GI Final Practical
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
what do the liver, gallbladder, and biliary ducts arise from? when?
endodermal foregut bud
4th wk
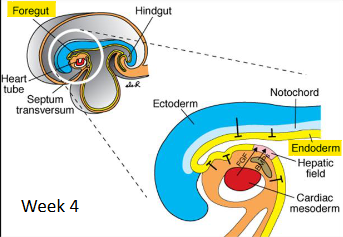
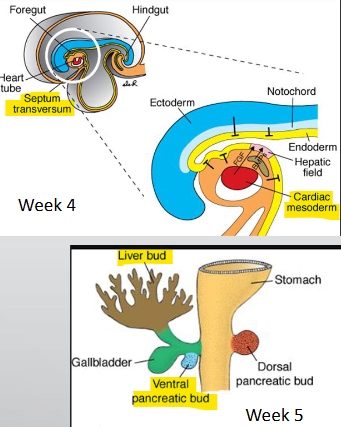
what does the hepatic diverticulum include? what is it induced by?
cranial liver bud, caudal ventral pancreatic bud, GB
induced via BMP (from septum transversum) + FGF2 (from cardiac mesoderm)
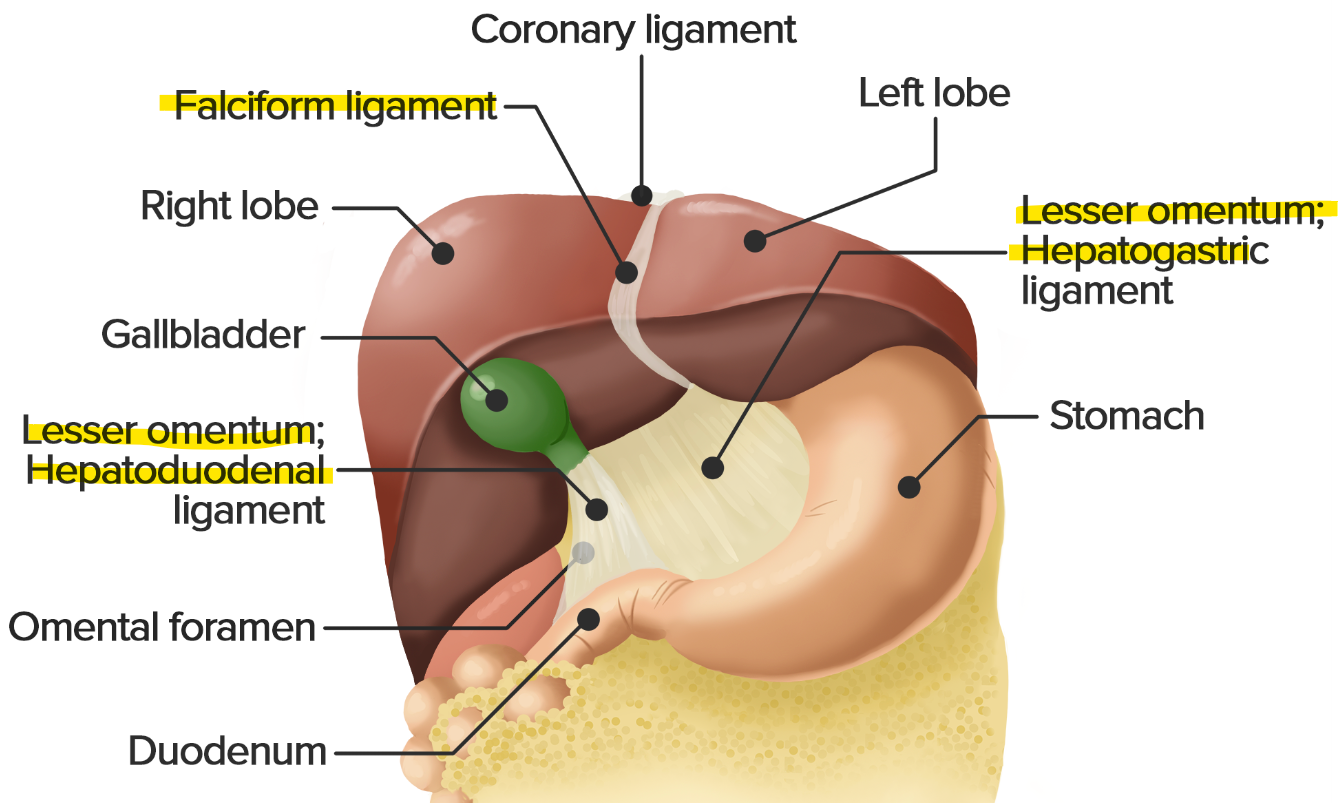
what does the liver bud extend into? what does it form?
septum transversum (mesoderm)
ventral mesentery
lesser omentum (hepatogastric + hepatoduodenal)
falciform lig. w/ umbilical v. (round/teres lig.)
what does the vagus nerve and celiac plexus supply?
vagus → parasympathetic
celiac → sympathetic
GB, pancreas, liver
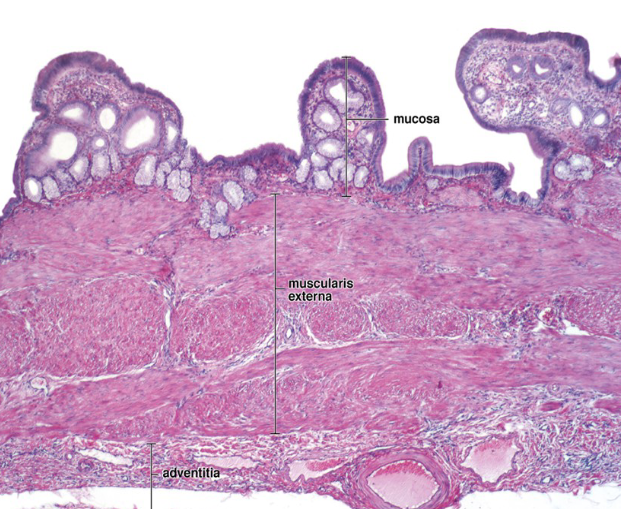
function of gallbladder? what stimulates it? wall layers?
conc., store, sec. bile → 2nd part duodenum
CCK (contract), fatty food, vagus stim.
mucosa (simple columnar, LP), muscularis externa, adventitia/serosa
lacks muscularis mucosa + submucosa
only absorptive cell
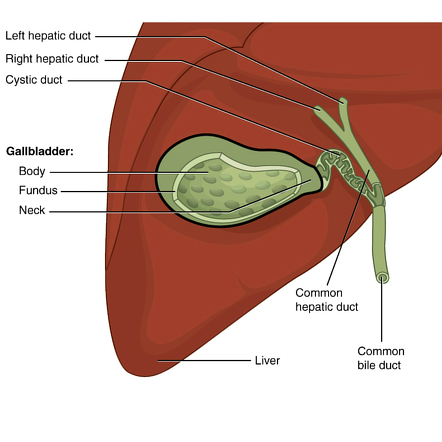
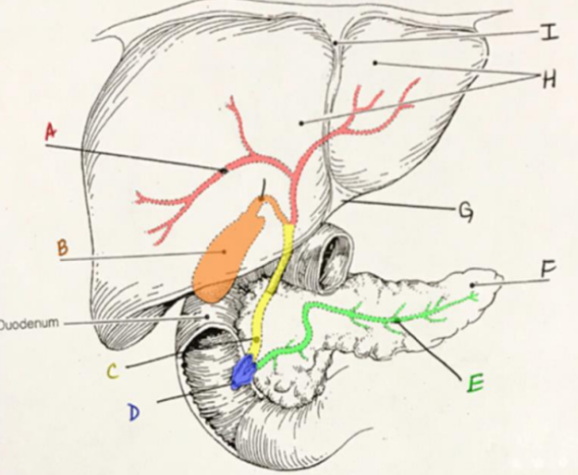
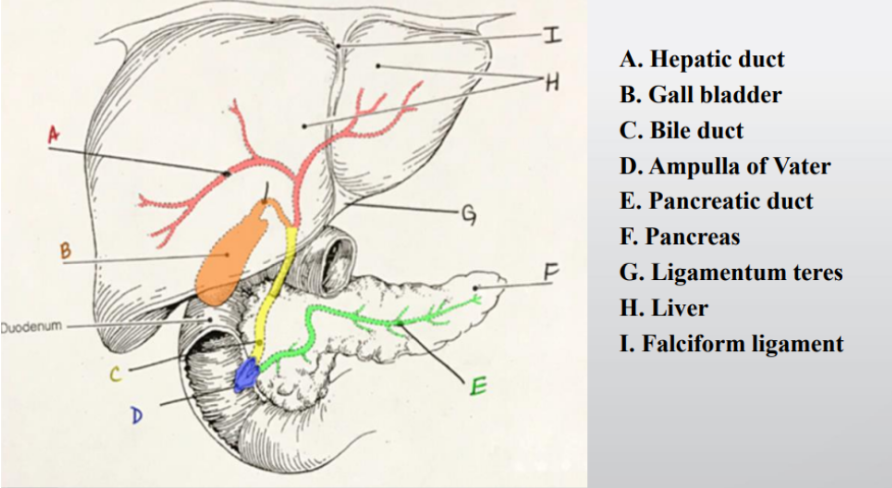
what is the flow of bile?
R. + L. hepatic duct → common hepatic duct → cystic duct jxn (to GB) → common bile duct
what is the supply of the gallbladder?
arteries: cystic a. (RHA branch)
veins: cystic v.
LN: cystic LN
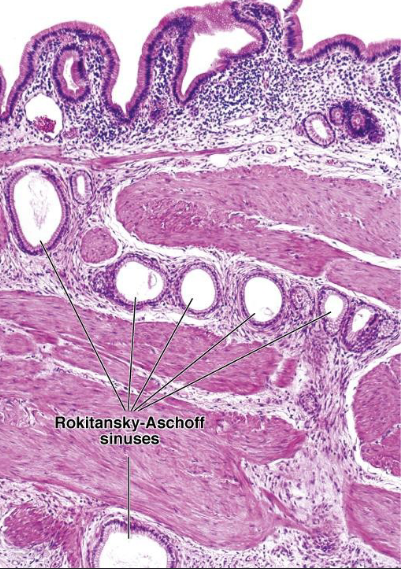
what are the rokitanksy-aschoff sinuses of the gallbladder? when is it more prominent?
deep diverticula/outpouchings of mucosa
prominent → cholecystitis
what is cholelithiasis? confirmed by? what does obstruction cause? risk factors?
gallstones (pigment or cholesterol), typically confirmed w/ US
cyst duct obstructed → cholecystitis
inc. serum bilirubin if common bile duct blocked
female, >40, obesity, high cholesterol
what are cholecystitis symptoms? complications? acute vs chronic?
inflammation of GB
RUQ pain, vomit, fever, high WBC
complications: pancreatitis, CBD inflammation, GB rupture, ischemia
acute > 3 mth, chronic < 3 mth
function of pancreas? regulation?
exocrine → pancreatic juice from pancreatic acini
some endocrine → islets of langerhans (hormones)
EEC (SI I cells)→ secretin + CCK
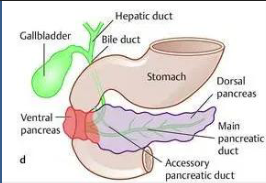
what portion of the pancreas do the ventral and dorsal endodermal buds form?
ventral → head + uncinate process
dorsal → neck, body, tail
visceral mesoderm → CT
what is an annular pancreas?
ventral bud migrates opposite direction
pancreatic tissue surrounds duodenum (constriction)
pancreas outer structure? what projects? what does it hold?
thin capsule + stroma → loose CT
interlobular CT septa project from capsule into parenchyma (creates lobules)
interlobular septa houses interlobular ducts, BV, nerves, and lamellar (Pacinian) corpuscles (sensory receptor)
what do acinar cells contain?
zymogen granules → produce digestive enzymes
amylases, proteases, lipases, nucleases
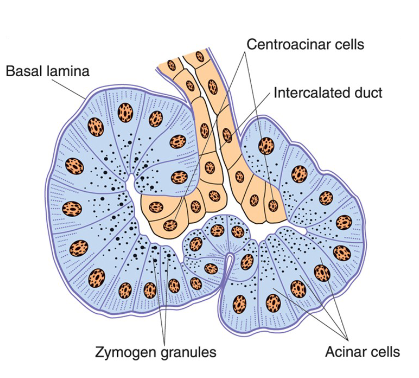
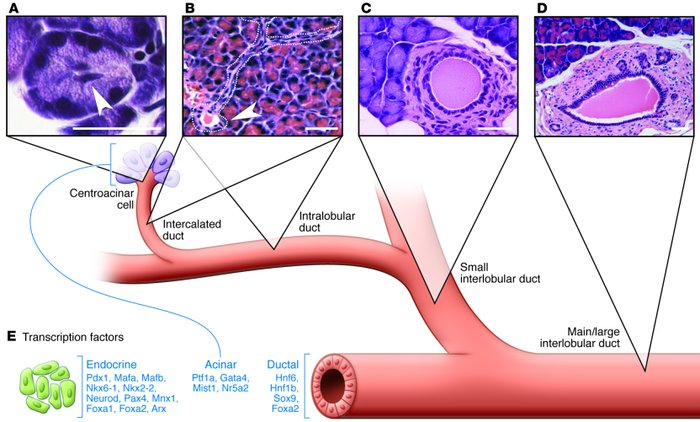
what do centro acinar and intercalated duct cells secrete? function of secretion?
HCO3 →
alkalinize + transport hydrolytic enzymes produced in acini
what is the flow of the pancreas-duct system?
centroacinar cells (HCO3 sec.) → intercalated ducts → intralobular ducts → interlobular ducts → main pancreatic ducts (of Wirsung)
2nd part duodenum w/ common bile duct → thru major papilla @ ampulla
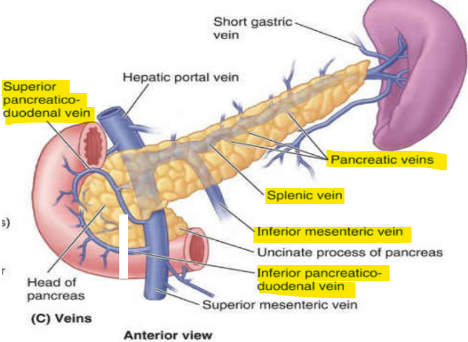
what is the supply of the pancreas?
arteries: sup (common hepatic → gastroduodenal) + inf. (SMA) pancreaticoduodenal a.
veins: PD v., pancreatic v. (splenic → IMV)
pancreatosplenic → celiac LN
what can lead to pancreatitis?
chronic alcohol intake (inc. zymogen sec.) , gallstones (blocks sphincter of oddi)
lead to acinar cell injury or impaired zymogen sec. (e.g trypsinogen act. early)
what is infected pancreatic necrosis? what would a CT scan show?
multiple organ failure, fever, inc. WBC + blood glucose, abdominal pain
via pancreatitis (inflammation)
CT → walled off, peripancreatic collection w/ gas inside (pseudocysts)
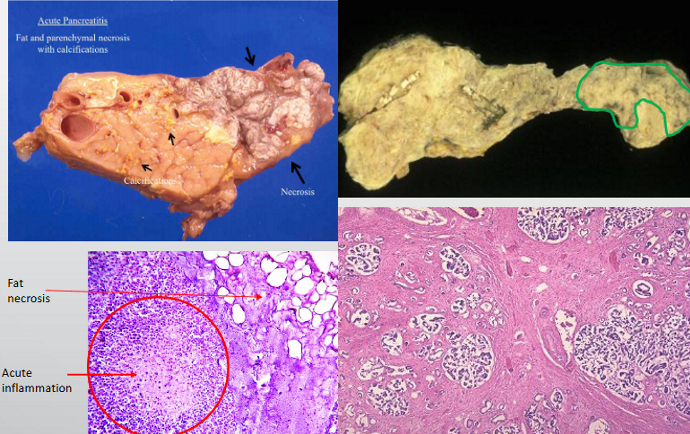
what’s the difference between acute and chronic pancreatitis?
acute → pancreatic + fat necrosis
autodigestion via alcohol, CFTR, trauma
high lipase/amylase
chronic → repeat episodes = fibrosis (ito cells), acinar atrophy, calcification
diagnosed w/ CT/ECRP
leads to pancreatic insufficiency (weight loss, steatorrhea), DM
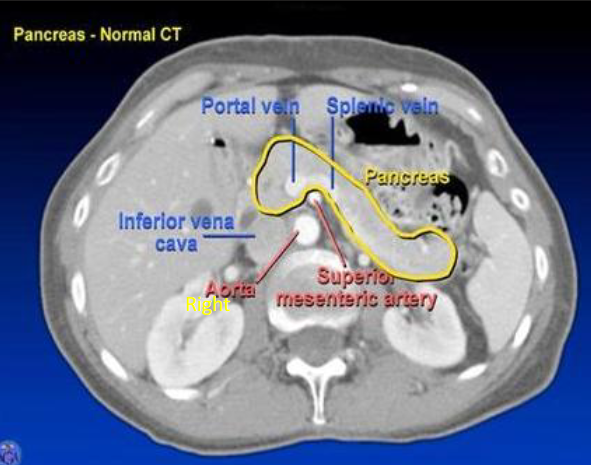
what does a pancreatic CT shown?
tail → @ splenic hilum
head → @ IVC
body → @ aorta + SMA
what proteins does the liver produce?
albumin
angiotensinogen
coagulation factors
transferrin
apolipoprotein
C-reactive protein
ceruloplasmin
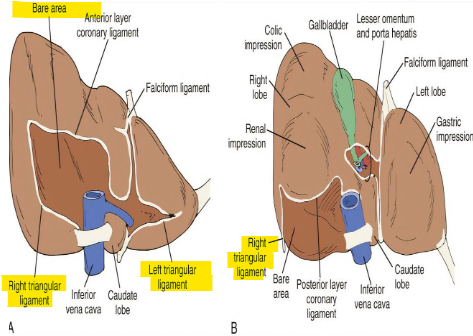
bare area of liver? triangular ligament of liver? ligamentum teres of liver?
bare area → no peritoneum, coronary lig. form boundaries
R. + L. triangular lig. → connected w/ R. + L. coronary lig.
ligamentum teres (round lig.) → umbilical v. remnant; connects liver to umbilicus
what can stop bleeding caused by laceration to liver lobes?
pringle maneuver → hepatoduodenal lig. compression
contains portal triad
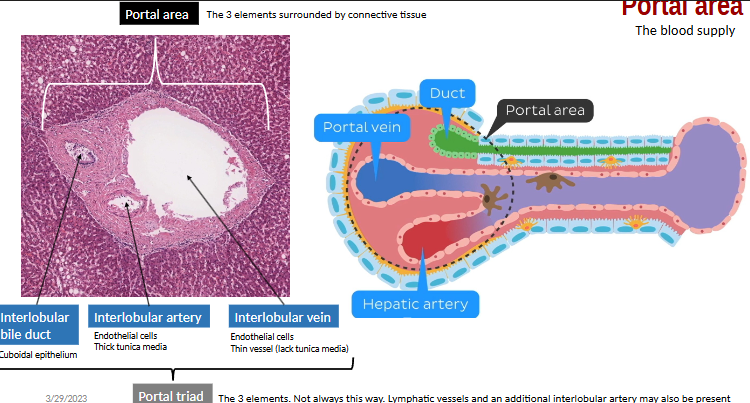
what is the liver stroma? what does it surround? what do these structures contain?
CT cont. w/ fibrous capsule of Glisson
portal space/area → portal triad
contains: BV, nerves, lymphatics vessels (thoracic duct), bile ducts
what forms the common bile duct? what can lead to jaundice?
common hepatic duct + cystic duct, cuboidal cells
dilation (via obstruction) + constriction of common bile duct
what is the blood supply of the liver?
portal v. (75%) + hepatic a. (25%)
portal v. = splenic v. + SMV
hepatic a. = celiac trunk
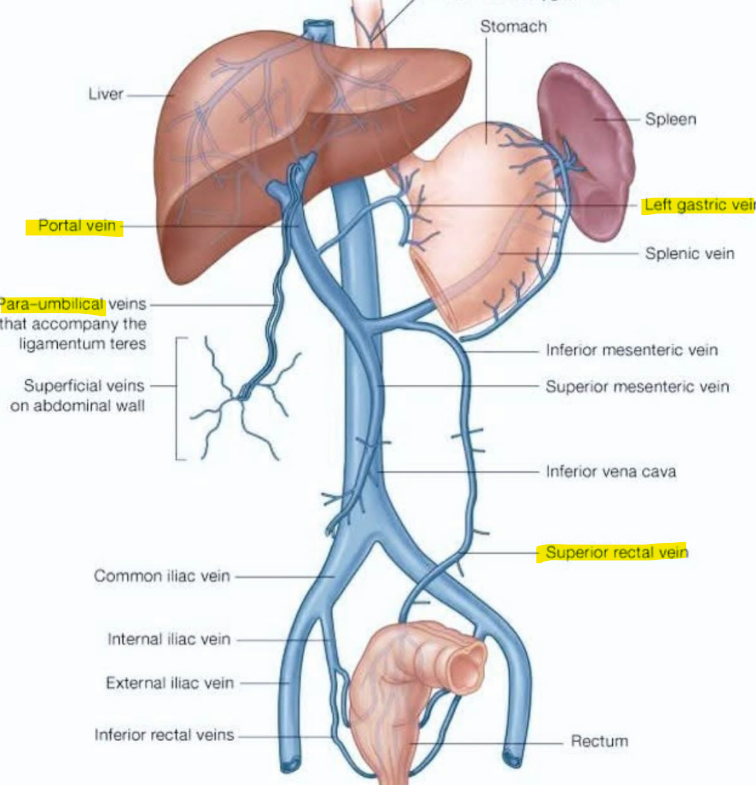
what is portal hypertension? causes?
inc. pressure in hepatic portal v. → varices (can rupture)
caput medusae → prominent periumbilical v.
cause: cirrhosis (=scarring + fibrosis → obstructs blood flow), budd-chiari syndrome, R. heart failure
what are common varices (abnormal dilations via portal HTN) locations?
esophageal: L. gastric v. (portal) + esophageal v. (systemic) → azygos v.
caput medusae: paraumbilical v. (portal) + epigastric v. (systemic) → SVC/IVC
rectal: sup. rectal v. (portal) + middle/inf. rectal v. (systemic) → IVC
what are interlobular vessels? septa?
branches of portal v. + hepatic a. occupying portal space
septa → thin CT, divides lobules (contain portal triads)
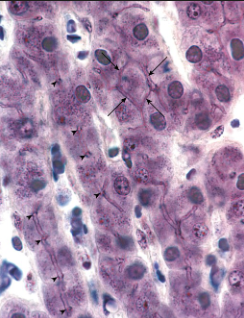
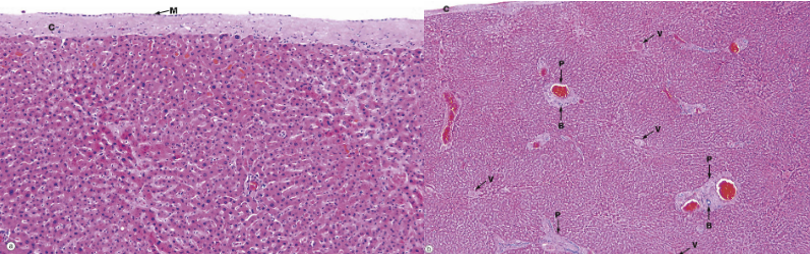
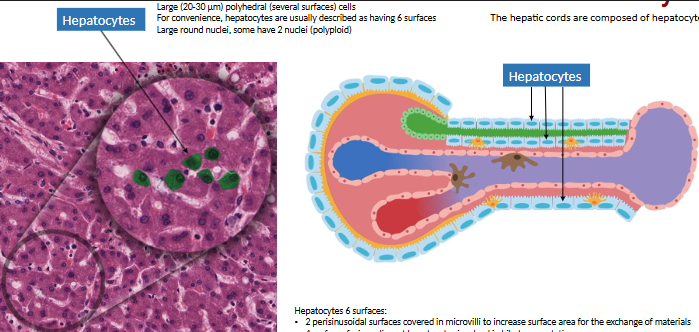
what is the liver parenchyma composed of?
hepatic cords → organized plates of hepatocytes separated by sinusoidal c.
hepatocytes → large, polygonal cells w/ large # ribosomes, mitochondria, golgi complex, lysosome, peroxisome

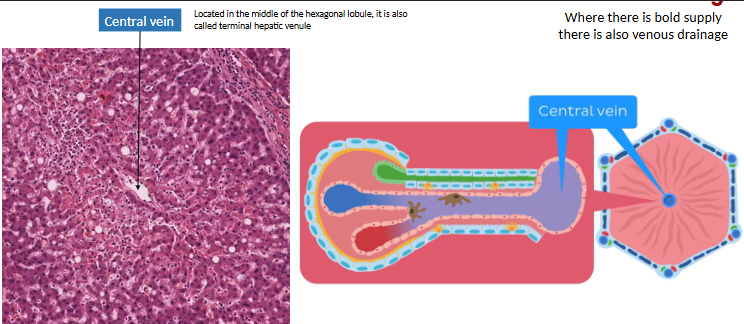
what are sinusoidal capillaries (sinusoids)? venous drainage path?
vascular channels btwn hepatic cords
interlobular vessel → sinusoids → central v. → sub lobular v. → IVC
central v. runs through center
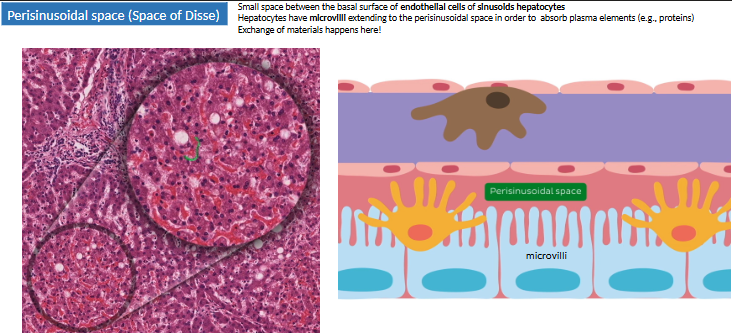
where are the perisinusoidal spaces (space of Disse)? function?
btwn sinusoidal endothelium (hepatic a. + portal v.) + hepatocytes (bile duct + outer)
XC of materials here → hepatocytes have microvilli extending to perisinusoidal space to absorb
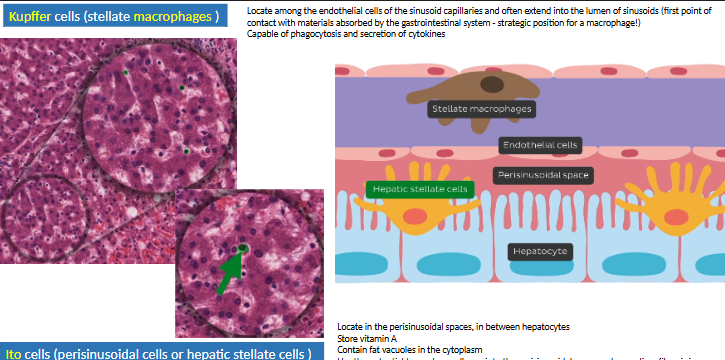
what are the cells of the perisinusoidal spaces (space of Disse)?
kupffer cells (endothelium) → MO
Ito cells (microvilli) → store fat + vit A
activated via cytokines → fibrosis
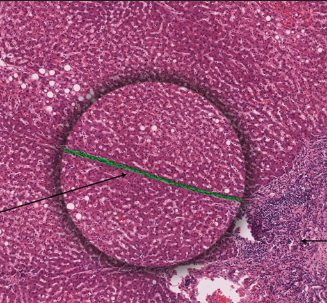
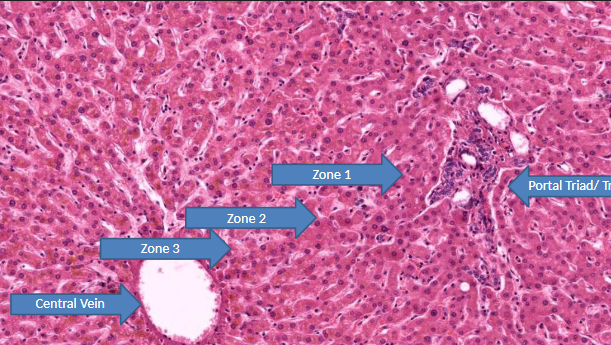
what are the liver lobules (functional units)?
hepatic lobule → anatomical, site of lymph formation
portal lobule → bile sec. (exocrine), contain bile duct
liver acinus → correlation btwn blood perfusion, metabolic activity, liver pathology
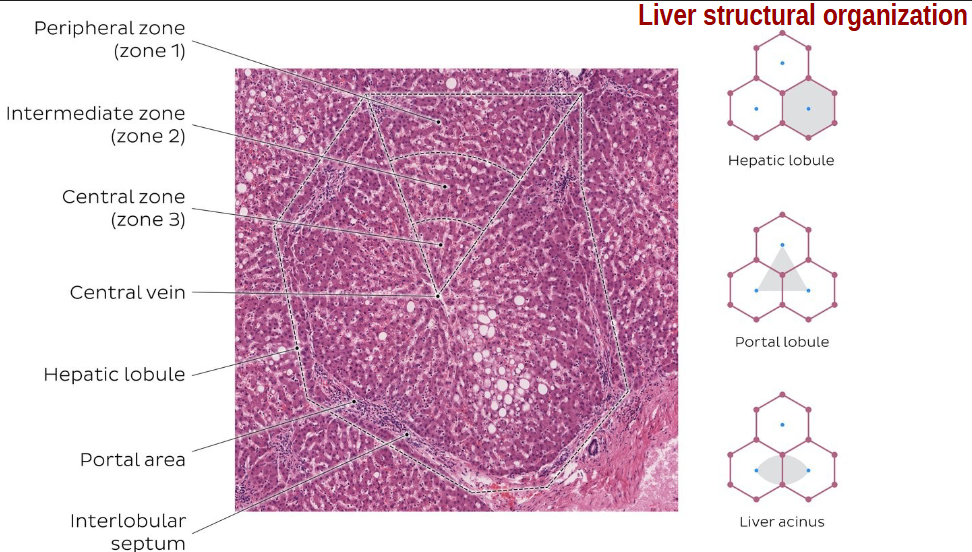
what occurs in zone 1 (peripheral/peri lobular) liver acinus? what is it resistant to?
highest metabolic activity (most O2 since O2, nutrients, toxins arrive here 1st)
most resistant to circulatory compromise → last to die
what is zone 1 (peripheral/peri lobular) of liver acinus affected by 1st?
viral hepatitis
ingested toxins (cocaine)
bile duct obstruction (bile stasis)
what would occur to ammonia levels if the liver is removed?
serum ammonia inc. bc zone 1 converts ammonia → urea
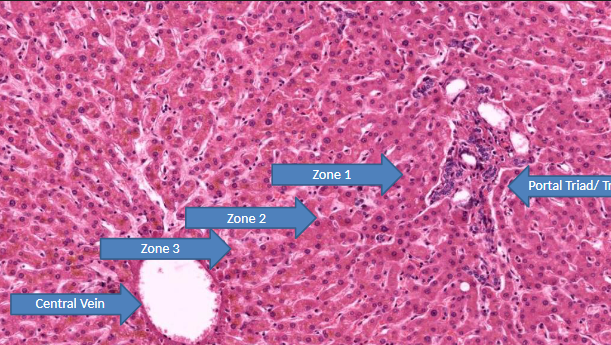
what is zone 2 (intermediate/mid lobular) of liver acinus? what is it affected by?
transitions metabolic processes
affected by yellow fever
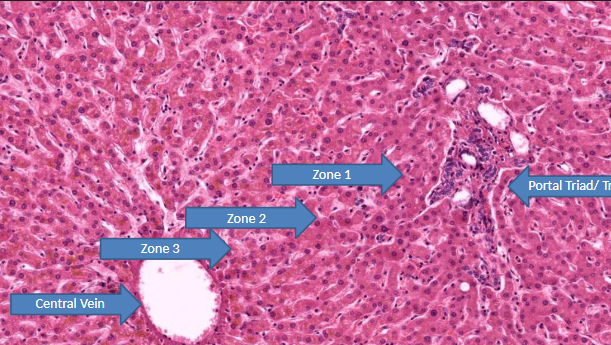
what occurs in zone 3 (central/centri lobular) of liver acinus? high concentration of what? sensitive to what?
lowest metabolic activity (O2, nutrients, toxin arrive here last)
high conc. → cytochrome P-450 (drug/toxin metabolism)
sensitive to metabolic toxin (EtOH, CCl4, halothane, rifampin, acetaminophen)
what occurs if circulation is impaired to liver? what occurs if bile duct is obstructed? what is common site of alcoholic hepatitis?
zone 3 first to die
zone 3 last to show bile stasis
zone 3
what is hepatic cirrhosis?
excess deposition of CT btwn hepatic nodules
what is acute liver abscess cause? symptoms?
cholecystitis, ECRP, infections, DM, cirrhosis, alcohol
inc. WBC, fever, upper abdominal pain, liver fxn dec.
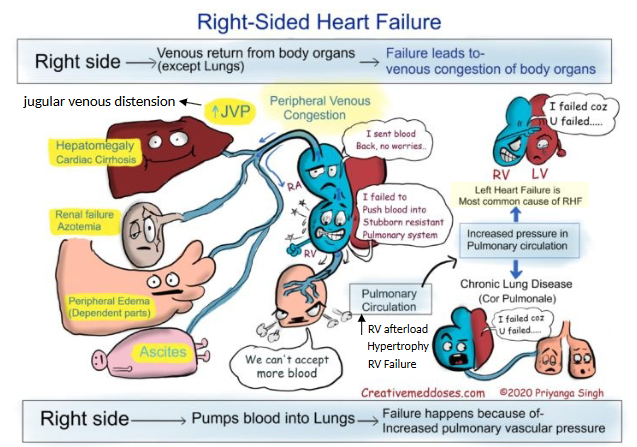
what are right heart failure symptoms?
hepatomegaly (cardiac cirrhosis), renal failure, peripheral edema, ascites (abdominal distension)
failure for venous return from organs → venous congestion of body organs
inc. pulm. vasc. resistance → failure of blood to pump to lungs
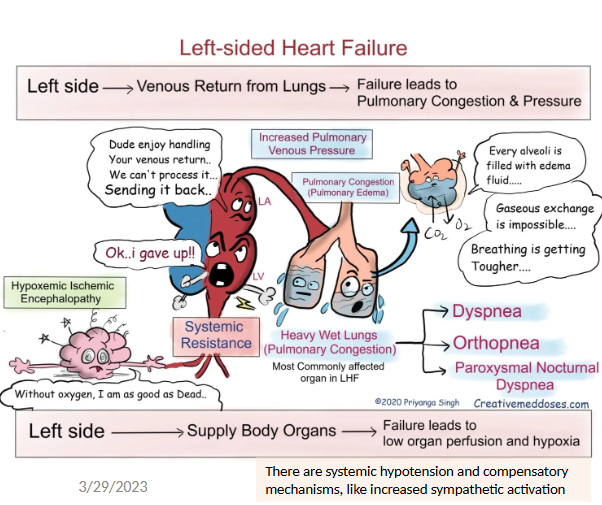
what are left heart failure symptoms?
dyspnea, orthopnea, paroxysmal nocturnal dyspnea
failure for venous return from lungs → pulm. congestion (edema) + pulm. venous pressure
failure to supply body organs → low organ perfusion + hypoxia
what is the same between primary sclerosing cholangitis (PSC) and primary biliary cholangitis (PBC)?
autoimmune, inflammation/scarring → cirrhosis + liver failure
mild fatigue, pruritus, RUQ pain
gross:
early → smooth liver w/ green (cholestasis =blocked bile)
later → scarring + poor fxn
what is the difference between primary sclerosing cholangitis (PSC) and primary biliary cholangitis (PBC)?
PSC → men (30-50), large bile duct (extra + intrahepatic), inflammation + fibrosis (irregular bile duct)
ass. w/ IBD (UC)
pANCA elevated
PBC → women (40-60), autoimmune (AMAs), small intrahepatic bile duct
what are the boundaries of the anterolateral abdominal wall (AAW)?
sup: cartilage of 7th-10th ribs + xiphoid process
inf: inguinal lig. (ASIS to pubic tubercle) + sup. margin of pelvic girdle (iliac crest, pubic crest, pubic symphysis)
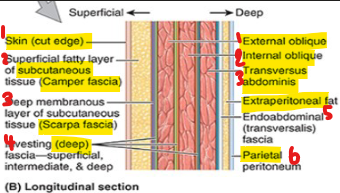
what are the AAW layers (fascia and muscle)?
skin → outer w/ sensory nerve endings
superficial fascia of subcut. tissue
camper fascia
scarpa fascia → deep membranous
muscle layers (EO, IO, TA)
deep fascia (each layer)
extraperitoneal fat (cushion)
parietal peritoneum (serous)
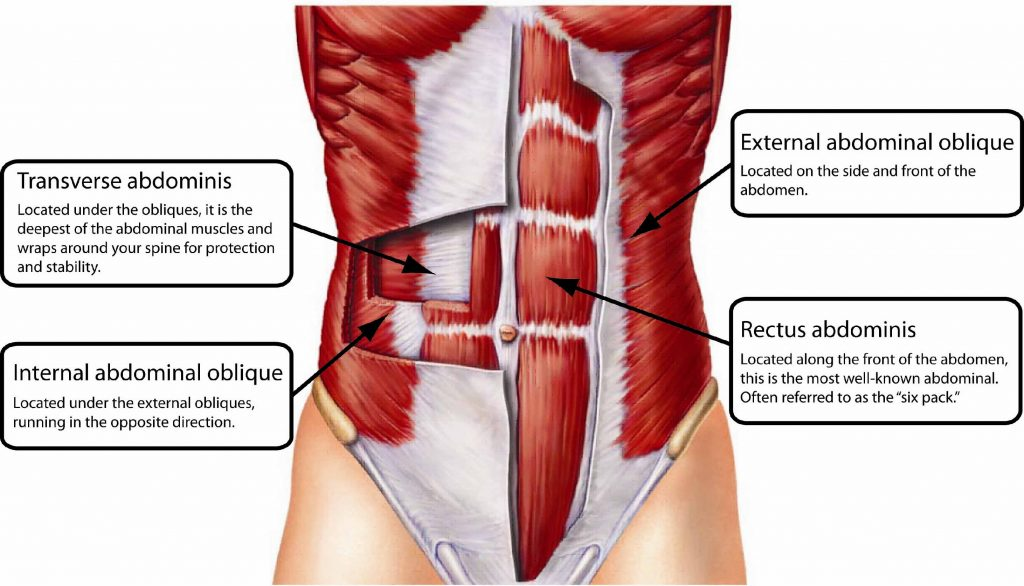
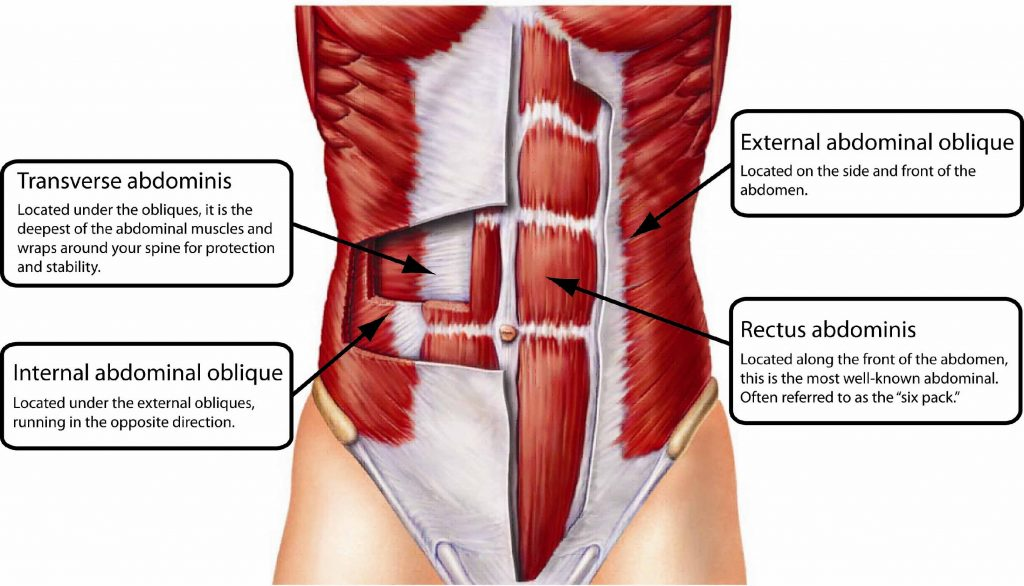
what is the function of the abdominal muscles? what are types?
support, protection, movement, pressure regulation, assist respiration
flat (TO, EO, IO) and vertical (RA, Py)
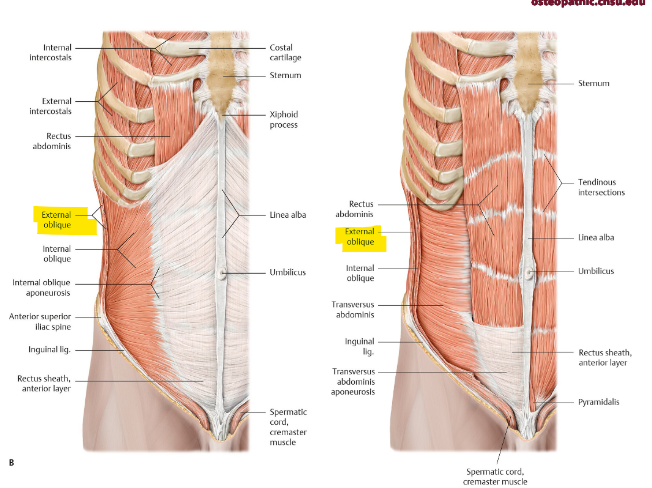
what is the function of the external oblique? origin and insertion? fibers
bilateral contraction → flex trunk + compress abdominal content
unilateral contraction → rotate trunk to opp. side + bend to same side
5-12th rib → linea alba, public tubercle, ant. iliac crest
inf. medial (hands in pocket)
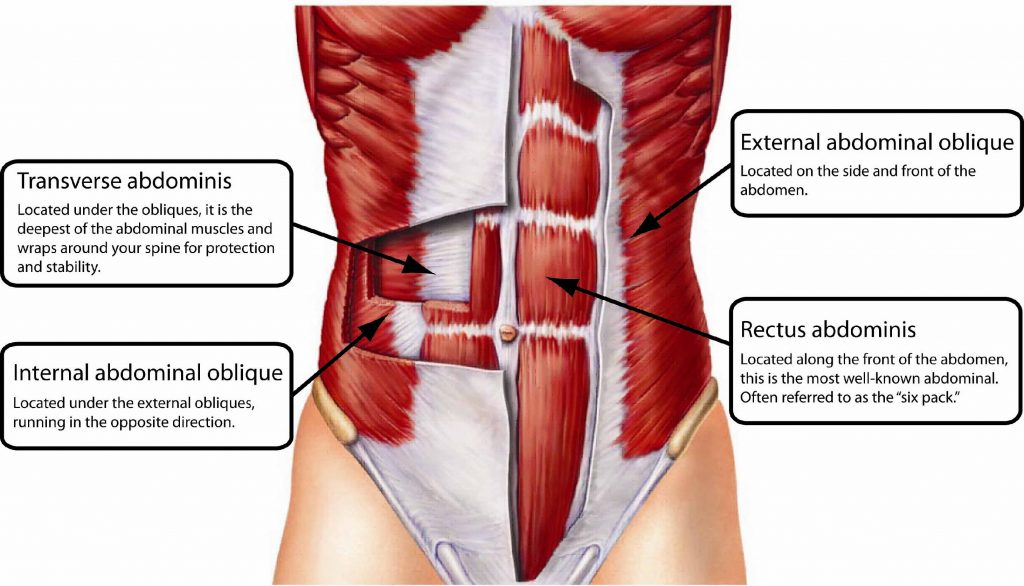
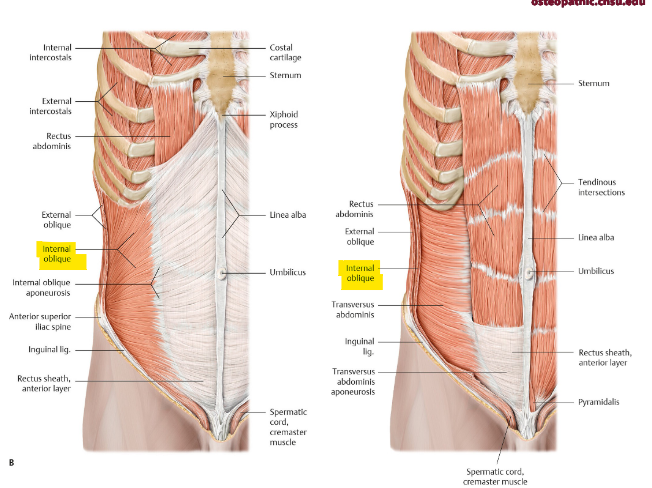
what is the function of the internal oblique? origin and insertion? fibers
bilateral contraction → compress + support abdominal viscera, flex trunk
unilateral contraction → rotate trunk to same side + bend laterally
ant. 2/3 iliac crest → inf. 10-12th rib
sup. medial
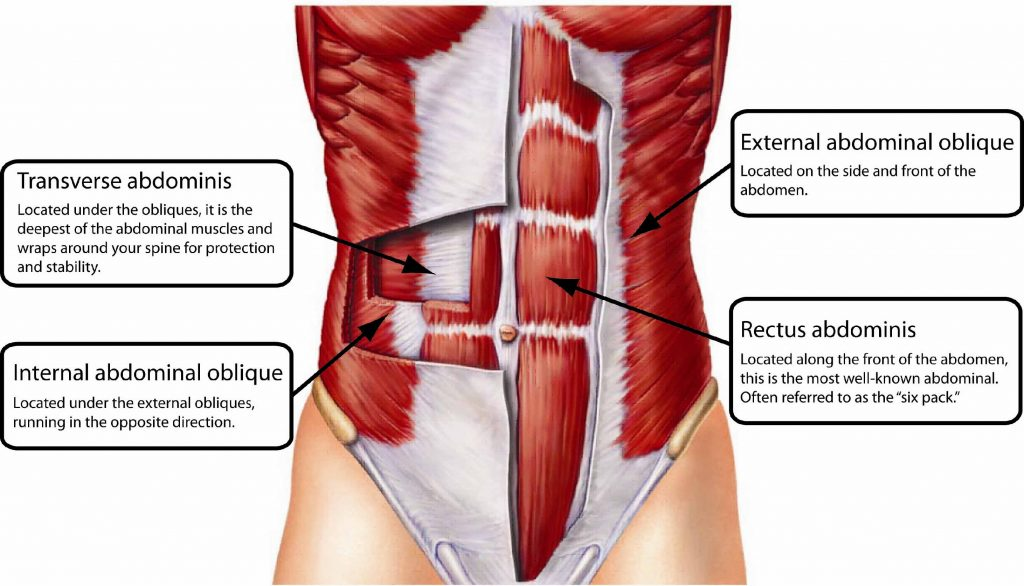
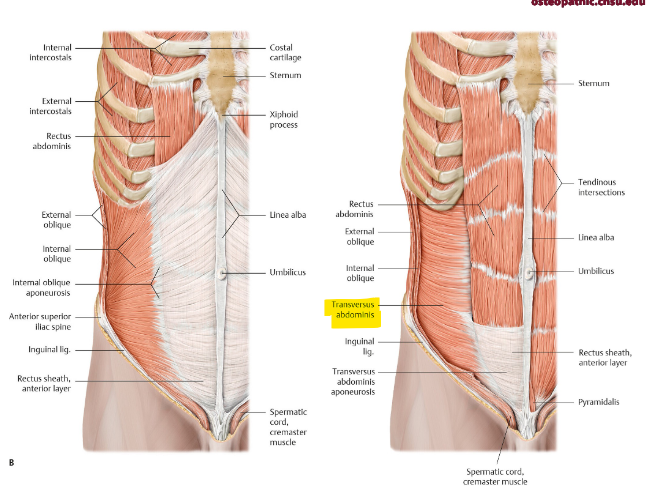
what is the function of the transversus abdominis? origin and insertion? fibers?
core stabilization
compression abdominal content → inc. intra abdominal pressure
forced expiration, defecation, childbirth
7th-12th costal cartilage → linea alba, pubic crest
horizontal
what is the conjoint (inguinal falx)? function?
int. oblique + transversus abdominis
strengthens post. wall of inguinal canal (protects against direct hernias thru hesselbach)
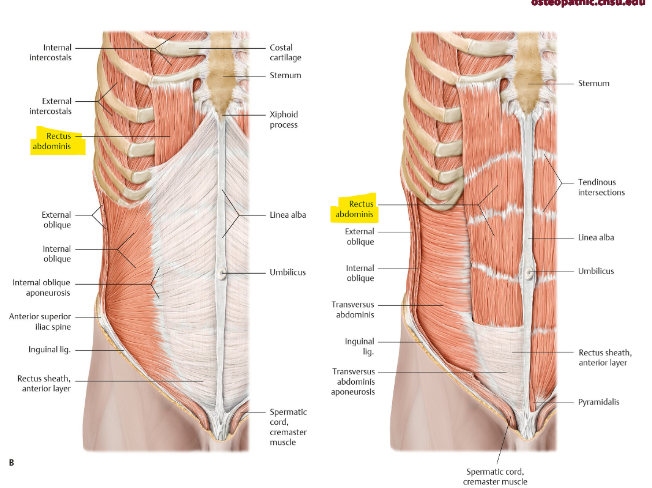
what is the function of the rectus abdominis? layers? origin and insertion?
flex trunk, compress abdominal content, stabilize pelvis (anti lordosis)
rectus sheath → enclose RA + Py
layers (S→D): ant. rectus sheath, RA muscle, post. rectus sheath, endo-abdomina fascia
pubic symphysis + crest → xiphoid process/5-7th costal cartilage
what is the function of the pyramidalis? clinical connection?
tenses linea alba (absent/nonfxn, but can be mistaken for pathology)
linea alba → midline fibrous seam (xiphoid to pubic symphisis)
surgical incision to avoid muscle tissue
diastasis recti → postpartum condition, from linea alba stretch
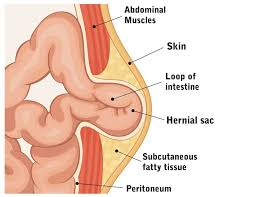
what are abdominal hernias? types?
protrusion of abdominal contents through weakened area of anterolateral abdominal wall
neonatal, acquired, epigastric, spigelian
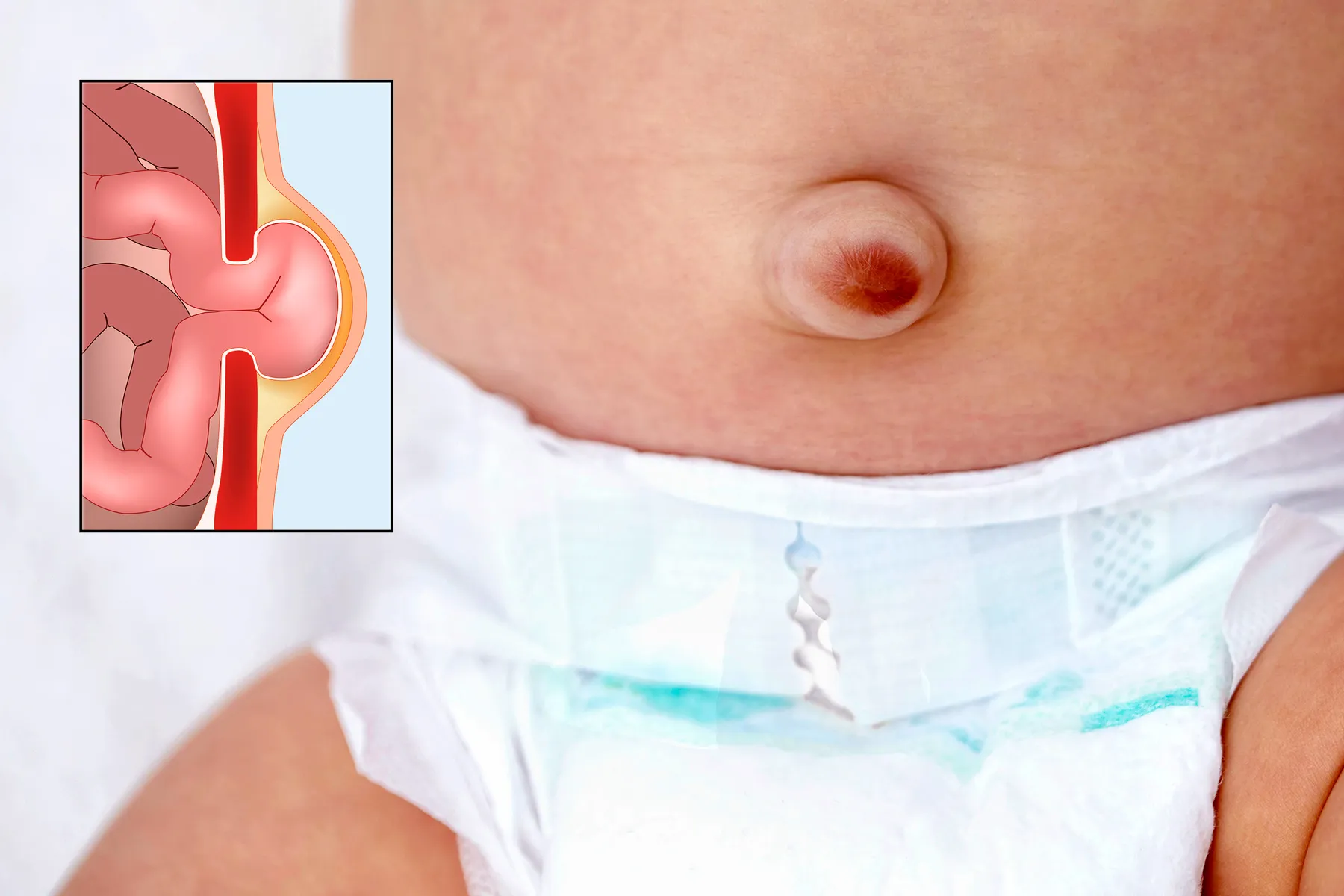
what is a neonatal umbilical hernia? common in?
failure of umbilical ring closure after birth
small, close spontaneously
common in low birth weight
what is an acquired umbilical hernia? common in?
inc. intra abdominal pressure + weakness of abdominal wall = extra peritoneal fat/peritoneum protrudes
common in women + obese
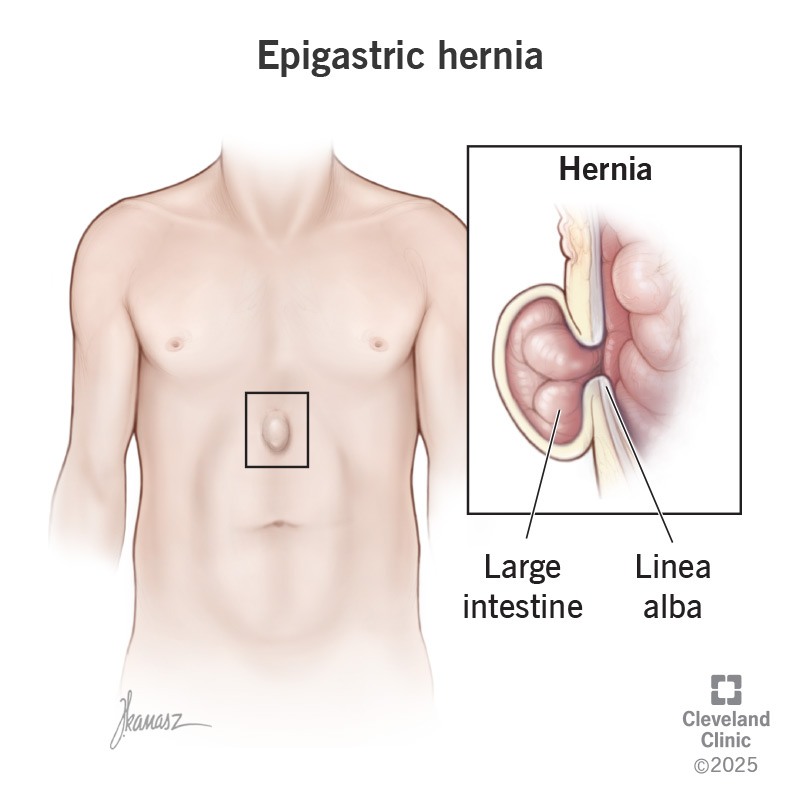
what is an epigastric hernias?
protrusion of lobules of fat (rather than bowel) along linea alba
painful, esp. if compressed nerve
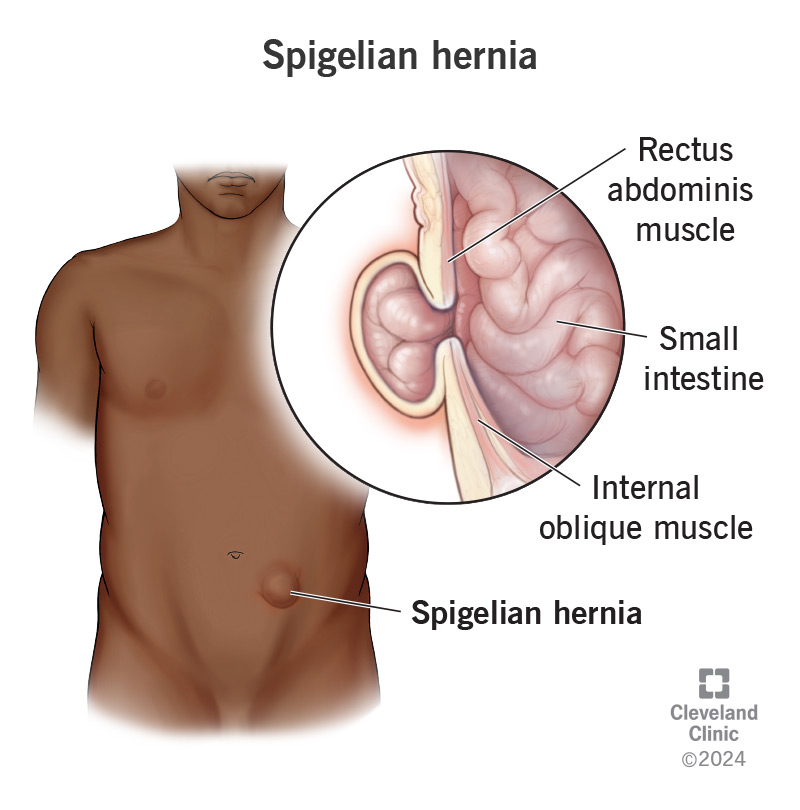
what are spigelian hernias? common in?
hernial sac composed of peritoneum
often covered by only skin + subcut. fat along semilunar lines (lat. to rectus sheath)
common in 40+, obese
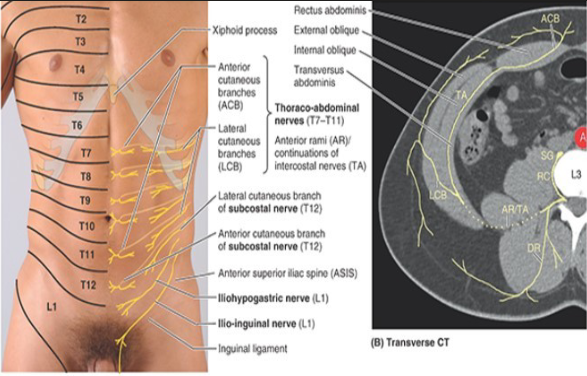
what are the dermatomes of AAW?
T7-T9 (above umbilicus)
T10 (@ umbilicus)
T11-L1 (below umbilicus)
L1 (inguinal fold + pubic region)
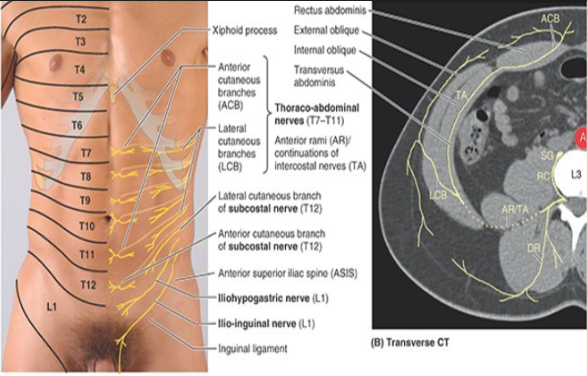
what is the neuro vasculature of AAW?
ant. rami of spinal nerves T7-T12
L1 ant. ramus (bifurcates into iliohypogastric + ilioinguinal)
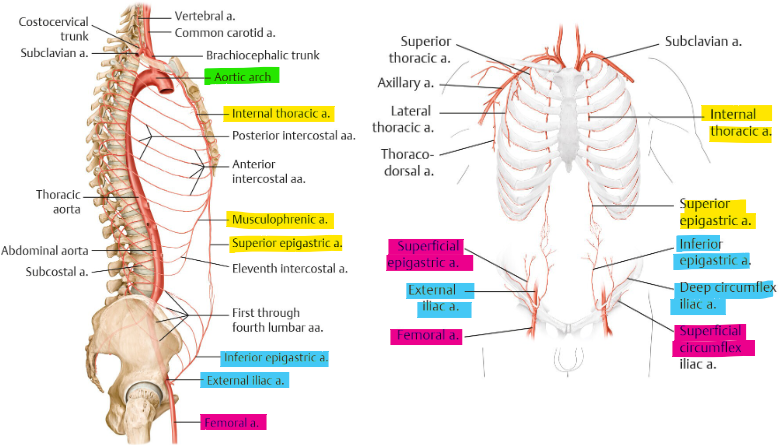
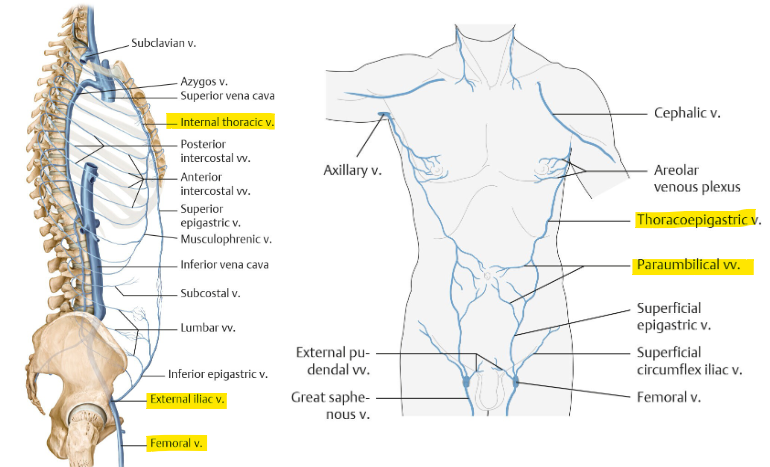
what is the superior blood supply of AAW?
from int. thoracic → musculophrenic, sup. epigastric
diaphragm vs RA, umbilical
from aorta → 10/11th post. intercostal a. + subcostal
lateral (lumbar/flank)
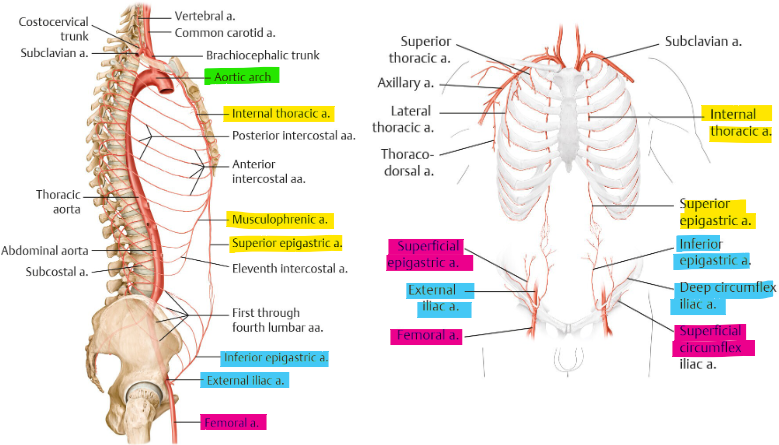
what is the inferior blood supply of AAW?
from ext. iliac a. → inf. epigastric + deep circumflex iliac
RA, pubic, inf umbilical VS iliacus, inguinal
from femoral a. → superficial circumflex iliac + superficial epigastric
inguinal, ant. thigh VS pubic, inf. umbilical
what is the venous drainage of AAW?
thoracoepigastric v. + paraumbilical v.
drain into int. thoracic, ext. iliac, femoral v.
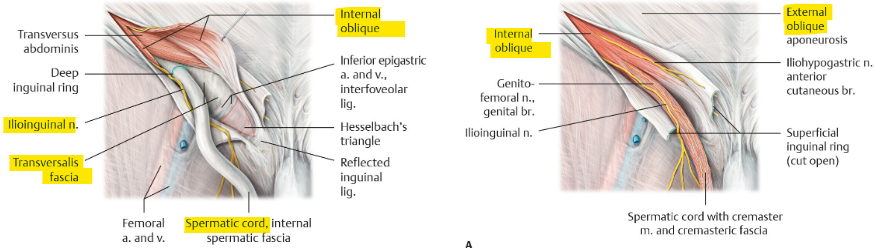
what is the inguinal canal? contents?
oblique passage inf. to anterolateral abdominal wall
content: ilioinguinal nerve, genital branch (genitofemoral nerve), spermatic cord/round lig.
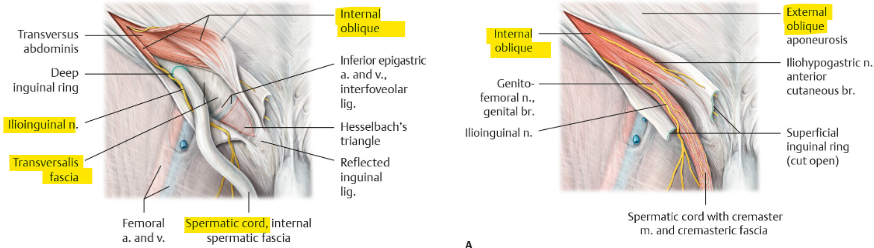
what are the boundaries of the inguinal canal?
ant. wall → EO + IO (lateral)
post. wall → transversalis fascia + inguinal falx (conjoint tendon)
floor → iliopubic tract (laterally) + inguinal lig. (centrally)
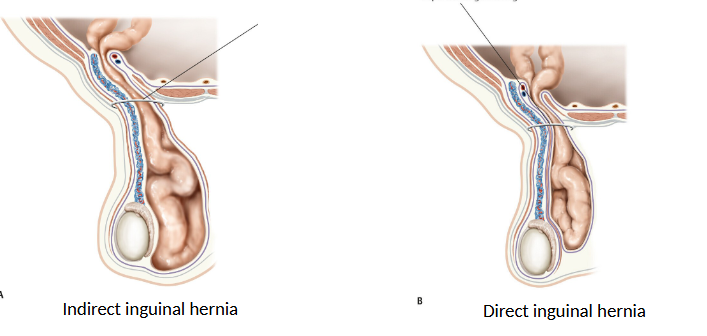
what are the types of inguinal hernias?
direct → through inguinal/hesselbach triangle (not scrotum)
med. to epigastric a.
indirect → through deep inguinal ring (in scrotum)
lat. to epigastric a.
femoral → inf. to inguinal lig. w/in femoral canal
aberrant hepatic arteries?
RHA → SMA
LHA → L. gastric a.