because it and other anticholinesterase inhibitors promote oral and bronchopulmonary secretions it is best to withhold them until the crisis is resolved.
HOCM patients that require ICD placement:
In high-risk patients, ICD placement is recommended.
High-risk patients include those with an
- extremely thick (>3 cm) interventricular septum
- evidence of non-sustained ventricular tachycardia
- a family history of sudden death
- a history of syncope.
Surgical septal myomectomy may reduce the risk of sudden death but it does not eliminate it.
How many calories per day
25 kcal/kg per day
How much protein per day
1.2-2.0 grams per kg
Correction rate for acute and chronic hypernatremia
Acute: 12 mmol/(Lxday)
Chronic: 8-10 mmol/ (Lxday)
*it is hyponatremia correction NOT hypernatremia correction that leads to osmotic demyelination syndrome.
Correction rate of hyponatremia
0.5 mEq/hr: no more that 8-10 mEq per day.
Using 3%Na
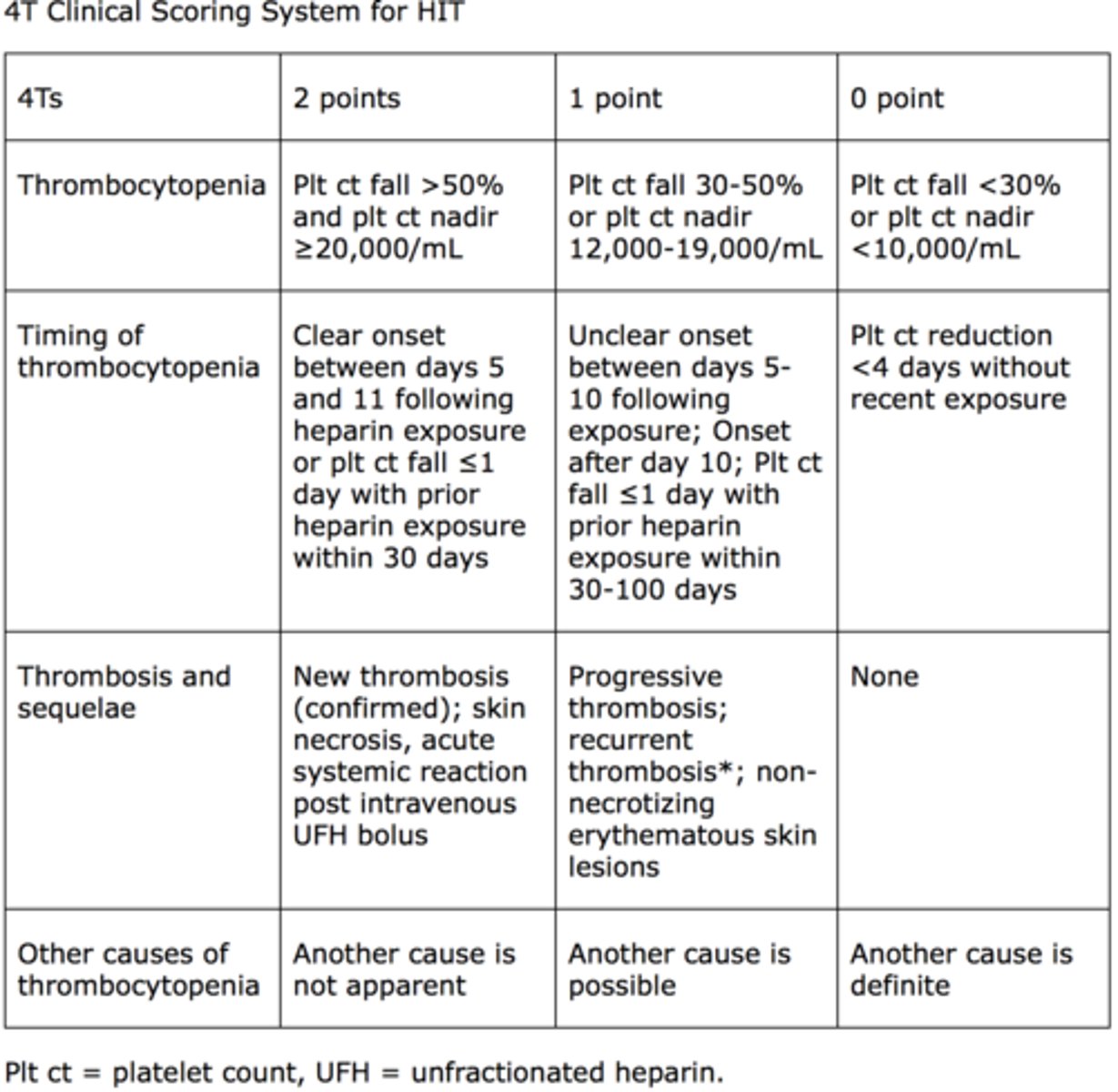
4T score for HIT
Independent predictive factors for MG crisis post-anesthesia
chances of MG crisis peri-op 12-18%.
- pyridostigmine 360 mg/day
- woman <55, 4:1 likelihood over men
- bulbar symptoms or chronic lung disease
- hx of previous crisis
- post-op pulmonary infection
When do you see Native Lung Hyperinflation
known complication with single lung transplant patients (most commonly done with COPD patient's).
can present acutely with hemodynamic instability and respiratory distress but more commonly presents progressively.
Treatment for native lung hyperinflation
Lung volume reduction surgery of hyperinflated native lung, can improve ventilation of the transplanted lung.
Must to bronchoscopy and transbronchial biopsy first to rule out acute or chronic rejection.
Adverse effect of IABP
thomocytopenia. Occurs in 47-82% of people. Max percent reduction from baseline platelet count usually 30-35%.
Severity of c-diff and treatment (mild/moderate vs severe)
generally oral option preferred when patient is functioning enterally.
Mild/moderate: metronidazole
Severe: vanc
When to use and how much of a dose of methylene blue?
used for treatment of methemoglobinemia. Acts by giving electron to NADPH methemoglobin reductase which converts methemoglobin to hemoglobin again.
1-2 mg/kg.
Adverse effect of certain topical anesthetics
conversion of hemoglobin to methhemoglobin
Treatment for cyanide poisoning
Ferrous state has more affinity for cyanide and can be used as a treatment option for cyanide poisoning by intentionally converting hemoglobin to methemoglobin which binds to cyanide and then is excreted from the body by treating with thiosulfate which binds to methemoglobin cyanide complex forming thiocyanate which is a complex that is excreted.
Nitrites and dapson can lead to ferrous state
TEVAR prevention of intraoperative spinal cord ischemia
Lumbar drain reduces risk of injury by 4-7% according to literature.
Not well validated but practiced, keeping hematocrit above 12 and maintaining elevated BP.
Strongest indicator for stress ulcer prophylaxis
mechanical ventilation 48 hours.
What are lung protective settings on a vent
low tidal volume (6 ml/kg) and plateau pressure <30.
With low tidal volume, minute ventilation and alveolar ventilation are lower which results in a tolerable mild hypercarbia.
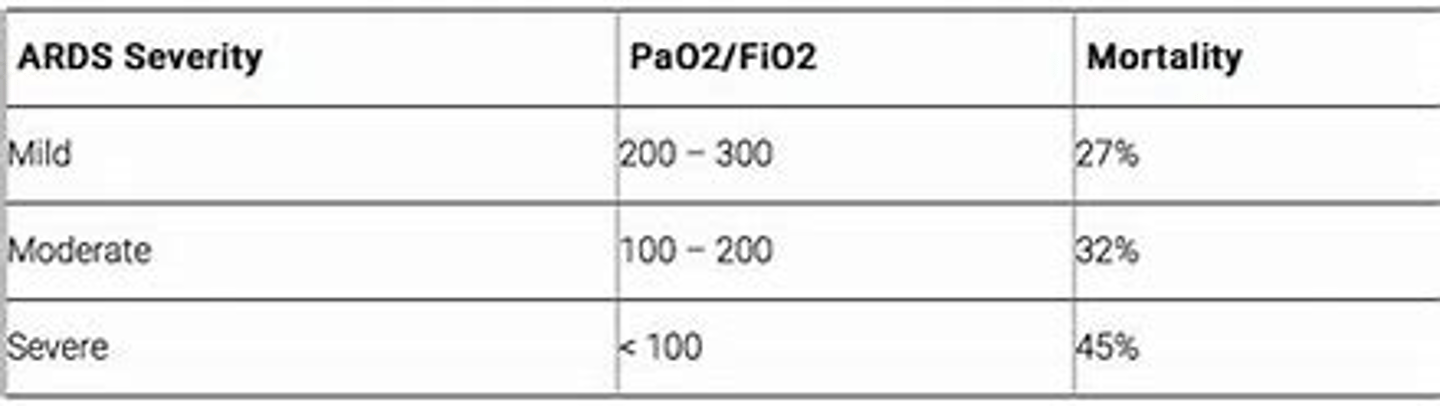
ARDS Severity (P/F ratio) and positioning
if moderate to severe severity, mortality benefit seen in early prone positioning.
TRALI what is it, how does it present and how to treat?
transfusion related lung injury. Thought to be due to neutrophil activation in response to blood products.
Can occur up to 6 hours after transfusion. Presents with sudden onset hypoxia and dyspnea with pulmonary opacities on CXR. May have fever and hypotension.
Treatment is supportive.
Signs of cyanide poisoning and anectdote
headache, nausea, vomiting, seizures, flushing, confusion, obtundation.
Treatment, stop nitroprusside (or nitrate or depo causing it) and if bad, can give nitthiosulfate which binds the cyanide methemoglobin complex.
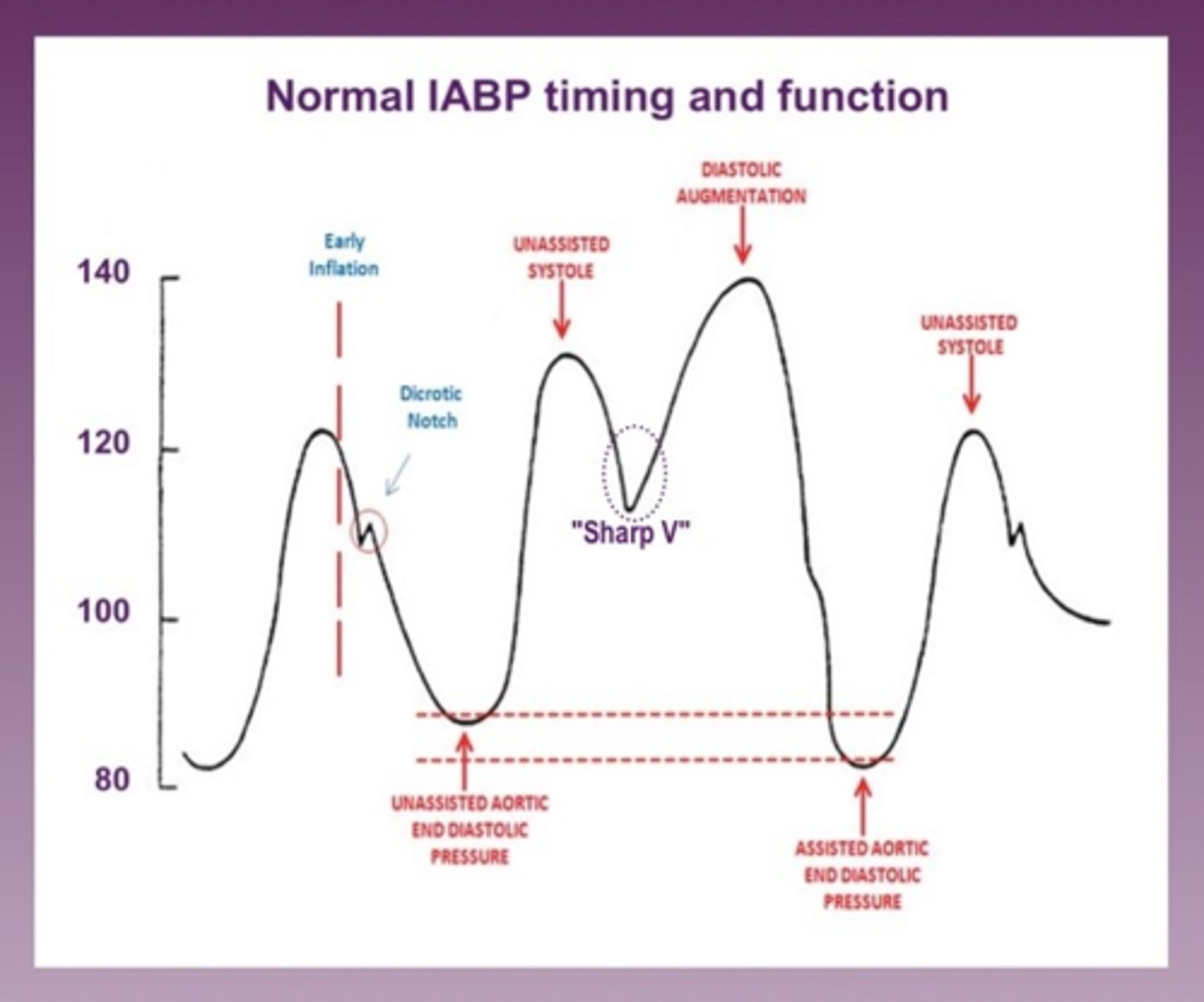
IABP timing issues graphed
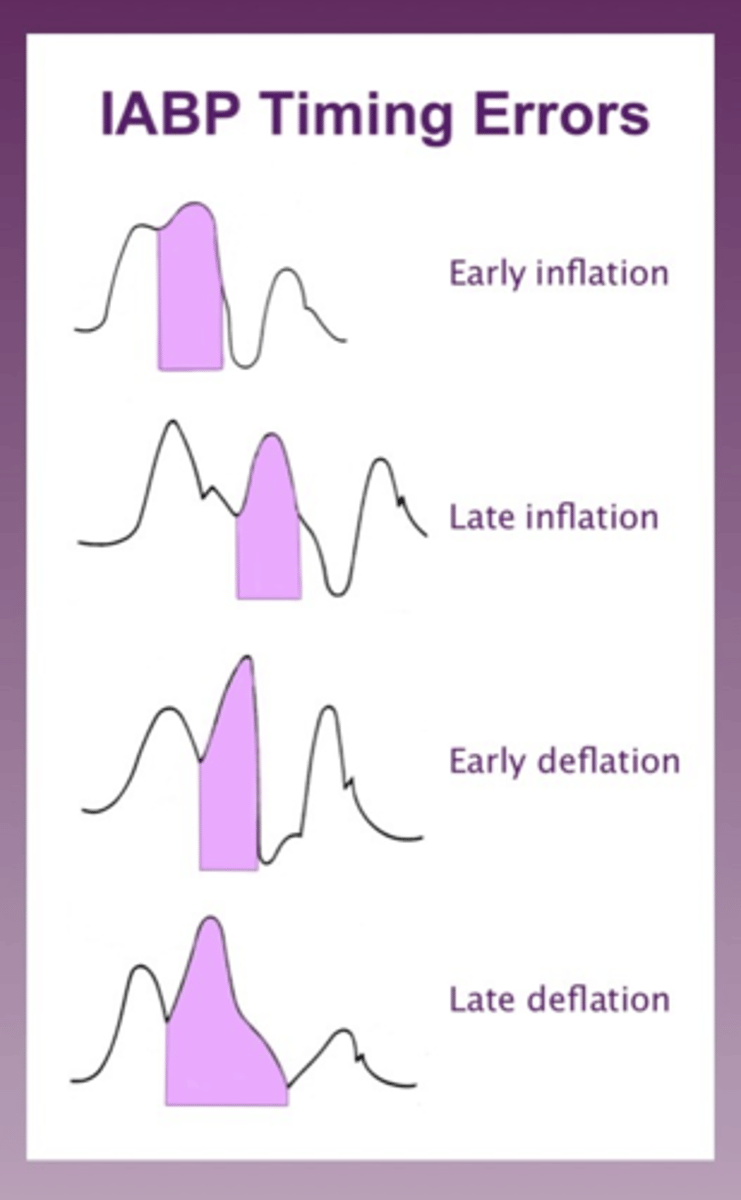
sharp V that you want with appropriately times IABP
Fick principle formula
CO = rate of O2 consumption / 10 (1.36x hemoglobin x arterial O2 content - pulmonary artery O2 content)
O2 consumption= 125xBSA
old standard for calculation CI for patients when swan is likely to be inaccurate.
Likely to be inaccurate when tricuspid regurgitation, intracardiac shunts, irregular rhythms, low cardiac output.
Massive, submassive and limited PE definitions
Massive: PE wit hypotension <90
Submassive: PE without hypotension but wit cardiac alterations (wall stress on eco, troponins, elevated BNP)
Limited: PE wit low risk and treated wit anticoagulation.
What to be aware of for vasopleia in patients on SSRI treatment algorithm
beware of giving methylene blue because it is also a MAO inhibitor which leads to serotonin syndrome and can be deadly.
Treatment for serotonin syndrome
Cyrproeptadine is treatment for serotonin syndrome.
Myasthenic Crisis: preoperative prevention and management
If higher risk, can give preoperative plasmapheresis to reduce risk.
If have crisis, intubate, IVIG or plasmapheresis, stop anticholinesterase inhibitor b/c increases secretions while intubated and give high dose steroids.
Factors that put patient at higher risk for MG crisis
if have bulbar symptoms
preoperative expiratory weakness
preoperative vital capacity <2L
hx of MG crisis
antiacetylcholine receptor antibody >100 nmol/L
intraoperative blood loss >1L
Drug used to wean off iNO by helping with pulmonary hypertension after cardiac surgery
sildenafil.
phosphodiesterase inhibitor oral medication
predictors of poor outcome when placed on VA ECMO
diabetes
low EF
SBP <90
prolonged CPB times during prior operation
persistent metabolic acidosis after being on ECMO
increased age
hypoxemia after pulmonary contusions management strategies on ventilator
1st increase PEEP
2nd: prone position with neuromuscular block has had survival benefit in these patients.
VV or VA ecmo help with survival as well.
Dementia in ICU (haldol, Seroquel, precedex, Benzos)
haldol: not recommended for delirium other than that associated with alcohol withdrawal
Seroquel: only for delirium associated with danger to the staff or patient themselves.
precedex: improves duration of delirium when used.
Benzos: worsen delirium.
most common organisms for sternal infection
MSSA then MRSA then GNB then coag neg staph then strep.
pulmonary vascular resistance is increased by :
hypercarbia, acidosis. hypoxemia.
most common cause for readmission after lobectomy
infection post op: pneumonia, empyema, wound infection.
major bleeding on warfarin reversal technique
PCC with vitamin K
only if no PCC do you give FFP (plasma)
Idrarucizumab
reversal agent for dabigatran (direct thrombin inhibitor).
Subsegmental PE treatment guidelines
if low risk of VTE and no DVT in LE's then clinical surveillance recommended over anticoagulant.
if high risk of VTE and/or have DVT in LE's then anticoagulation over clinical surveillance is recommended.
Initial treatment for actinomyces lung abscess
IV penicillin 4-6 wks followed by 6-12 months oral penicillin.
Mechanism in which ARDS causes cor pulmonale (right heart failure)
hypoxia induced pulmonary hypertension
first therapy is to fix oxygenation/optimize the vent settings.
Initial treatment for severe hypercalcemia
IV fluids that do not have calcium and loop diuretics for intravascular balance.
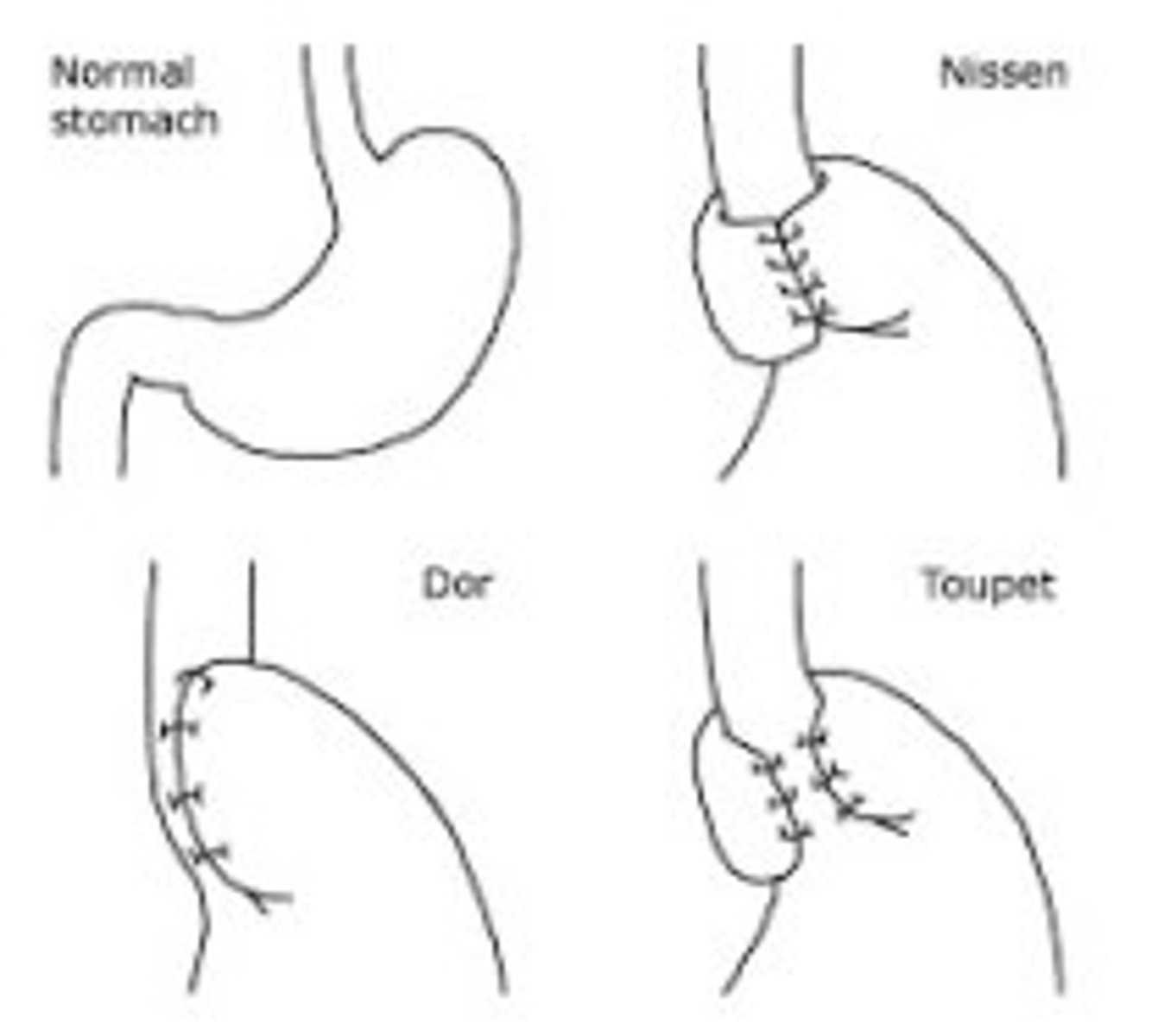
Nissen, Dor, Toupet
Nissen 360 back wrap
Dor: 180 front
Toupet: 270 back