Urinary System - chapter 21
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
major roles of the kidneys
1) filter metabolic wastes from the blood (urea, uric acid, and creatine) and excreted them from our body In urine
2) regulate the blood volume and blood pressure by altering the volume of urine produced an day releasing renin into the blood, which activates angiotensin II promoting vasoconstriction and aldosterone secretion. Maintain blood osmolarity of 300mosmoles/L
3) production of erythropoietin in response to low O2 levels. Erythropoietin stimulates erythrocyte proliferation and maturation in the bone marrow
4) regulate the amount of electrolytes (ie Na, L, Cl,Ca, phosphate) in the blood and extracellular fluid by altering the urine concentration and composition. In addition the kidneys are responsible for activating vitamin D3 calciferol, which promotes Ca absorption in the small intestine
5) regulates the body’s pH by controlling the amount of H+ secreted and HCO3 reabsorbed from the filtrate
6) assits liver detox
ureter
the 30cm smooth muscular tube exiting each kidney from the hilum. It carries urine to the bladder by paristalsis, hydrostatic pressure & gravity
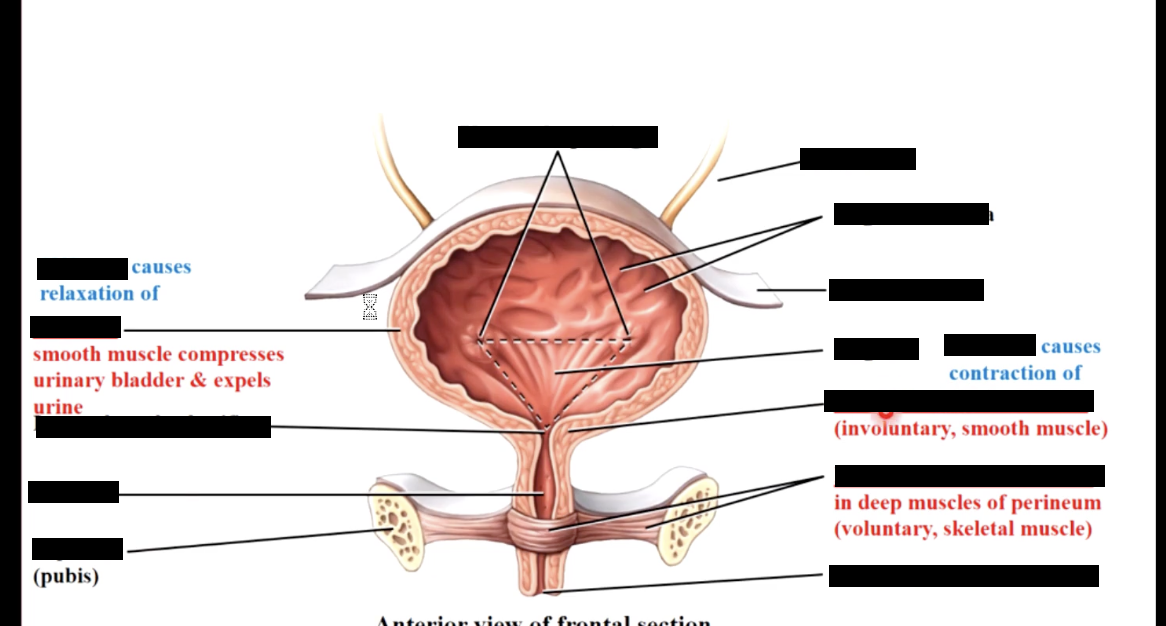
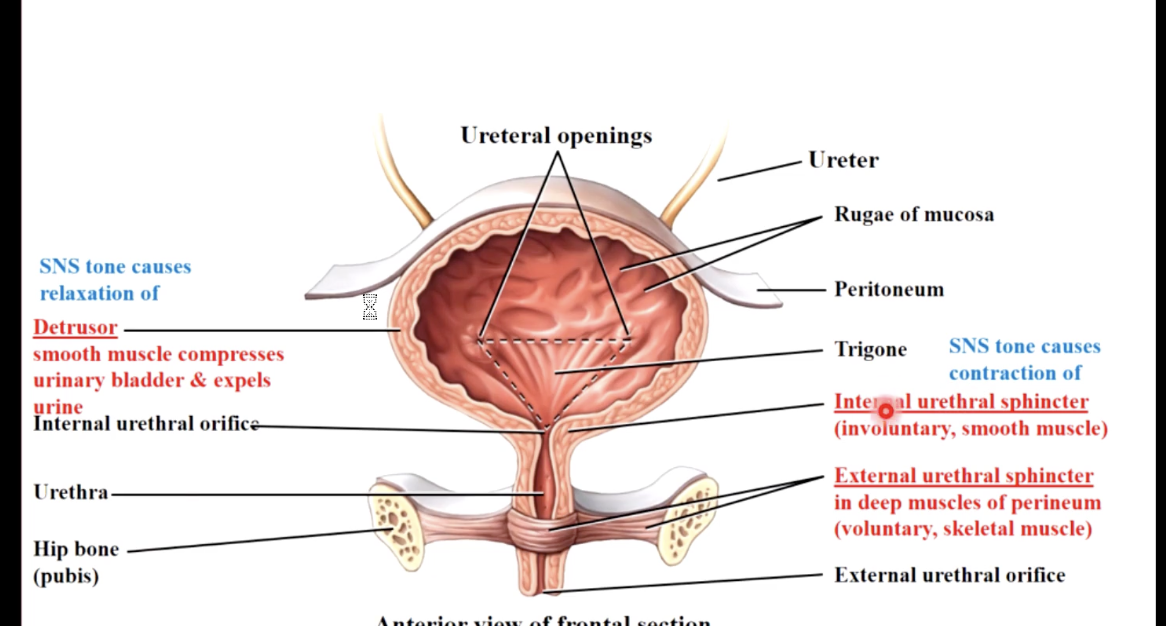
urinary bladder
a hollow, stretchy, muscular organ. It contains two sphincters - internal (non voluntary) and external (voluntary but the ANS can override). It’s capacity is approx 500-1000mL ; at 250 mL you feel like you need to pee
urethra
a smooth muscular tube exiting the base of the bladder. in males it is approximately 20cm and in females approximately 4cm
females are 50x more susceptible to infection
the kidneys
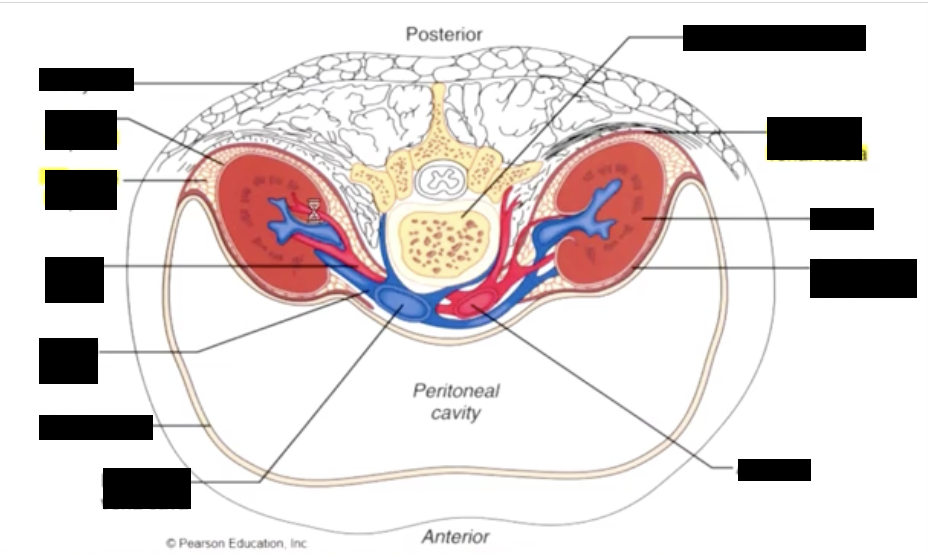
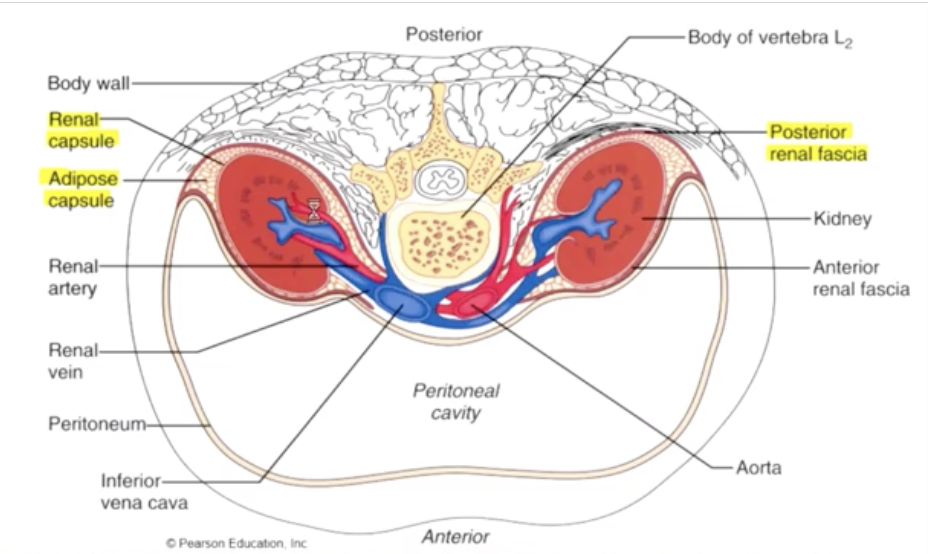
the kidneys are retroperitoneal, and are partially protected by the lower ribs
the kidneys receive blood (20% cardiac output) 1200mL/min, from the renal arteries, which branch directly from the aorta, and return their cleansed blood to the inferior vena cava through the real veins
urine produced in the kidneys travels down the 30cm ureters to the urinary bladder for storage
the kidneys are located posterior to the peritoneum (the connective tissue surrounding the go tract) in the retroperitoneal area between T12 and L3
each kidney is covered by outer renal fascia (dense, irregular CT), inner fibrous renal capsule (dense regular CT) & middle layer of adipose tissue (perinephric fat). Kidneys are suspended by collagen from renal fascia packed at AT
there are no pain receptors within the kidney, pain is only present when there is impingement (pressure) on the renal capsule or ureter
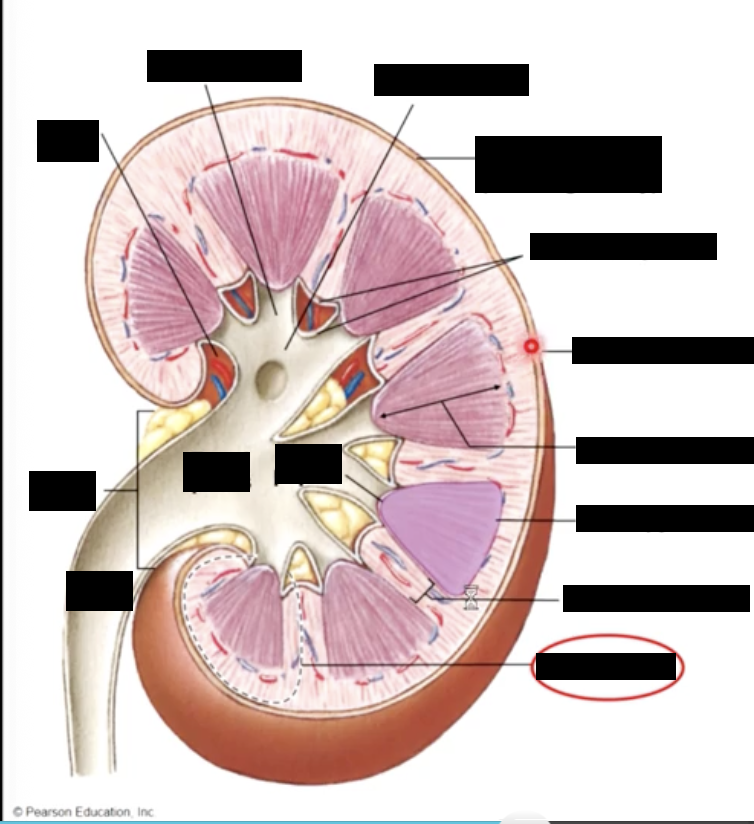
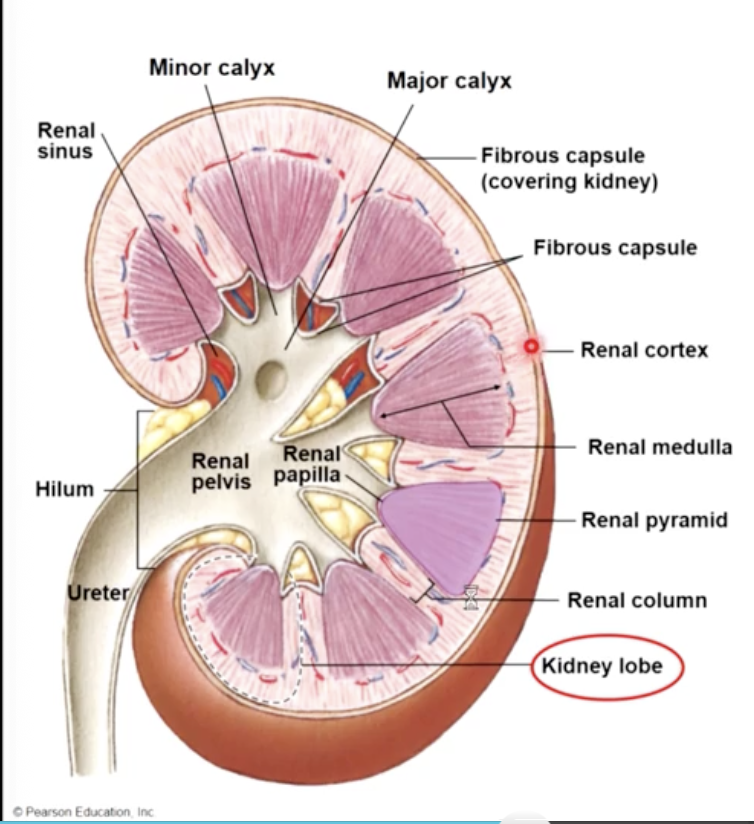
kidney blood flow
blood enters the kidney and is transported by smaller arteries to the outer position of the kidney, called the cortex. The majority of the blood is filtered here
the inner portion of the kidney (medulla) arranged in triangular shaped structures (medullary pyramids), alters the composition of the filtrate & forms urine. The area is susceptible to ischemic damage since it is very metabolically active, & has a low pO2 (due to Na/K pumps and slight arteries-venous diffusion shunt)
the urine drains into calyces collecting ducts in the medulla and eventually passes to the renal pelvis and into the ureters for transport to the urinary bladder
the renal artery branches off the aorta and enters at the renal hilum
the renal vein exits the renal hilum & branches onto the inferior vena cava
path of urine drainage
papillary collecting duct - minor calyx - major calyx - renal pelvis - ureter - urinary bladder
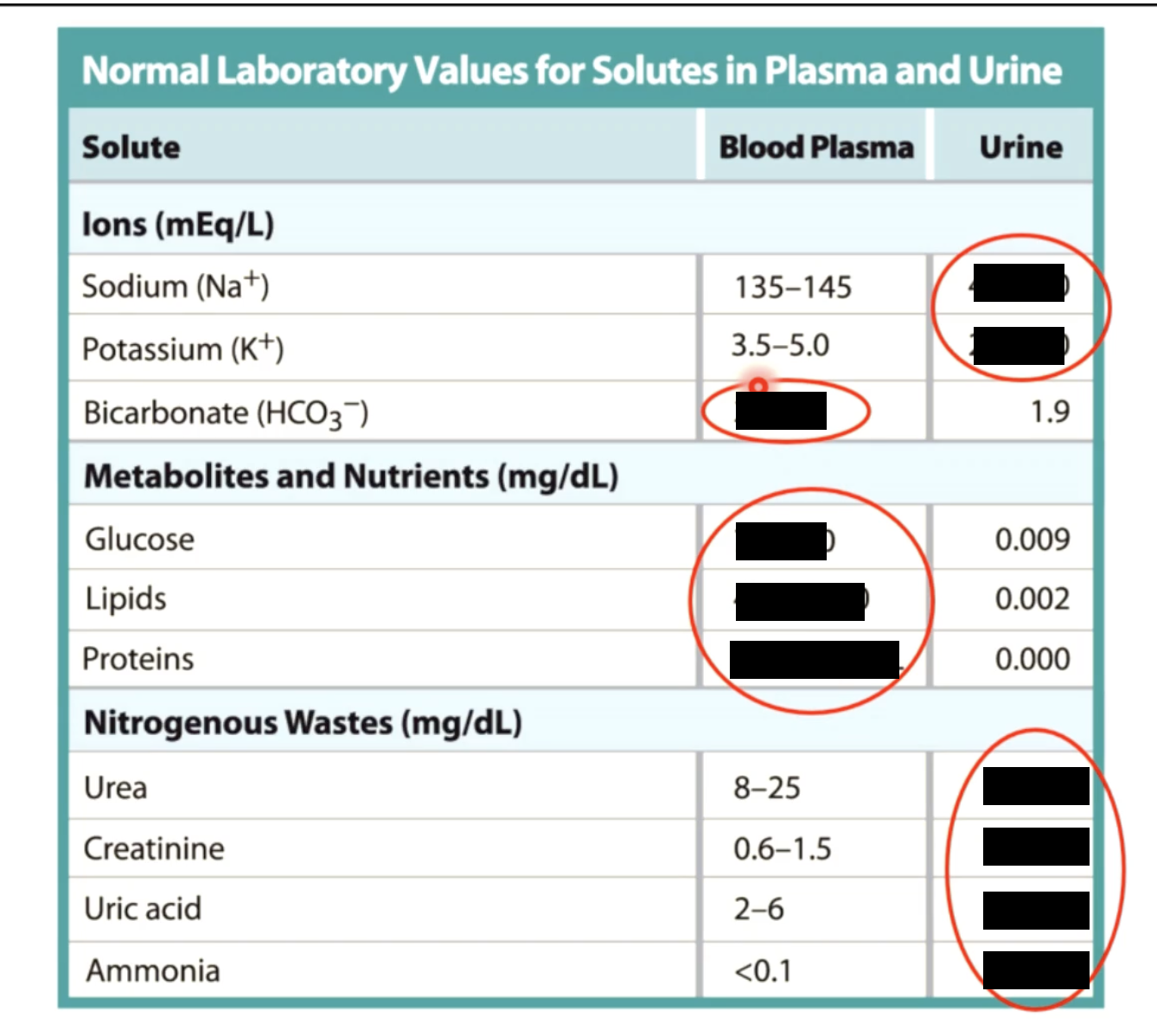
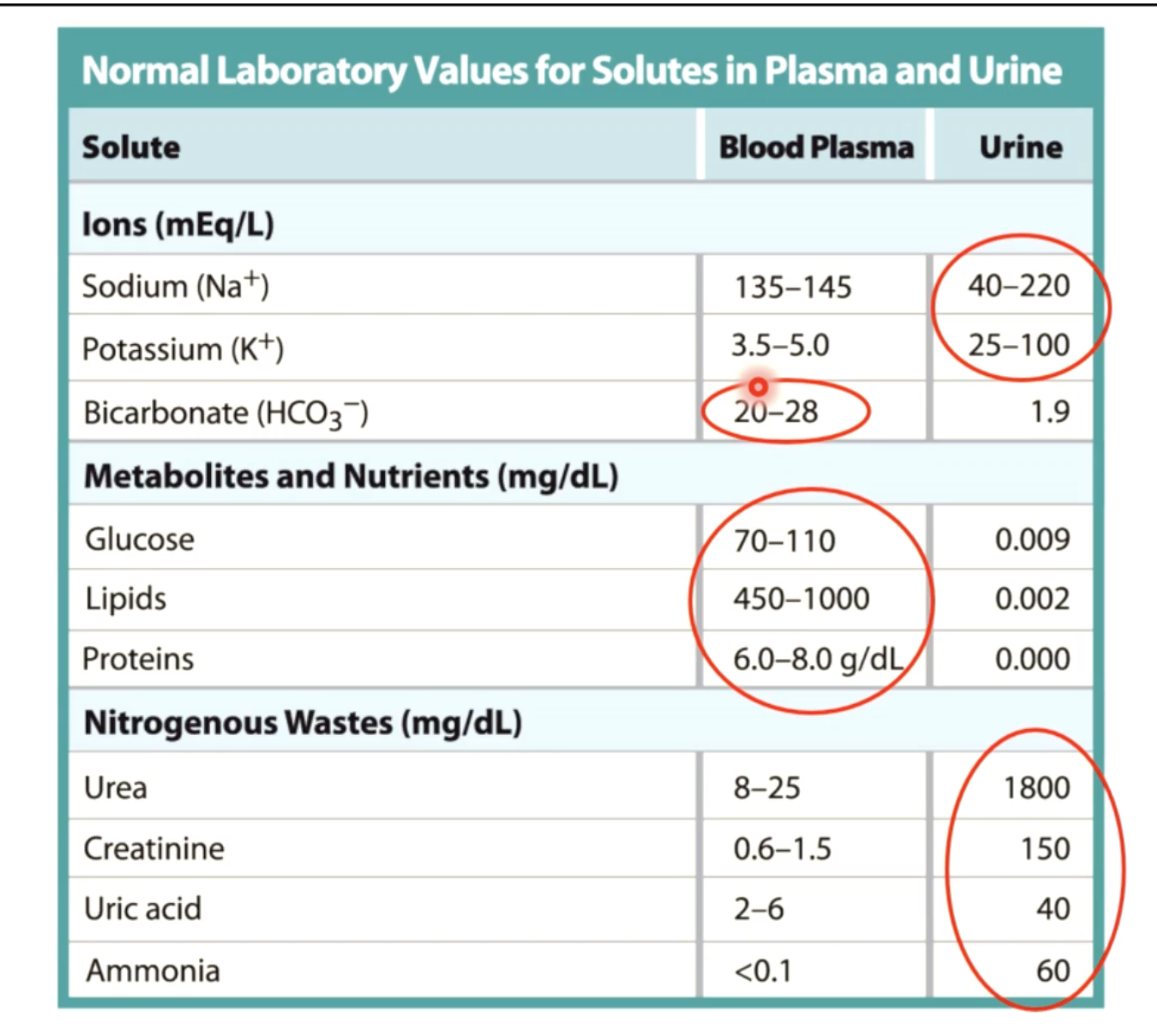
3 wastes eliminated in urine
1) urea - is produced in the liver from amino acid breakdown (21g) involves 2 steps:
amino acid → ammonia (very toxic to cells)
ammonia → converted to urea by combining with CO2. Urea, which is less toxic is sent to the kidneys for excretion in the urine
2) creatine - produced in skeletal muscles from breakdown of creatine phosphate, a high energy molecule (1.8g)
creatine phosphate is used to generate ATP in resting muscles, it is sent to the kidneys for secretion
3) uric acid - a waste product of adenine and guanine (RNA) (480g)
the build up and crystalization of uric acid is gout.
kidney stones are composed of calcium, phosphate, uric acid and proteins
homeostasis - water/salt balance
kidneys maintain BP & volume by regulating the water/salt balance of the blood
without kidneys:
if plasma salt concentrations increase, water will leave tissue fluid and enter capillaries, causing an increase in blood volume and pressure resulting in dehydrated cells
by maintaining appropriate concentration of plasma, blood pressure and volume are kept constant and cells are kept appropriately hydrated
so if blood solute concentration increases the kidneys absorb excess salts (Na, K, Ca) and excrete the excess salts in urine to maintain homeostasis. Likewise the kidneys remove excess water from plasma to maintain water/salt homeostasis and maintain normal BV and pressure
homeostasis - acid-base balance of blood
kidneys monitor H+, OH and HCO3 ion concentrations in order to maintain constant blood pH of 7.4
if blood becomes acidic the kidneys excrete H+ ions and reabsorbs the HCO3 into the bloodstream. This is the most common as all cells create acid byproducts due to cellular respiration (CO22 conversion to H2CO3 in blood). Therefore average pH of urine is 6.0
If blood becomes basic the kidneys excrete excess HCO3 ions and reabsorb the H+ ions into the bloodstream
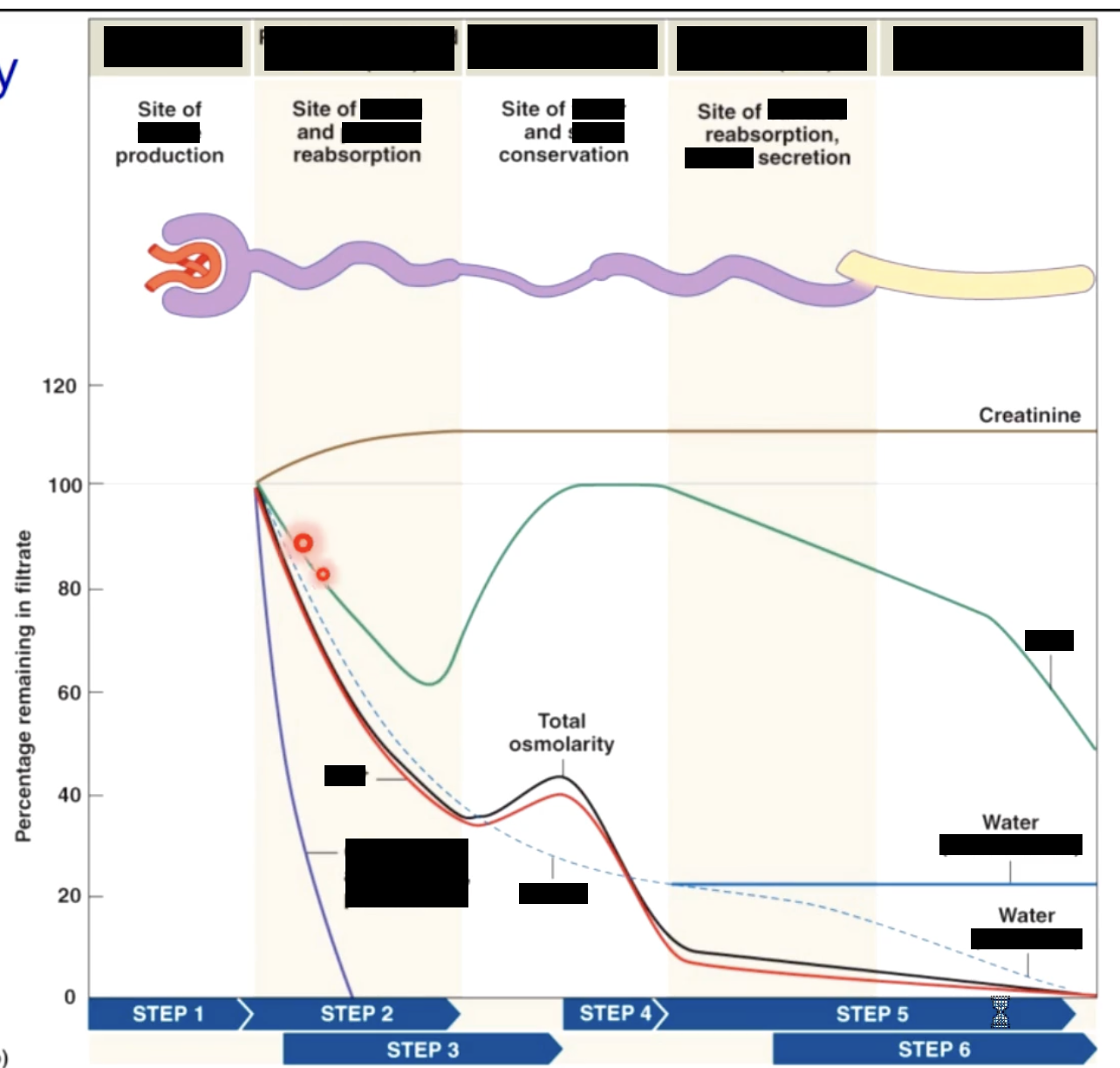
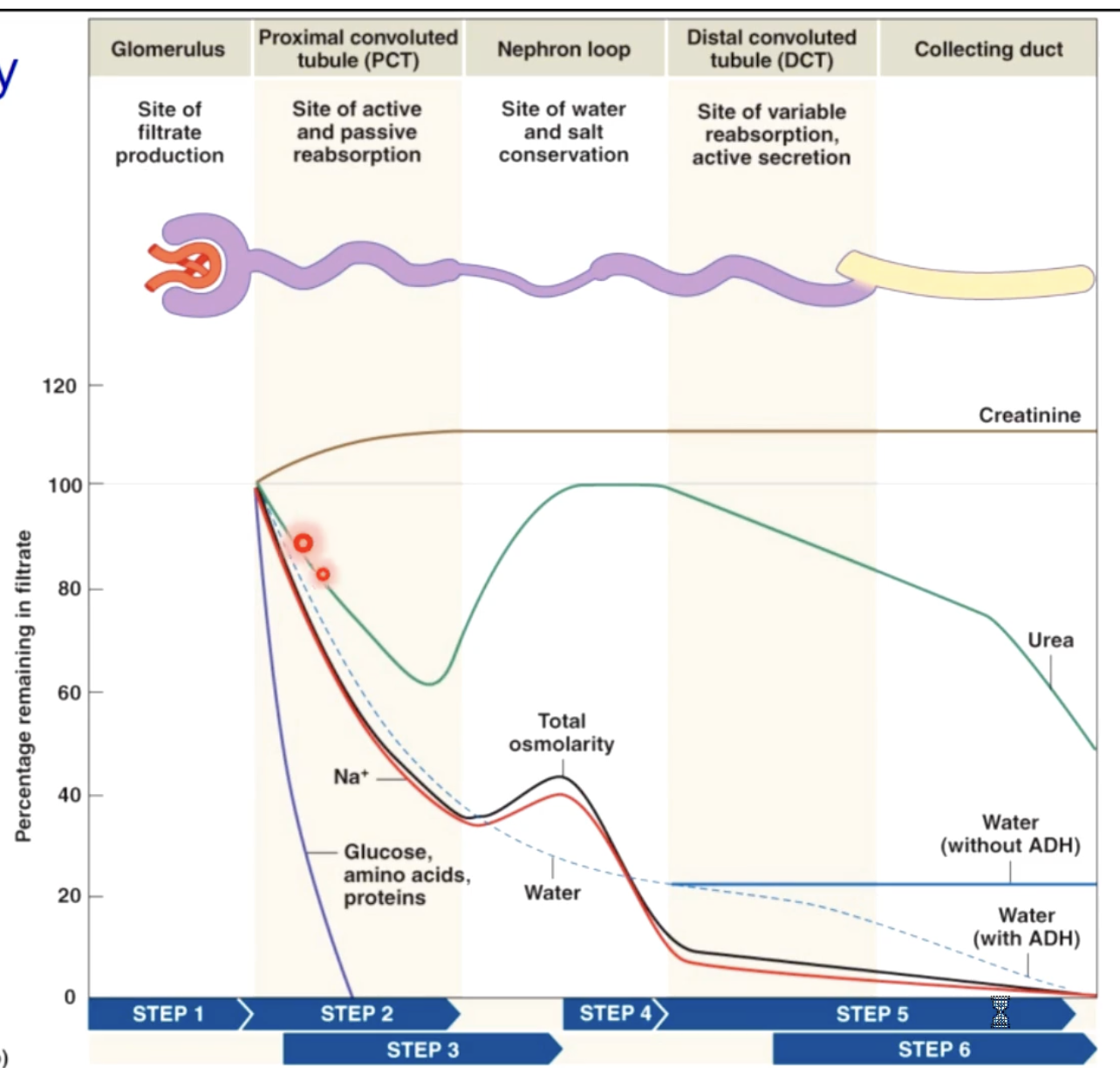
the nephron
the urine producing apparatus in the kidney
the nephron consists of a glomerulus, that filters the blood and forms a filtrate, and a tubule, that converts the filtrate into urine by reabsorbing water and electrolytes from filtrate
the tubule has 3 regions
teh proximal convoluted tubule, 2) loop of henle, which enters into the medulla of the kidney and 3) the distal convoluted tubule
the distal convoluted tubule drains into a common collecting duct that makes some final modifications to the urine and ultimately transports the urine into the ureters
85% are cortical, 15% are juxtamedullary nephrons
kidneys can produce urine 4x more concentrated than plasma
blood supply to the nephron
blood flows into the glomerulus through the afferent arteriole, which divides into the glomerular capillaries
these capillaries are very plus and allow large amounts of blood plasma to filter out into the glomerular capsule and into the proximal tubule
blood leaves the glomerulus through the efferent arteriole, which divides into the peritubular capillaries. These capillaries surround the tubule and function to absorb water and electrolytes from the filtrate (tubular fluid)
3 processes used to produce urine
1) filteration - water and dissolved solutes smaller than 8nm (urea, glucose, salts) are filtered through the glomerular capillaries and into the tubule
2) reabsorption - 99% of water, glucose, amino acids, fatty acids, vitamins and selected electrolytes are transported into the tubular cells and enter into the peritubular capillary blood
3) H+,K+, some metabolic wastes and drugs are secretes from the tubular cells into the tubular fluid
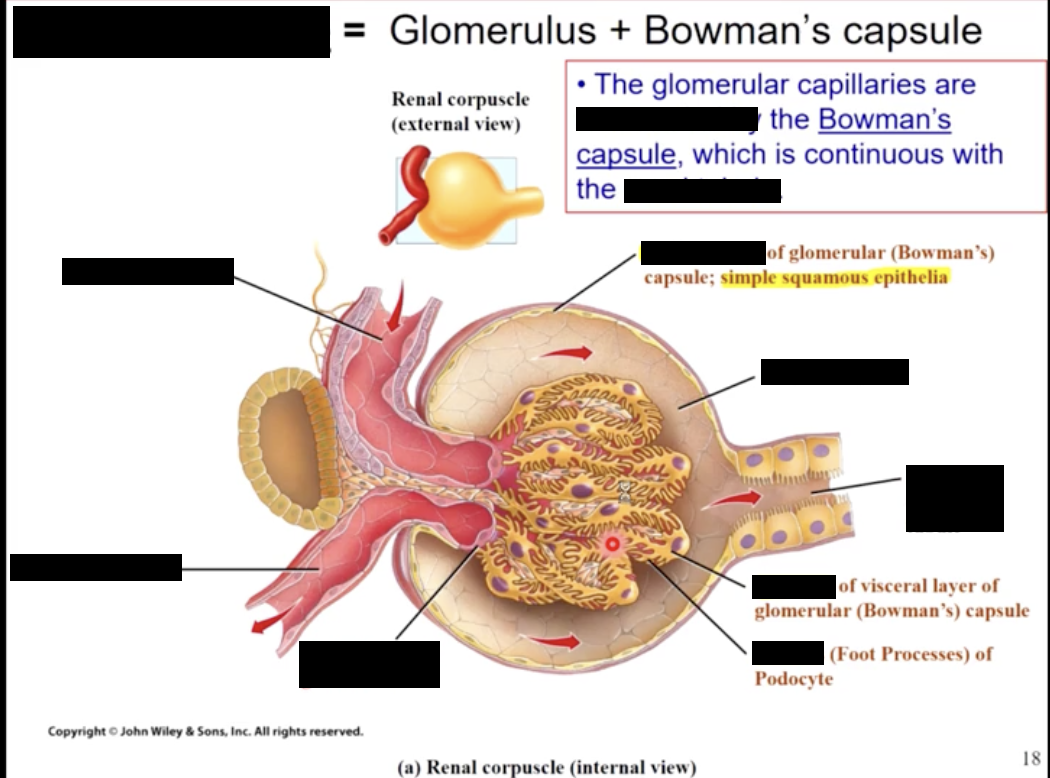
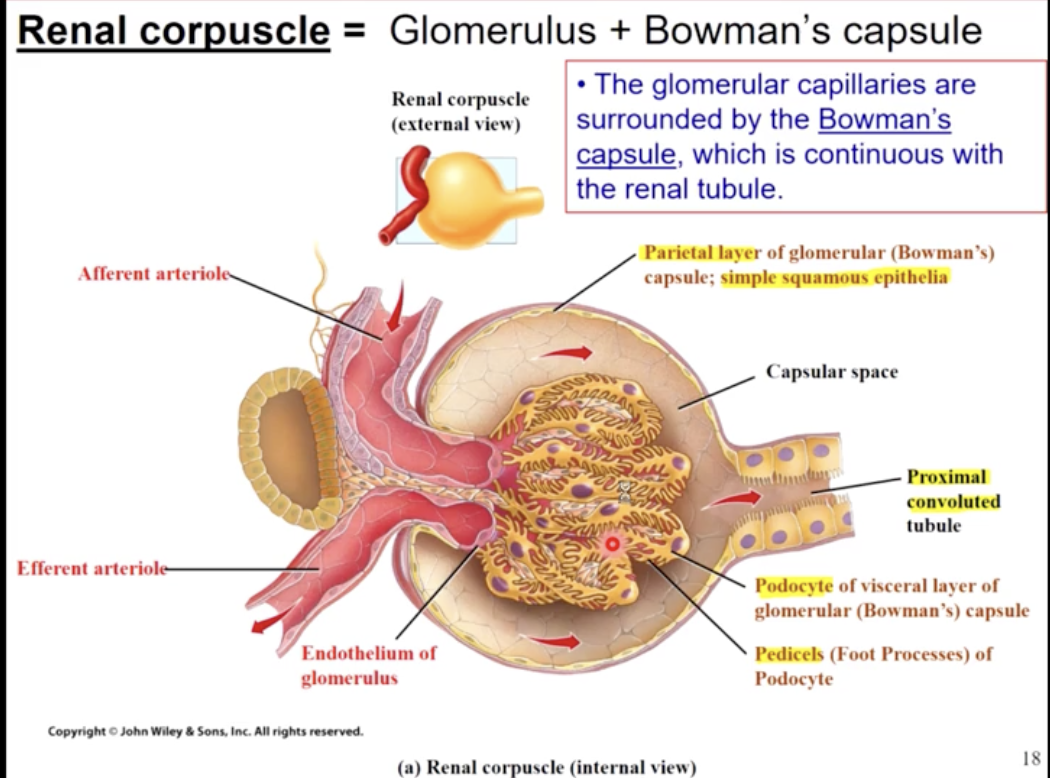
the glomerulus
the glomerular capillaries are formed from the afferent arteriole
like most capillaries, the glomerular capillaries are comprised of endothelial cells, however these have pores called fenestrations & are covered by pedicels of epithelial cells called podocytes
the fenestrations only allow particles less than 8nm to pass; however the capilariy basement membrane (laminate dense) contain collagen & negatively charged proteoglycan. This effectively repels other anions, like the protein albumin
molecules permitted - water, glucose, vitamins, amino acids, peptides, ammonia, urea, creatine and ions
not permitted - WBC, RBC, platelets, and proteins
control of filtration
glomerular capillaries are 50x leakier than other capillaries (even leakier than fenestrated because they lack a diaphragm)
glomerular pressure is high, because the diameter of efferent arterioles is smaller than afferent arterioles
glomerular capillaries have a large surface area
the amount of SA available is regulated by the contraction of mesangial cells; when mesangial cells are relaxed, filtration slit SA in increased and there for GFR (glomerular filtration rate) is increased
renal blood pressure
blood to the kidney is regulated to maintain filtration, & not to satisfy the metabolic needs of the tissue. At rest the kidneys receive 25% of the cardiac output (1.2 L/minute) . These increased with exercise
the blood pressure in the glomerular capillaries is 55 mmHg. This high pressure is maintained by flow through the afferent arteriole (BFg) and high resistance to flow in the efferent arteriole (Rg). The glomerular blood pressure (BPg) id the driving force to create filtration and is determined by: BPg = BFg x Rg
where BFg is increased with afferent arteriolar dilation and decreased with constriction, and Rg is increased with efferent constriction and decreased with dilation
when BPg is increased, filtration is increased, and when BPg is decreased, filtration is decreased
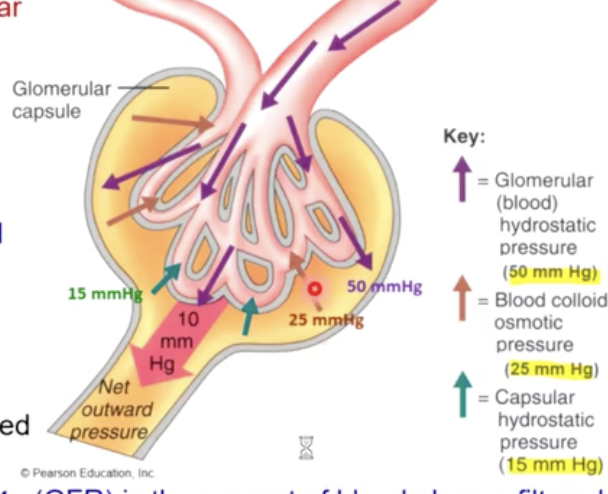
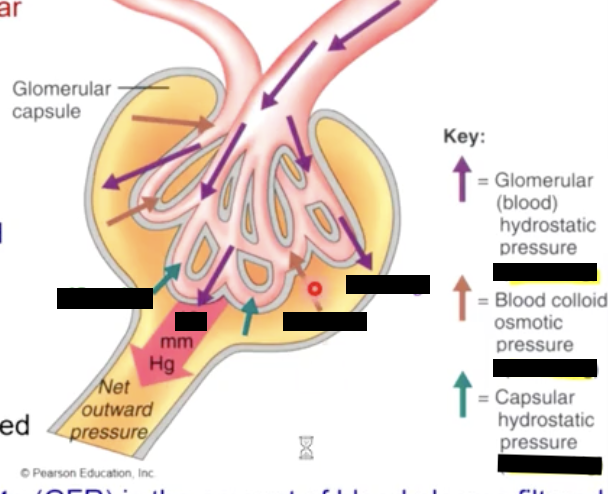
glomerular filtration rate
filtration through the glomerular capillaries is governed by the same forces as any other capillary in the body
blood hydrostatic pressure pushes fluid out and the colloid osmotic pressure pushes fluid into the capillary
the glomerulus capillaries are fenestrated to increase their permeability, also the blood pressure is high compared to other capillaries
the glomerular filtration rate is the amount of blood plasma filtered through the capillaries by both kidneys in one minute (125mL/min)
GFR is regulated primarily by altering the glomerular blood pressure (BPg). Increasing flow through the capillaries (afferent constriction) increases GFR
where as decreasing flow and decreasing resistance would decrease GFR
why is CHP different than IHP
Capillary hydrostatic pressure is higher because of back pressure (elastic recoil from capsule). due to the glomerulus being in a contained space
if there a difference in filtrate produced depending on gender
150L for female
180L for male
due to difference in body size
The renal tubule
the renal tubule is responsible for reabsorbing glucose, amino acids, water & electrolytes from filtrate (tubular fluid)
other substance (K+) may be secreted into the tubular fluid
reabsorption and secretion may occur passively or by active process
passive processes may include diffusion and osmosis; where as active processes require ATP either directly (primary active) or indirectly (secondary active or co transport)
180L/day of water is filtered through the glomerulus and the normal urine volume is only 1L/day. Therefor, more than 99% of filtrate is normally reabsorbed
The proximal tubule
most reabsorption in the proximal tubule is transcellular & occurs by Na co transport
a Na concentration gradient is created by the Na/K pump on the basal surface of the tubule called
this gradient is used to power the absorption of other molecules like glucose
the glucose transporter is called the sodium dependent glucose transporter (SGLT, sodium glucose linked transporter)
Cl ions diffuse passively through Cl- channels and paracellular route (through not so tight junctions) to maintain electrochemical neutrality
60-70% of water is reabsorbed in the PCT, the osmotic gradient created by reabsorption of solutes. Water passes the plasma membrane through pores created from the protein aquaporin-1 and also use paracellular route
Transport maximum
Tg
65mg/dL amino acids. 180mg/dL glucose, low for water sol-vitamins
the loop of henle
the primary function os to remove water from filtrate
this is achieved by a highly concentrated interstitial fluid (ISF) that becomes more concentrated deeper into the medullary pyramid. This concentration gradient in maintained by the vasa recta
as filtrate decends into the loop, water is pulled out by osmosis because of the ISF concentration
the loss of water creates a highly concentrated filtrate. As the filtrate ascends the loop Na and Cl are actively reabsorbed to reduce the filtrate concentration. Osmotic concentration (solute particles/L goes from 300 to 100Osm)
the net result is a greatly diminished filtrate volume
depending and ascending loop
thin depending limb - permeable to water, impermeable to solutes
thick ascending limb - impermeable to water, active solute transport
active transport of NaCl along the ascending thick limb results in the movement of water from the descending limb
papillary duct - permeable to urea
the permeability of both the collecting duct and the loop tend to concentrate urea in the tubular fluid and in the medulla.
The nephron loop DCT and collecting duct and impermeable two urea. As water reabsorption occurs, the urea concentration rises
sodium potassium pump in loop of henle
the mechanism of sodium and chloride ion transport involves the Na+ - K/2Cl carrier at the apical surface and 2 carriers at the basal surface of the tubular cell: a potassium - chloride cotransport pump and a sodium-potassium exchange pump. The net result is the transport of sodium and chloride ions into the peritubular fluid
concurrent vs counter current flow
kidneys use countercurrent flow to remove water from urine so the body can retain water used to move nitrogenous waste products
a countercurrent multiplier system where a high medullary interstitial concentration of solute is maintained allowing the kidney to concentrate urine
the loop of henle is the counter current multiplier actively pumping out NaCl in ascending limbs
a positive feedback loop is created as NaCl removal “pulls” water out of descending limb increasing NaCl concentration, which then is actively pumped out
the vasa recta is the counter current exchanger
the vasa recta is a portion of the peritubular capillary system which enters the medulla. If the vasa recta did not exist the high concentration of solutes in the medullary interstinium would be washed out
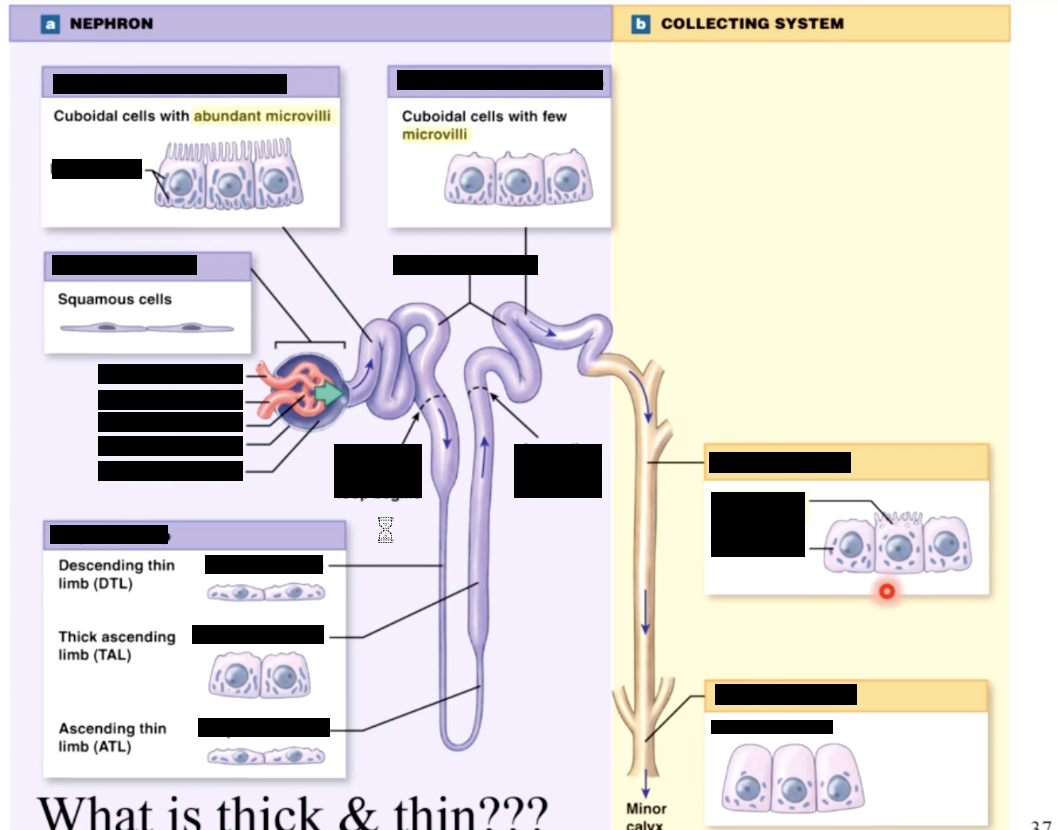
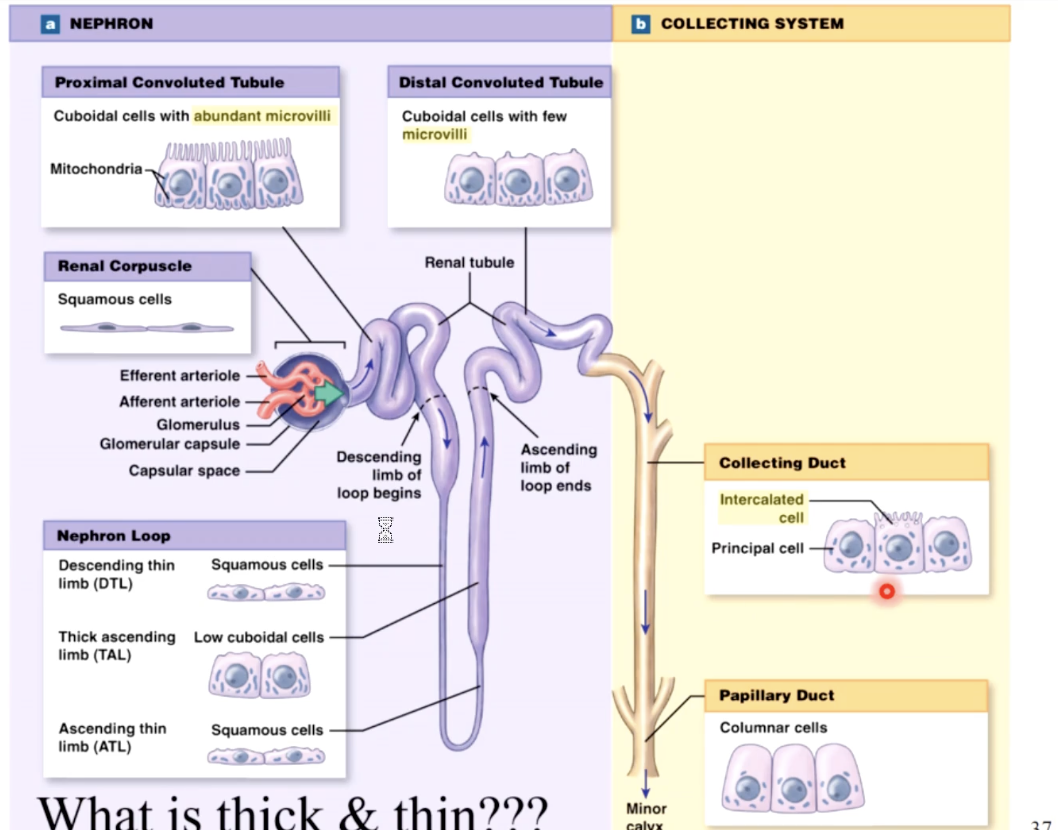
types of intercalated cells and principal cells
type A intercalated - secrete hydrogen, reabsorb HCO3
type B intercalated - secrete HCO3, reabsorb hydrogen (H)
principle - secrete K, reabsorb H2O
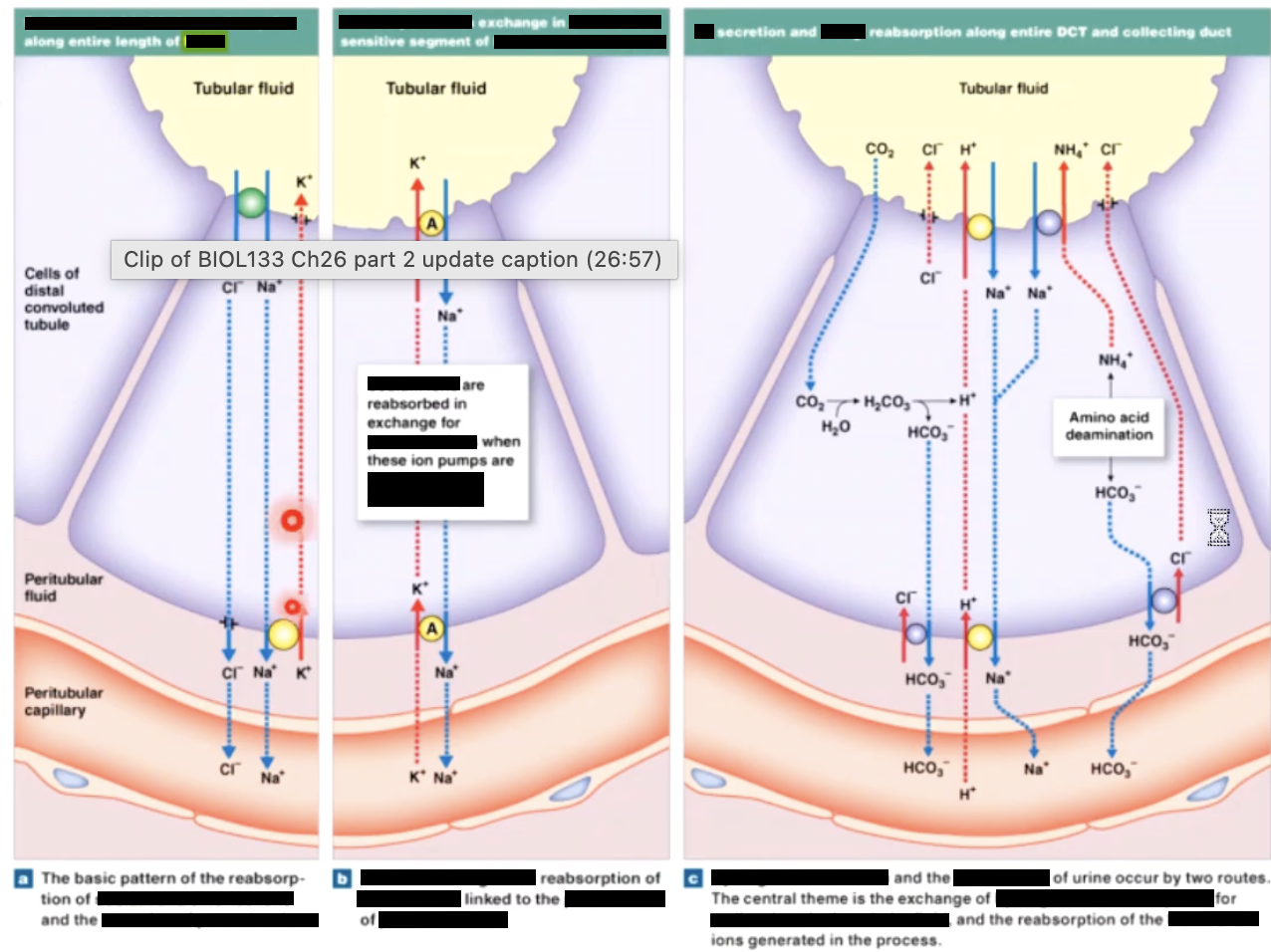
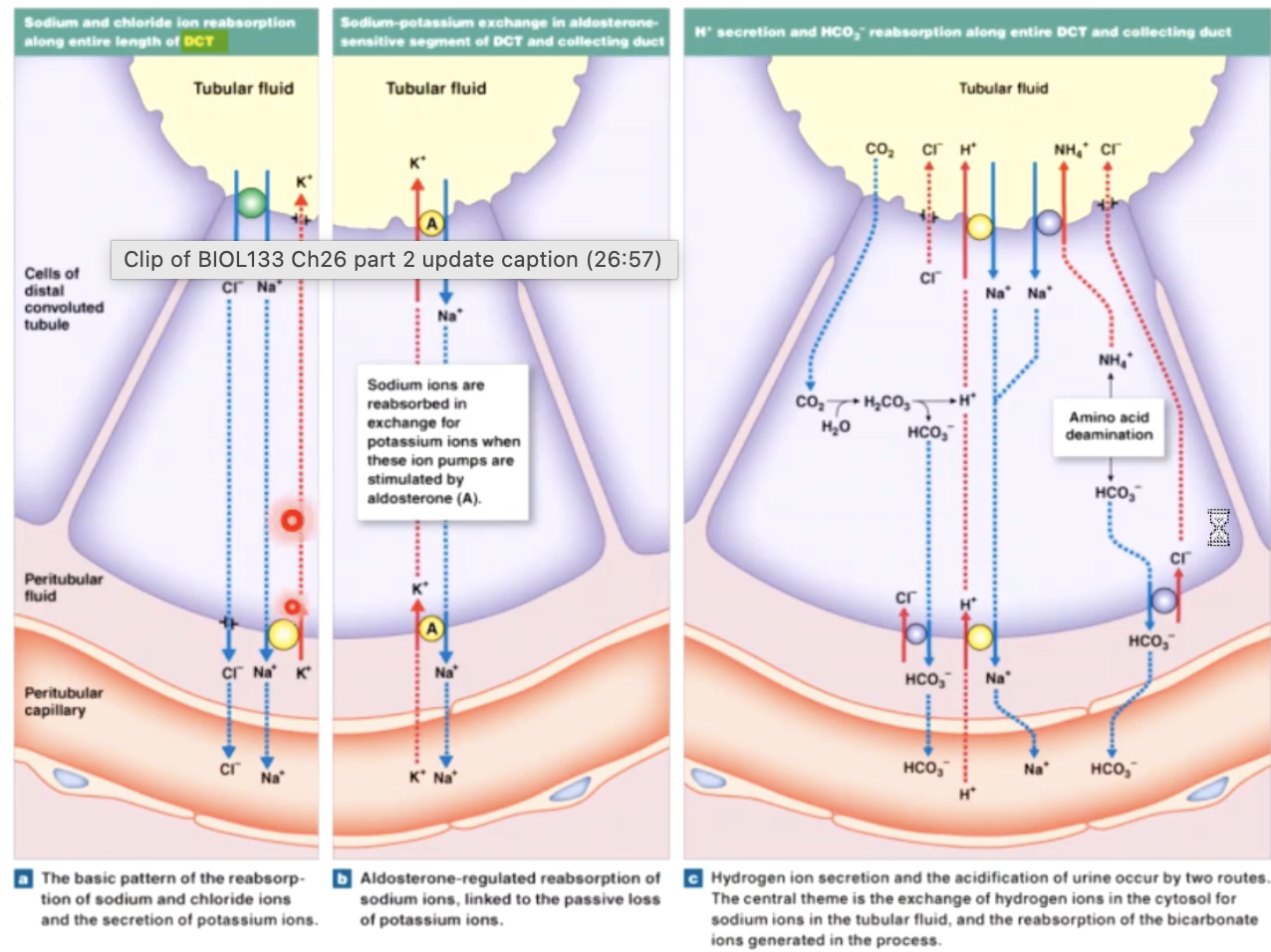
aldosterone and ADH
both aldosterone and ADH (vasopressin) exert the majority of their effects on the collecting ducts the kidneys
Aldosterone is released from the adrenal cortex in response to angiotensin II, it increases the production of epithelial sodium channel (ENaC). This increases the sodium absorption from the collecting duct, water follows osmotically through aquaporin-1
ADH is released by the posterior pituitary in response to high extracellular fluid osmolarity or low BP. ADH causes a a vesicle bound aquaporin-2 to move to the plasma membrane and increase the absorption of water
renal control of acid base status
The proximal tubule cells utilize the enzyme carbonic anhydrase to help regulate the body’s pH
this enzyme converts CO2 and H2O into H+ HCO3, and visa versa
CO2 from the peritubular capillaries for from filtered HCO3 is converted into H and HCO3 within the cells
H+ is then secreted into the filtrate through the Na+/H exchanger, while HCO3 is reabsorbed
This system is regulated by the pCO2 in peritubular capillaries - if pCO2 is elevated, more H+ is secreted and HCO3 absorbed.
K+ tends to be conserved when more H+ is secreted. If pCO2 is decreased, less H+ is secreted and HCO3 absorbed
glomerular filteration rate
amount of filtrate both kidneys produce each minute
averages 125mL/min
about 10% of fluid delivered to kidneys leaves blood stream to become filtrate this is the basis of kidney function (health) tests
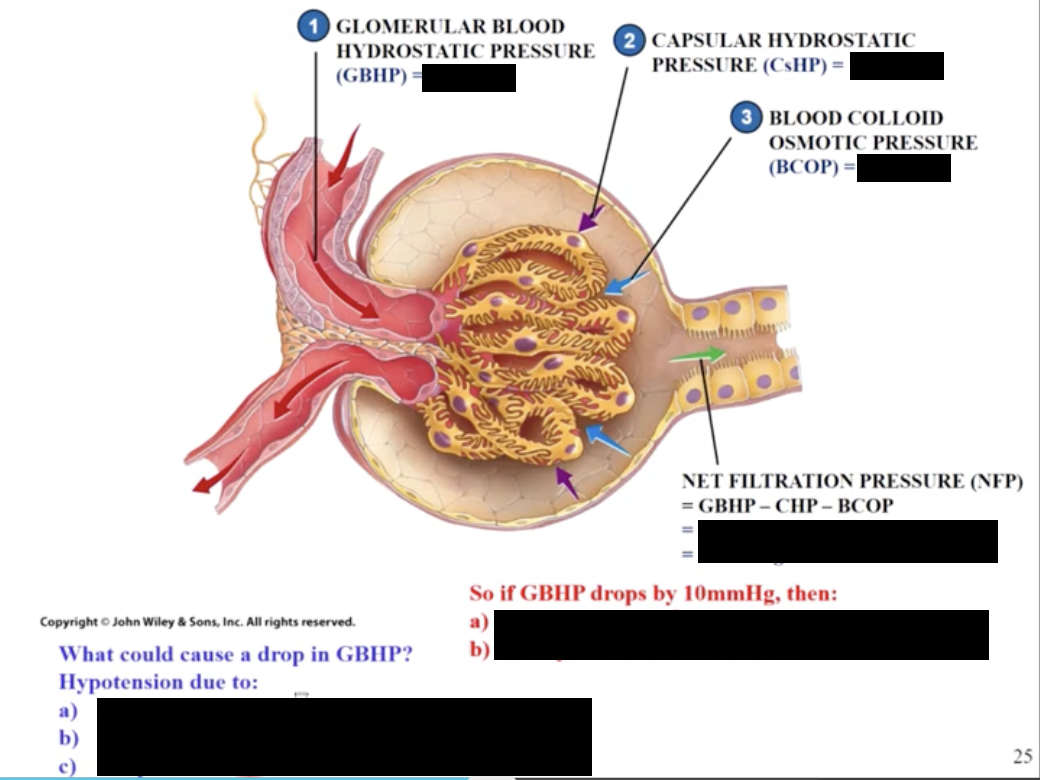
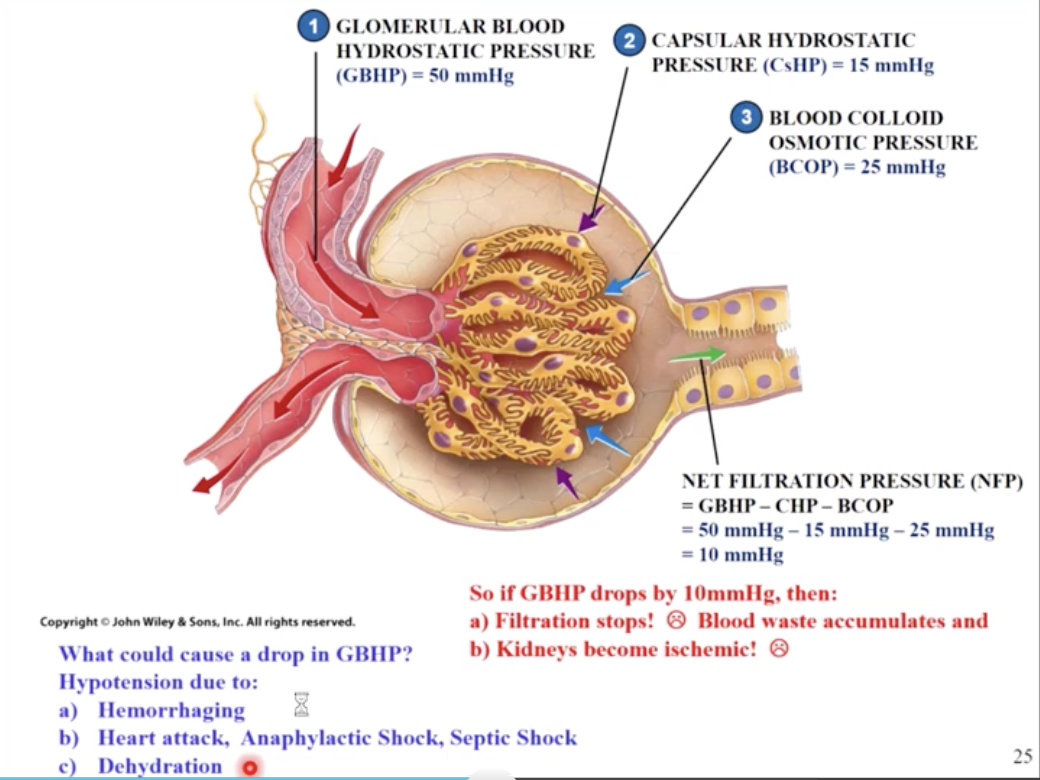
net filtration pressure (-10mmhg) determines GFR
if GHP drops from 50mmHg to 40mmHg then NFP=0 and GFR will be zero (no kidney filtration)
hypotension can cause cause a drop in GBHP
caused by hemorrhaging, heart attack, dehydration
if renal flow & GFR not restored, will lead to acute renal failure
creatine Clearance tests
compare the amount eliminated in urine with plasma concentration
ex: patient A: 84mg/h in urine and plasma creatine conc. is 1.4mg/dL, so
84/1.4 = 60dL/hr= 100mL/min
importance in maintaining GFR
the body needs to keep GFR of 125mL/minute to maintain adequate filtration of blood
GFR changes throughout the day
will increase if BP or BV increase (BP increase during exercise or stress, BV increase If over hydrated)
will decrease if BP or BV decreases (BP decreases in sleep and BV decreases if dehydrated)
body controls GFR using autoregulation, hormonal regulation and autonomic regulation
neural regulation
renal nerves
innervate kidneys & ureters (most are sympathetic nerves)
enter each kidney at hilum
follow branches of renal arteries to individual nephron
sympathetic innervation
adjusts rate of urine formation by changing blood flow and afferent and efferent arterioles
influences urine composition by stimulating release of renin
autoregulation
maintains adequate GFR despite changes in local blood pressure & blood flow
myogenic
involves changing luminal diameters of:
afferent arterioles - if renal BP increases, afferent vessel wall stretch induces smooth muscle to contract, causing vasoconstriction. If this doesn’t happen GHP will be too high & GFR will be too high
efferent arterioles maintain tone that is narrower that afferent arteriole so that kidneys GFR is 125mL/min
glomerular capillaries - if GFR is too high, intraglomerular mesangial cells contract to decrease both glomerular capillaries diameter & filtration slit size = decreased GFR
intraglomerular control diameter of glomerular capillaries and size of filtration slits. Also provide glomerular support (and capable of phagosizing debris) - made up of modified smooth muscle (actin)
hormonal regulation
activation of the Juxtaglomerular complex which is composed of
macula dense epithelia cells of DCT, near renal corpuscle (function as chemoreceptors or baroreceptors)
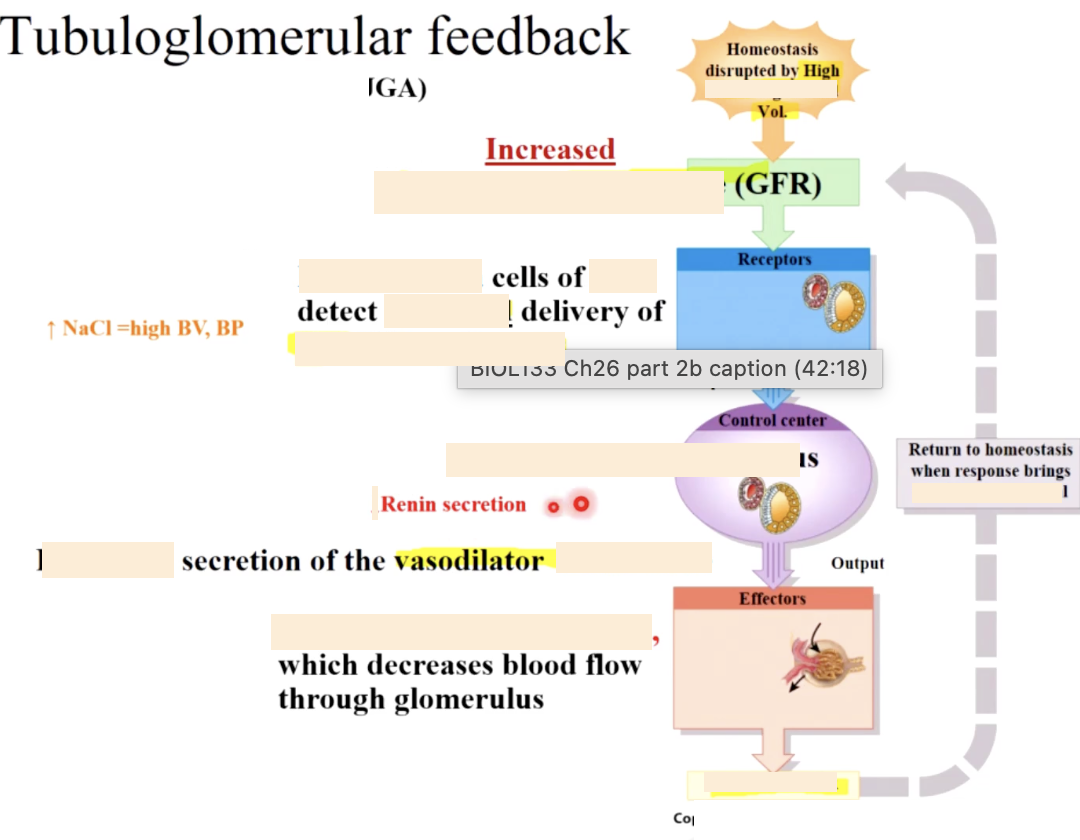
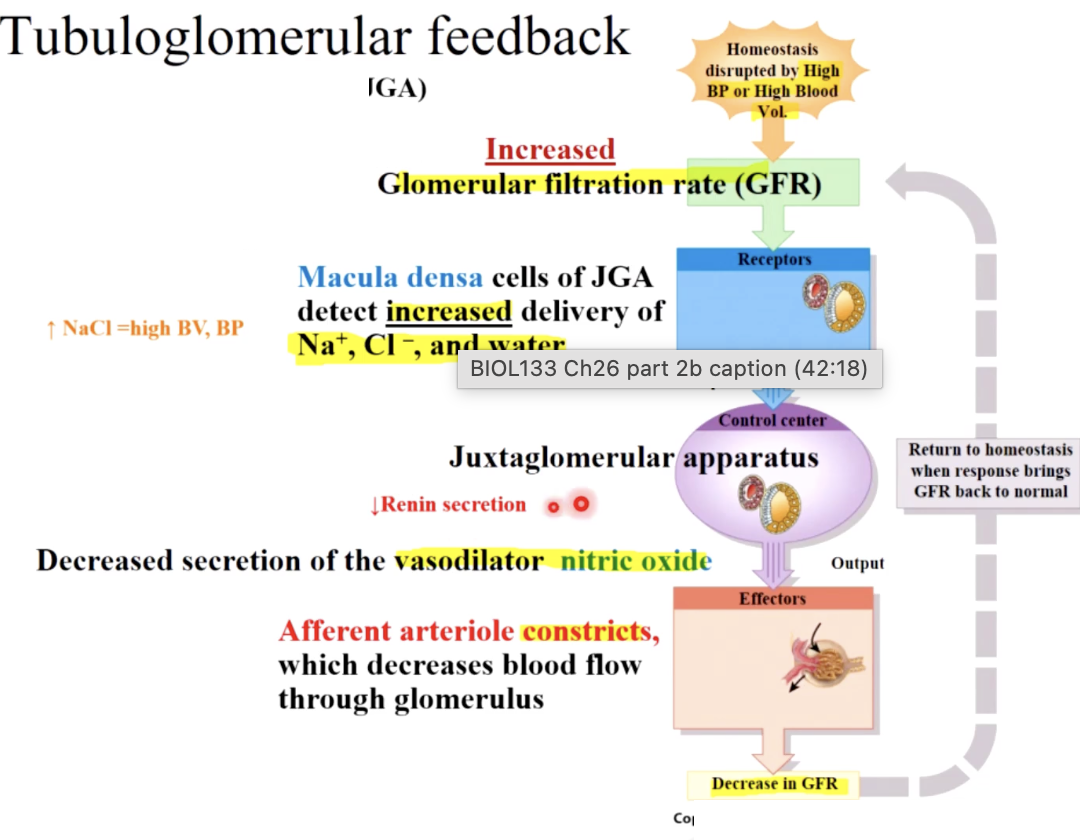
juxtaglomerular cells - smooth muscle cells in afferent arteriole wall (function as baroreceptors and secrete renin & EPO), generate tubuloglomerular feedback
extraglomerular mesangial cells - located between afferent artioles, provide feedback control , but exact function is unclear
activation of RAAS (renin-angiotension-aldosterone system)
how does JGc help control urine concentration
also helps control BP and BV
1- the macula dense is part of the distal convoluted tubule & senses Na and Cl conc. changes in the filtrate, & can dilate or constrict the arterioles appropriately
1 - a decrease in BP or BV causes a decrease in GFR resulting in less filtration and a decrease in salt conc. in the filtrate (because there is more time for reabsorption)
2- the macula dense will sense this then:
trigger dilation of affront arteriole to increase GFR
trigger the juxtaglomerular cells lining the affront arteriole to produce & release renin. JG cells function as baroreceptors and can also release renin independently of the macula densa
2 - The (granular) juxtaglomerular cells secrete EPO & renin in response to low BP or macula densa or SNS stimulation
EPO stimulates maturation of RBC ‘s, which increases BV and BP
Renin catalyzes the activation of angiosten I, which is converted to angiosten II. Ang. II stimulates ADH & aldosterone increases H2o & NaCl reabsorption into the blood. This increases BV & BP, vasoconstriction increases BP
Juxtaglomerular apparatus
made up of 3 cell types
extraglomerular mesangial cells
macula densa cells
juxtaglomerular cells
Regulating MAP affects GHP & GFR
GFR can be overridden by SNS and RAAS
normally autoregulation can alter GHP to keep GFR constant however
if hemorrhaging - BP is very low (less than 80mmHg ) then blood will be shunted to vital organs and even lower renal blood flow and pressure may occur- which will damage kidneys if not rectified
ANP and BNP
they can both override autoregulation (myogenic & JGC) during extreme events (eg, hyponatremia due to over hydration)
Micturition sacral reflex
1 - stretch receptors in the bladder are activated & output is activated by sensory neurons to spinal cord, cerebrum & pons
2- PSNS nerves are stimulated and cause bladder detrusor muscle to contract (normally a sympathetic tone causes relaxation of detrusor and contraction of internal sphincter). normally voluntary motor neuron has constant tone stimulating contraction
3 - cerebrum determines if location is appropriate then stimulates pons to inhibit sympathetic output to detrusor & internal sphincter. Voluntary motor neuron to external sphincter stops firing so sphincter relaxes