Lec 12: Ostomy Care
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
excoriation def
injury to the surface of the skin = abrasion
melena def
partially digested blood in stool
peristomal def
area around the stoma
occult blood def
hidden
effluent def
material discharged from stoma
steatorrha def
stool with abnormally high fat content
What is an Ostomy def
opening in the abdominal wall to eliminate feces or urine
can be temporary or permanent
An ostomy may be required in;
cancer
inflammatory bowel disease
obstruction
necrosis
trauma/perforation
congenital malformation
what are the diff types of ostomies
urostomy
ileostomy
colostomy
Urostomy def
diversions are surgical procedures which creates a new path for urine flow from the kidneys to a location other than the bladder
2 main types=continent and incontinent
Incontinent Urinary Diversion def (urostomy)
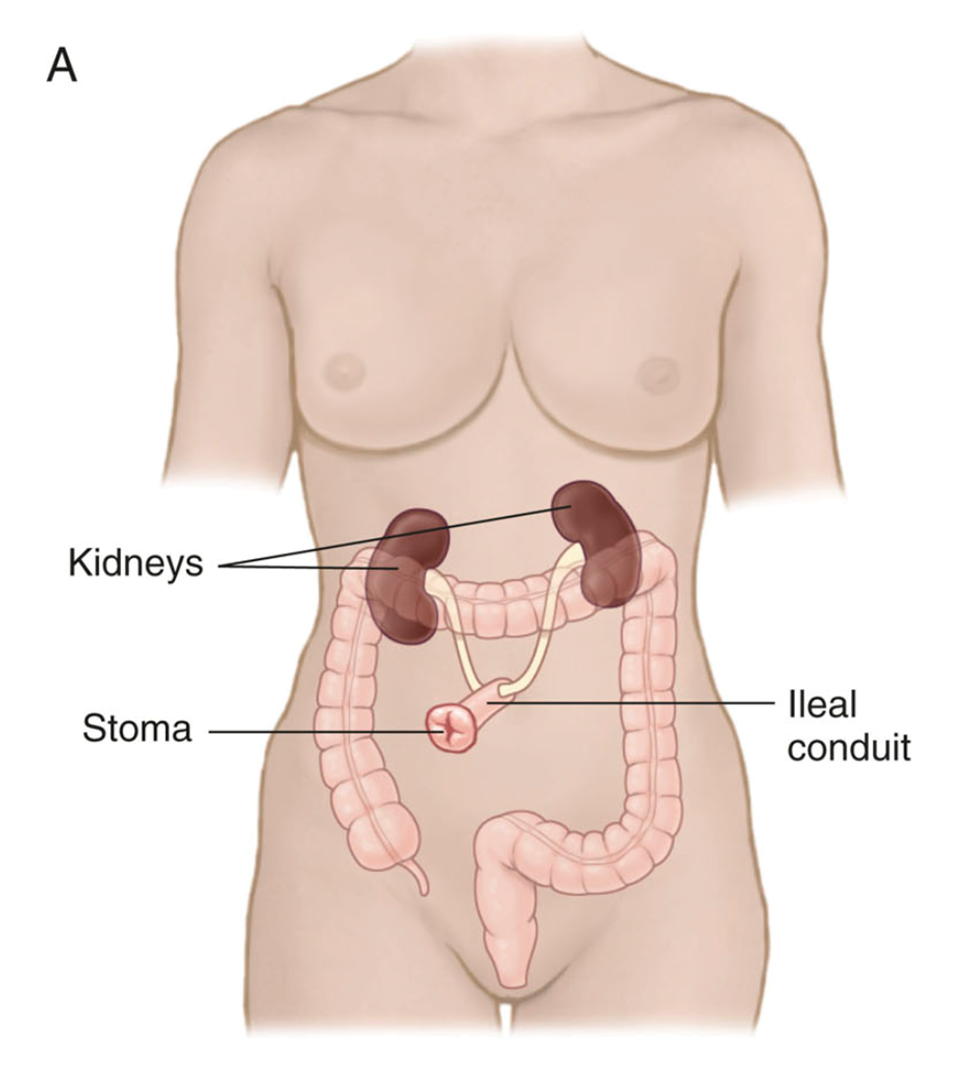
rerouting of ureters to a stoma using a part of the pts intestine ex ileal conduit, or ureterostomy
Incontinent Urinary Diversion characteristics
may have a larger stoma (ileal conduit) or one flush with the skin (cutaneous ureterostomy)
appliance is applied to collect urine
peristomal skin health is essential=must never leak onto skin
complications=infection, stomal issues, blockage, peristomal skin issues
Continent Urinary Diversion def (urostomy)
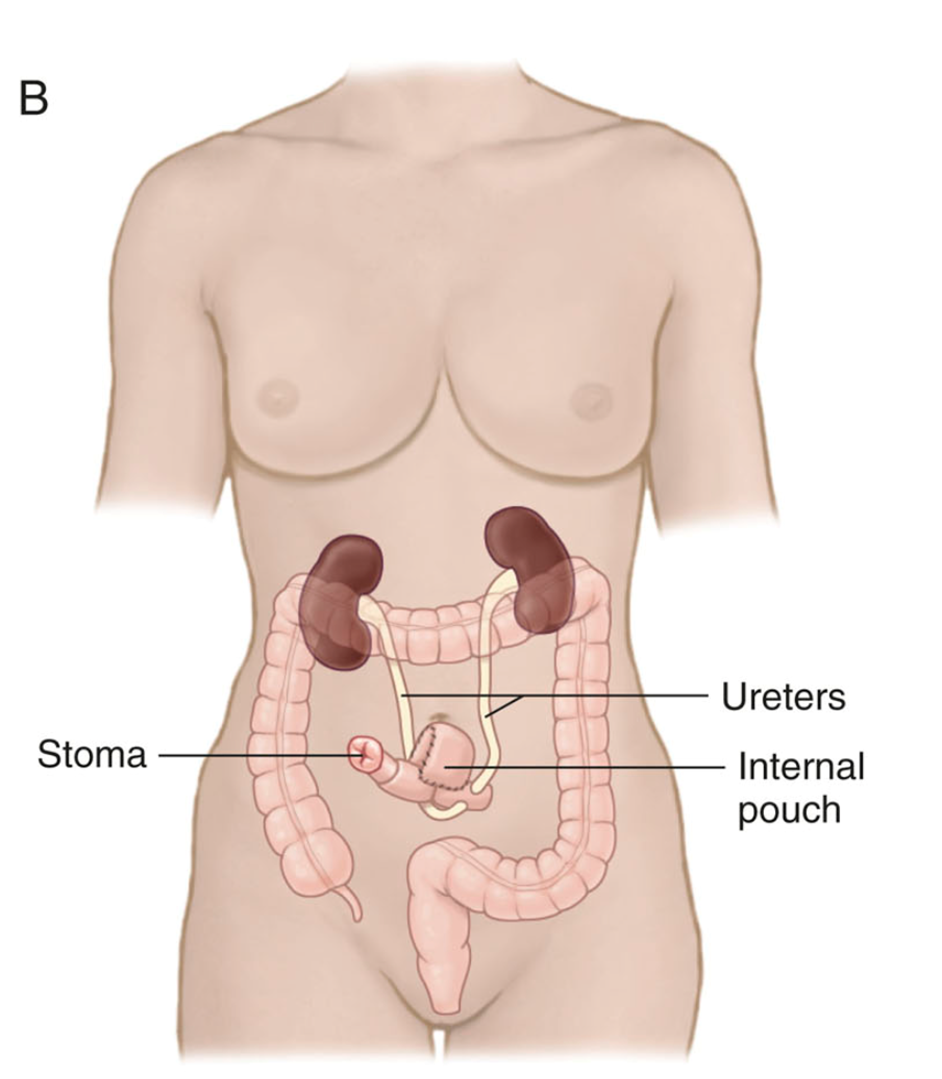
rerouting of ureters to a pouch (reservoir) and stoma created by a portion of the large intestine and ileum
Continent Urinary Diversion characteristics
pouch emptied with a clean catheter q4hrs, and is covered by a small dressing
gives pt more control over the passage of urine
complications=infection, blockage, stomal and peristomal skin issues
no drainage should leak or touch the skin=irritating, and cause skin breakdown
Ileostomy appearance and when does fecal drainage start
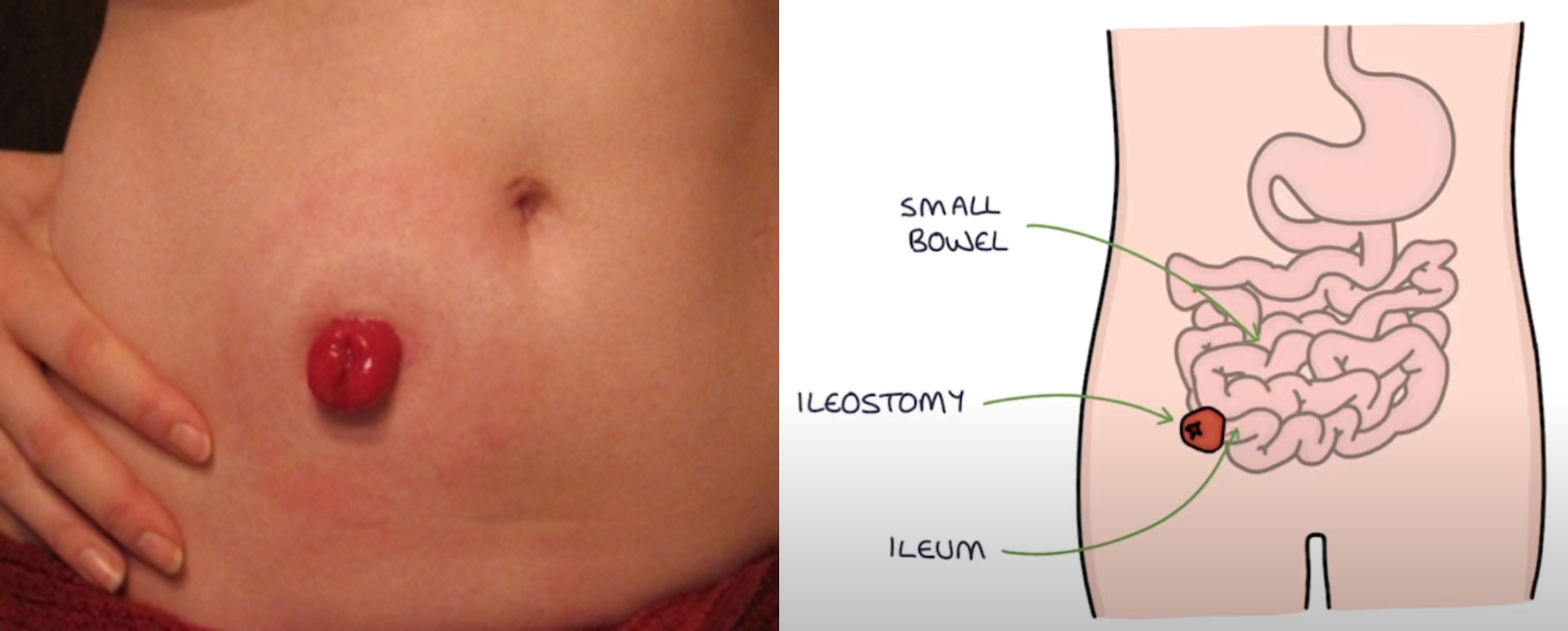
protruding stoma d/t f risk that fluid will irritate stomal area
fecal drainage begins 24-48 hrs after surgery
ileostomy stool/frequency characteristics
production is frequent
fluid like-to mushy, dark green, usually not odorous
when does the colostomy start to function with output
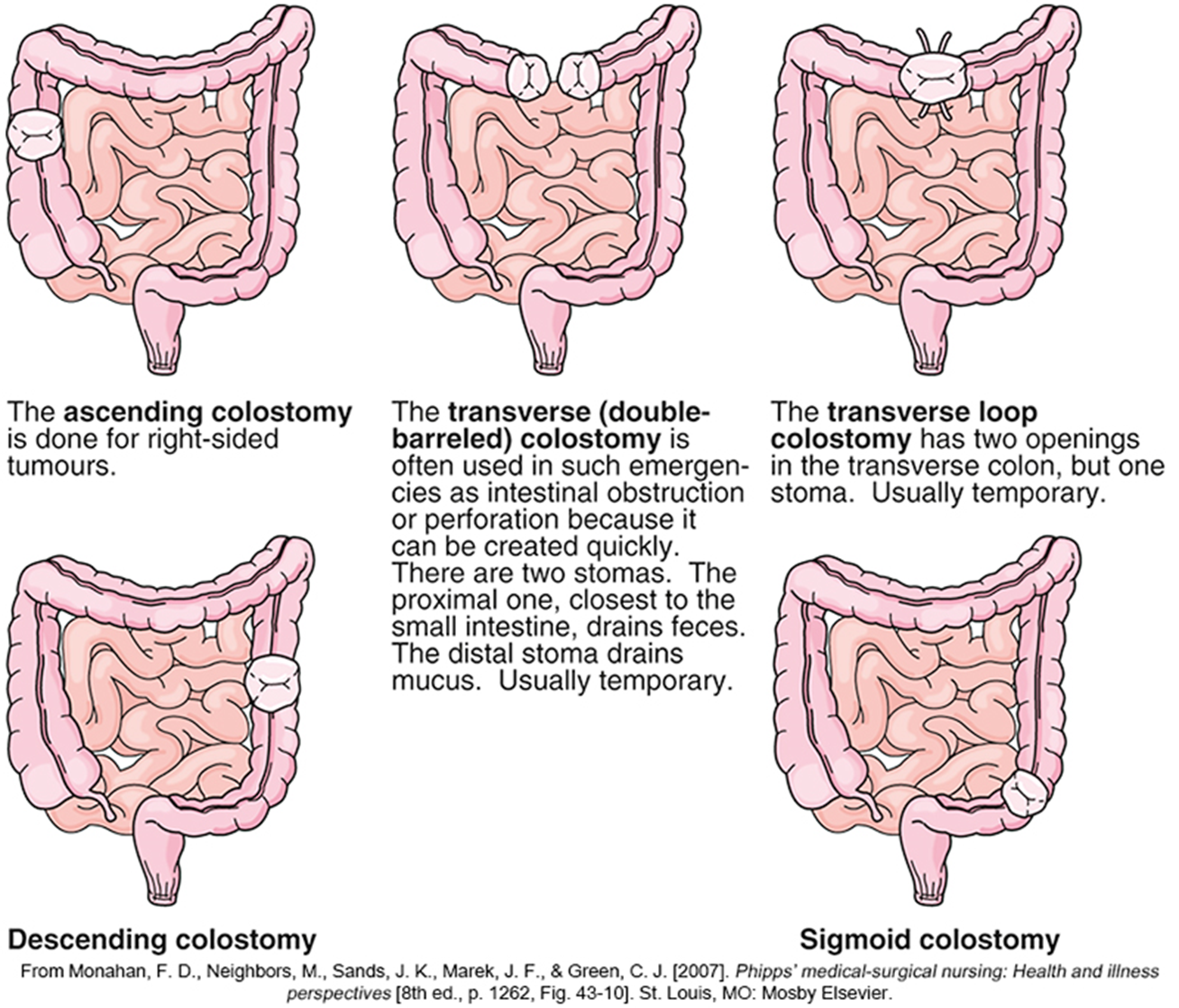
3 to 6 days after surgery
stool more firm
urostomy frequency rate and consistency of output
frequent/continuous
urine, may have mucous threads
colostomy frequency rate and consistency of output
less frequent, few times a day
semi solid or formed with gas
one piece system colostomy characteristics
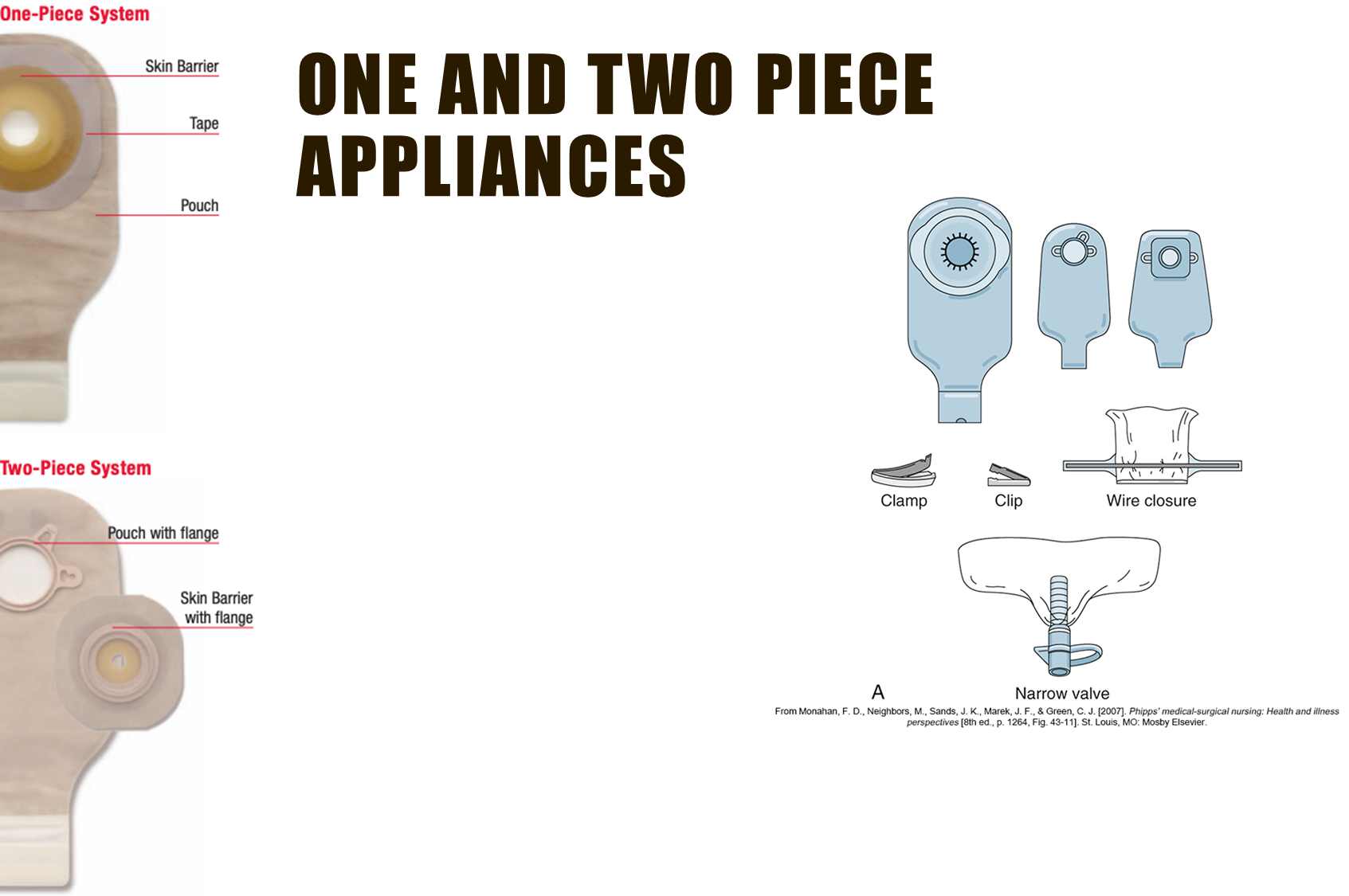
skin barrier is already attached to the pouch, peel/stick
pouch lies flat against the skin and may show less under clothing
bulge/hernia near your stoma=best fit with a one-piece pouch
two piece system colostomy characteristics
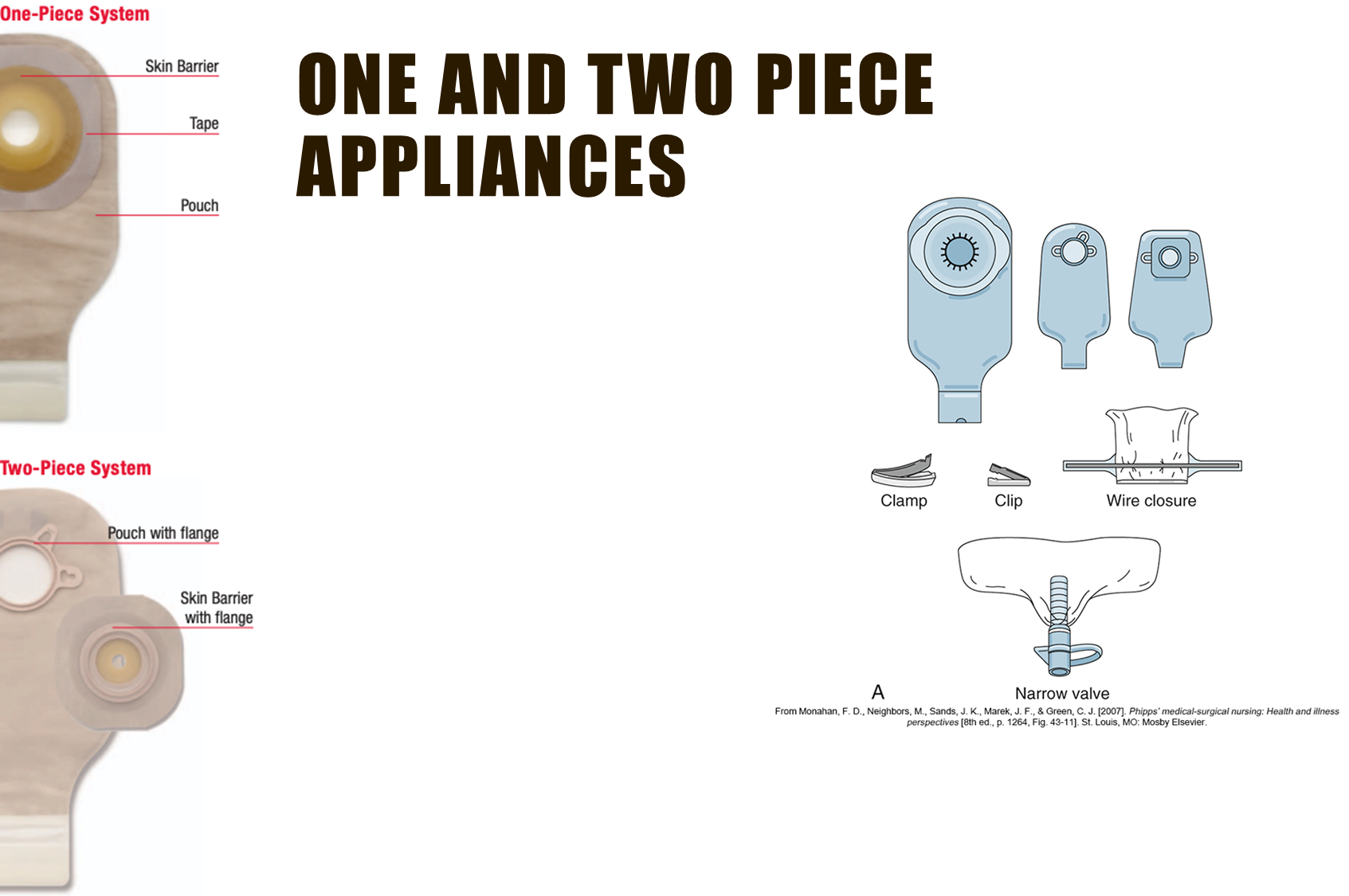
skin barrier is separate from the pouch, pieces snap together with a flange
allow you to apply a new pouch without removing the skin barrier from your body each time
can wear diff pouches depending on activity level
can put your fingertips under the flange to help prevent pressure
how often are ostomy appliances changed?
changed at least every 7 days
how do we cleanse the Peristomal area
use a soft cloth moistened with warm water to cleanse peristomal area after appliance has been gently removed
dry thoroughly
may not need soap or cleansers, but if used rinse off
dont use moisturizers on the peristomal skin area = reduces adherence of appliance
only use products developed for use in ostomy care, and those rx such as a skin protectant
Measuring the stoma pic
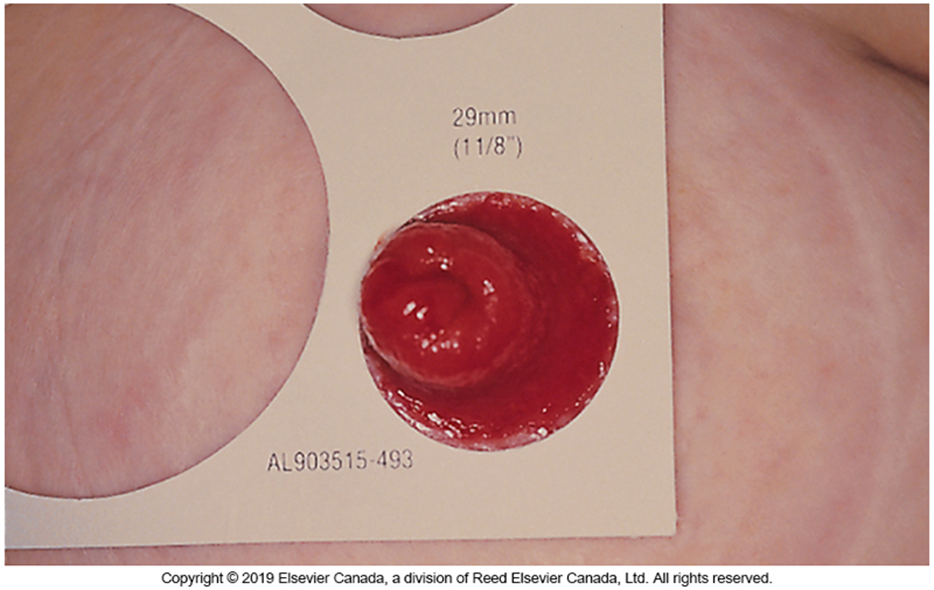
add 1 1/8th inch
what can we use to in crevices to fill and gaps and make wafer application easier
paste
Teaching for a patient with an ostomy (GI), what to mention
management and changing of appliance, supply acquisition
address concerns re self image, sexuality, pregnancy etc
supports in community
fluids and electrolytes (Ileostomy) must monitor losses especially during hot weather, exercise, and when ill, and replace
expected vs unexpected findings, monitoring for complications; peristomal skin issues, diarrhea, blockage, stomal issues; stomal stenosis, dehiscence, prolapse, other ex urinary calculi (stones)
dietary recommendations for ostomy pts
if new usually begin with a low residue diet initially to allow bowels time to adapt
few dietary restrictions but should avoid hard to digest food items=popcorn, corn, poppy seeds etc
avoid foods that cause odor or gas
flush stoma unexpected finding

may be intentional (by the surgeon) or occurs over time
increased risk of peristomal skin exposure to effluent from stoma
requires use of a convex pouching system or stoma paste or barrier ring
retracted stoma unexpected finding
recessed slightly below the skin
can occur as a result of internal scar tissue formation, changes in patient’s weight, or significant nutritional deficit
requires use of a convex pouching system or stoma paste or barrier ring
prolapsed stoma unexpected finding

when the intestine extends outward, over itself much further than expected (expected is 2-3 cm)
there is a risk that the the prolapse can progress to intussusception = this is a surgical emergency
requires surgeon consult
peristomal candidiasis unexpected finding

causes=leakage from stoma, perspiration, antibiotic therapy, warn/humid environments, broken skin.
S&S=yeast irritation - itchy, bumpy red skin
yeast infection may simultaneously occur in vaginal area, armpits, mouth, or any skin folds (ex buttocks, groin)
allergic contact dermatitis unexpected finding

causes=exposure to irritants on the skin ex tape, tegaderm, skin barriers, soaps, powders, pastes, or even the ostomy wafer
S&S=red itchy broken skin, yeast irritation in area under pouching system
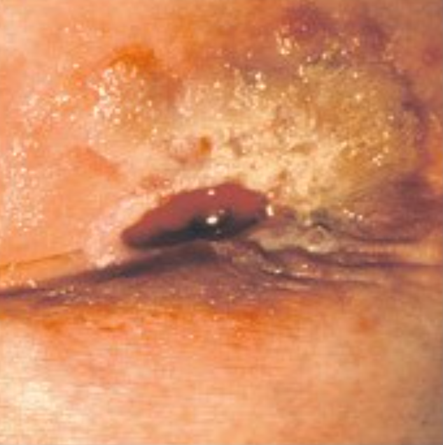
irritant dermatitis unexpected finding
causes=inflammation of peristomal skin from contact with urine or stool leaking from under the pouching system
ex not a good seal of the wafer to the peristomal skin
S&S=redness, pain, open-weeping areas of the skin
pressure injury/ulcer unexpected finding

causes=direct contact and pressure from an ostomy appliance, tight clothing, peristomal hernia, or repetitive contact from activity or work-related habits
S&S=pain or bleeding, irregularly shaped ulcer, pouch leaking, decreased wear time of ostomy appliance
if left untreated, may develop into fistulas
The nurse is emptying a colostomy bag for a patient. Which of the following needs to be reported immediately?
presence of blood in the stool
should seek medical attention immediately if;
stoma is protruding further out than usual
stoma appears dark red/purplish in color