Looks like no one added any tags here yet for you.
normal BP
< 120 and < 80
elevated BP
120-129 or <80
stage 1 HTN
130-139 and 80-89
stage 2 HTN
≥ 140 and ≥ 90
determining BP stage
go with the higher number
modifiable risk factors for HTN
Diet
Salt
High sodium
Processed foods
Smoking
Alcohol
non-modifiable risk factors for HTN
Age
Genetics
Family history
Race
secondary HTN
Results from another disease
kidney disease
Side effects of medications
Steroids
Immunosuppressants
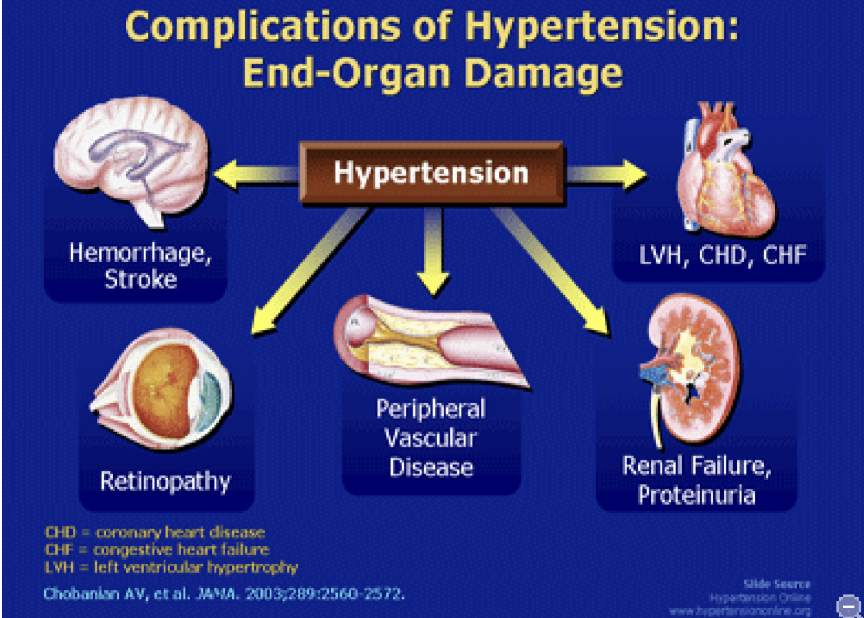
complications of HTN
Prevent end stage organ damage
Renal failure
HTN treatment
Lifestyle modifications
2300mg of Na
AHA - < 1500
Average intake is 3900
Exercise 150 mins/week
BP goals <130/80 if they are HTN
Lose weight
Eat fruits and veggies
moderate ETOH intake
DASH diet
High in grains and fruits
Low in fat
first line treatments
Thiazide –type diuretics
do not give with kidney disease
Calcium Channel Blockers
Limit rate at which Ca flows into arterial walls
Relaxes and widens vessels
Angiotensin-converting enzyme (ACE) Inhibitors
Interfere with renin-angiotensin mechanism
Reduce ace activity
Angiotensin Receptor Blockers (ARBs)
Block action of angiotensin on vessels and other tissues
never give ACE and ARBs together
beta-blockers
given with heart disease
treatments for different stages
Stage 1 hypertension
Single antihypertensive drug
Blood pressure goal of <130/80
Stage 2 hypertension
Combination of 2 first-line antihypertensive drugs with an average BP more than 20/10 mm Hg above the BP target
malignant HTN
Sx = blurred vision, headache, confusion
Or may have NO symptoms
Requires immediate treatment
Target BP <160/<100 short term
Mean arterial pressure should not be lowered more than 10% -20 % first hour
Then approximately 25% during next 23 hours
Want to take it down slowly to avoid causing ischemia
side effects of HTN meds
All cause fatigue
ACE
Cough (chronic and dry)
Beta blockers
ED
malignant HTN basics
Adverse outcomes
Cerebral edema
Retinal hemorrhage
Acute renal damage
Causes
Unknown
Pt. abruptly discontinues meds
Preeclampsia of pregnancy
Therapy = medications immediate actions
Medications may include:
Nitrates
Clonidine
Captopril
Furosemide (Patients that are fluid overloaded)
Monitor BP q 5-30 minutes
Bedrest, quiet environment
pre op teaching
Better post op outcomes with teaching
IS
cough/deep breath
pain management
post-op drains
compression devices
mobility exercises
foot
leg
why mobility
prevent Constipation
Increase circulation
improve Respiratory status
prevent DVT
NPO
No gum
No hard candy
NPO guidelines
Fasting Period for healthy patients of all ages undergoing
elective surgery (not including women in labor)
Clear liquids-2 hours (e.g. water, fruit juices without pulp,
carbonated beverages, clear tea, and black coffee)
Breast milk-4 hours
Infant formula-6 hours
Nonhuman milk-6 hours (amount needs to be considered)
Light meal-6 hours (e.g. toast and clear liquids)
Meals that include fried, fatty food, meats-8 hours
Guidelines does not guarantee complete gastric emptying
emergent
Life or death situation
Level 1 trauma needs to have an OR ready to go with staff
Severe bleeding, trauma, gunshot wounds, subdural hematomas
urgent
Needs prompt attention
24-30 hours until surgery becomes emergent
Acute cholecystitis (inflamed gallbladder), Fractures, abscesses
elective
Patient should have surgery but failure to would not have dire consequences
Cysts, hernia repair
required
Needs the surgery but can be done in weeks and months
Needs it done before it can cause extreme health issues
Prostate hyperplasia, breast mass, thyroid disorders
optional
cosmetic
pain management
Teaching pain communication skills preoperatively results in greater pain relief
Explain use of pain scale preoperatively
Instruct patient to ask for pain medication as frequently as needed for pain relief
Very subjective
Cannot compare two patient's pain
Ask what an acceptable pain level
PCA pump
Patient controlled analgesia
Self-medicate
How much it can give them in a single dose, over a specific time frame
Need to monitor respiratory status
Administer Narcan to reverse
Patient needs to be cognitively intact enough to give themselves their pain meds
preop holding area
Upon arrival to holding area, patient checked in by preop holding area nurse
Two identifiers used to identify patient
Verification of
correct person
correct site
correct procedure
joint commission
Universal Protocol for Preventing Wrong Site, Wrong Procedure and Wrong Person Surgery
Requirements
Pre-procedure verification
Mark the Procedure Site
Time Out
2004- Pennsylvania Patient Safety Authority initiated mandatory wrong-site surgery reporting
PACU assessment
ABC, LOC, Vital Signs
Drains, Dressings
Fluids, Pain, Nausea
Assessing the patient
Maintaining a Patent Airway
Maintaining Cardiovascular Stability
Pain Relief
Stable vital signs, pain controlled
Other dependent on type of surgery
neuro assessment
Monitor the patient’s neurological status
Observe for ability to maintain airway
Patient may be sedated but should be easy to arouse by verbal stimuli
Check patient’s orientation level (person, place, time)
time out
Prior the starting the procedure
Standardized throughout the hospital
Initiated by a designated member of the team.
Involves all the immediate members of the procedure team.
Involves interactive verbal between all team members
Any team member can express concerns about procedure verification
It has a defined process for reconciling differences in response.
During the time-out all other activities are suspended
CV assessment
Monitor heart rate and regularity.
Monitor Blood pressure
Can be affected by
Pain
Anesthesia
respiratory assessment
Observe patients' ability to maintain airway
Observe patient’s respiratory rate and depth
Monitor oxygen saturations with pulse oximeter
O2 delivery systems
Nasal cannula
2L = 20%
2-6L
Higher concentrations need to be humidified
Can dry out lung secretions, and airway
Face mask
40-60% at 5-8L
Need at least 5L so they do not re-inhale their CO2
Switch to aerosol face mask
Nonrebreather
Last ditch effort before intubation and CPAP
At least 10L
atelectasis
Part of lung becomes airless and collapses.
Causes
Patients are not taking deep breaths
Respiratory depression from pot op opioids
Pt not moving
Symptoms
Decreased breath sounds
Decreased sats
Anxious
No pain
Treatment
Get them up and moving
Deep breathing exercises
IS
pneumonia
3rd most common post op infection
Cause
Microbial infection
Symptoms
Increase in WBC
Fever
Chills
Chest pain on inspiration
Decreased breath sounds
Decreased sats
hyperthermia
Cause
Early – body inflammatory response to surgery
Will resolve in 2-3 days
Serious complications
UTI
Pneumonia
Surgical site infection
Intervascular catheters
thrombitis
pain
Have to know patients pain level
Increase HR and BP
DVT
Symptoms
Circumference will be bigger
Pain
Redness
Warm
Tenderness
Nurse Interventions
Stop SCDs
Have pt remain in bed
Call MD for doppler studies
assess lungs
prevent clotting
Low molecular weight
Enoxaparin (lovenox)
Unfractionated heparin
SCDs
Compression garments
Ambulation
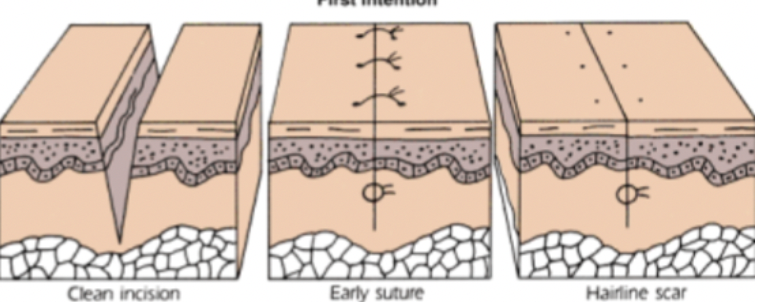
first intention
surgical site
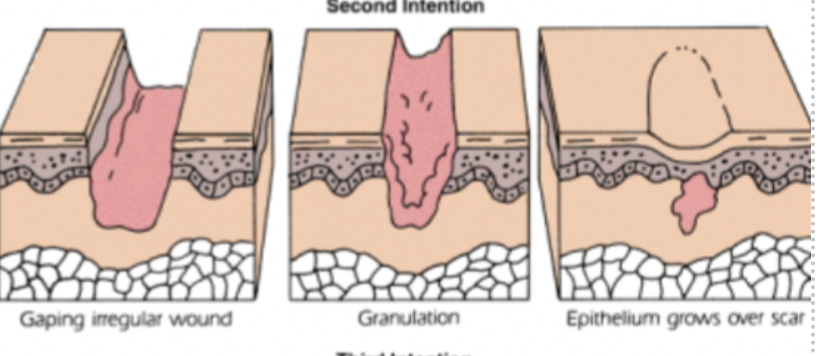
second intention
Seen with abscess
Pressure ulcer
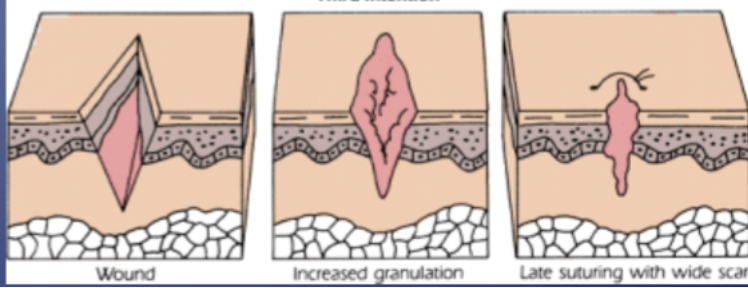
third intention
Delayed closing
Granulation starts and then closure
dehiscence
Incision opens up
RF
Obesity
Poor nutrition
Diabetes
Old adults
Steroids
Interventions
Let physician know
Not emergent unless wide open
Monitor for expansion
Monitor for infection
Use binder for abdominal support if abdominal
evisceration
Emergent
Organs come through incision
Intervention
Notify MD immediately
Sterile saline and sterile gauze
Soaked in NS
Put dry dressing over sterile gauze
Make sure they have patent IV
Low fowlers if abdominal (knees up)
surgical infections
Teach pts what to look for
Can educate while monitoring incision
Approximated well
Its closed
Signs and symptoms
Increase WBC
Purulent discharge
Fever
Warm
Red
Swelling
Odor
surgical dressings
First dressing is done by surgical team
Post first change will be the nurse
Sterile technique
Protect incision site
Absorb drainage
Physical and mental comfort for pt
Document amount of drainage
Color of drainage
Signs of infection
Dehiscence
Odor
fluid volume deficit
Loss > 500 need blood or surgery
Causes
N/V
NG tube
Decrease in vascular volume
interventions
Lower HOB, then vitals, Increase perfusion
Then call MD
And ask for fluids
Oral replacements are preferred
May need IV fluids (isotonic in vascular space)
Hgb 7 or below – give blood
Teach about sitting on edge of bed and go slow when OOB
Monitor BUN, Cr, electrolytes, hct, Hypokalemia, hyponatremia, Urine output
Good IV access
urinary retention
240mL in 8 hours
May occur due to:
Anesthetics, anticholinergic drugs, opioids
Pain
Difficulty in using bedpan or urinal
Can be mental
How to know its retention not deficit
Bladder scan
Do not need doctor's order
More than 400mL ask MD for a straight cath
Nursing Interventions
Bladder scan
Straight cath
constipation
Manipulation of abdominal organs may cause loss of normal peristalsis for 24-48 hours
Anesthesia and opioids decrease peristalsis
Immobility decreases peristalsis
Can have paralytic ileus with liquid stool
Interventions
Encourage fluids
Eary ambulation
Stool softeners
Notify MD if BS are present but no BM
sodium
Normal range: 135- 145 mEq/L
Recommended daily intake:
CDC dietary guidelines < 2300
American Heart Association < 1500mg
1 tsp is 2300mg
hyponatremia
Results in
Swelling of cells
Cells have higher concentration of sodium than vascular space
Depletional (Excess sodium loss)
Kidney disease
Adrenal insufficiency
Diuretics
N/V
GI suction
Repeated tap water enemas
Excessive sweating
Dilutional (Excess water gain)
HF
Liver disease
Hypotonic IV fluids
Self-induced water intoxication
hypernatremia
Causes
Water deprivation
Elderly
Babies
Neurological disorders
Stroke
Water loss
Fever
Burns
Diarrhea
Osmotic diuresis
Excessive intake
Results in
Solute inside the cell is lower than the vascular space
Water leaves the cell and cell shrinks
hypernatremia assessment, treatment and promotion
Health History
Duration of sx
Precipitating factors
Physical assessment
Neuro assessment
vitals
Treatment
Water
Hypotonic solution
D5 and ½ NS
BP checks
Neuro status check
Monitor labs
Oral care
Health promotion/patient education
Need to offer fluids on regular intervals
What foods are high in sodium
Canned, frozen, lunch meat, pickles, ketchup, processed
If on tube feeds
Ordered free water flush
hyponatremia assessment, treatment, and promotion
Assessment
Current symptoms
Duration of sx
Precipitating factors
Neuro status
VS
Pulses
Edema
Daily weight
2.2 lbs for every 1L
Treatment:
Depletional
Isotonic IV fluids
NS, lactated ringers
If 110-150 then 3% sodium chloride
Can end up with central pontine myelinolysis
Dilutional
Diuretics
Lasix (loop diuretic)
Fluid restriction
Sodium tablets
Health Promotion/ Patient Education
Educate on signs and symptoms
Drink fluids with electrolytes during exercise
hyponatremia sx
Headache
Fatigue
Stupor
Tremors
Hyperreflexia
Coma
convulsions
potassium
Normal range: 3.5 – 5 mEq/L
Primary cation in intracellular fluid
hypokalemia
Value: < 3.5
Results from
Loop diuretics
Bumex and furosemide
NG tube
Ileostomy
High risk for hypokalemia and hyponatremia
Liquid stool
Signs and symptoms
Cardiac dysrhythmias
Flattened t waves
Prominent u wave
Prolonged PR interval
ST depression
Decreased CO
Digoxin
Increased risk for dig toxicity
Muscle weakness
N/V
Decreased BS
Altered kidney function
hypokalemia assessment, treatment, and promotion
Diagnostic Tests
EKG
Electrolytes
ABGs
Increased pH
Renal
BUN, Cr
Assessment
VS
Pulses
Orthostatic Hypotension
Mental status
GI assessment
Musculoskeletal assessment
Treatment
Call MD
Potassium supplement
Runs of K
10mEq/100mls/hr
hyperkalemia
Value: > 5.0
Results from
Chronic kidney disease
Excessive intake
Signs and Symptoms
Peaked T waves
Prolonged QRS
Can arrest
Numbness
Muscle tremors
Weakness
Abdominal cramping
hyperkalemia treatment, asessment, and promotion
Assessment:
Health history
Symptoms and duration
Precipitating factors
GI assessment
CV assessment
Monitor reduced urine output
EKG
Check pulses
Labs - electrolytes
Treatment:
Diuretics
Binding Agents
Veltessa (patiromer)
Binds potassium in exchange for calcium so it is passed out through feces
Lokelma (sodium zirconium cyclosilicate)
Binds in exchange with H and Na and potassium is excreted
Not used in emergencies
Insulin, hypertonic dextrose
In emergencies
D50 to counteract hypoglycemia
Albuterol
Potassium shifts into cells
Contraindicated in pts with acute MI and unstable angina
causes tachycardia
Calcium Gluconate and Calcium Chloride
For cardiac arrythmias
Dialysis
Health Promotion/Patient Education
Pseudo hyperkalemia
If someone uses a needle too small, they can hemolyze the blood and gives false high K
Assess pt to see if it is false high or not
calcium
Normal Range: 8.5-10 mg/dL
Function
Supports structure and function
Helps with muscle movement
Neuro transmission
Hormonal secretion
99% is found in the bone
hypercalcemia
Level: > 10 mg/dL
Results from:
Increased bone resorption
Hyperparathyroidism
Malignancies
inactivity
Signs and Symptom
Muscle weakness
Anorexia
Fatigue
n/v
Neuro changes
Confusion
Lethargy
Ekg dysrhythmias
Increase urine output
Kidney stones
hypercalcemia assessment, treatment, and promotion
Assessment
Excessive intake, immobility, malignancy, endocrine disorder
Symptoms and duration of symptoms
Precipitating factor
Vitals
Apical pulse
Mental status
GI
Muscle strain
Deep tendon reflexes
Diagnostic Tests
PTH
Ekg
Shortened QT
Shortened ST
Wide T waves
Wide QR
Monitor bone density
Treatment
Depends on severity
Low < 12
Moderate 12-14
Increase food intake
Weight bearing activity
Medications
Moderate to severe
IV
IV fluids (2-3L)
Loop diuretics
Patient education
Encourage weight-bearing activities
Fluid intake
Limit intake of dietary and over the counter Calcium
hypocalcemia
Value: < 8.5
Results from
Risk Factors
Older adults
Women
Lactose intolerance
Bariatric surgery
trousseaus
Signs and Symptoms
Numbness and tingling
Hyperactive reflexes
Tetany
Carpal pedal spasms
Bone pain
fractures
hypocalcemia assessment, treatment, and promotion
Assessment
Symptoms and duration of symptoms
Precipitating factor
Older adults
Removal of parathyroid
Lactose intolerance
Laryngeal spasm
Dysrhythmias
Seizures
Monitor vitals
Signs and Symptoms:
Chvostek's Sign
Trousseau’s
Diagnostic Tests:
Total serum calcium
Serum albumin
Corrected calcium (mg/dL) = measured total Ca (mg/dL) + 0.8 (4.0 - serum albumin [g/dL])
Low serum albumin can cause false low Ca
Serum magnesium level
Serum phosphate level
Would be high
Parathyroid hormone level
ECG
Treatment
Oral or IV Ca
Vitamin D
Monitor vitals
Monitor airway
Health Promotion/ Patient Education
Bone screening
Weight bearing exercise
Diet
Supplements need full glass of water 1-1.5 hours PC
phosphate
Normal Range: 2.5 - 4.5 mg/dL
Function
O2 delivery
hyperphosphatemia
Value: > 4.5 mg/dL
Results from:
Heat stroke
Hyperthermia
Disruptions in Ca level
Kidney disease
Signs and Symptoms
Same as signs and symptoms of hypocalcemia
hyperphosphatemia treatment
Treatment
Monitor labs
Monitor airway
Neuromuscular status
Limit phosphate intake
hypophosphatemia
Value: < 2.5 mg/dL
Results from:
Increase in renal secretions
Respiratory alkalosis
IV glucose
Antacids
Steroids
Diuretics
Signs and Symptoms
Intentional tremor – on movement
Bleeding disorder
Impaired WBC
Decreases O2
RBC destruction
Decrease in O2 in heart muscle
Dysrhythmias
Chest pain
hypophosphatemia treatment, assessment, and promotion
Treatment
Dietary oral supplements
IV phosphate if less than 1
Monitor electrolyte
Health promotion/Patient Education
Avoiding phosphate binding antacids
magnesium
Normal Range: 1.8-2.5 mEq/L
Function
Enzyme reactions
Protein synthesis
Muscular and CV function
hypermagnesemia
Value: >2.5
Results from:
Renal failure
OTC laxatives
Signs and Symptoms
Brady cardia
Heart block
Cardiac arrest
Decreased CNS
Lethargy
Weakness
Confusion
Reflexes are weak or absent
Respiratory depression
HTN
Dysrhythmias
hypermagnesemia treatment and assessment
Treatment
Underlying cause
Calcium gluconate – for cardiac effects
Respiratory support
Pacer
Assessment
Monitor vs
Monitor CV status
I&O
reflexes
hypomagnesemia
Value: < 1.8 mEq/L
Results from:
Deficit in intake
Starvation
Alcoholism
Ileostomy
Diarrhea
Excessive urination
DKA
Signs and Symptoms:
Positive Babinskis
Increase in neuromuscular excitability
Decrease in CNS
Cardiac dysrhythmias
Torsade's de pointes – lethal
Cannot come out until mg level is normal
hypomagnesemia treatment tests
Diagnostic Tests:
EKG
Lab tests
Treatment:
Give Mag
What's causing it
our job as nurses
Identify pts who are likely to develop imbalances
Monitor pts who are likely to develop imbalances
Monitor pts for early manifestations
Implement interventions to correct and prevent imbalances
Education patients on prevention