Rehabilitation of Common Knee Conditions
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
Common Conditions
conservative treatment of ligament injuries
meniscal pathology
knee fractures
anterior knee pain
osteoarthritis
rehab of surgical knee:
TKA
ligament repairs
return to sport
protocols for reference
Knee Rehab musts
control swelling ASAP — may elevate with knee in some flexion
no pillows under post surgical knees or acute knee injuries (unless with elevation)
get the extensor mechanism facilitated - QUADS!!!
get full knee extension - ASAP
get at least 90 degrees flexion - ASAPabove and below - often controls middle
normalize gait mechanics ASAP
match your progression with healing time tables
get functional fast
DEFLATE STRAIGHT to 90 = FULL WEIGHT GAIT
How to get rid of knee swelling
RICE (which is the best)

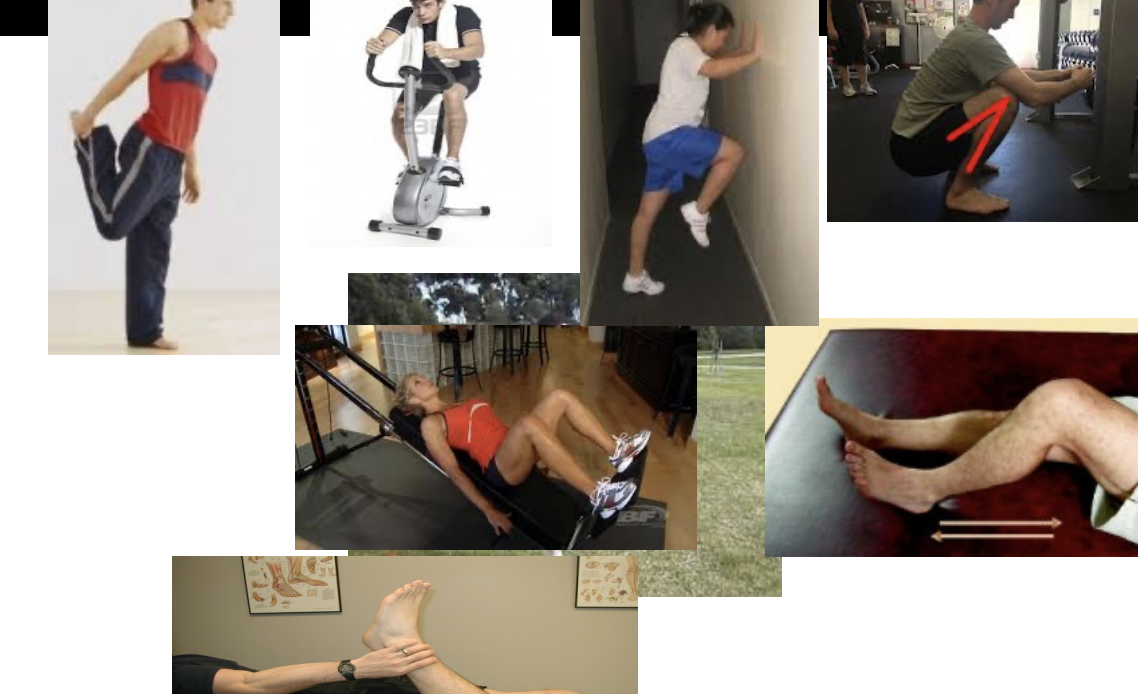
How to get full knee extension (and fire up the extensor mechanism)
mobilize, stretch, exercise (example)
mobilize
patella mobs, femur dorsal glides/tibial anterior glides (**if indicated**) soft tissue/scar mobilizations
Stretch
hamstrings, gastrocs/soleus, hip flexors
exercise
promote desired movements
use synergist
knee and hip exteners
standing TKEs

How to get knee flexion
MOBILIZE, STRETCH, EXERCISE
protect the incision
mobilize
patella mobs, tibial dorsal glides, soft tissue/scar mobilizations
stretch
quadriceps, hip flexors
exercise
promote desired movements
use synergist
knee and hip flexors
CPM’s - Controversial (patient values)
Exercise Progression Guidelines
if no soreness from prior visit, progress by modifying one variable
if soreness is present, but decreases with warm-up, stay put
if soreness remains, increased swelling, etc. back off progression
Remember the Hip and trunk
3 way SLR’s — yes… but are they functional?
standing impulse drills for extension, abduction, and flexion
hip ER exercises — T-band — multiple ways
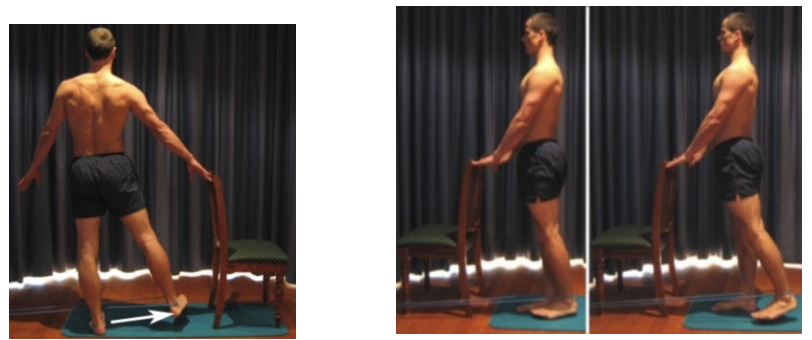
Functional is Fun
Normalize Gait mechanics
motion before strength
precursor to all other ambulatory movements (ie. running)
no pain, no limp, no swelling, match assistive device
sagittal, frontal, and transverse planes
Balance/proprioceptive training
awareness of joint position in space
react to various movement and forces
mass and momentum
gravity and ground reaction forces
aide in restoration of biomechanics and normal
should be performed from day one
often until the end
perturbation training
Hip and Ankle mobility and stability
use multiple moving parts:
arm and leg drivers
aides in restoration of global biomechanics
Copers - May not require Surgery
< 1 episode of giving way - NO INSTABILITY FUNCTIONALLY
> 80% 6m timed hop test
>80% KOS ADL subscale
>60% global rating of knee function
less active, not planning on high activity/cutting sports
no other injuries, meniscal, cartilage
ACL Non-operative
control swelling
gain ROM
optimize Quad function
address hamstring activation as secondary restraint
neuromuscular rehab - best copers improve the most in this!
progress in stages similar to operative protocol
Medial Collateral Ligament Injury
Location of tear
proximal, mid-substance — heal better, but more scare tissue formation = progress ROM early
distal tear — more-laxity, poor healing = progress ROM slower - may be immobilized in hinged brace up to 3 weeks
MCL Injury - ROM restrictions
perform exercises in sagittal plane
progress with tibial IR during resisted exercises
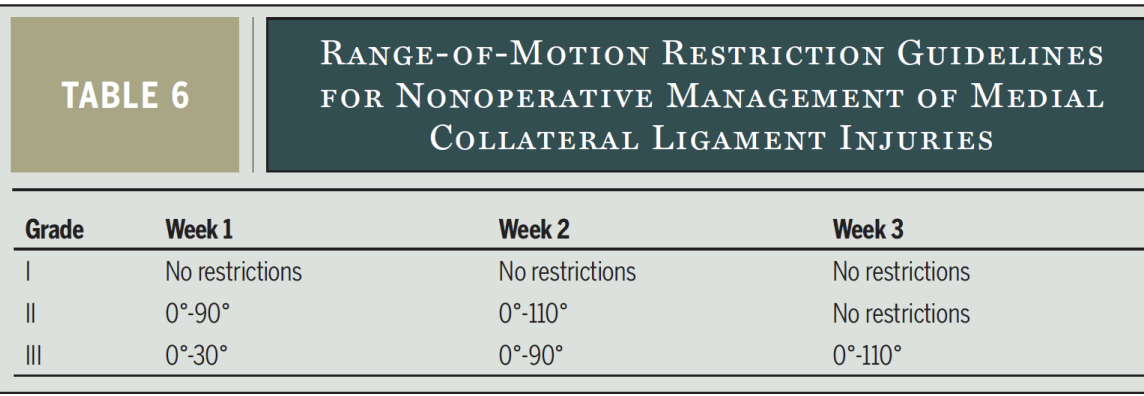
MCL Injury
Key Concepts:
avoid valgus stress early
quad control and knee extension attained early
progress with functional activities when good quad control and good static leg balance
Lateral Collateral Ligament Injury
progress slower than MCL Injuries
full weightbearing at 4 weeks
Key concepts:
quad, knee motion attainment
control swelling
avoid early varus stresses
Posterior Cruciate Ligament Tear
progress conservatively with flexion, limit posterior translation by avoiding excessive isolated hamstring strengthening
weightbearing depending on other injuries
if unstable with gait, consider a hinged brace for 3-6 weeks
focus on quads
follow criterion based progression for ACL with PCL reconstruction surgery
Acute Meniscus Tears
manage pain and inflammation (hemarthrosis)
relative rest (introduce gentle ROM and can begin isometric exercises after 72 hours)
ice
compression
elevation
activity limitation
progressive and graded exercises with a return to activity plan
Acute Meniscus Tears: Exercises
Limit excessive endrange knee flexion (especially with high load)
Minimize tibial rotation
Watch progression in weight-bearing, start exercises open chain, progress to closed chain
Regular force on the meniscus is necessary for proper healing
Six week return to activity program minimum
Chronic Meniscus Tears
Likely that they also have osteoarthritis, or greater likelihood of developing osteoarthritis
Manage like OA
“sufficient evidence had accumulated to show significant benefit of exercise over no exercise in patients with osteoarthritis, and further trials are unlikely to overturn this result.”Uthman, 2013
Focus on improving motor control and muscle stability in order to decrease stress on the meniscus
Meniscus Treatment
Manual Therapy
painfree
tibiofemoral distraction
anterior tibial glides
posterior tibial glides progress in flexion
oscillations in flexion or extension
Knee Fractures
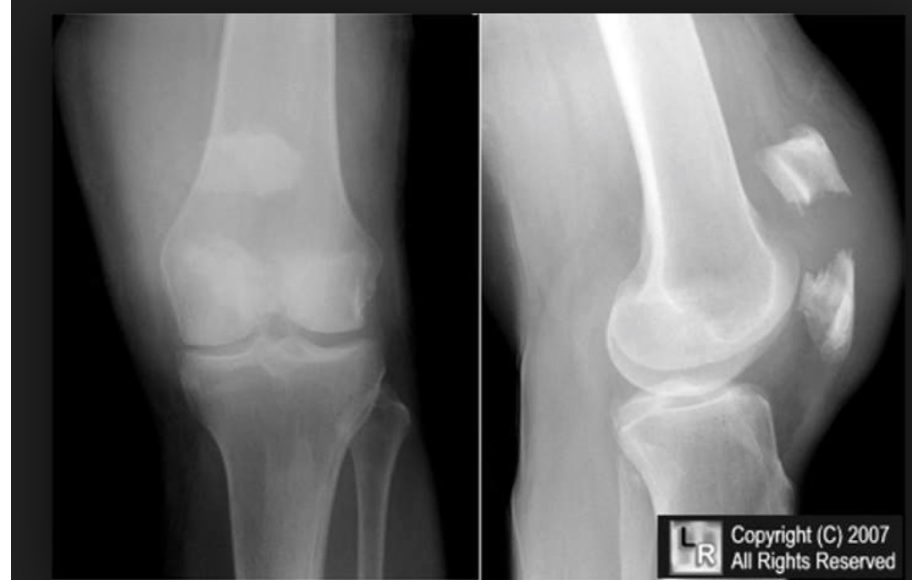
Fracture Care
movement and muscle activation dependent upon stability of fracture
ALWAYS CONSULT PHYSICIAN
precautions — weightbearing
stability
motion allowed
Knee Fractures: Immobilization Phase
immobilized 4-6 weeks for most fractures
patient education, prevent DVT’s protection of fracture, Compliance
Knee Fractures: Mobilization Phase
WBAT progress to full weightbearing
manual therapy — check with physician
exercise progression
Anterior Knee Pain
Contributions of:
Hip
excessive IR
weak external rotators/extensors
Foot/ankle
navicular drop
tight gastrocs
poor footwear/training
muscular tightness
lateral quads, IT band
patellar mal-alignment - Alta, baja, medial, lateral tilts, rotation
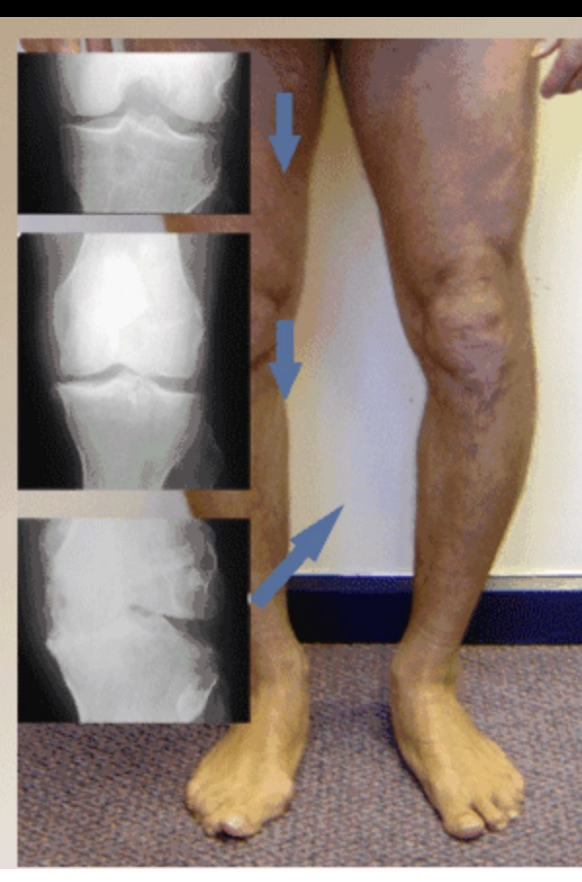
Knee OA
The Evidence- What we know:
obesity affects outcome
interferential current for pain relief
manual therapy plus exercise better than home program
alignment affects pain and disability
psychosocial - self efficacy improves function
adherence - improves long term outcomes
OA Knee
What We Do?
Encourage weight loss- Be nice
Reduce reactivity- Ice, IFC
Normalize Gait- Crutches, (Cane-or not)?
Assess mobility- Get accessory mobility back-Soft tissue, capsular, flexibility
Alignment- Foot wedge, orthotics, bracing if severe
If knee varum, lateral foot wedge
If knee valgum, medial foot wedge
Psychosocial- Encourage activity, progress without pain
Exercise- Open and Closed Chain both OK, keep them OUT OF INCREASED PAIN with activity
(Lin DH, et al. JOSPT 2009)
Follow up- Booster- Phone Call, re-assessment
Management of Common Surgical Conditions
total/partial knee replacement
ACL reconstruction
multi-ligament considerations
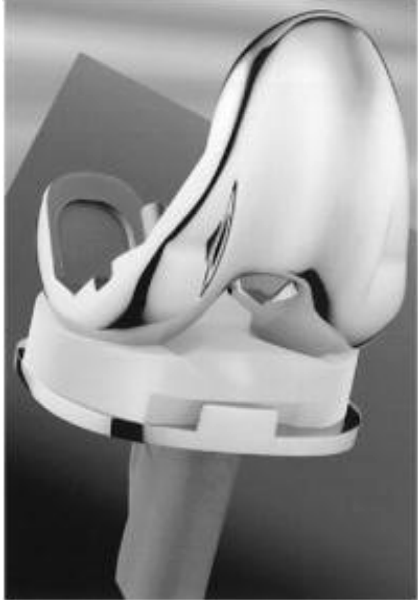
Types of Arthroplasty
unicompartmental arthroplasty
patellofemoral arthroplasty
total knee arthroplasty
Uniarthroplasty
used for isolated medial
> lateral compartment disease
all ligaments must be intact
<8% of all arthroplasties
good candidates are normal weight, elderly

Patellofemoral replacement

Total knee arthroplasty
3 types: All types REMOVE ACL
CR = Cruciate retraining (PCL retained)
PS = posterior stabilized
RP = rotating platform

rotating platform
special type of PS TKA design to increase surface area to reduce contact stresses
the poly piece can rotate side to side separate from tibia
increased conformity of tibiofemoral articulation
mobile bearing used to diminish any kinematic conflicts
Total Knee Arthroplasty
monitor incision for signs of infection
DVT - Wells criteria
take girth measurements
move the patella
WBAT - Good gait
progress ROM as tolerated
too much WB = too much swelling = stiffness
stop the madness
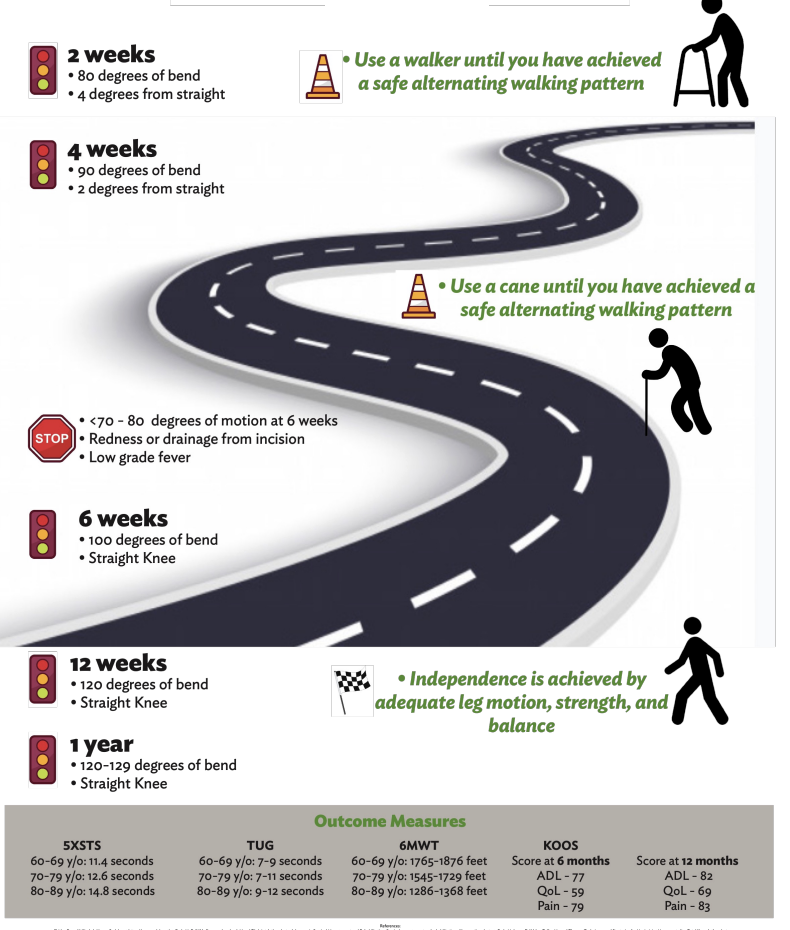
stiffness of <70 degrees 2 weeks post-op
may require manipulation
best 8-12 weeks post
risk of fracture increases over 12 weeks
pre-op stiffness = post op ROM loss
if unusual amount of unrelenting pain, SOMETHING IS WRONG
Total Knee Replacement: Road to Recovery
To Cope or Not to Cope
Few Studies have actually shown the ACL reconstruction restores dynamic knee stability
No clear evidence that Repair or non-Repair is any different on degenerative changes later in life
Screening Exam has poor predictive value of determining copers and non-copers
Copers
Movement consistent with good knee stability
Less episodes of giving way of knee
Less anterior joint laxity
Higher Knee Outcome Survey
Higher Activity level
Hop Testing > 90%
Non-Copers
Poor movement patterns, alternate strategies
More episodes of Giving way of knee
More anterior joint laxity
Lower Knee Outcome Survey
Modified activity levels
Hop Testing < 90%, but after one year equal to copers
ACL Reconstruction Guidelines
Isolated tear, versus concomitant injury
meniscus debridement, repair, replacement
other ligament disruption
chondral defects
Isolated ACL Reconstruction
control swelling
get extension — gradually gain flexion, but don’t push early
patellar mobility
quad activation
restore normal gait
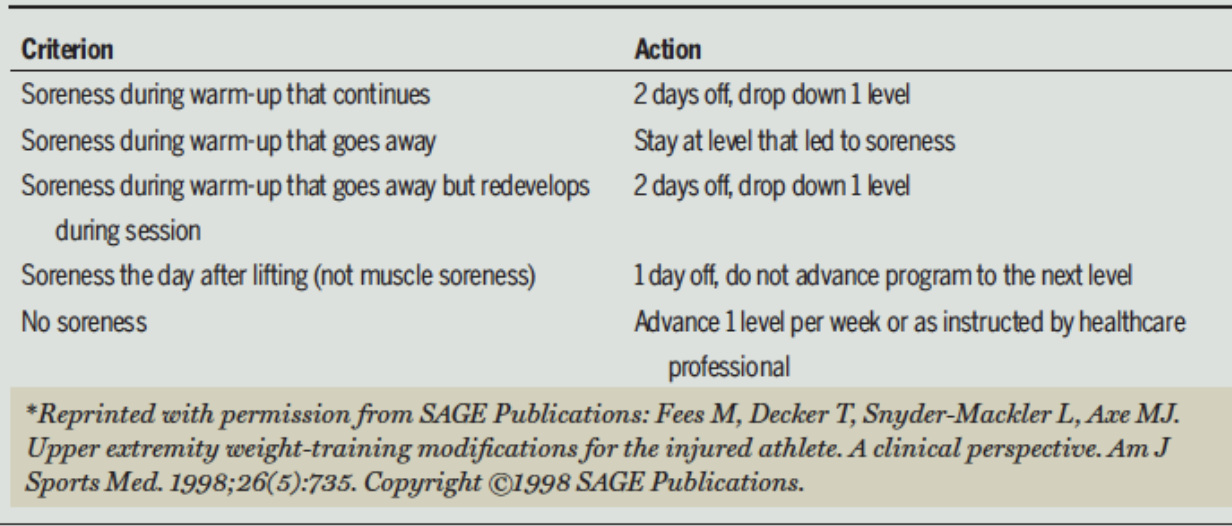
ACL Reconstruction Rehab Guidelines
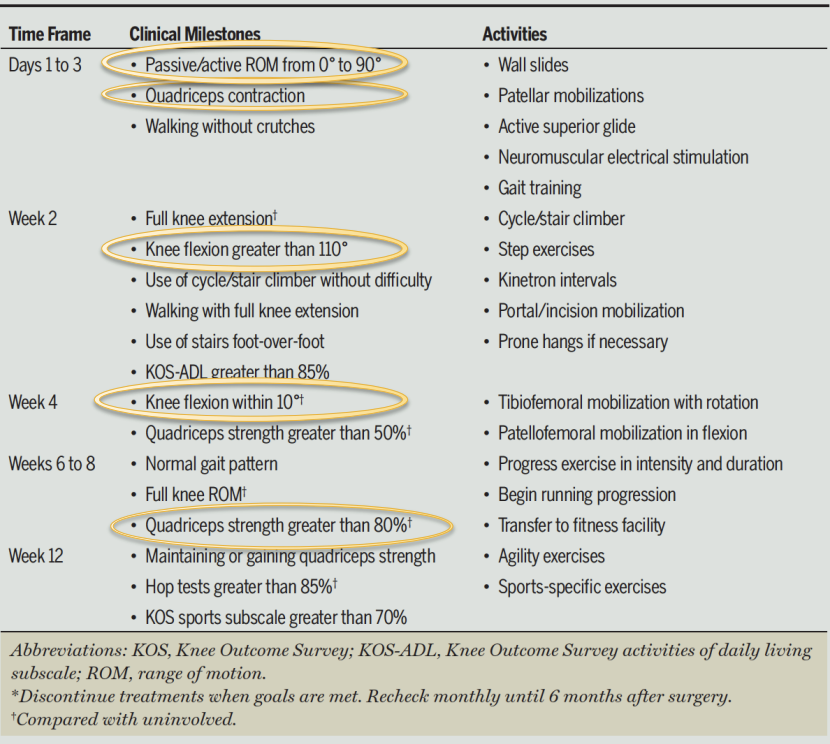
Soreness Rules
Multiligament Reconstruction: DELAY
Usually ACL and PCL, and either MCL, LCL or Posterolateral Structure Involvement
Follow more conservative PCL protocol
3 Ligaments, 3 Delays: weightbearing, mobilization, functional progression
Usually Non-Weightbearing for 6 weeks
Immobilizer up to 8 weeks
Functional Progression
Running progression no earlier than 12 weeks
Functional Testing no earlier than 16 weeks
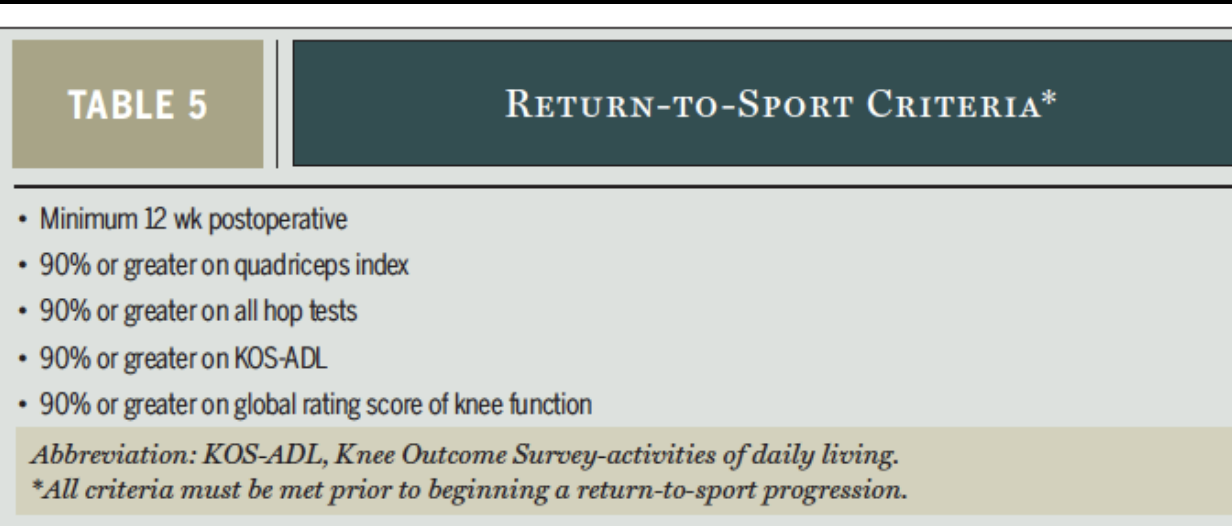
Return to Sport
ACL or PCL: 9-12 months
earlier than this runs risk of reinjury or INJURY TO OTHER SIDE
Rule of 90s
KNOWWW
Return to Sport PROGRESSION
Walk, stairs, run, hop, cut, PREVENTION
Walk- good gait, full ROM
Stairs- step up/down with good alignment, control, painfree
Run- same as walking but faster
Hop- Hop Tests
Cut- Cutting drills
Prevention- FIFA 11, etc
Hop Tests - 90% of uninvolved
Single leg hop
Timed hop
Triple hop
Cross over hop
Practice, 3 trials, average
For timed hop take Uninvolved/Involved 100
For others Involved/Uninvolved100