general and oral pathology diagnostic processes and soft tissue tumors
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
diagnosis
the determination of the nature of a disease or condition;; an explanation for your findings
correct diagnosis→ most appropriate and effective treatment
diagnostic process
gathering information
analyzing information
establish a diagnosis or possible diagnosis
gathering information
patient chief complaint (primary symptom)
history of present illness
past medical history
medication and allergy
social/family history
physical exam
intra and extra oral examination
paraclinical/lab and imaging tests
biopsy
patient chief complaint
the primary symptom that a patient states as the reason for seeking medical care
history of present illness
following the chief complaint in medical history taking, a history of the present illness refers to a detailed interview prompted by the chief complaint or presenting symptom
a detailed chronological narrative, as much as possible in the patients own words, of the development of the current health problem from its onset to the present
past medical history
prior illness, their treatments and sequelae
medications/ allergies
list of medications taken at the time of diagnosis by patient
list of any allergy
social hisotry
marital status, past and present occupations, travel, hobbies, stresses, diet, habits, and use of tobacco, alcohol, or drugs
family history
present health or cause of death of parents, brothers, sisters, with particular attention to hereditary disorders
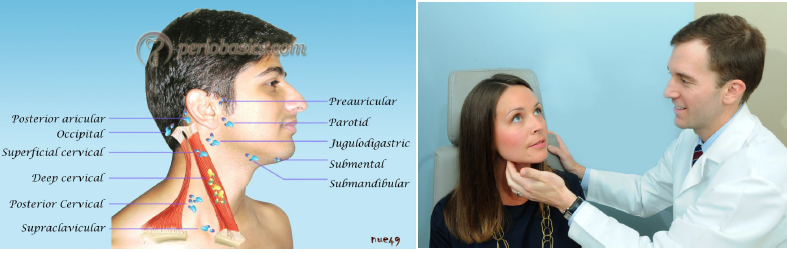
physical examination
examination by means such as visual inspection, palpation, percussion, and auscultation to collect information for diagnosis
very important to know normal anatomy and variations so that abnormalities are easily recognized
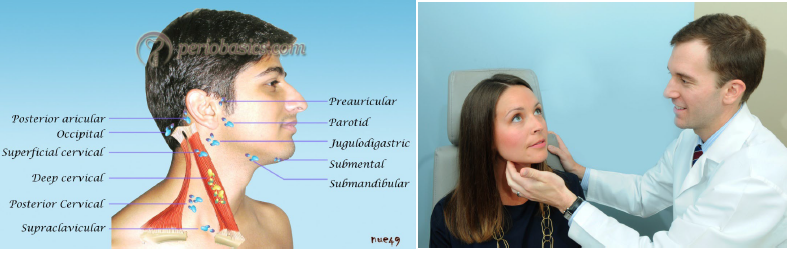
extraoral examination
observation the eyes and pupils
examination of the skin of head and neck for detection of any lesion
palpation of the head and neck lymph nodes for any induration, mobility, and tenderness of lymph nodes and lymphadenopathy
examination of thyroid gland
bilateral palpation of the temporomandibular joints and examination of the patient for any limitations in opening the mouth or for any joint sounds
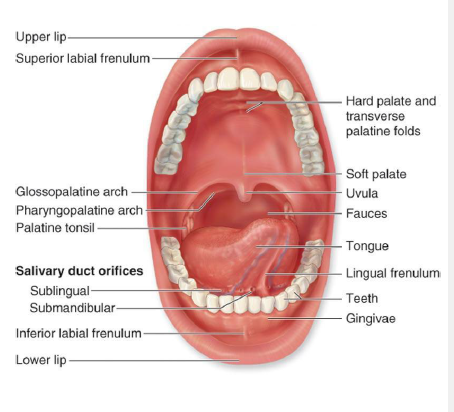
intraoral examination
oropharynx and tonsils examination
visualize and palpate the soft and hard palates and the maxillary tuberosity
stretch out the buccal mucosa and labial mucosa, visulaize and palpate for any abnormality
examine the mandible
floor of the mouth
tongue examination
attached gingiva
assess the amount and quality of the saliva (thick foamy saliva→ dry mouth)
evaluation of parafunctional habits (bruxism)
describing and recording lesions
size
color
site/location
distribution
and character should be noted
describing and recording the size of the lesions
record the dimensions of the lesion in mm or cm (don’t say small or large as they are too vague)
intraoral: use perio probe as ruler
extraoral: use flexible rulers

describing and recording the color of lesions
normal mucosa-like color, white (keratotic), red, black-brown, bluish-grey…
homogenous (even throughout) or variegated (uneven) color are one of the features distinguishing a nevus from melanoma

describing and recording the site/ location of lesions
be specific
give anatomic relationships (left buccal mucosa, anterior to parotid papilla)
left, right, anterior, posterior
superior, inferior, medial, lateral
facial, lingual
describing and recording the distribution of lesions
localized (found in one are only) or generalized (located in most of the tissues in one area)
single or multiple
in case of multiple lesions, being discrete and separate or being coalescing
margins: well defined or circumscribed vs poorly defined
describing and recording the character of lesions
flat, raised, or depressed
surface texture: smooth, rough (papillary, granular, shaggy, pebbly, ulcerated)
consistency on palpation: fluctuant (fluid filled), soft, doughy, rubbery, firm (fibrous), hard
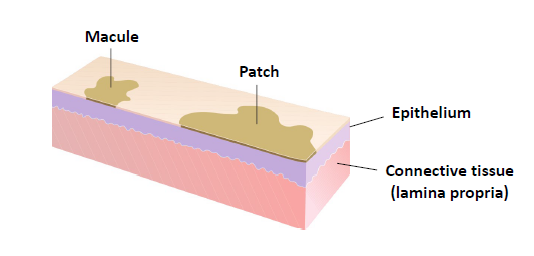
macule/ patch
a flat lesion differentiated from surrounding tissue by color alone
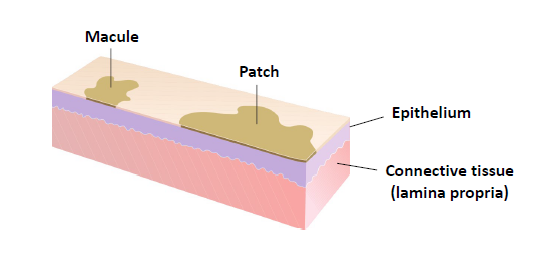
macule
less than 1 cm in diameter
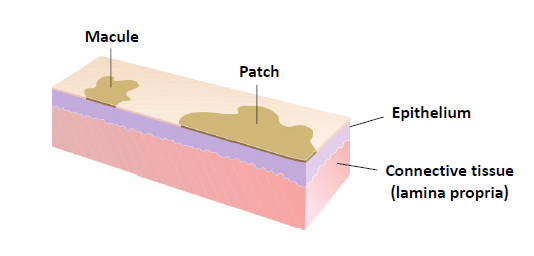
patch
more than 1 cm in diameter
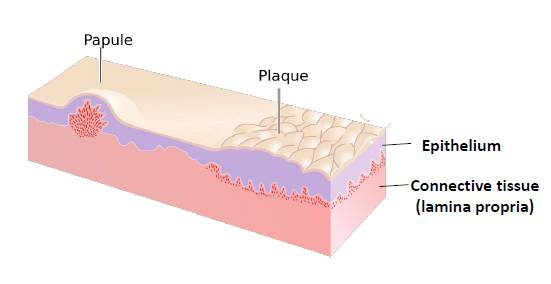
papule
a solid raised lesion less than 5 mm
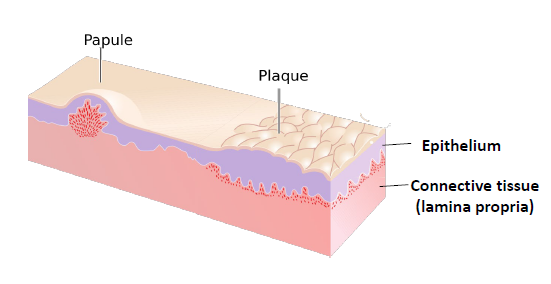
plaque
a solid, raised, flat topped lesion greater than 5 mm in diameter
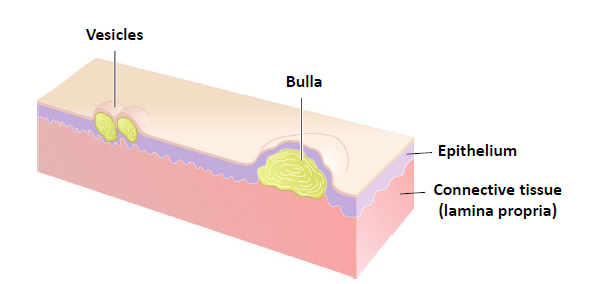
vesicle
an elevated lesions less than 0.5 cm in diameter, filled with a clear fluid. if larger than 0.5 cm, is called bulla
pustule
a raised lesion filled with pus

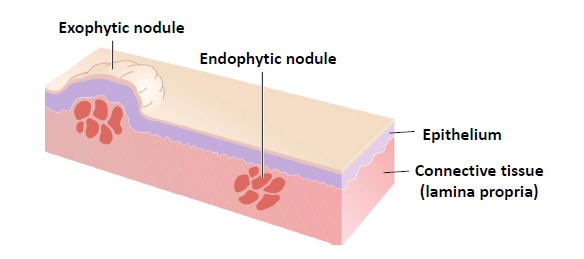
nodule
a slightly larger papule, less than 2 cm
anything larger may be called a tumor or mass
exophytic nodule, grows outward from the surface of the tissue
endophytic nodule, grows into the surrounding tissues and presents as palpable mass with or without any noticeable swelling
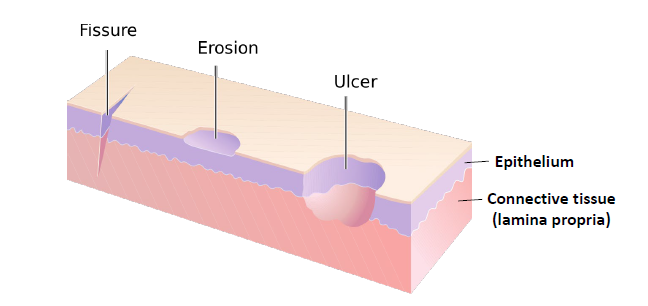
erosion
slightly depressed are of skin or mucosa in which part or all of the epidermis or epithelium has been lost
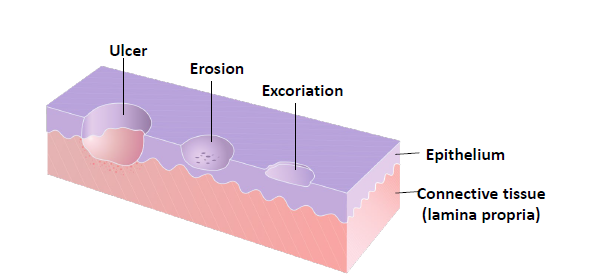
ulcer
loss of epithelium and underlying connective tissue
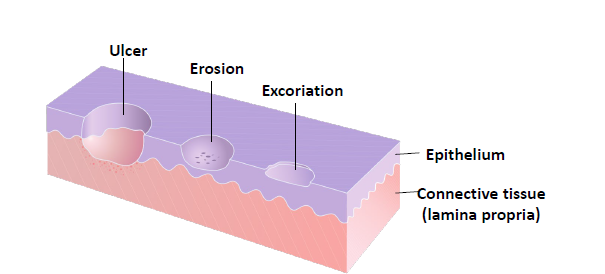
fissure
a linear cleavage of skin or mucosa which may extend into the dermis or underlying connective tissue
differential diagnosis
a list of possible diagnostic considerations
arranged in descending order of probability
1st on your list = most likely diagnosis
working diagnosis
tentative diagnosis; your clinical impression
the most likely consideration from the differential diagnosis
should be the first one listed on your differential diagnosis
paraclinical/lab and imaging tests
blood/ serum test (CBC.,…)
radiography/imaging (x-ray, CT, MRI, ultrasound…)
molecular/cytogenic tests (most of the times for confirmation of final diagnosis)
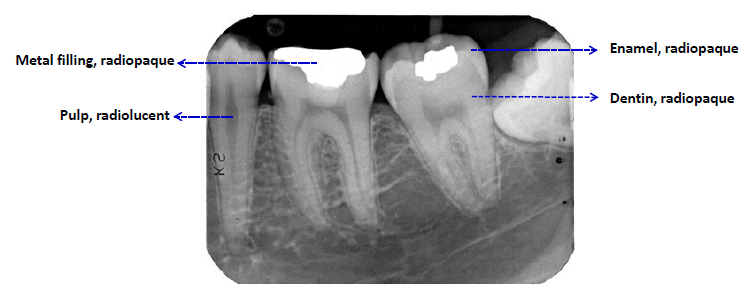
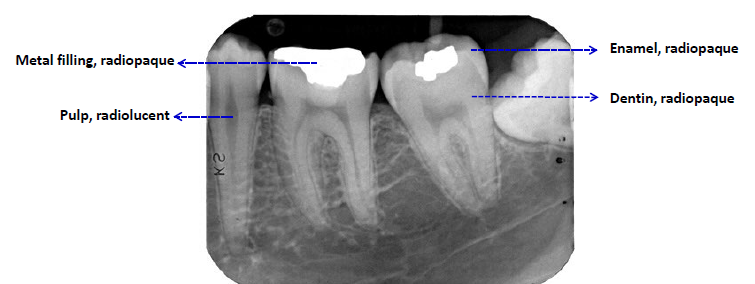
radiopaque or radiodense
stronger x-ray absorption
whiter/lighter apprearance
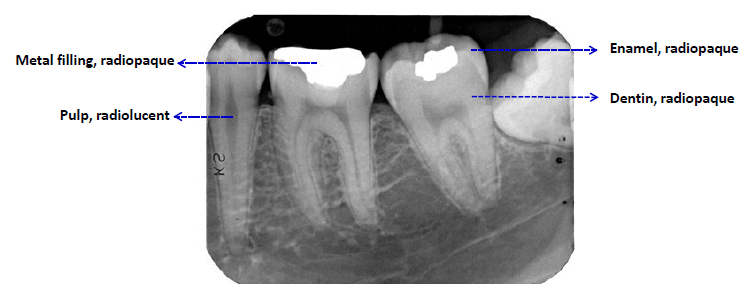
radiolucent
darker appearance (weaker x-ray absorption)
describing radiographic findings
localization: anatomic position, localized vs generalized, unilateral vs bilateral, single or multi
shape: round, ovoid, scalloped, irregular, etc
periphery (border): well defined vs poorly defined (invasive and malignant tumors)
internal structure: radiolucent (unilocular or multilocular, radiopaque, or mixed RL/RO)
effects on surrounding structures: resorption of teeth or expansion of bone, or resorption of cortex
serologic tests
CBC
urinolysis
detecting some compounds filtered out by the kidney such as hydroxyproline as a marker for bone destruction in Paget disease
microbiological cultures
to find appropriate antibiotics
antibody tests
such as SSA and SSB for Sjogren syndrome
DNA-PCR (polymerase chain reaction)
identifying some viruses such as HIV
ELISA
enzyme-linked immunosorbent assay
for detecting hormones, bacterial antigens, and antibodies
salivary function tests
for example in Sjogren syndrome
electromyography
for diagnosis of neurological and neuromuscular problems such as TMJ disorders
biopsy
the process of taking a sample of living tissue for histopathologic examination
gold standard for definitive diagnosis
tissue specimen is process into glass slides and histologic features are evaluated microscopically
biopsy methods
excisional biopsy
incisional biopsy
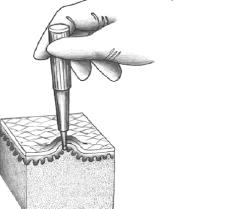
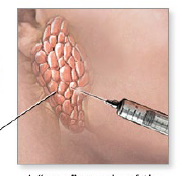
needle biopsy
fine needle aspiration
excisional bipsy
total removal of lesions, either as a surgical biopsy or a punch biopsy
incisional biopsy
representative sample of the lesion either as surgical biopsy or punch biopsy
needle biopsy
using a large-bore needle
fine needle aspiration
using a small diameter needle
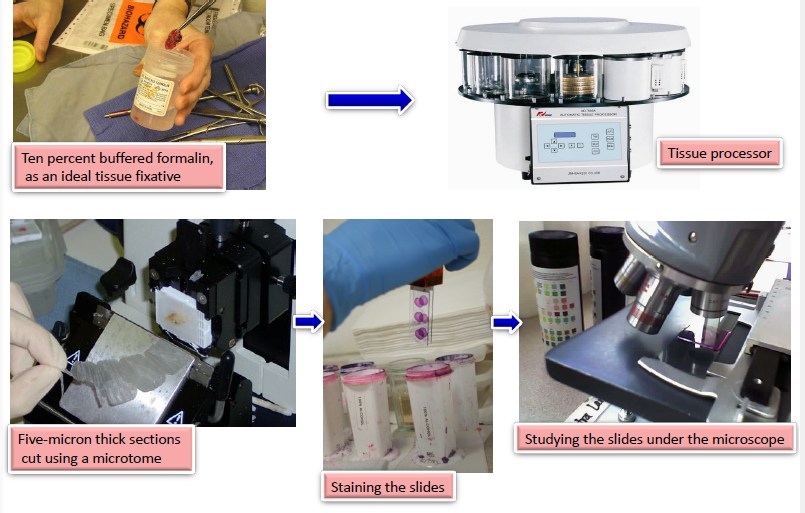
biopsy and tissue processing
ten percent buffered formalin, as an ideal tissue fixative → tissue processor→ five micron thick section cute using a microtome→ staining the slides→ studying the slides under the microscope
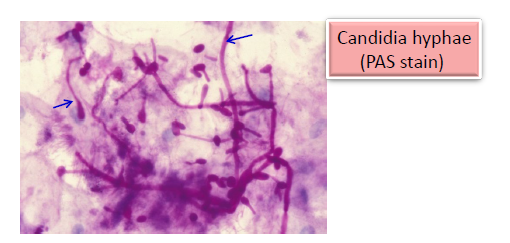
exfoliative cytology - brush biopsy
a cytologic smear
scraping surface cells form the skin or mucous membranes
non invasive procedure, no need for anesthesia
oral cytological smears, helpful in diagnosis of candidiasis
brush biopsy, collecting cells for cytological evaluation
limited conclusions about the diagnosis
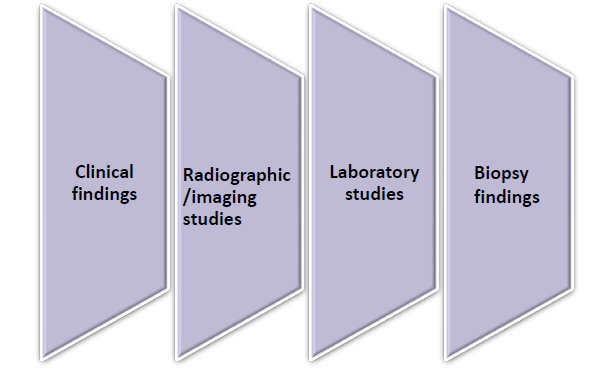
final diagnosis
determined after analysis of all the diagnostic information, including
clinical findings
radiographic/ imaging studies
laboratory studies
biopsy findings
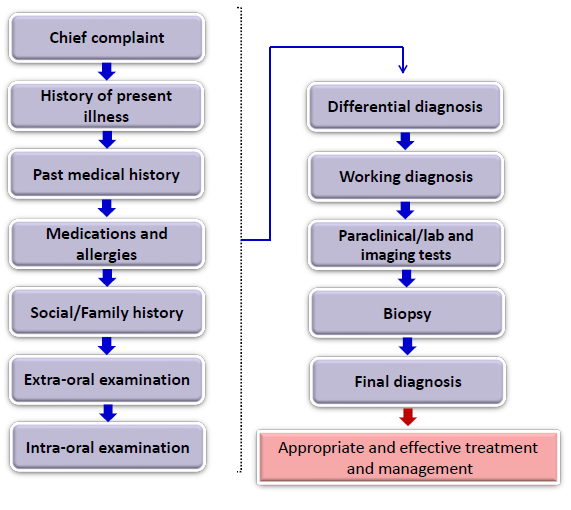
summary of diagnostic process
chief complaint
history of present illness
past medical history
medications and allergies
social/ family history
extra-oral examination
intra-oral examination
differential diagnosis
working diagnosis
paraclinical / lab and imaging tests
biopsy
final diagnosis
appropriate and effective treatment and management
reactive/ inflammatory conditions
very common lesions
patient may have local factor such as bacterial plaque or food retention that tissue has overreacted to
fibroma
giant cell fibroma
pyogenic granuloma
peripheral giant cell granuloma
peripheral ossifying fibroma
benign neoplasms of adipose tissue
lipoma
benign neoplasms of neural origin
neurofibroma/ neurofibromatosis
schwannoma
granular cell tumor
congenital epulis
benign neoplasms of vascular origin
hemangioma
lymphangioma
vascular malformation
fibroma
most common “tumor” of the oral cavity
not a true neoplasm- inflammatory/ reactive tumor
reactive lesion, secondary to trauma or chronic irritation
buccal mucosa as the most common location
labial mucosa, tongue, and gingiva
conservative surgical excision as the treatment, recurrence is rare

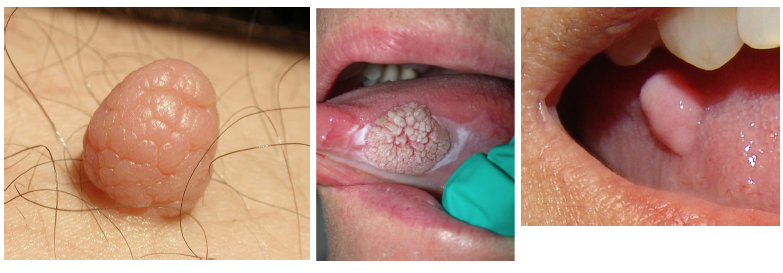
giant cell fibroma
a fibrous tumor with distinctive clinicopathologic features
may be clinically mistaken for a papilloma
50% of cases on the gingiva
tongue and palate as other sites of involvement
clinically may be misdiagnoses as squamous papilloma

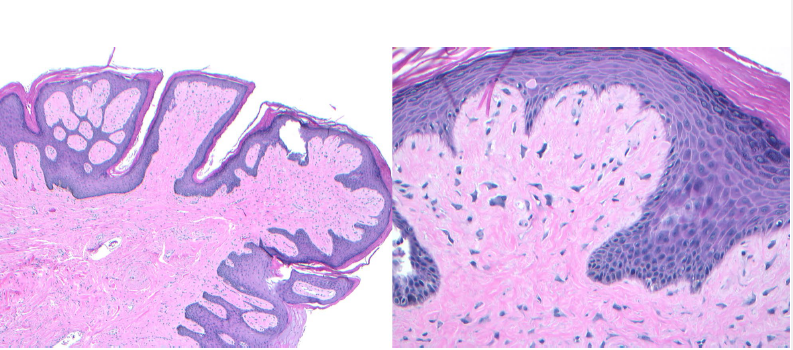
giant cell fibroma histopathologic features
papillary surface
presence of giant stellate-shaped fibroblasts in the lamina propria
giant cell fibroma treatment
simple, conservative excision
recurrance is rare

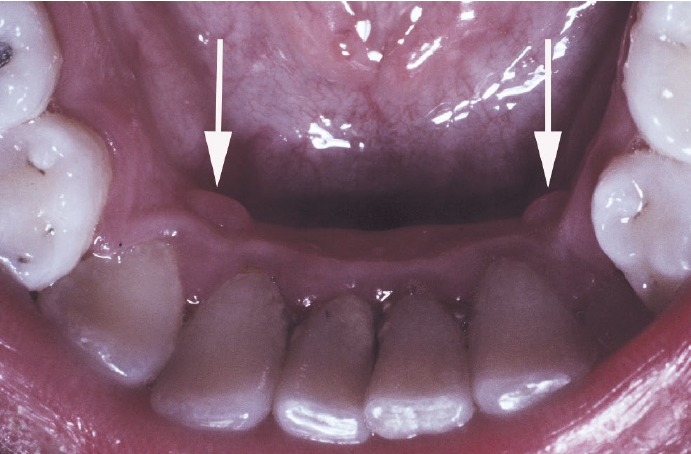
restrocuspid papillae
a normal anatomic variation
on the gingiva lingual to the mandibular cuspid, frequently bilateral
microscopically like giant cell fibroma
no need for treatment
pyogenic granuloma
a common non-neoplastic proliferation of granulation tissue
a misnomer (not pyogenic, not granuloma)
response to local irritation or trauma
usually ulcerated
gingiva is the most common site
common during pregnancy
easily bleeds

pyogenic granuloma treatment
conservative surgical excision with removal of any local factors
lesions associated with pregnancy may spontaneously regress postpartum
recurrences occur due to remaining local factors (calculus)

reactive lesion
fibroma is considered a
gingiva
most common site for pyogenic granuloma
peripheral giant cell granuloma
relatively common reactive lesion of the gingiva
histologically identical to the central giant cell granuloma
bluish-purple lesion
radiographic- may cause “cupping” resorption (saucerization)
almost exclusively on the gingiva or edentulous alveolar ridge

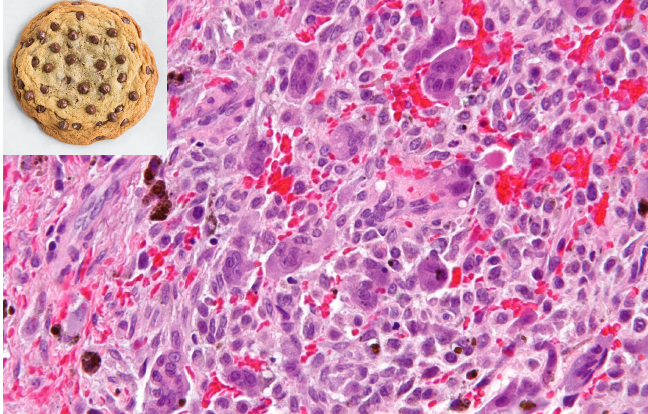
peripheral giant cell granuloma histopathologic features
chocolate chip cookie like histology
peripheral giant cell granuloma treatment and prognosis
local excision down to the underlying bone
removal of local factors
approximately 10% recurrence rate
peripheral ossifying fibroma
not confused with “peripheral odontogenic fibroma”
relatively common reactive lesion, probably arising from periodontal ligament
unrelated to the central ossifying fibroma
exclusively on the gingiva
maxilla> mandible
frequently ulcerated

peripheral ossifying fibroma treatment and prognosis
local excision down to the periosteum
elimination of local factors or irritants
approximately 16% recurrence rate
gingiva or edentulous alveolar ridge
peripheral giant cell granuloma occurs almost exclusively on
lipoma
benign tumor of fat
although rare in the oral/ maxillofacial area, the lipoma is the most common mesenchymal neoplasm
unrelated to metabolism/ body fat
F>M
soft nodule, most
commonly involving the buccal mucosa
normal or yellow in color

lipoma treatment and prognosis
conservative surgical excision
recurrence is rare
neurofibroma
as the most common type of peripheral nerve neoplasms
a mixture of cell types, including Schwann cells and perineural fibroblasts
skin as the most frequent location
tongue and buccal mucosa as the most common intraoral sites
on rare occasions, the tumor can arise centrally within the bone
solitary or syndrome-related
multiple lesions associated with neurofirbomatosis

neurofibromatosis type 1
one of the most common autosomal genetic problems that affects humans
occurs at a frequency of approximately 1 in 3,000 live births
approximately half are transmitted as autosomal dominant trait; other half appear to be new mutations
high variable gene expression- some cases are very mild, others are quite severe
variety of manifestations, both cutaneous and oral

neurofibromatosis type I skin lesison
cafe-au-lait spots
light brown (color of coffee with milk) macules with smooth (coast of California) borders
usually 6 or more greater than 1.5 cm
axillary freckling
lisch nodules (benign pigmented nodules of iris)
multiple neurofibromas

multiple neurofibromas
small, discrete lesions or massive pendulous ones
neurofibromatosis type 1 skin lesion

neurofibromatosis type 1 management
treatment consists of removing traumatized neurofibromas or disfiguring lesions
genetic counseling
follow for potential malignant transformation (malignant peripheral nerve sheath tumor)
schwannoma
benign neural tumor of shwann cell origin
uncommon, but often involved the head and neck
young and middle aged adults
slow growing
variable symptoms
oral tumors most commonly involve the tongue and may arise within the bone, causing an expansile, unilocular radiolucency

schwannoma treatment and prognosis
surgical excision
recurrence is not expected
malignant transformation is rare
malignant peripheral nerve sheath tumor, malignant schwannoma, neurofibrosarcoma
neurofibromatosis type 1
which is associated with cafe-au-lait spots and lisch nodules
granular cell tumor
a benign soft tissue neoplasm showing significant predilection for oral cavity
of schwann cells origin
tongue as the single most common site of involvement
treatment: conservative surgical excision

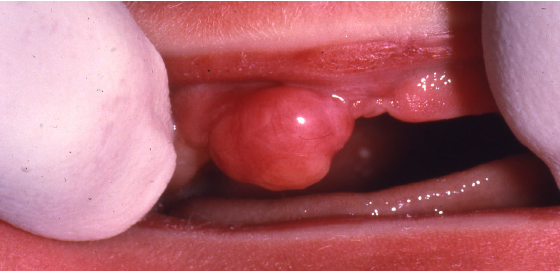
congenital epulis
rare lesion of underdetermined histogenesis
found at birth on the maxillary ridge of girl babies
smooth surfaced, often pedunculated, lobulated nodule
vary in size
the cells are granular histopathological
benign neoplasms of vascular origin
hemangioma
lymphangioma
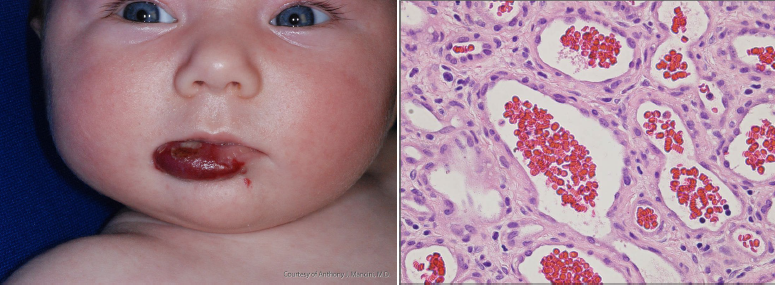
hemangioma
most common soft tissue tumors of infancy
prevalence of 1-2% in neonates and 12% by the age of 1 year
rapid postnatal growth for 8-12 months, followed by slow regression for the next 1-5 years
head and neck as most common location
capillary, cavernous, and juvenile as subtypes
arterior venous (vascular) malformations
uncommon errors on vascular morphogenesis
distinct from hemangioma
not a neoplasm
present at birth but may not clinically evident
consist of abnormal channels lined by normal endothelium
classified as arterial, venous, capillary, lymphatic, or combinations

vascular malformations
are present at birth
no rapid increase in size
no involution

hemangioma
not always present at birth
rapid increase in size
involution

presence at birth and involution
key distinguishing feature between infantile hemangioma and vascular malformation
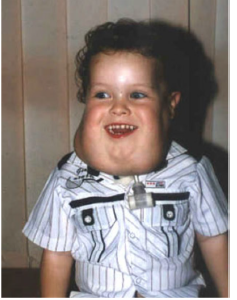
lymphangioma
benign lymphatic counterparts of hemangiomas
simple capillary lymphangiomas
cavernous lymphangiomas (cystic hygromas)
oral lesions: tongue is the most common sites with a “frogs egg” appearance
deeper tumors appear as ill-defined masses
alveolar lymphangiomas

simple (capillary) lymphangiomas
raised lesions, up to 1-2 cm, predominantly seen in head, neck, and axillary subcutaneous tissues
cavernous lymphangiomas (cystic hydromas)
found in the neck or maxilla of children up to 15 cm in size
75% occur in head and neck
lymphangioma treatment and prognosis
surgical excision when appropriate
recurrence common
cystic hygroma usually has a lower recurrence rate