UPDATED SESATS Congenital Cardiac
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
87 Terms
What complications are higher in atrial switch over long term (~10 years) for Transposition of great arteries surgery?
higher rates of arrhythmias and ventricular dysfunction (30-40%) at 10 years.
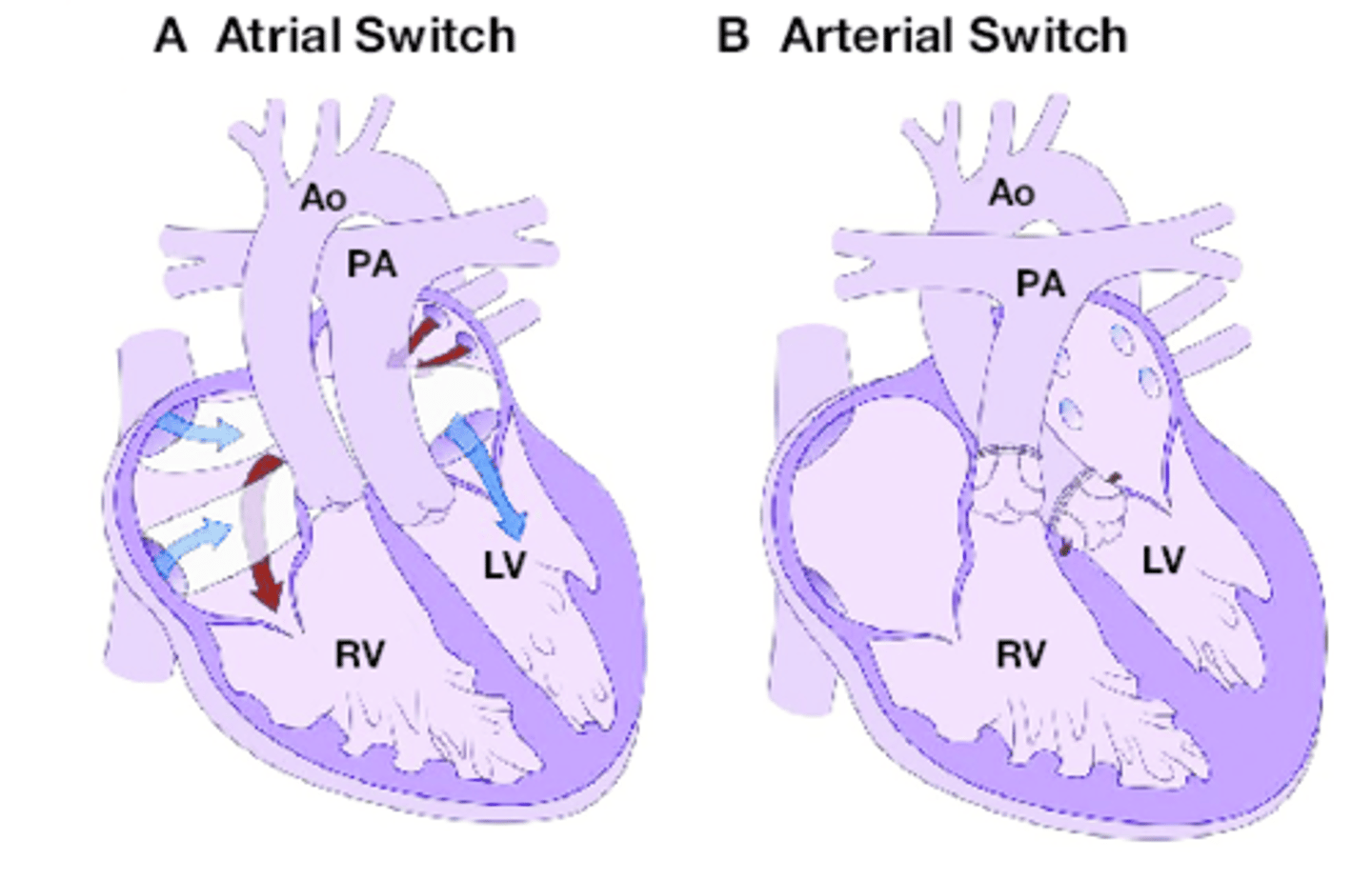
What complications are higher in arterial switch over long term (~10 years) for Transposition of great arteries surgery?
Arterial switch: Right ventricular outflow tract (RVOT) stenosis is the most commonly seen complication requiring re-intervention following arterial switch.
What intraoperative pressure is needed in the femoral artery to prevent paraplegia during coarctation repair?
In children over 1 year a femoral pressure >50 mmHg during the cross-clamp time is adequate to prevent paraplegia.
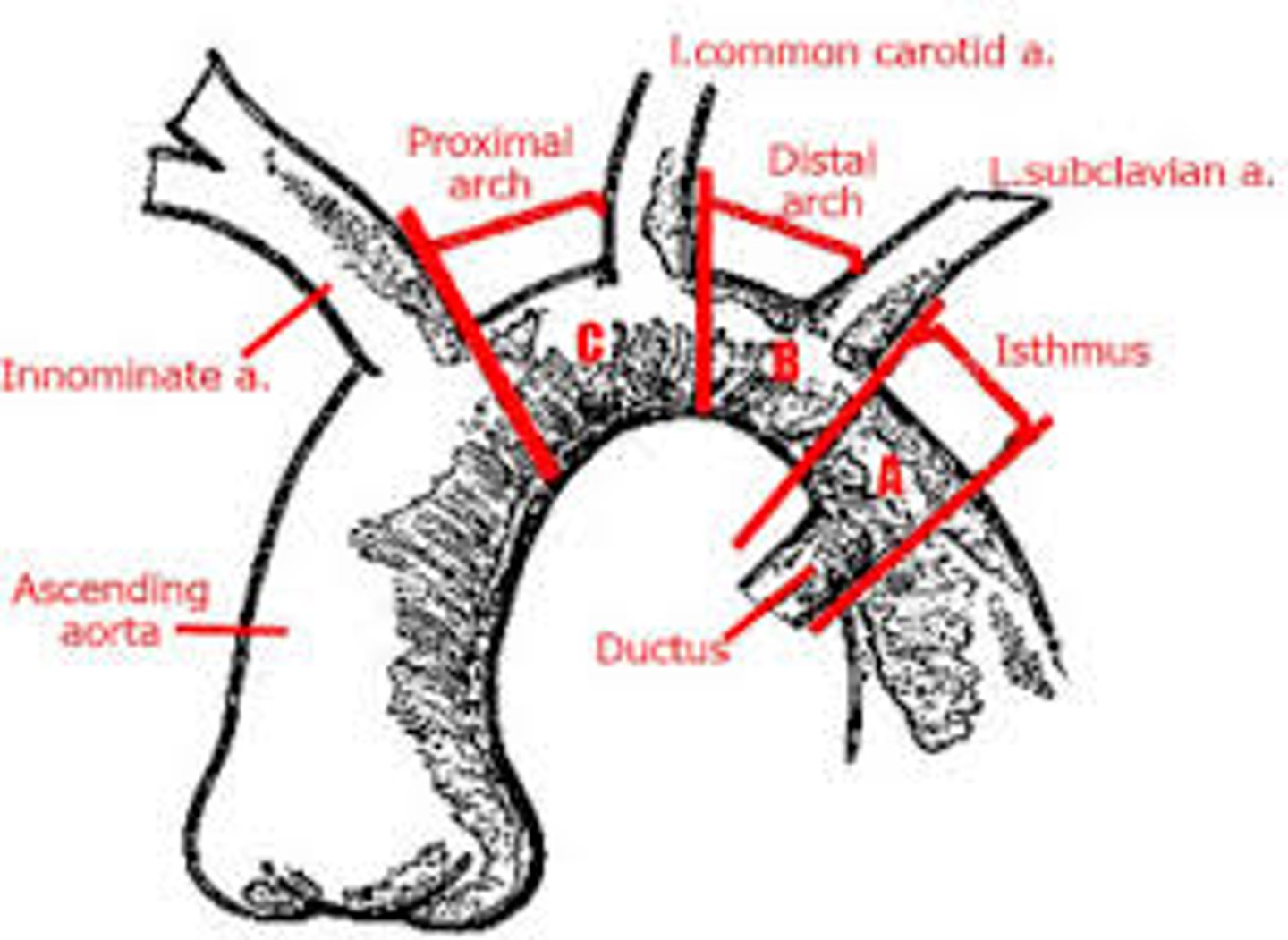
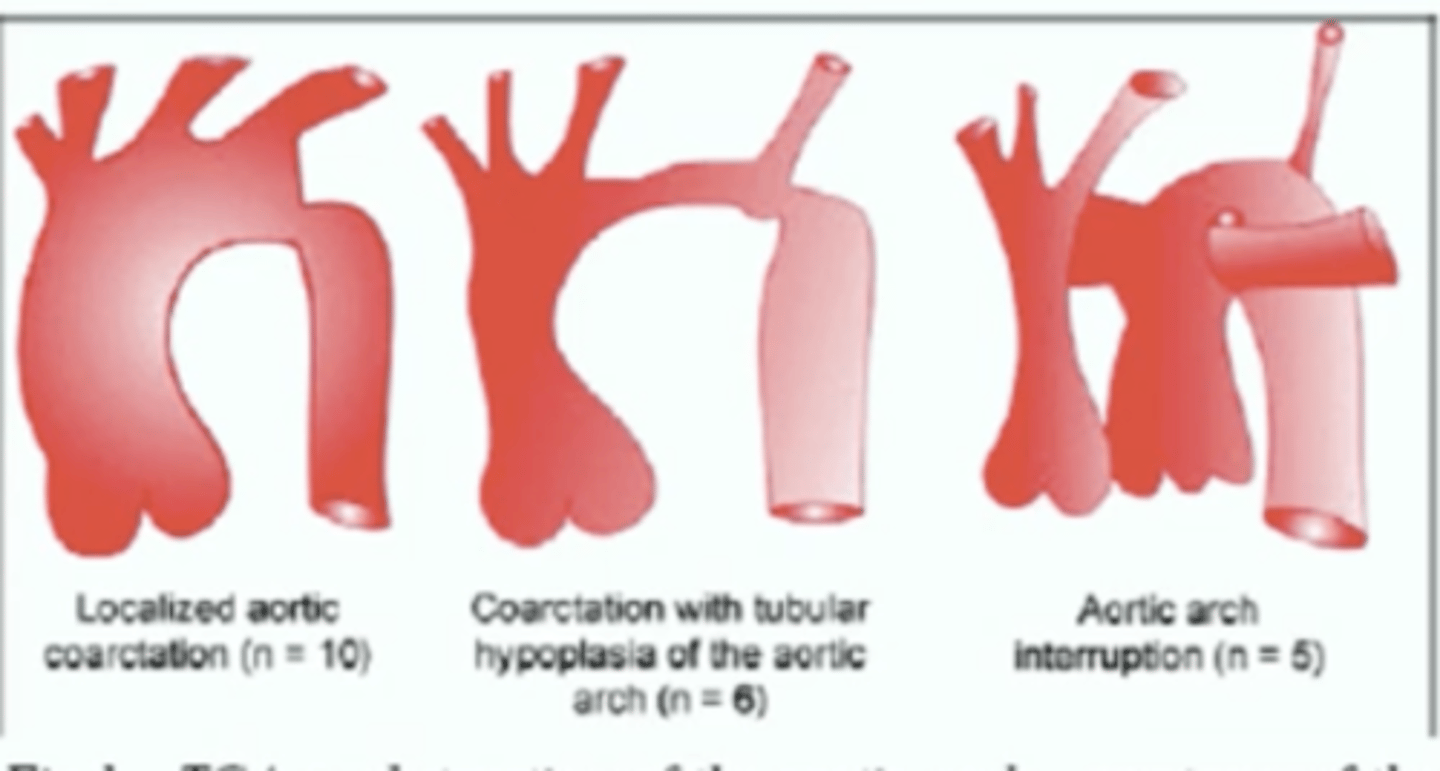
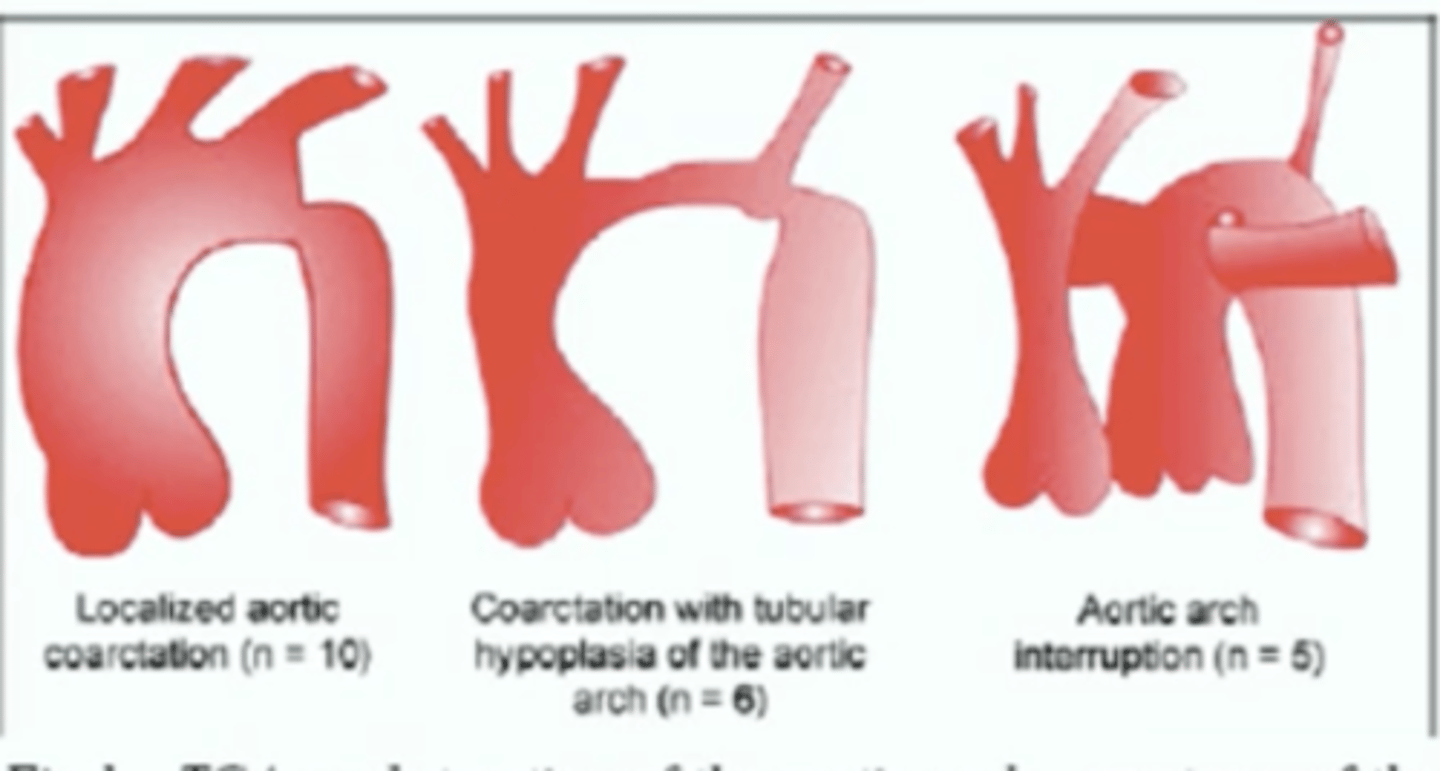
Types of interrupted arch
Most common is type B
What is the most common indication for reoperation after repair of AVSD.
left atrioventricular (AV) valve regurgitation (mild leave alone but if moderate/severe then reoperate).
After fixing transposition of the great arteries, these patients have increased risk of what?
3rd degree heart block.
Their conduction system anterior to the mitral valve and posterior to the pulmonary valve. This long pathway is associated with an elevated risk of developing of third-degree (complete) atrioventricular heart block.
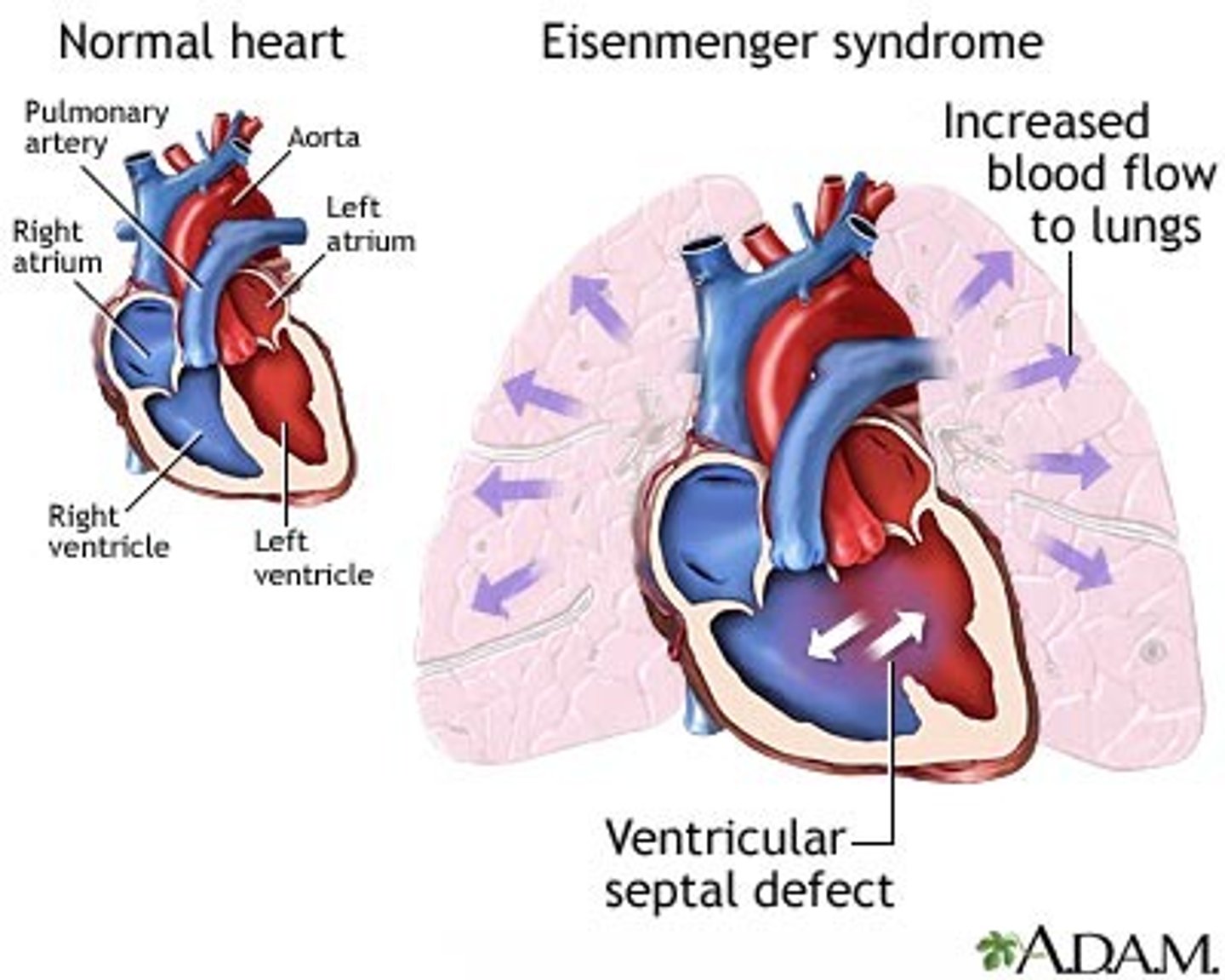
Eisenmenger Syndrome and Strongest mortality predictors
Reversal of flow from left to right to right to left due to development of pHTN over time.
Physiology presents in 2nd and 3rd decades of life leading to death in 40's and 50's.
Hypoxia and ventricular dysfunction are greatest predictors of mortality.
When can consider (although controversial) ASD secundum closure with device rather than open?
1. ASD size (mm)/Patient weight (kg)= <1.2
2. device to septal length ratio is < 0.58
3. Rim is present (for device closure)
Open vs transcatheter approach in infants <8kg is still controversial but transcatheter is growing and advancing.
*In general safer answer is open at this time.
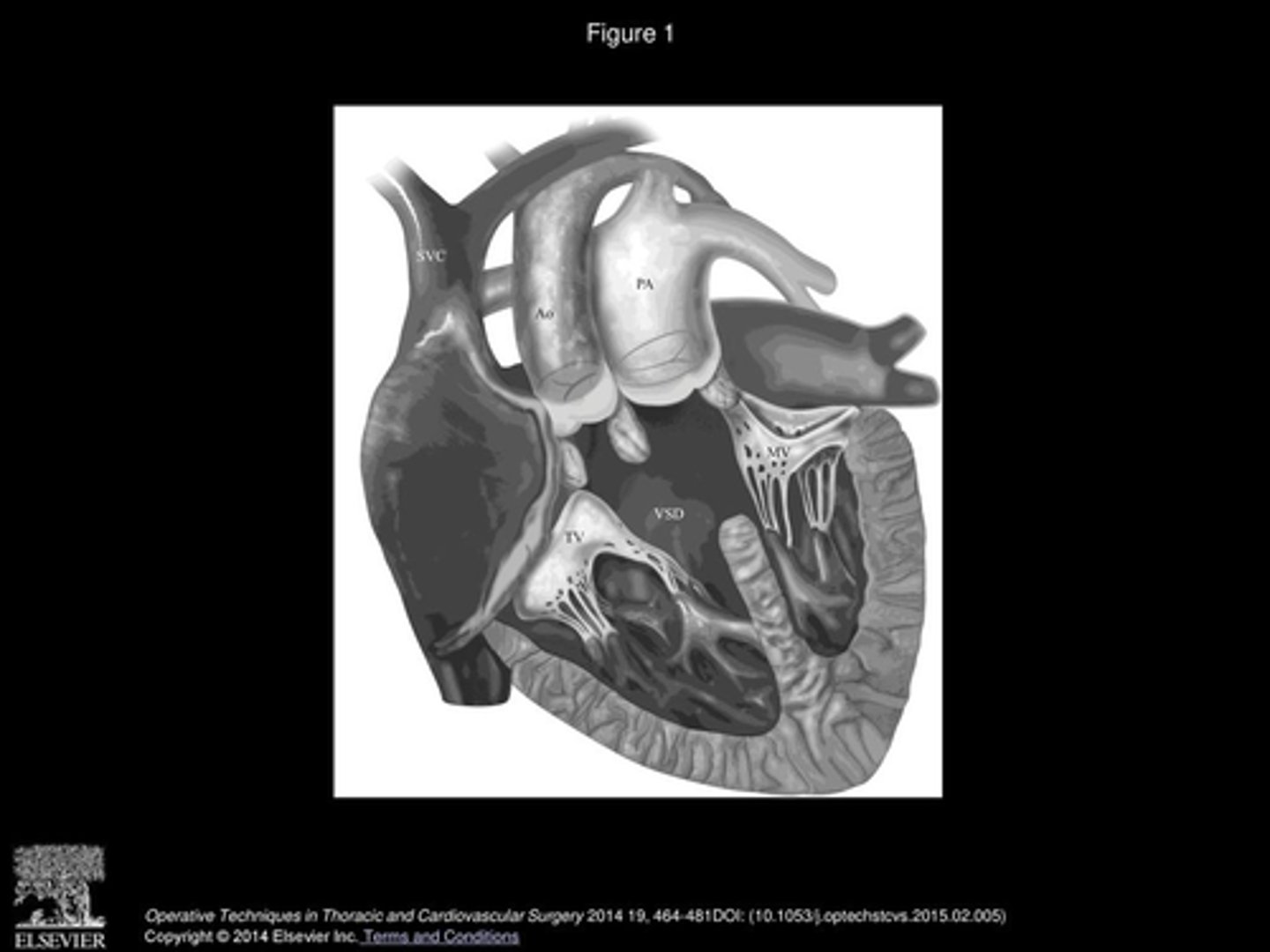
What VSD closure has highest risk of heart block?
Inlet VSD has greatest risk of heart block (7-12 %)
How to repair a perimembranous and muscular VSD at the same time?
DO NOT connect the VSDs and do one large patch bc the child will have heart block (inferior edge of perimembranous and superior edge of muscular VSD have conduction portions).
Do two separate patches.
Where does the conduction system lie for VSDs depending on the type?
For most vsds (perimembraous, inlet and subaortic), the conduction system lies on the inferior rim.
Exceptions: Transposition patients and muscular vsds, lie on the superior portion of the rim
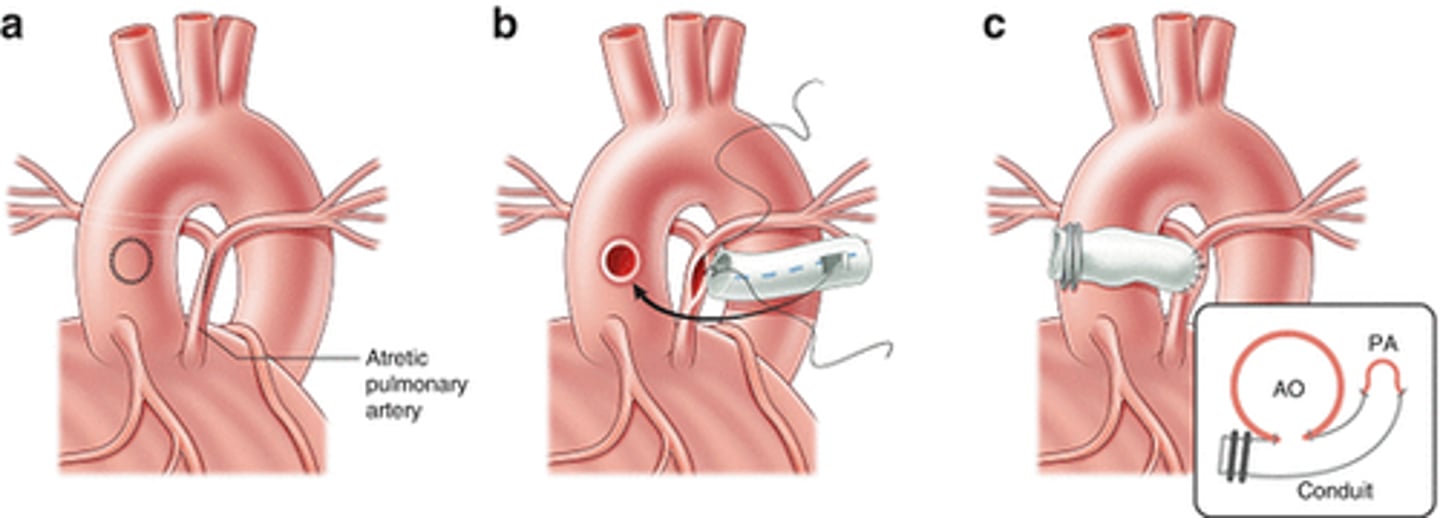
How to improve blood flow to small PA with child who has pulmonary atresia with VSD and multiple aortopulmonary collateral arteries (MAPCAs)
the sole source of blood flow to lungs is from MAPCAs.
The child needs better flow to small PA to enhance it's growth before ligating the MAPCAs. This is done by creating prosthetic shunt from aorta to PA via sternotomy or by creating a Mee shunt (creating direct anastomosis of tiny PA to the ascending aorta)
PVR equation
PVR (woods units)= (mPAPxPCWP)/Qp
*if want in dynes/sec/cm2 then take number in woods and multiple by 80.
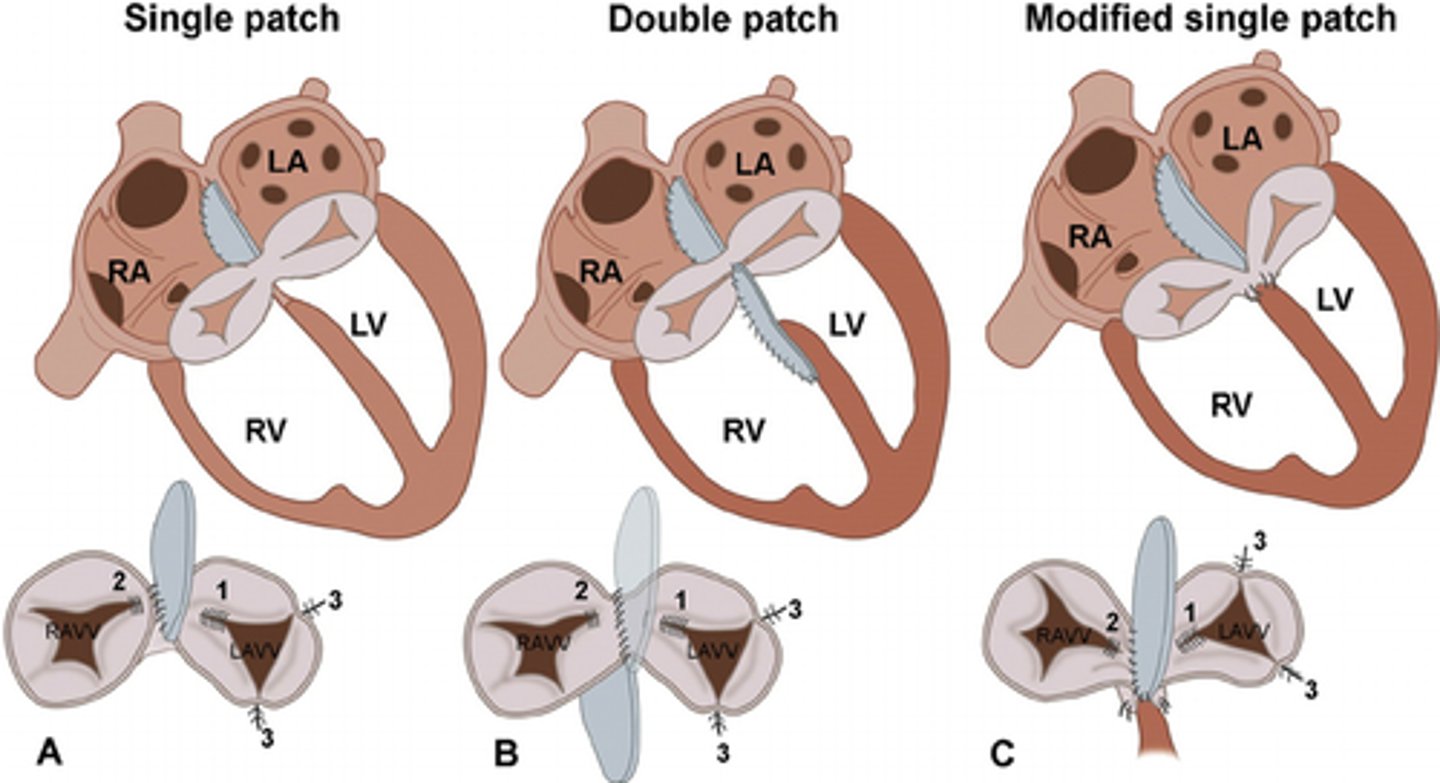
Modified single-patch repair for AV canal ASD and VSD repair
take the septation line of the common AV valve and secure it to the crest of the VSD to serve as closure of the VSD component then use a single patch to close the ASD.
** useful when the VSD is shallow or when there is significant chordal attachments to the crest of the VSD, making it more difficult to insert a VSD patch
Most common reason for reoperation after AVSD repair
development or persistence of AV valve regurgitation.
Not uncommon to have mild AV valve regurgitation after repair but anything more than moderate will likely progress over time.
Double orifice left av valve management
complicated 5% of all cases of AV septal defect.
In most cases the accessory cleft can be closed and treat it as an uncomplicated AV septal defect.
The accessory cleft is not a part of the original leaflets so bridging the tissues by dividing between isn't feasible.
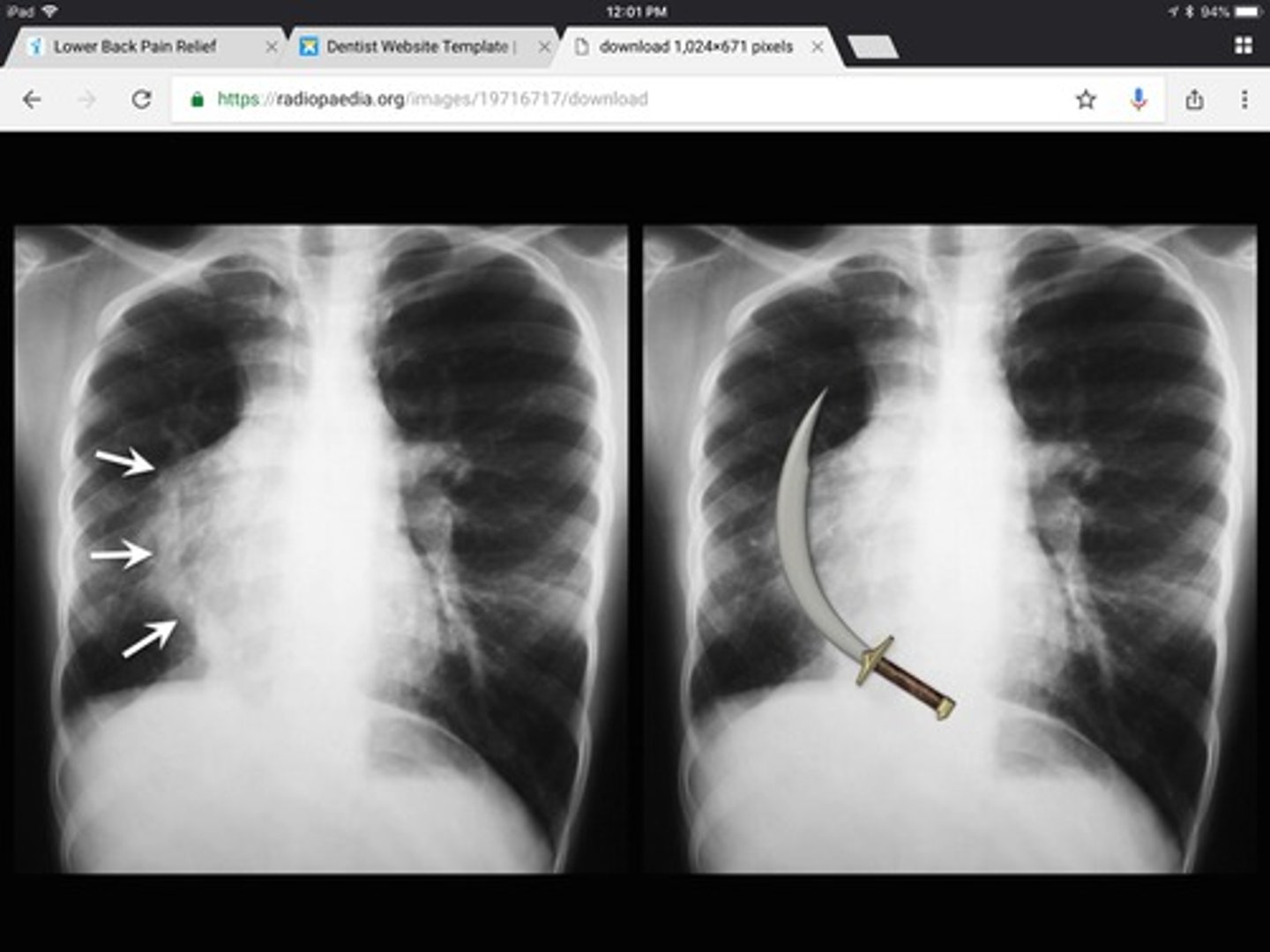
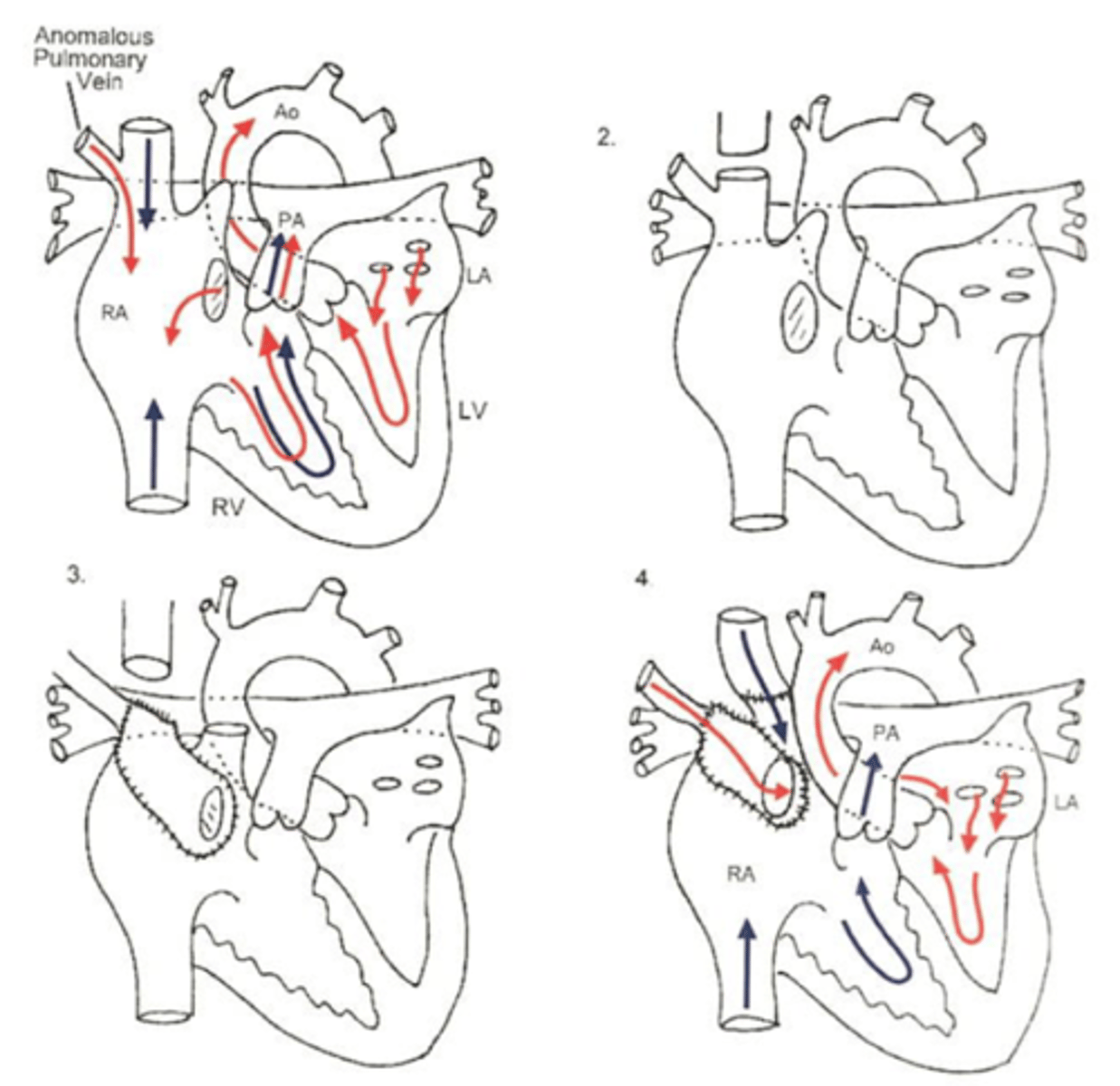
What is Schimitar syndrome?
rare congenital anomaly where pulmonary veins of entire right lung drain to the IVC.
What technique for TAPVR has the best outcomes?
"sutureless" pericardial pulmonary veins into pericardial pouch has best outcomes.
Ductus closure complications
MOST common is left vocal cord paralysis
others are bleeding, pneumothorax, diaphragmatic paresis (1-4%)
What peak gradient criteria between the upper and lower extremities tells you that you have recurrent coarctation s/p repair?
peak gradient of>20 mmHg
Factors that increase recurrence of coarctation after repair performed
Repair before 2-3 months, weight less than 2 Kg, post operative residual ductal tissue.
*Least likely with extended end-to-end anastamosis
What coarctation repair has a higher rate of aneurysm?
Aortoplasty because use Dacron patch and the area opposite the patch is at risk for further dilation due to difference in tension between patch and native tissue.
*Least likely to have aneurysm with extended end-to-end anastamosis
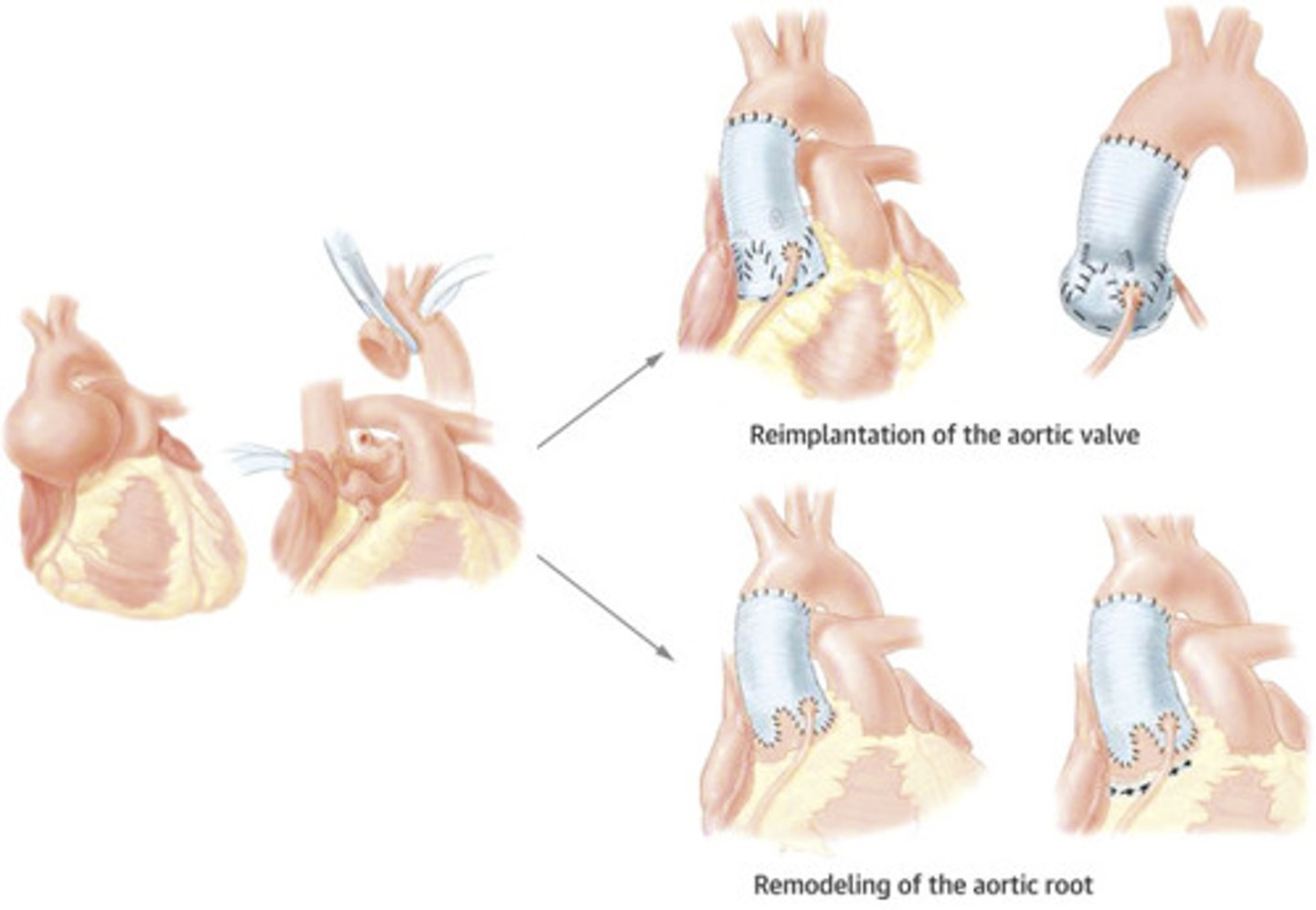
Aortic root repair: Remodeling vs Reimplantation.
Remodeling: only stabilizes the sinus of valve but not the annulus. Works best with elderly people with small annulus who you are not concerned for further dilation (DO NOT HAVE connective tissue disorders).
Reimplantation: stabilizes annulus AND sinus. Works well with Marfans patients who you worry about further dilation/regurgitation. <2% mortality. Valve competence is 90% at 20 years.
Marfans: What gene, inheritance pattern, how common and what subtype is the worst.
FNB1 gene
autosomal dominant
1 in 5000-10000 people.
2432 subtype has worst outcome with most aggressive progression of cardiovascular issues.
What to expect when see unexplained mitral valve regurgitation in a structurally normal heart in infant
ALCAPA until proven otherwise
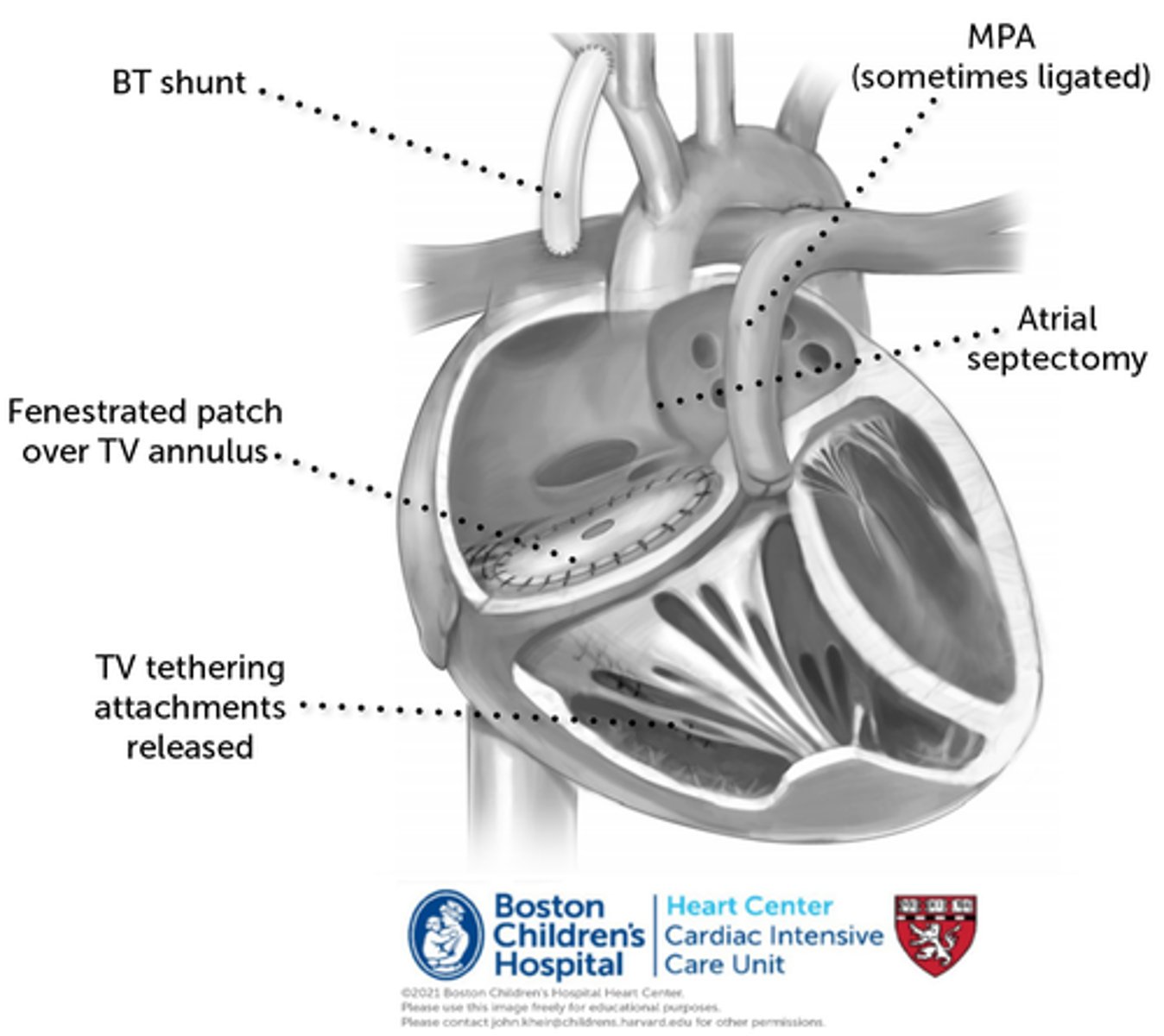
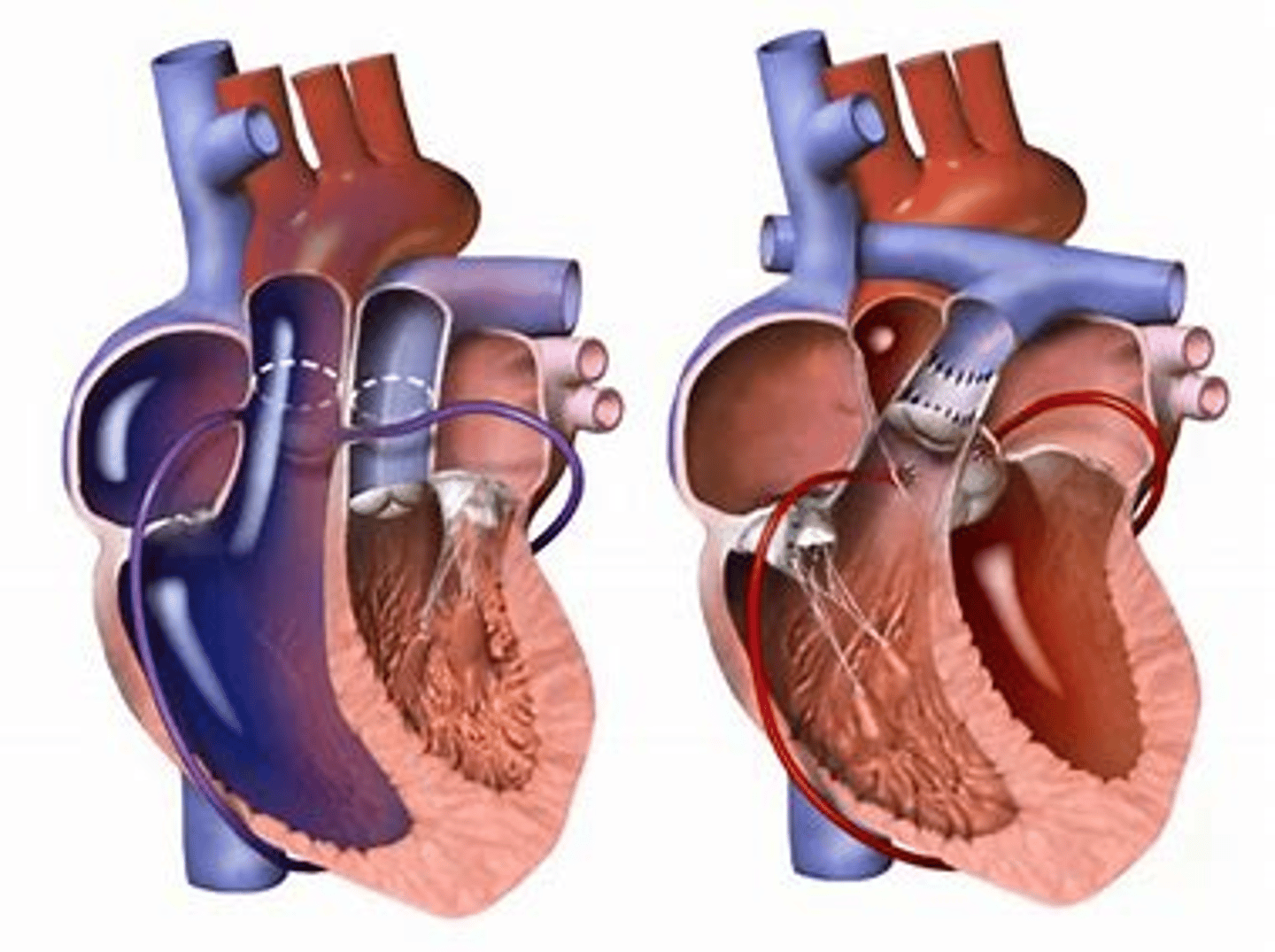
Starnes Procedure for Ebsteins Anomaly
Simpler option for palliation for sick baby compared to Cone procedure.
Involves patch closure of the tricuspid valve and modified BT shunt for pulmonary flow. Requires ASD.
Theoretically can be converted to a repair or replacement of TV at later point.
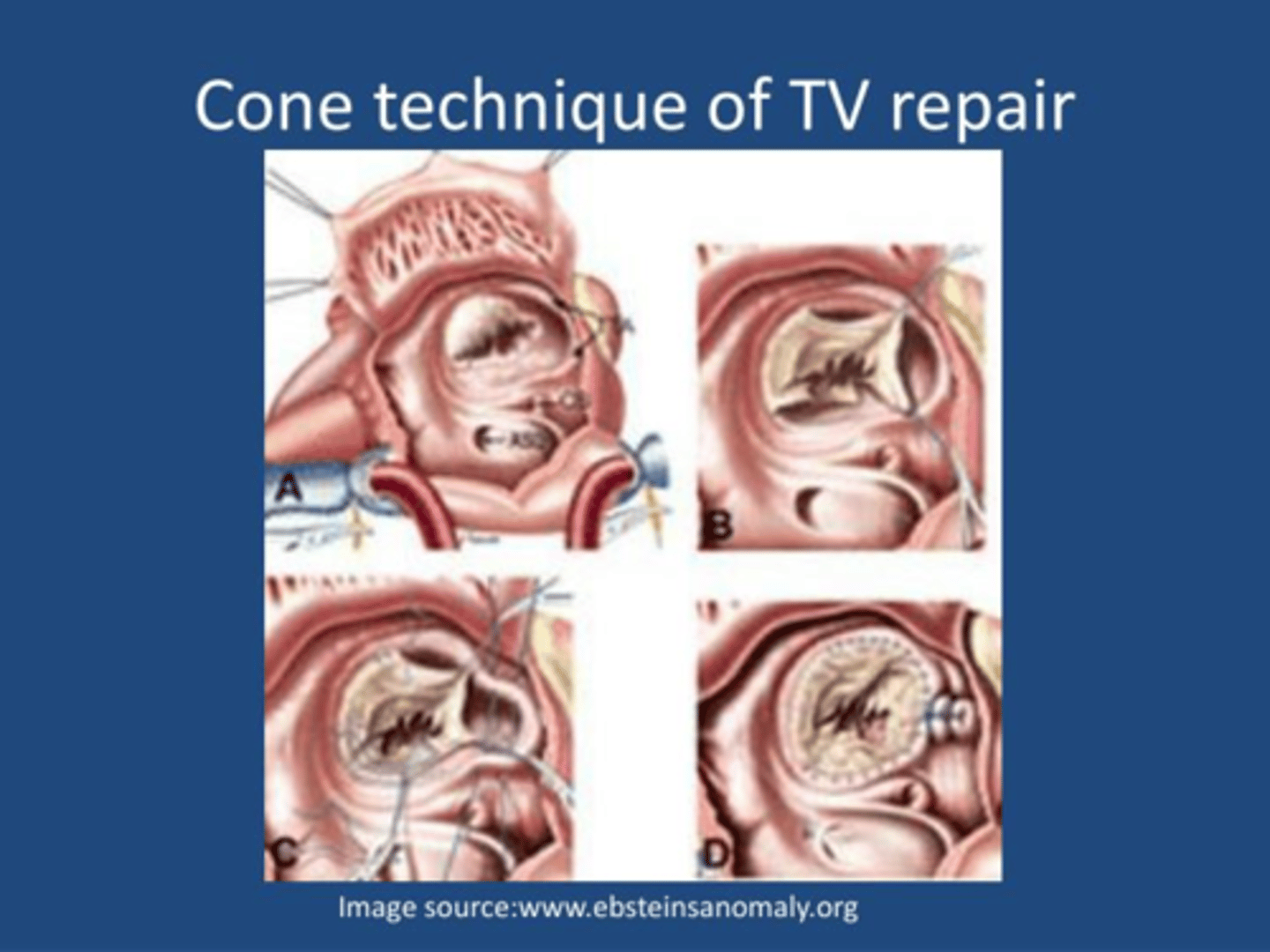
Cone Procedure for Ebsteins Anomaly
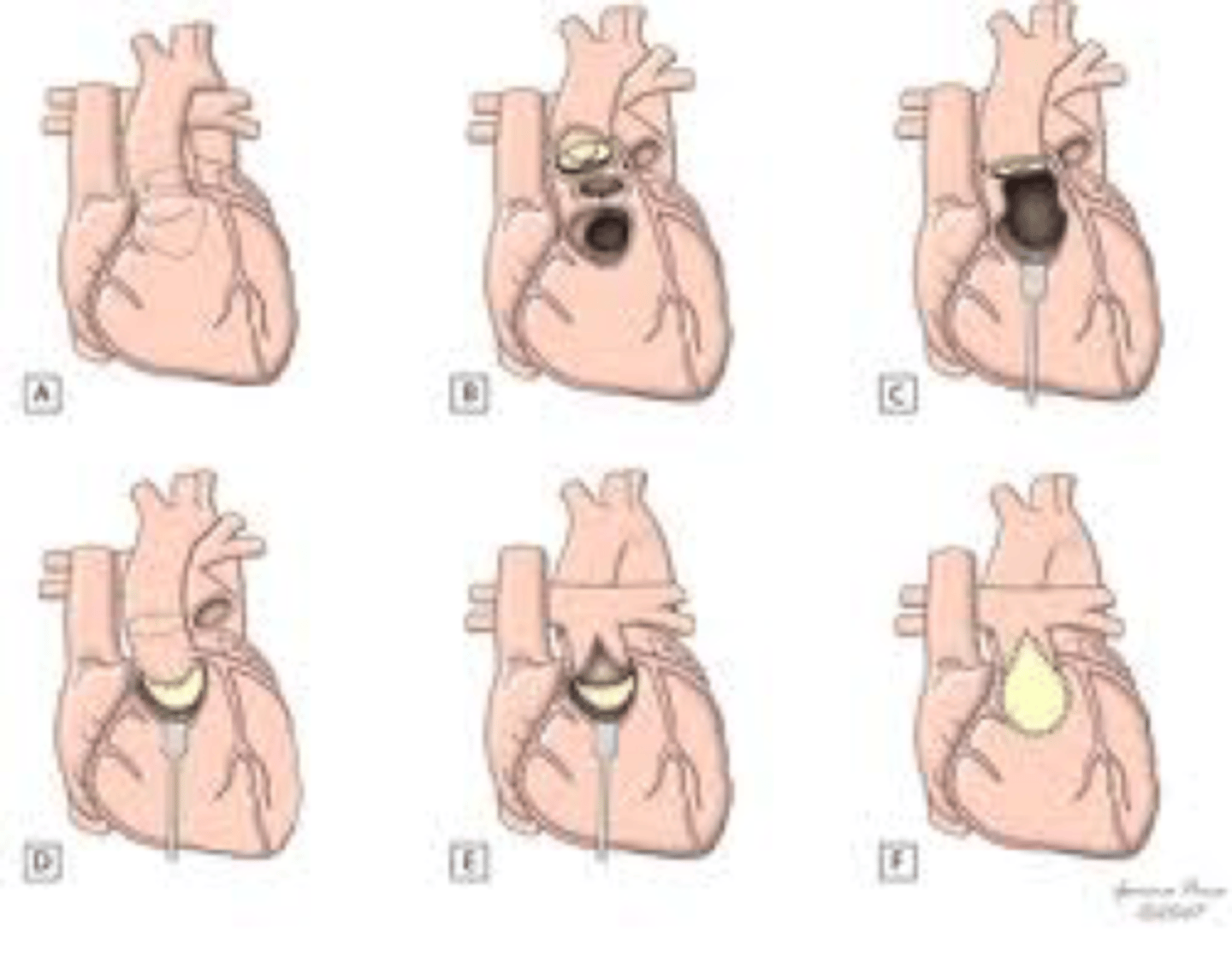
Operative steps for Ebstein’s anomaly repair.
A:Opened right atrium showing displacement of the tricuspid valve.
B, Detached part of the anterior and posterior leaflet forming a single piece.
C, Clockwise rotation of the posterior leaflet edge to be sutured to the anterior leaflet septal edge and plication of the true tricuspid annulus.
D, Complete valve attachment to the true tricuspid annulus and valved closure of the atrial septal defect.
May not be tolerated by a very sick baby in which a Starnes procedure may be better alternative for palliation.
CTR (cardiothoracic ratio) and meaning
Cardiothoracic ratio on cxr
cardiac width/chest diameter on AP film at 8th rib
In normal healthy infants normal range is 53%
Great Ormond Street Echo (GOSE): for Ebsteins anomaly
ratio of sum of right atrium and right atrialization to the ratio of the other chambers.
if >3 in cyanotic patients, mortality is 100%.
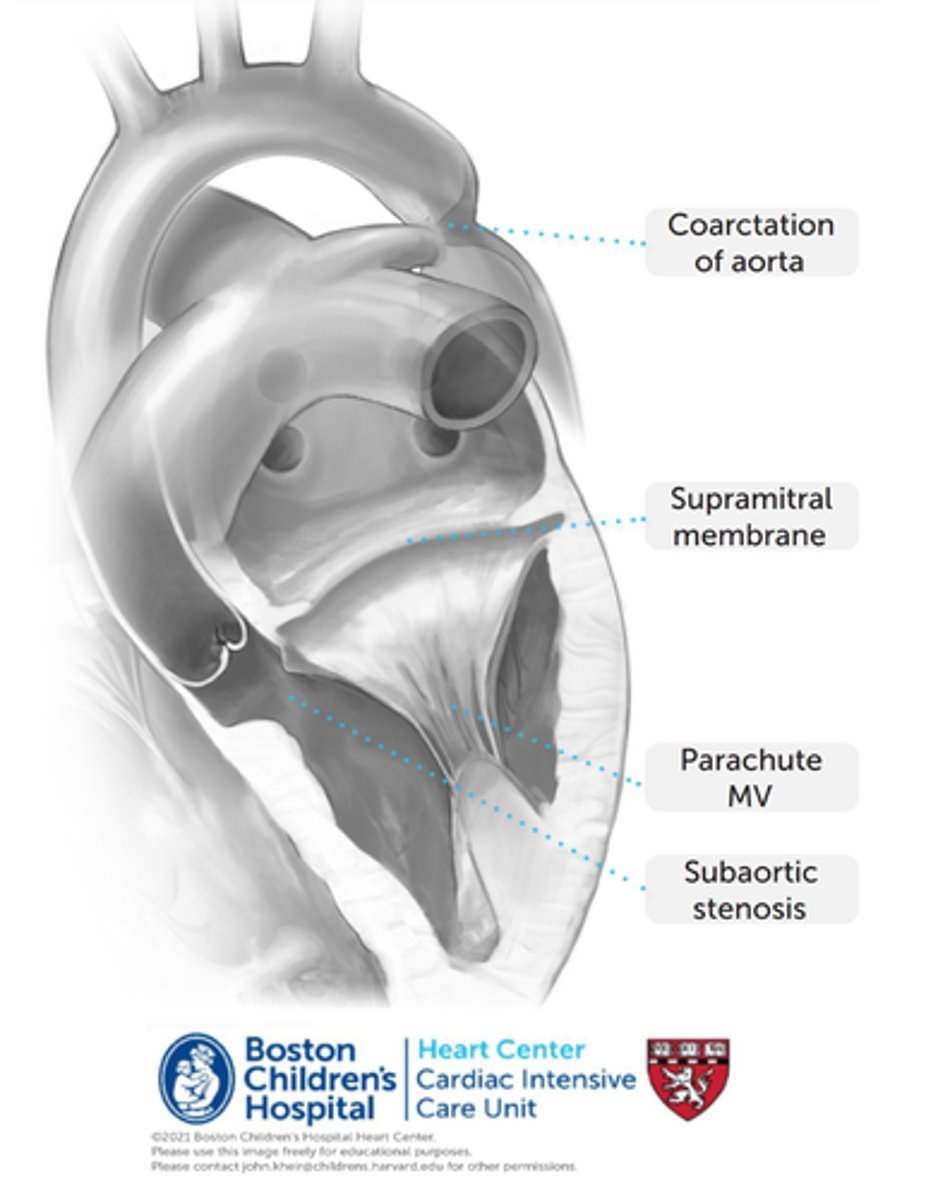
What is Shone's syndrome?
Rare congenital heart disease involving 4 left sided heart lesions. The Supravalvular mitral valve membrane is the first to occur and the other deformities that are more downstream occur after that.
1) Supramitral membrane in the left atrium. In the most extreme cases, this may be a stenosing, perforated diaphragm above the mitral valve at the mitral annulus. More commonly, this represents a non-obstructive ridge.
2) Parachute deformity of MV. Papillary muscles converge on a single papillary head (or narrowly spaced papillaries), which limits MV opening.
3) Subaortic stenosis. Usually associated with subaortic flow acceleration due to marked focal hypertrophy (bulging) of the basal anterior ventricular septum, resulting in a fibrous ridge on top of the muscular bulge.
4) Coarctation of aorta
When to place ICD for hypertrophic obstructive cardiomyopathy septal myectomy
when patient has had prior cardiac arrest or sustained vtach in past, family history of cardiac arrest or septum >30mm.
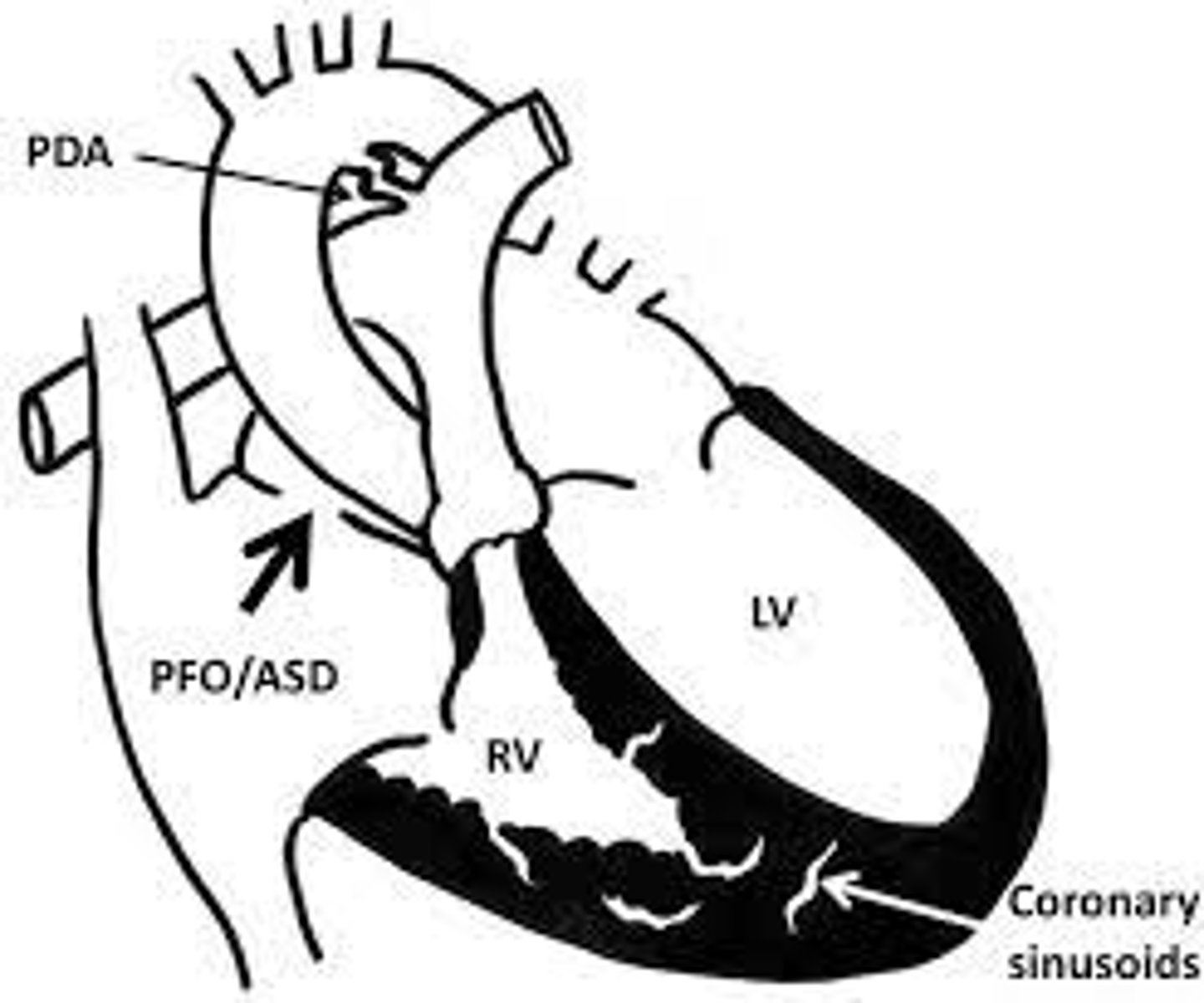
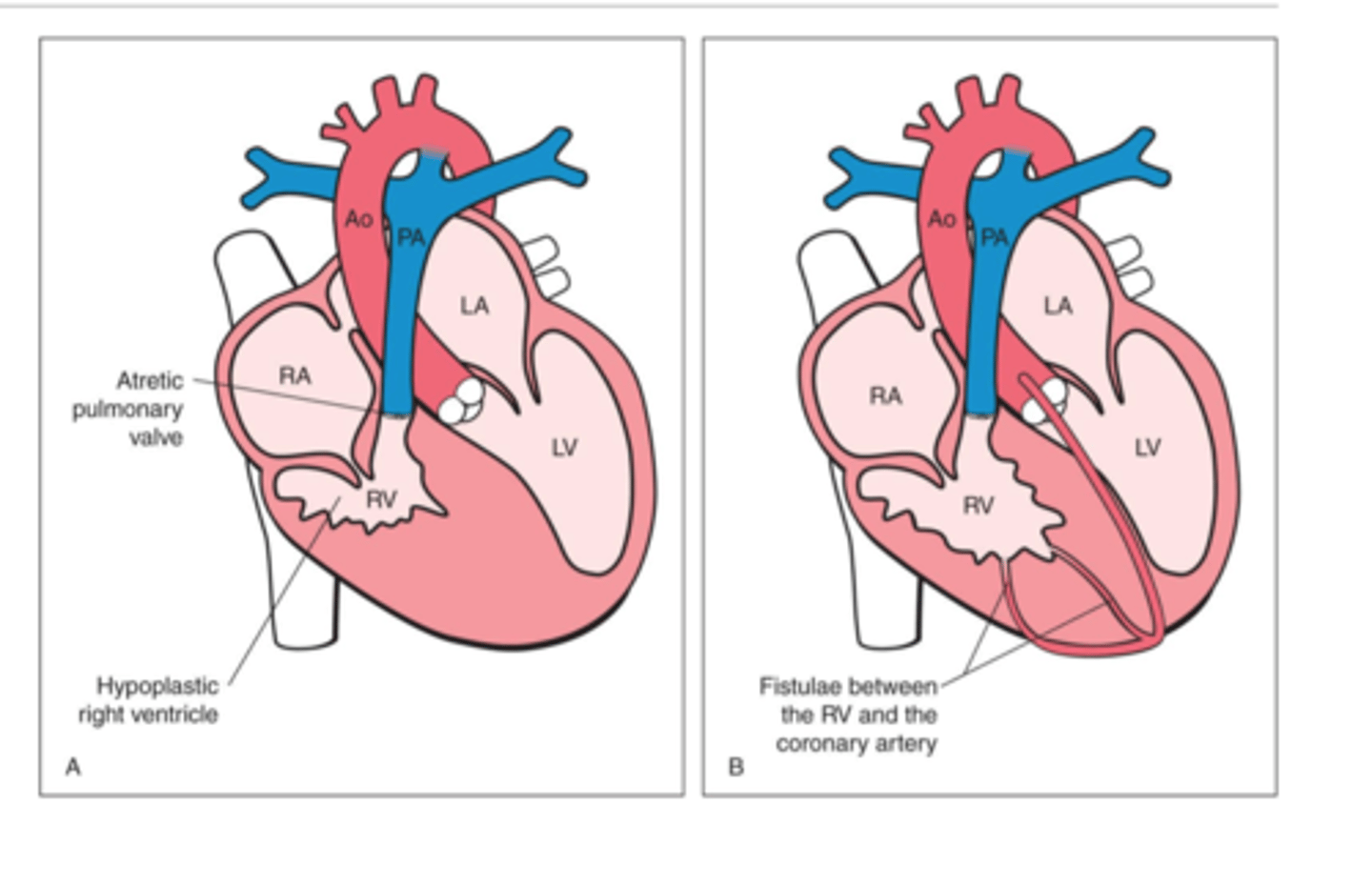
How do you manage coronary flow and overcome the outflow obstruction in patient with atretic/hypoplastic right heart with RV to right coronary sinusoids?
do not close off sinousoids b/c they may be the only blood flow to the coronaries. The proximal portions of the coronaries may be stenotic or atretric.
Only do a systemic to pulmonary shunt and do not do transannular patch.
The coronaries are relying on a high pressure RV to send blood to coronaries and by decompressing it ,the coronaries no longer get sufficient flow.
Truncus Arteriosus Repair based on regurgitation timing and management of valves?
delayed repair results in increased morbidity and mortality.
1-4 common valves (60% tricuspid). If regurgitation of common valve is MORE that moderate (if moderate then just do truncus repair) then do truncus repair in addition to valve repair. Valve repair usually done later if possible.
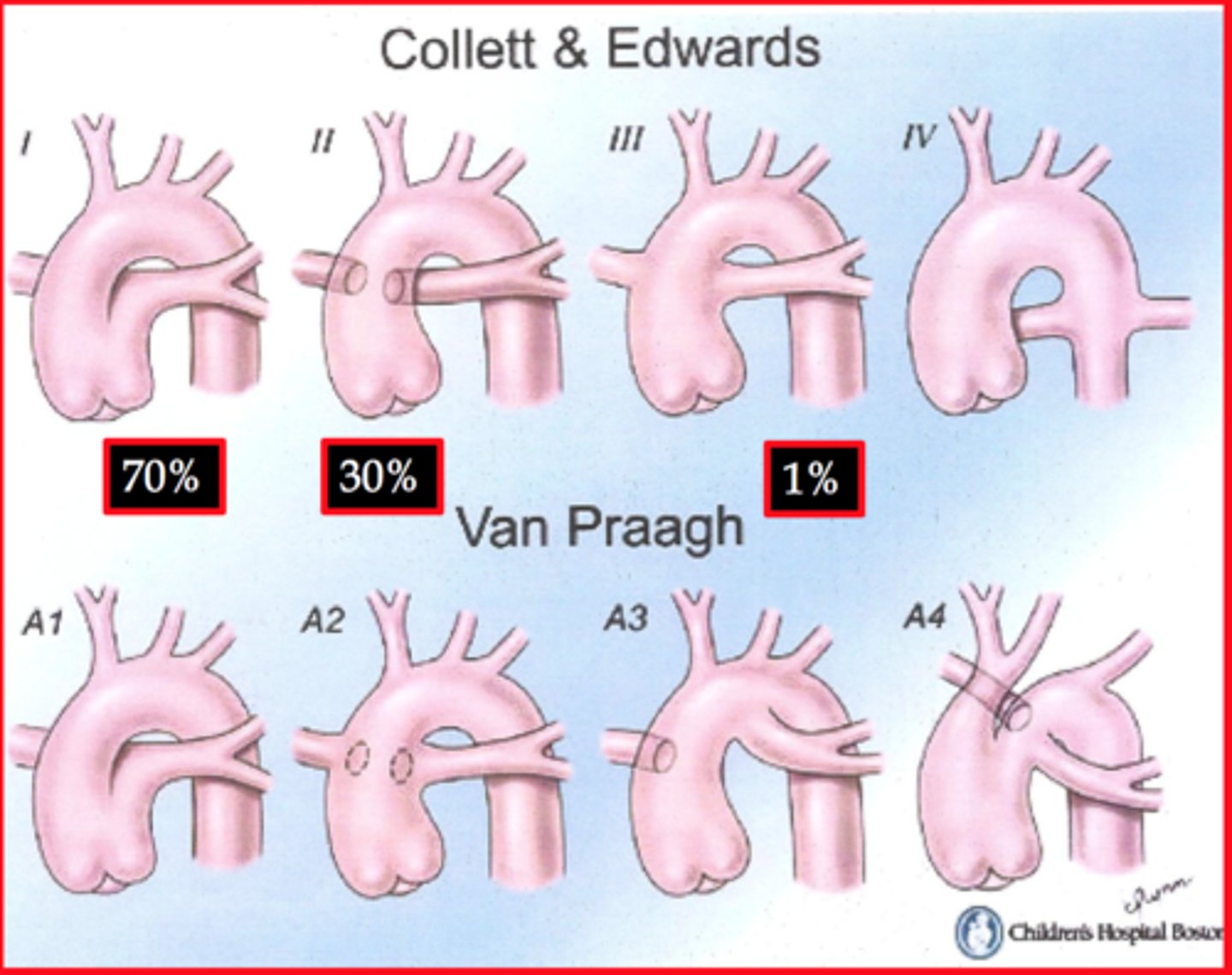
Truncus Arteriosus Types
Type I truncus arteriosus is characterized by the origin of both pulmonary arteries from a short pulmonary trunk.
Type II is characterized by the separate origin of the pulmonary arteries from the posterior aspect of the truncus.
Type III is characterized by the separate origin of the pulmonary arteries from the lateral aspect of the truncus.
Type IV is a pseudotruncus and is considered a form of pulmonary atresia where pulmonary arteries branches are supplied by major aorticopulmonary collaterals arising from the descending thoracic aorta.
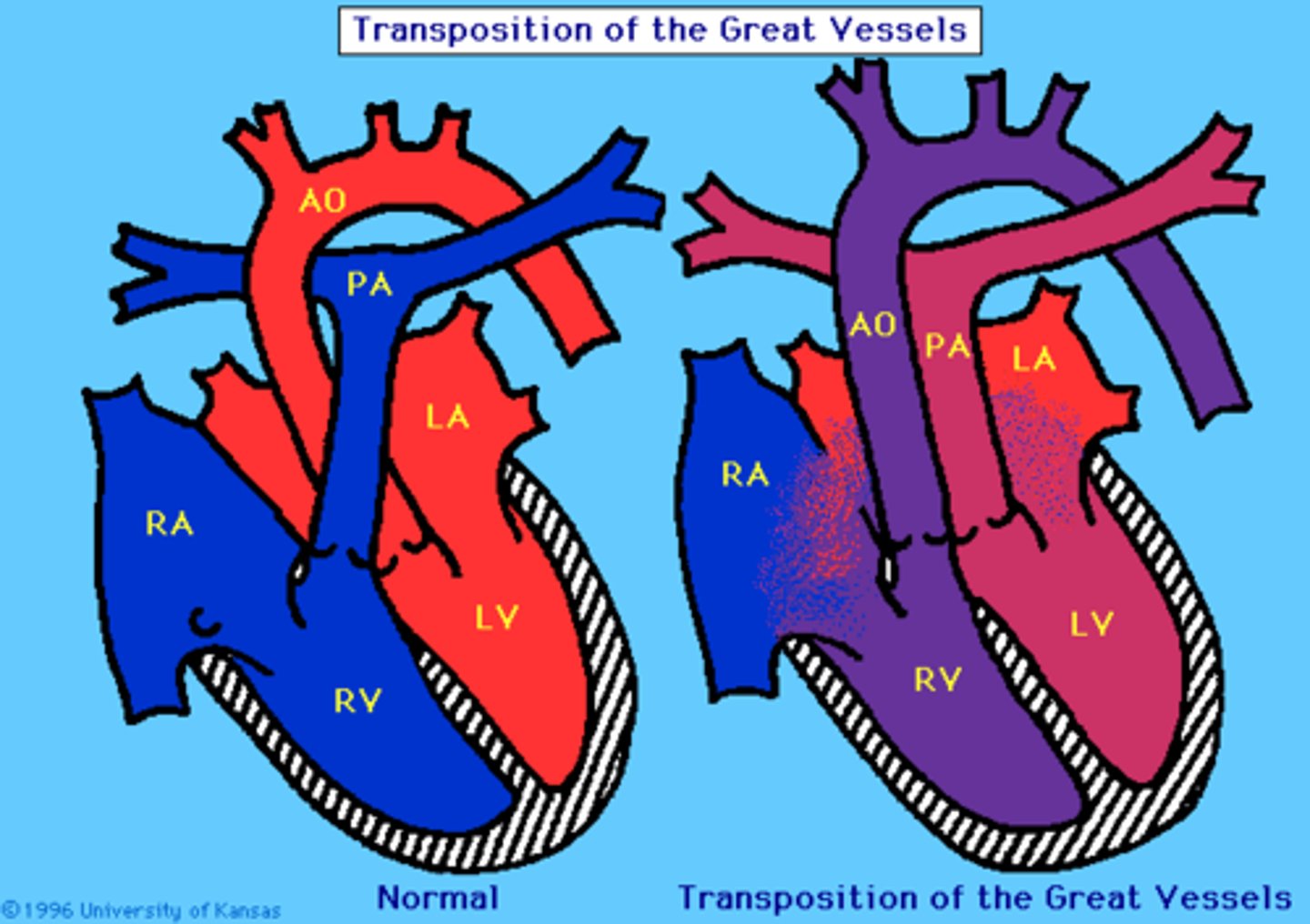
D-transposition of great vessels
aorta leaves RV (anterior) instead of LV (posterior) and pulmonary trunk leaves LV instead of RV, results from failure of aorticopulmonary septum to spiral
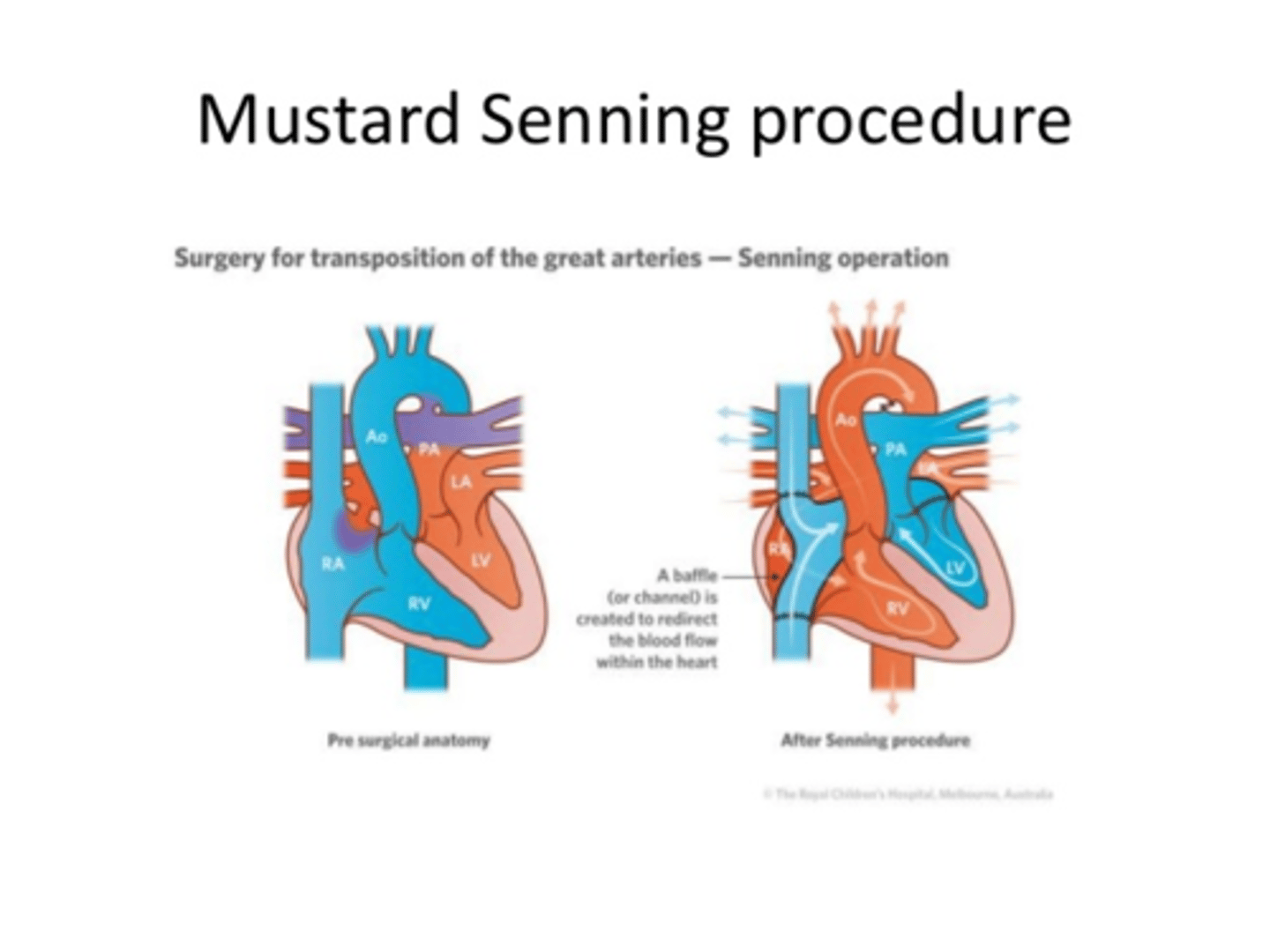
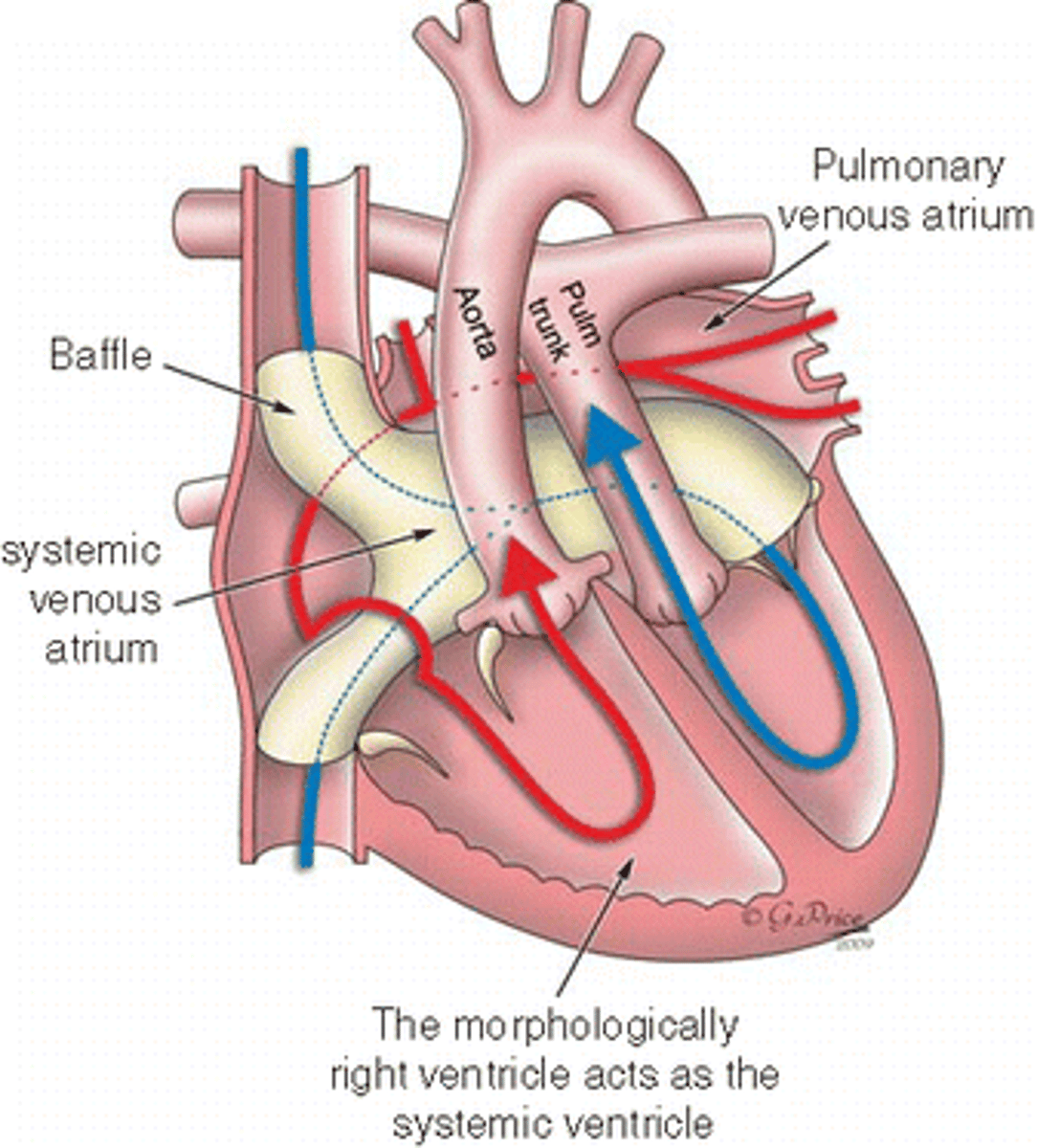
Mustard/Senning Procedure
Atrial Switch operation for D-transposition of the great vessels
creates a two-way baffle in the top part of the heart so blood going to left atrium is carried to the RV and the blood going to the right atrium is going to the LV. This baffle serves as a bridge between the two sides of the heart.
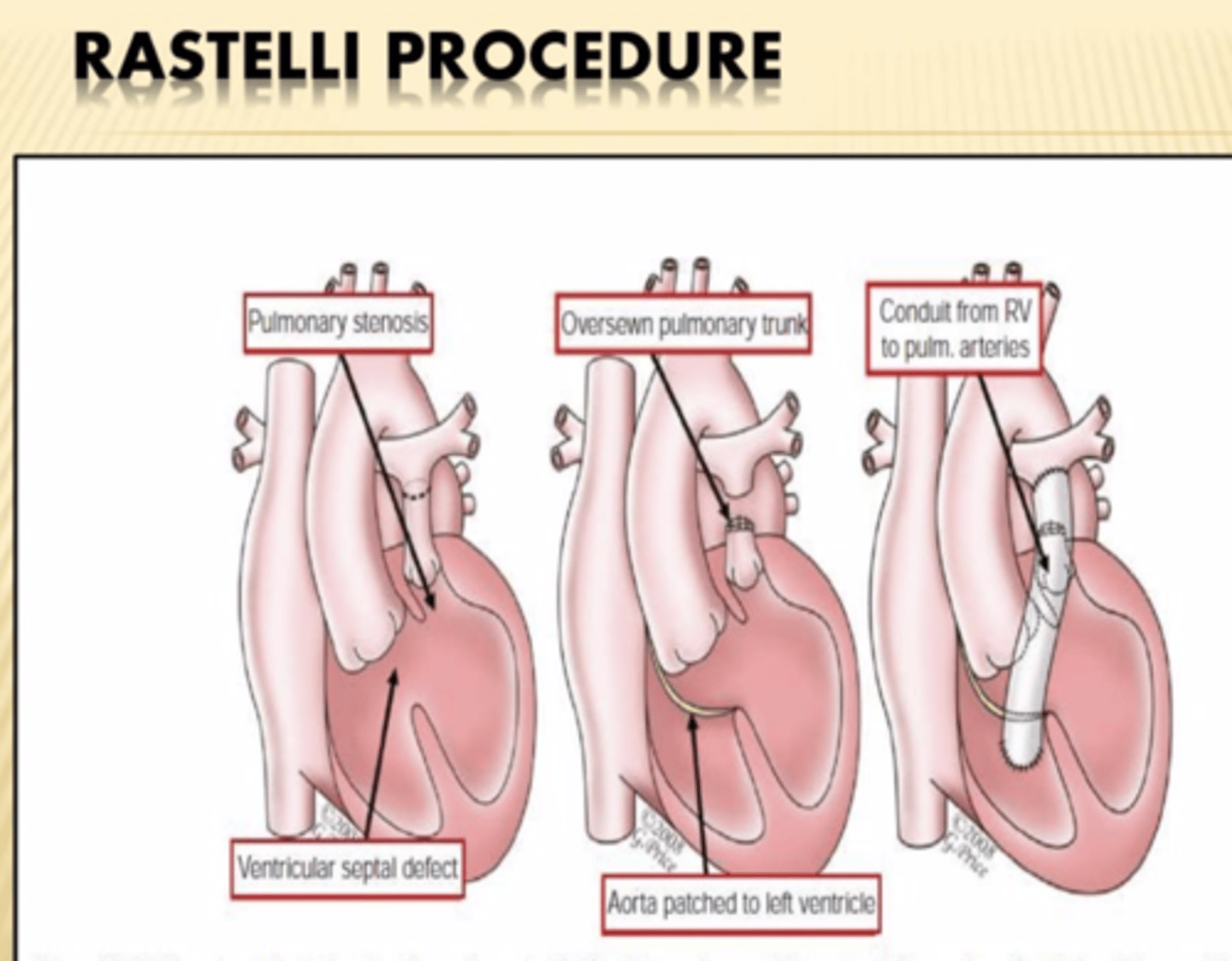
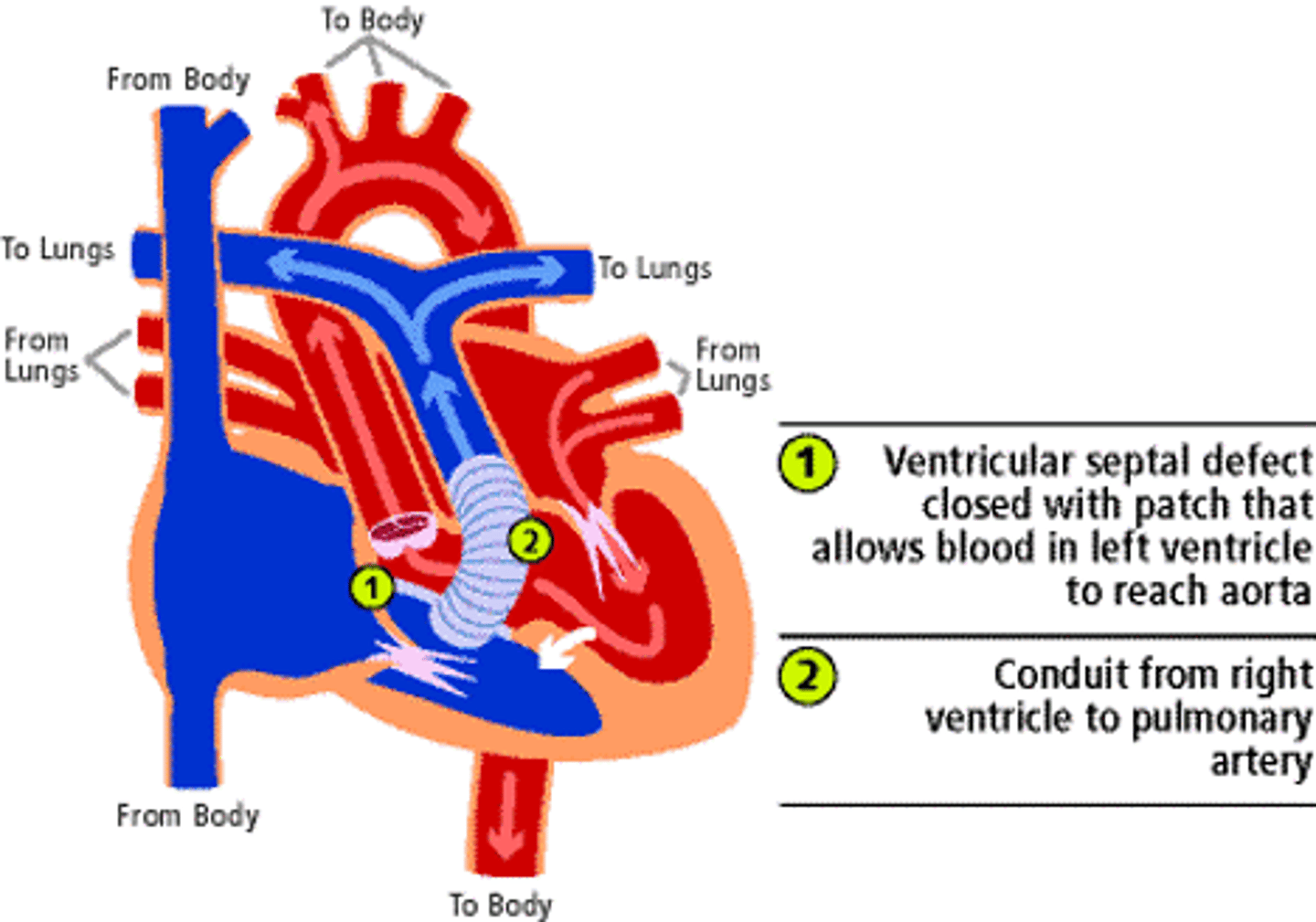
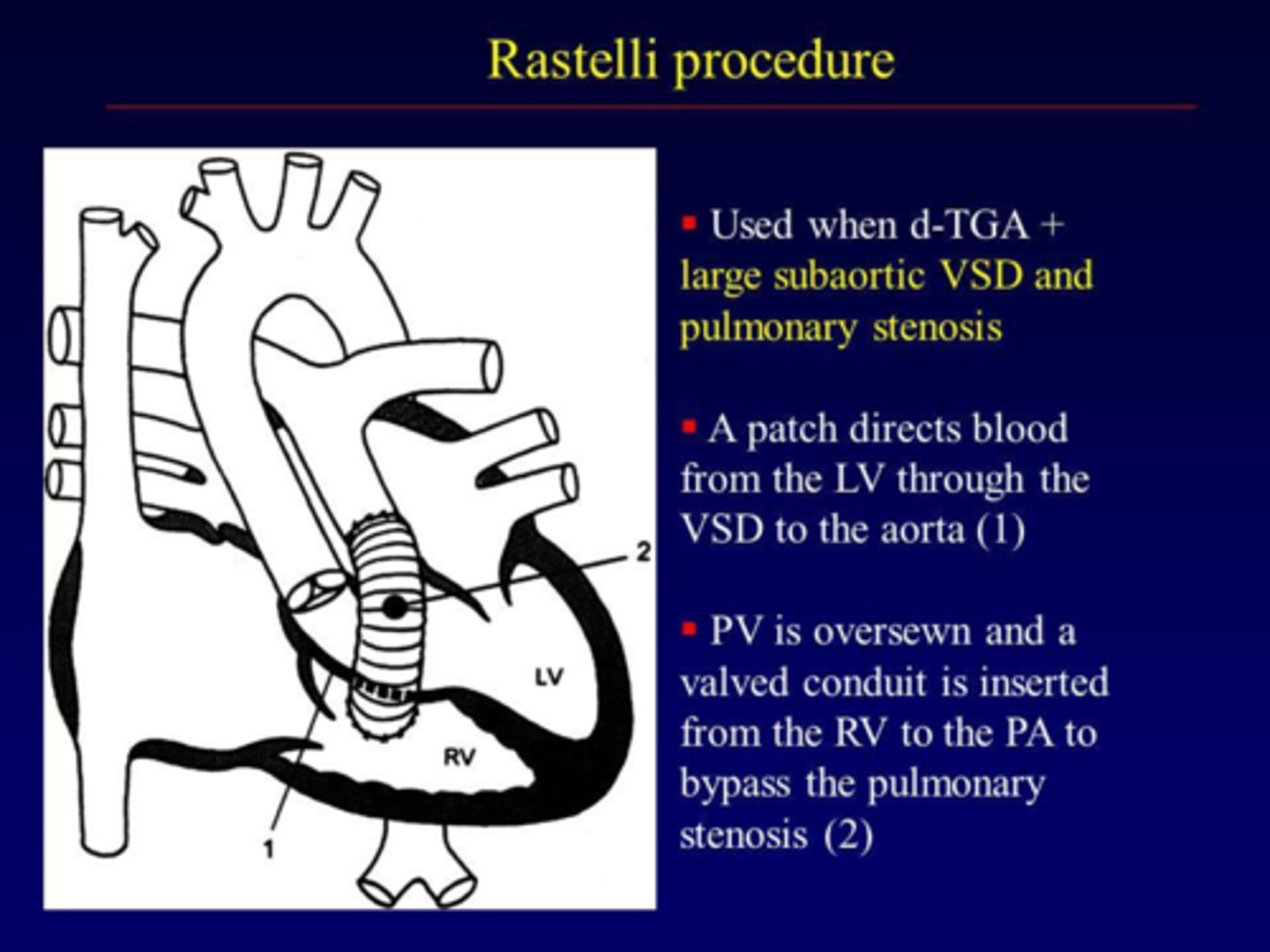
Rastelli Procedure
Correction of transposition of great arteries
Aorta is rerouted internally to LV across VSD and pulmonary artery is attached to RV externally.
RV hypoplasia is contraindication bc conduit from LV to aorta goes through VSD into already small RV.
PA-IVS (pulmonary atresia with intact ventricular septum), what does the child rely on for survival?
Child relies on ASD for survival
Celoria Classification for interrupted arch
Type A: distal to left subclavian artery
Type B: between left subclavian artery and left common carotid (MOST COMMON)
Type C: Between innominate and left common carotid (least common).
*Type B is commonly associated with abberant right subclavian and conoventricular VSD. Reconstruction of the abberant right subclavians not required.
Interrupted aortic arch associated syndrome and cannulation needs?
Digeorge syndrome frequently associated.
Surgical repair requires cannulation of both aortic segments in order to perfuse the upper and lower body.
Congenitally corrected transposition of the great arteries
Congenitally corrected transposition of the great arteries (CCTGA) is a rare heart defect in which the heart's lower half is reversed.
It is also called L-TGA. It is different from and much less common than "regular" transposition of the great arteries (TGA or D-TGA). Tricuspid is on left side of heart and mitral is on right side.
**Commonly will have "systemic" RV dysfunction with tricuspid regurgitation.
Rastelli procedure
Correction of transposition of great arteries
Aorta is rerouted internally to LV across VSD and pulmonary artery is attached to RV externally
Single ventricle reconstruction trial
largest multicenter randomized control trial comparing MBTS vs RVPA shunt.
Found better 1 year survival for RVPA but at 3 years this was no different. Did find that RVPA patients had decreased RV function and higher rate of catheter based interventions.
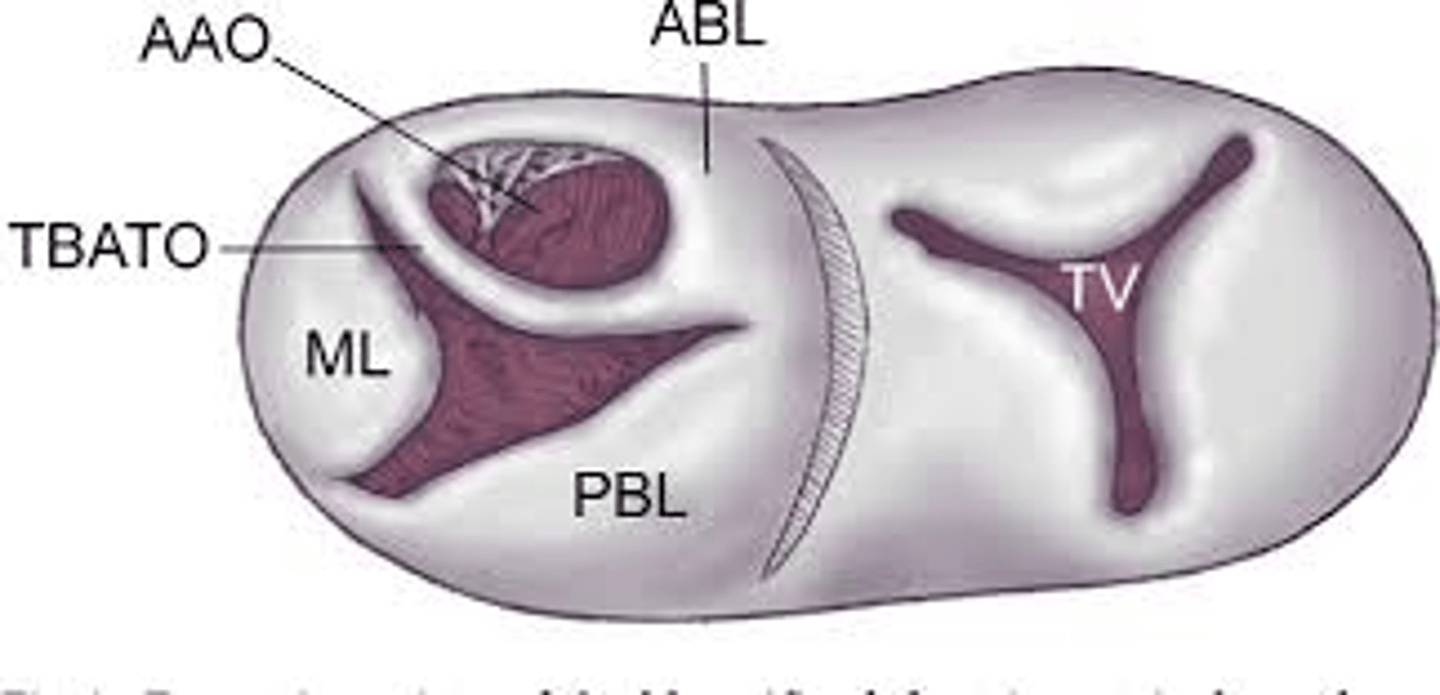
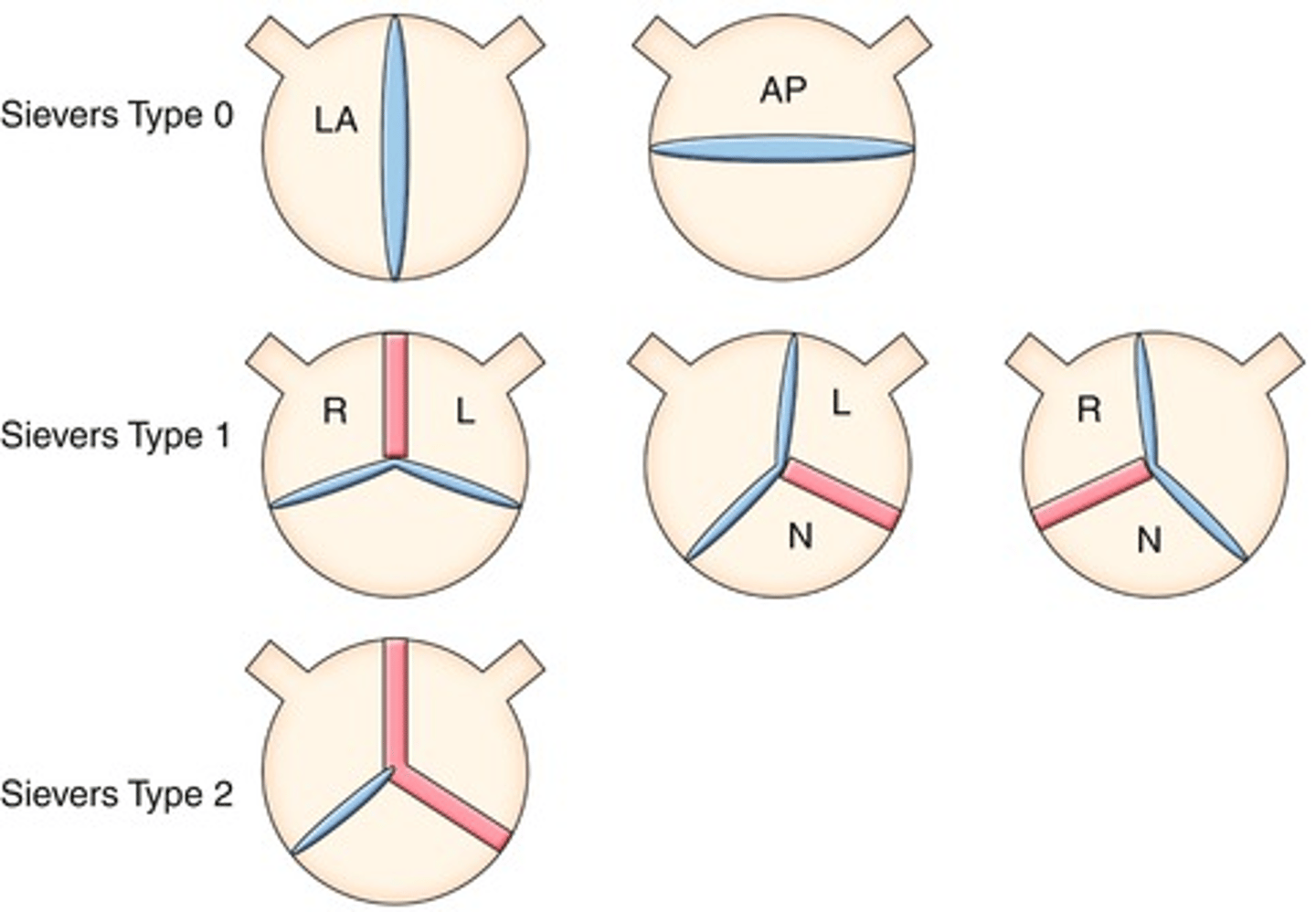
Sievers Bicuspid Valve Classification
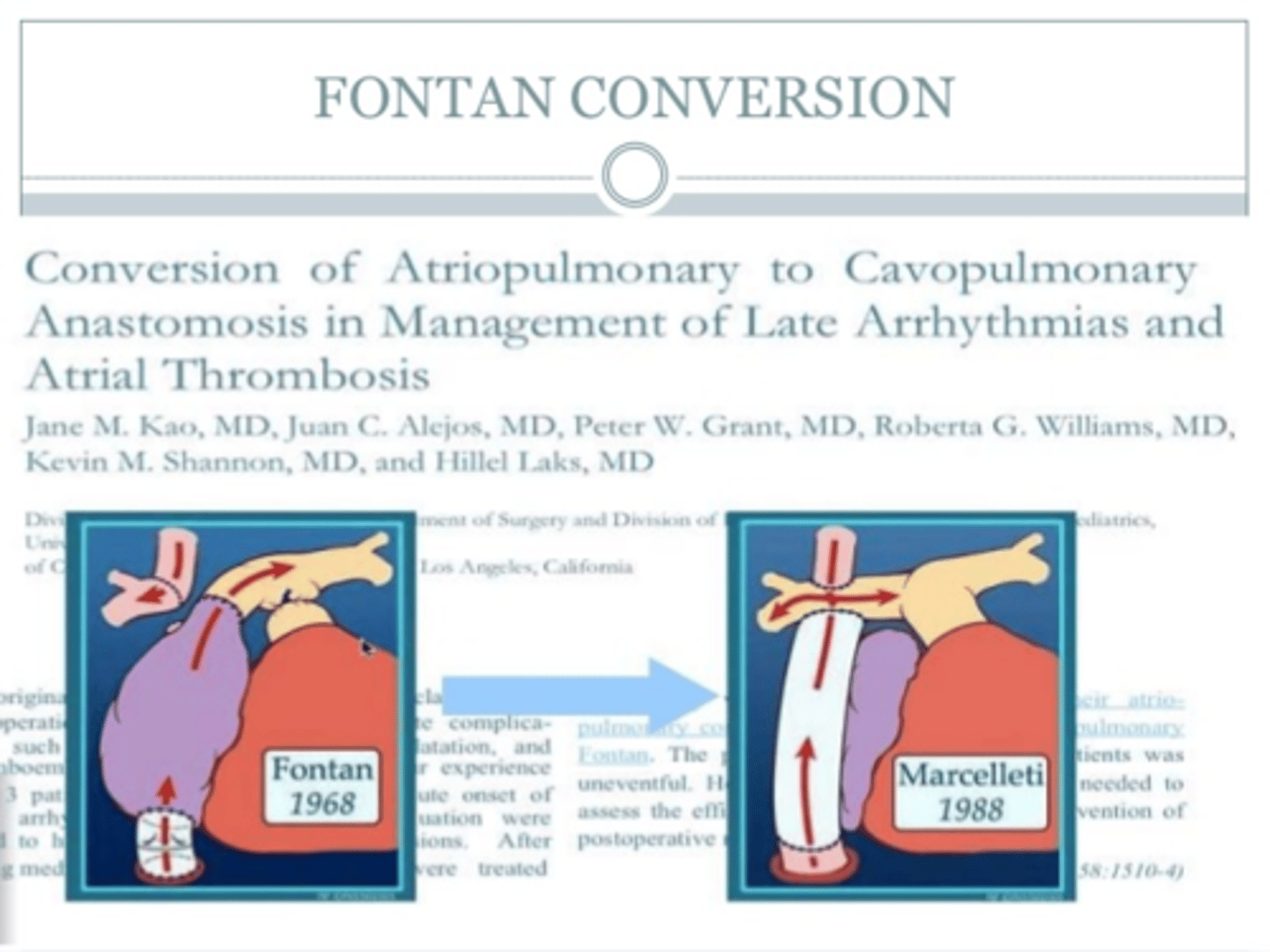
Fontan conversion procedure
People with earlier forms of the Fontan operation are can develop marked dilation of the top (atrial) chamber of the heart, arrhythmias and deterioration of functional status (which are indications for the conversion Fontan)
time frame where DHCP vs SCP doesn't make difference
if less than 40 minutes, no difference between DHCP and SCP (selective cerebral perfusion).
Once >45 min: direct correlation with injury per minute.
cerebral air embolism while on bypass
put in steep trendelenberg position, ventilate 100% oxygen to decrease size of air emboli by nitrogen diffusion out, put in LV/Aortic vent and vent, give retrograde cerebral perfusion through svc while venting. Systemic hypothermia helps as well by decreasing metabolic rate and decreasing the size of air emboli.
low output cardiac syndrome
occurs in up to 25% of neonates after CPB. Result in decreased CO and increase PVR and SVR. Can treat and prevent progression by giving Milrinone.
After lecompte procedure for d transposition of great arteries, most commonly injured structure after redo sternotomy
pulmonary artery bc it is now anterior to the aorta and adheres to sternum.
How to increase coronary perfusion without increasing HR or using aortic balloon pump
vasopressin
Increases SVR resulting in increased coronary perfusion but no B1 activity.
Calculating Qp/Qs
Qp/Qs= SaO2-MVO2/PVO2-PAO2
Systemic O2
Mixed Venous O2
Pulmonary Venous O2
Pulmonary Artery O2
What is Acute cellular rejection after cardiac transplant characterized by?
characterized by lymphocytic infiltrate in perivascular space with up to 1 location of myocardic necrosis .
Patients with superior cavo-pulmonary connection are at risk for what?
AVM's.
These patient's only receive pulmonary flow from upper body which doesn't have "hepatic factor" which leads to increased risk of AVM if do inferior cavopulmonary anastomosis then these resolve spontaneously.
When need to close VSD? What sign on the aortic valve tells you the VSD needs to be closed?
Qp/Qs > 1.5:1
The development of aortic valve regurgitation in a patient with perimembranous VSD means the VSD should be closed (this halts the progression)
How to assess and what is the criteria for pulmonary valve replacement for congenital hearts?.
MRI has proven to be the best tool for serial assessment of RV volumes.
Indications have included clinical symptoms such as decreasing exercise tolerance, arrhythmias, progressive right ventricular (RV) dilation (with resulting decrease in function), and onset of tricuspid regurgitation.
RVEDI of >150 ml/m2
RV systolic pressure >2/3 systemic
Pulmonary valve atresia repair with closure of VSD: when to fenestrate vs not.
After the VSD is closed and a conduit is placed, pressures in the PA, RV, and LV should be directly measured. If the ratio of the RV to the LV systolic pressures exceeds 0.85, the likelihood of a successful biventricular repair is low, and the VSD patch should be fenestrated.
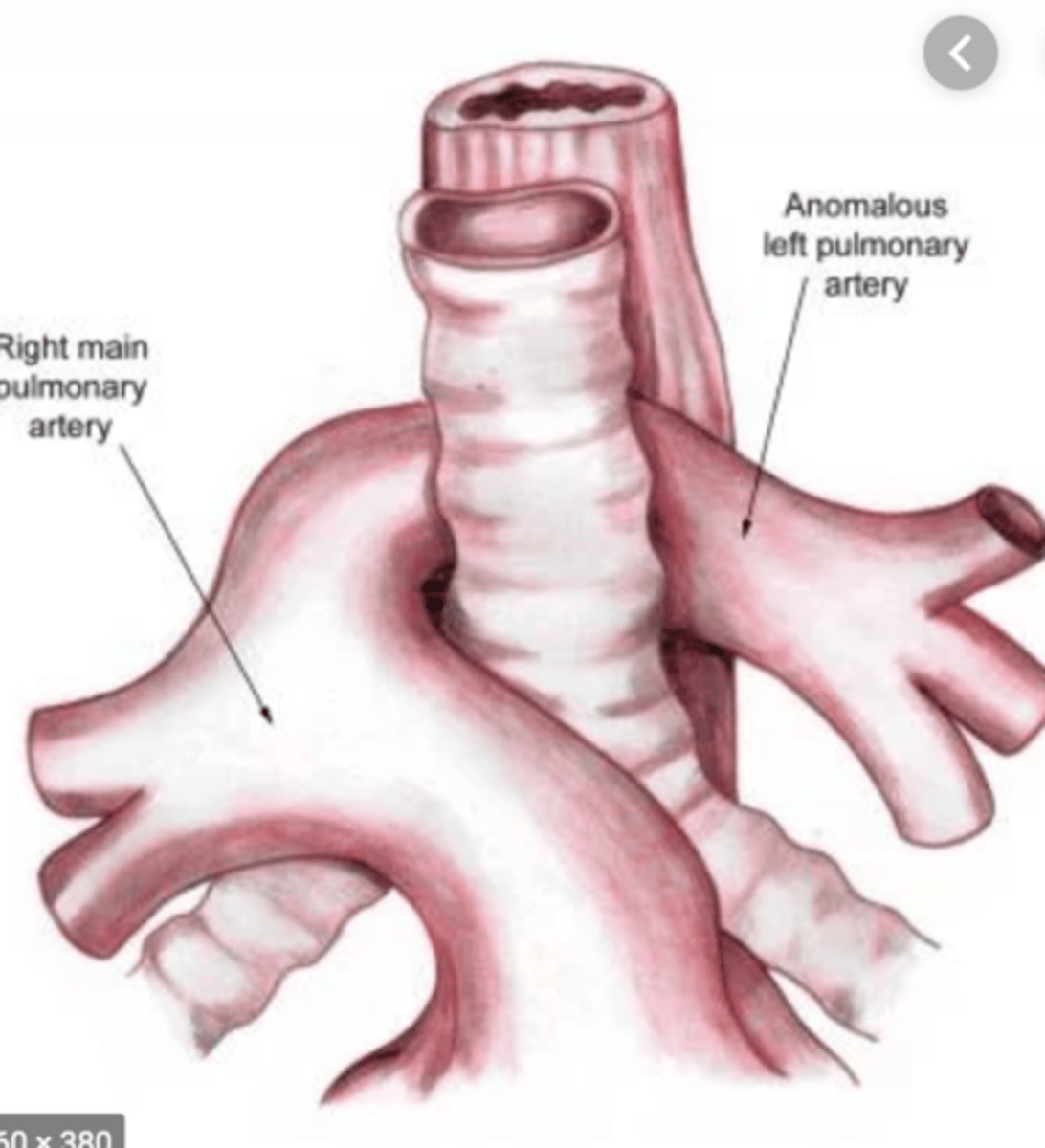
Left PA sling associated anatomic defect
Upwards of 80% of infants with a left PA sling will have associated anatomic tracheal stenosis characterized by complete circular cartilaginous rings (absence of the membranous trachea).
supravalvular mitral ring treatment and associated with what?
fibromuscular tissue leading to congenital mitral stenosis. Balloon valvuloplasty not sufficient for this like adults bc this is tissue above the valve, not the valve itself. Surgery is the answer with resection of this tissue. 90 % at 10 years do not have recurrence.
can be associated with shone's complex (multiple left sided lesions: coarctation, MV supravalvular ring, sub aortic stenosis)
Surgical indication to fix left to right shunting is when QP/QS is what?
>1.5 :1
Standard CVP for post operative Fontan patient
12-16 mm Hg.
Neonatal coarctation thoracotomy vs sternotomy approach
sternotomy when Z= -4.59 or more negative
otherwise, thoracotomy.
these z scores are of the proximal transverse arch and are cutoffs to reduce recurrence/reintervention need for these patients when followed.
calculating FENa
FENa: (urine sodium x plasma creatinine)/ (plasma sodium x urine creatinine)
<1 = prerenal
>3 = more likely intrinsic (can be post renal too)
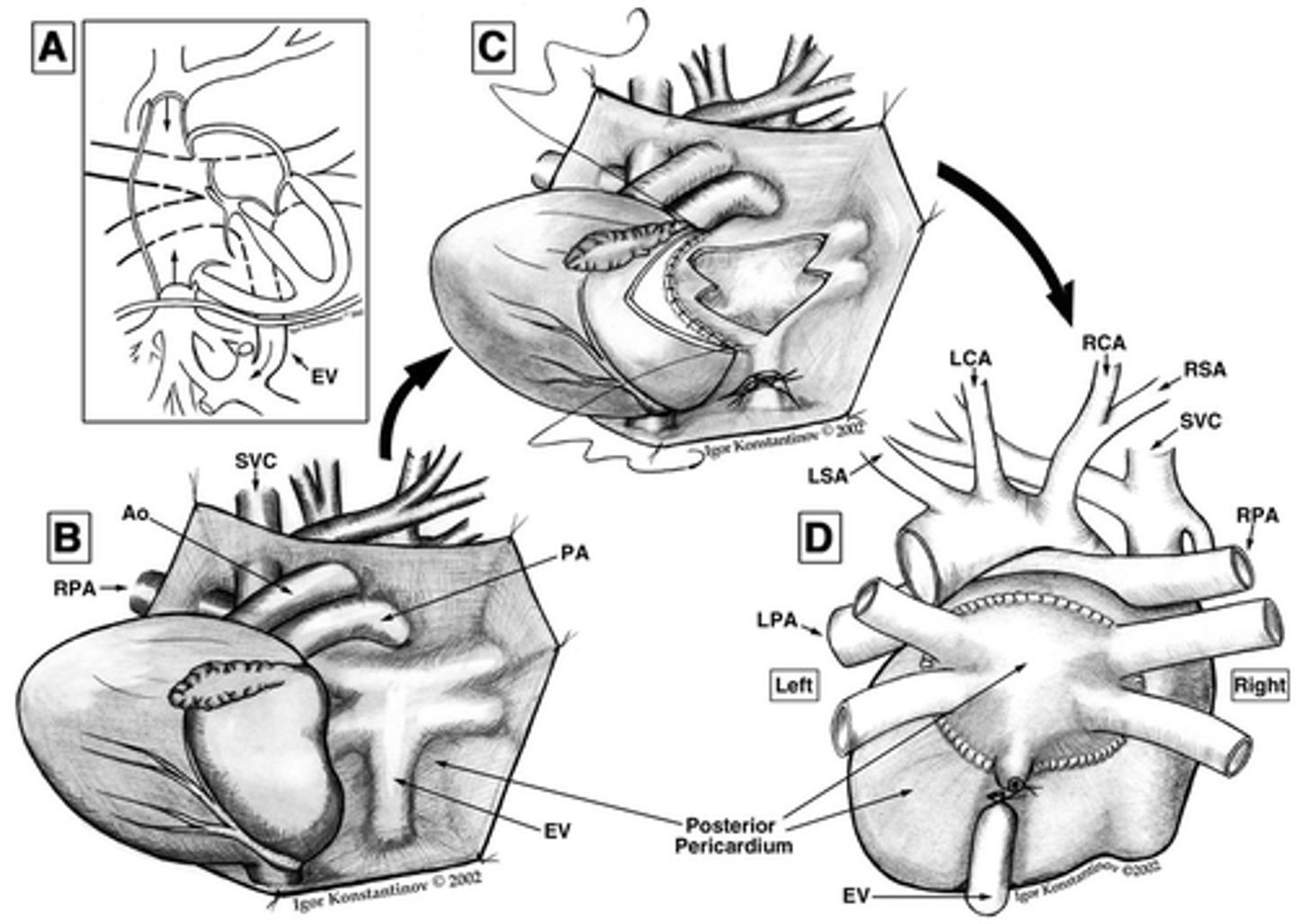
Sinus venous ASD due to pulmonary veins draining into SVC at right atrial/SVC junction treatment
Warden procedure if >2 cm from the SVC/RA junction or above the azygous junction: cut SVC cephalic and taking inferior portion and suturing to pulmonary veins and superior portion and suturing directly to right atrial appendage.
Otherwise, baffle directing flow from pulmonary veins into left atrium while directing flow from SVC into right atrium. If done with a two patch repair: one patch directing flow and other patch keeping SVC from getting stenosed. This second patch has risk for SA node interruption when suturing.
Taussig-Bing Malformation what is it and how to treat
more complicated version of DORV bc has subpulmonic VSD.
Pulmonary valve is overriding the VSD and the aorta is coming from the RV.
Treatment is switch procedure with closure of VSD.
Associations with anterior malalignment VSD vs posterior malalignment VSD.
anterior: RV outflow track obstruction, underdevelopment of RV and TV, aortic arch hypoplasia, coarct or interrupted arch.
posterior: projection of the conal septum into the LVOT. May be associated with PV stenosis, PV hypoplasia or bicuspid PV.
Ultrafiltration rate depends most on what?
Transmembrane pressure (TMP): (inlet pressure-outlet pressure)/2 - vacuum pressure.
blood flow rate, membrane pore size and length are important but not largest contributing factor.
*for hemodialysis, electrolyte concentration is rate determining factor.
Centrifugal pump vs roller pump response to downstream occlusion
centrifugal do not create high negative pressures so do not cause micro emboli and cavitation. This is unlike roller pumps which are not used as commonly anymore.

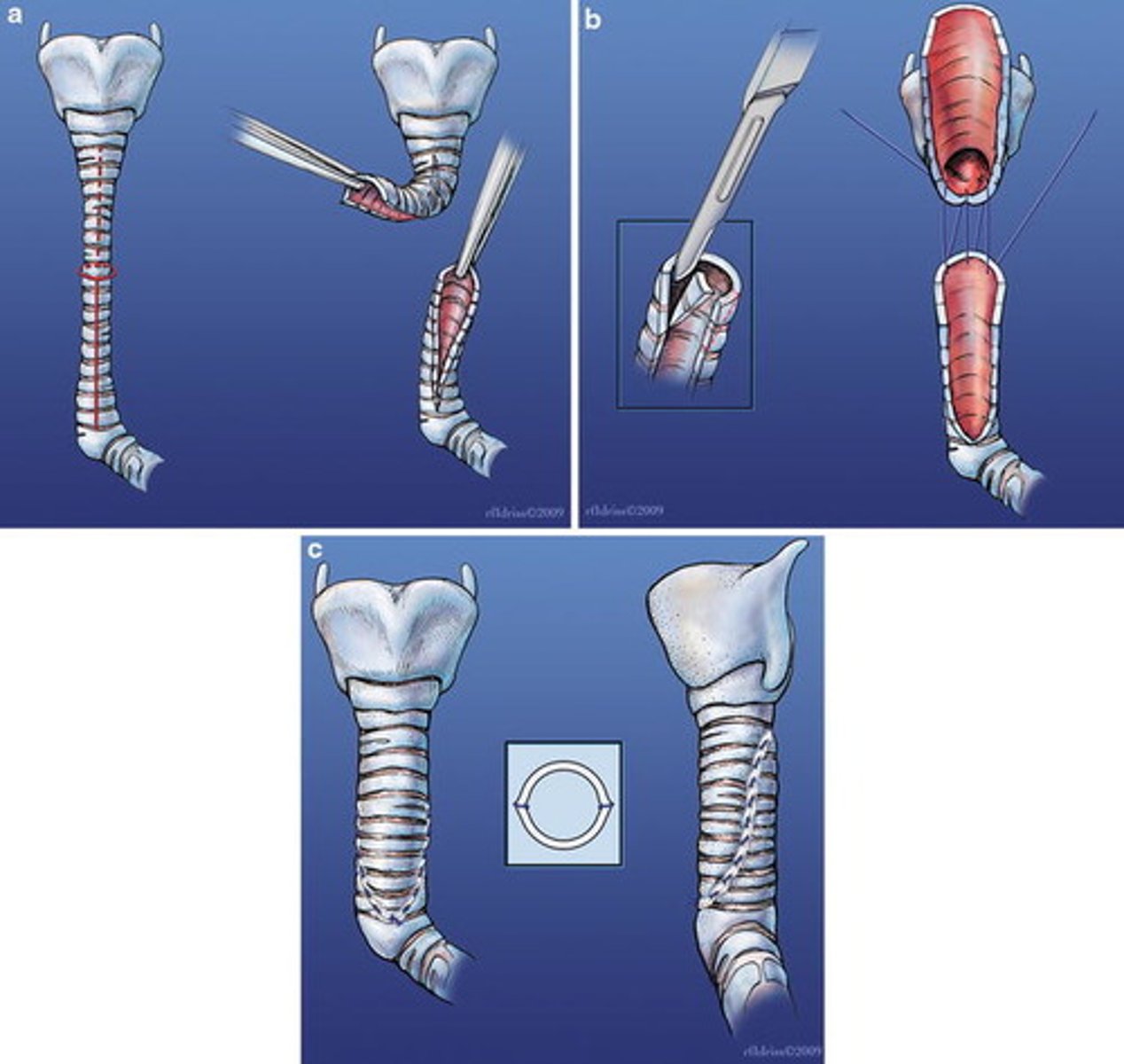
When to do a slide tracheoplasty?
for longer segment stenosis. smaller segments can just do resection and primary anastomosis.
When to do complete vs ventricular pericardiectomy
complete when have retained fluid and continued inflammation even after optimal therapy.
ventricular for constriction only with no retained fluid or inflammation
How to fix an apical muscular vsd closure in infant
enter RV next to LAD in vertical incision. primary challenge is avoiding network of trabeculations which can cover the true defect.
If need more exposure for VSD closure when going through TV then can...
perform tricuspid valve incision
First step when have baby with D-transposition of great vessels (if not crumping and needing echo)
percutaneous balloon atrial septostomy for blood mixing so can do operation under more elective time frame.
Damus-Kaye-Stansel procedure
aortopulmonary amalgamation (unification)
Rastelli procedure (correction of transposition)
Correction of transposition of great arteries
Aorta is rerouted internally to LV across VSD and pulmonary artery is attached to RV externally
Nikaidoh procedure (correction of transposition)
when vsd is shallow and unfavorably located then removal of stenotic LVOT and translocation of the aortic root to the LVOT helps long term results.
Senning procedure (correction of transposition)
SVC and IVC baffled into LV which is acting as the RV and pumping to the pulmonary system while pulmonary veins are emptying into the RV and out into the aorta.
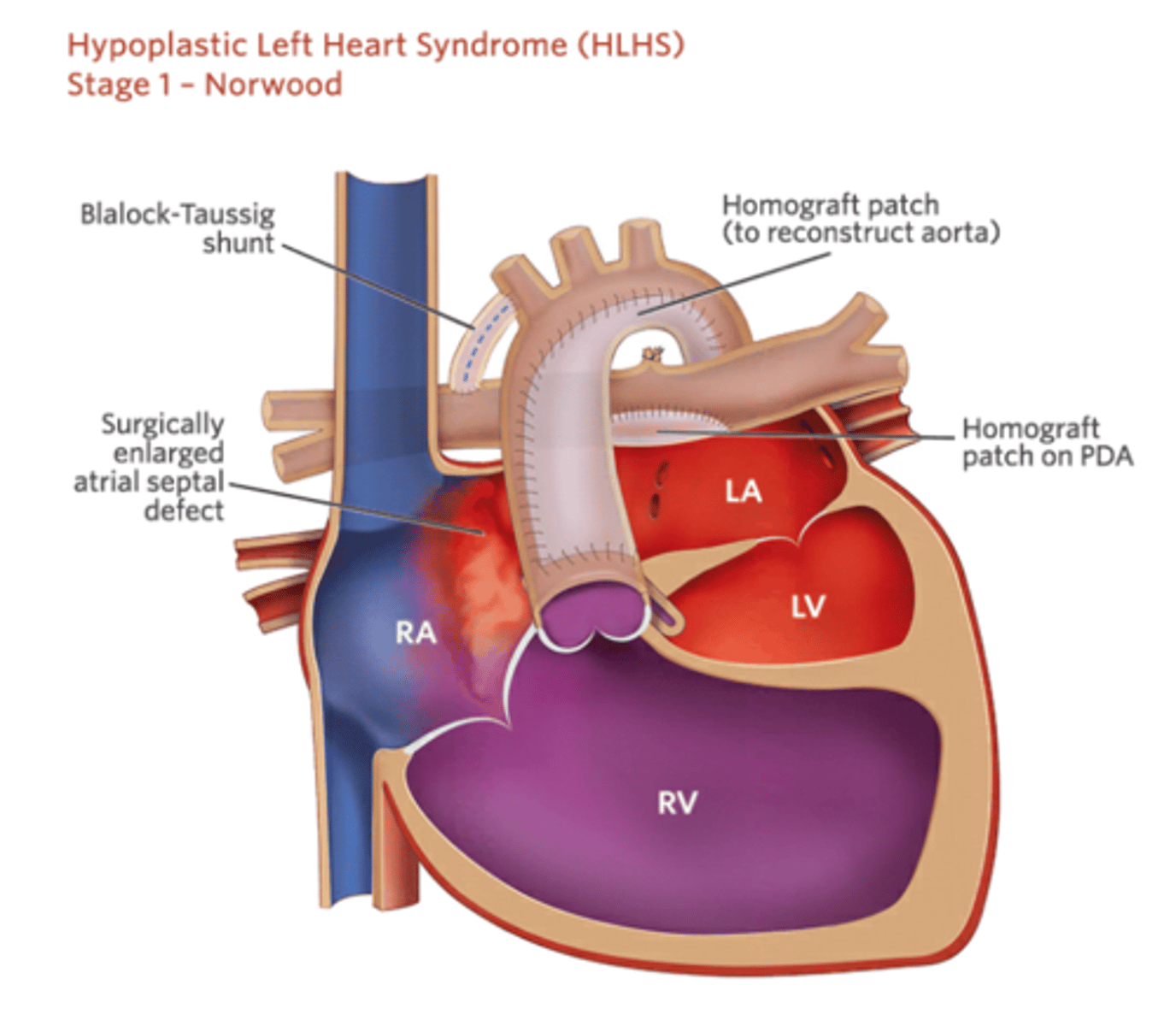
Sano vs MBTS for stage 1 outcomes
Sano had lower mortality right after but higher need for interventions and complications particularly increased need for pulmonary artery reinterventions.
Sano had higher transplant free survival at 1 year vs MBTS (74% vs 64%).
interstage mortality after doing one or the other was the same.
hazards of death or transplant or catheter interventions was the same at 6 years between the two.
Qp/Qs equation
Qp/Qs: (arterial SpO2- mixed venous SpO2)/(pulmonary venous SpO2- pulmonary artery SpO2).
assume Pulm vein and aorta are same or 100%
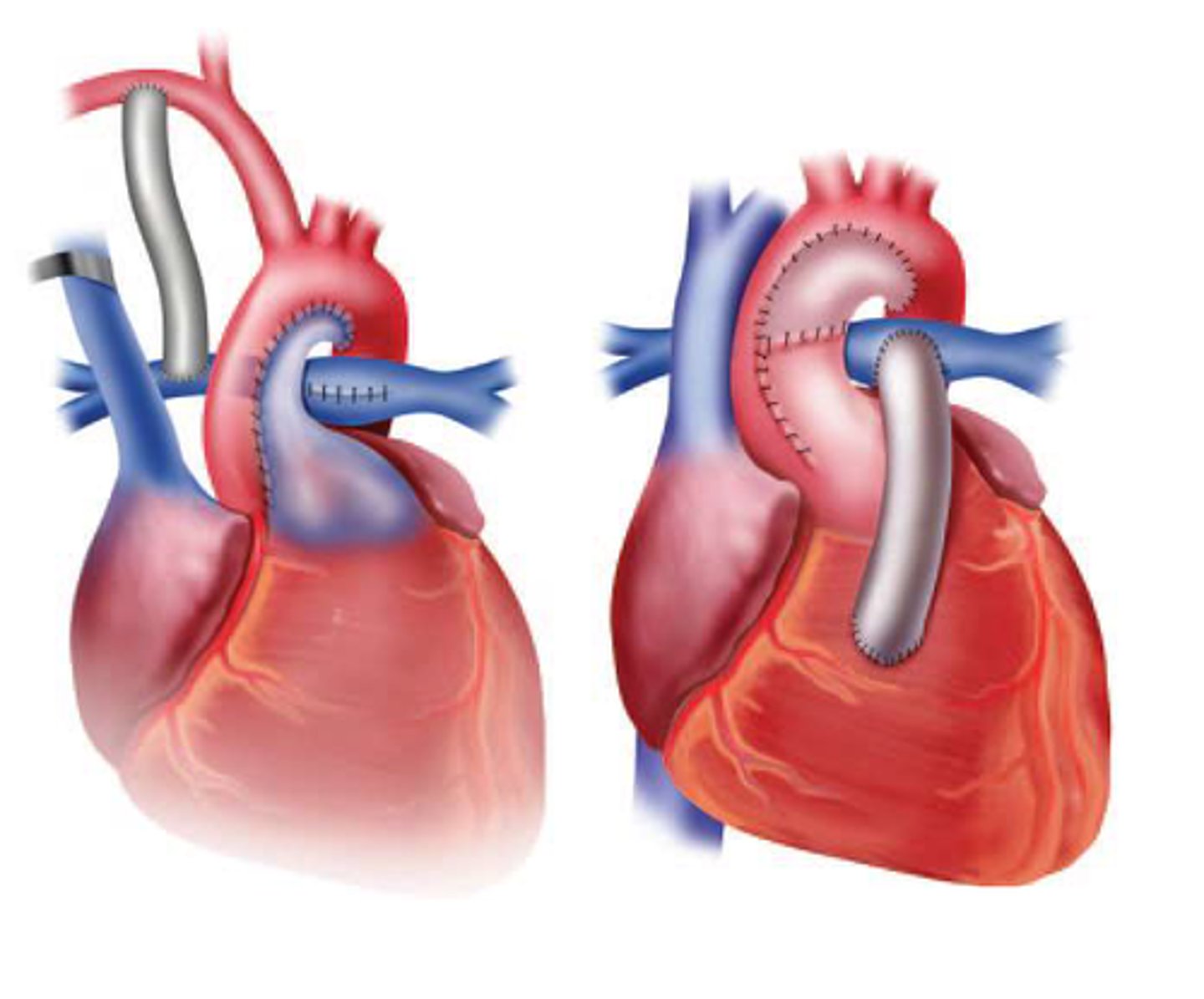
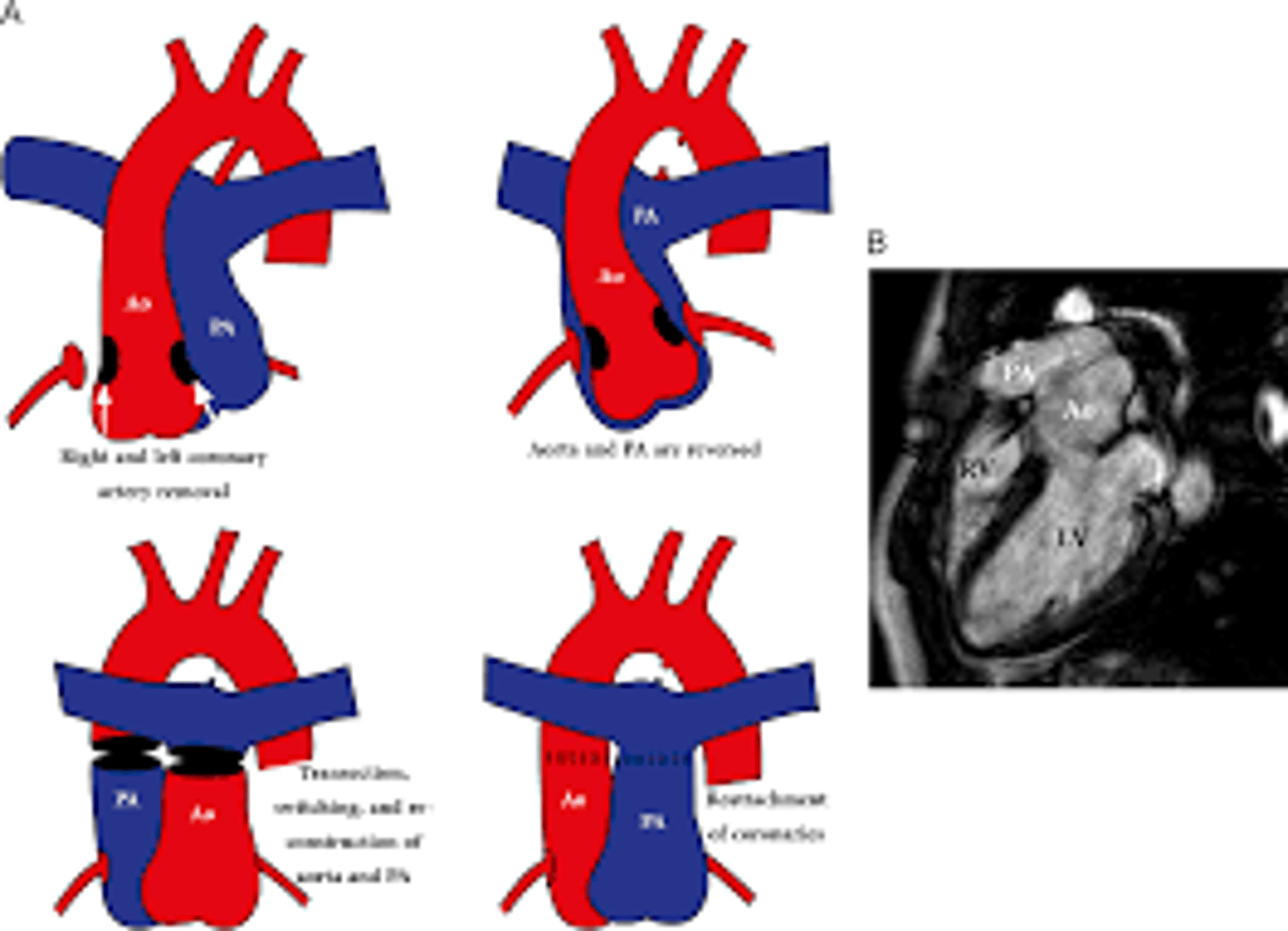
Lecompte maneuver
cutting the main pulmonary artery and moving it anterior to the aorta before reattaching the pulmonary artery during the following reconstruction of the great vessels.
Common arterial trunk associated anomaly
anomalies of coronary arteries origin
What can worsen risk of paraplegia during coarctation repair?
Intraoperative hyperthermia has been shown to result in paraplegia even in patients with relatively short cross-clamp times.
If a patient's core temperature cannot be normalized before cross-clamp application, the operation should be canceled and the origin of the fever elucidated.
At what point is pulmonary hypertension considered fixed?
A pulmonary vascular resistance of more than 10 Wood units that is unresponsive to pulmonary vasodilators indicates that the PVR is fixed.
What other physiologic issues are associated with Schimitars Syndrome?
many times ASD involved (70-80%) and aortopulmonary circulation (30-70%)
* if symptoms from aortopulmonary overcirculation (hemoptosis or pHTN), advised to close off shunt through catheter approached coil occlusion of aorta to pulmonary sytem.
There is hypoplasia of the native right pulmonary artery. Systemic collateral arteries traverse the diaphragm or run in the inferior pulmonary ligament to perfuse part (often most) of the lung.
How do you treat schimitars syndrome and when?
can reimplant pulm veins to LA or create a intra-atrial baffle through ASD but both can lead to obstruction at reimplantation or through ASD.
When possible try and delay operation to after infancy.
How often do you see acute cellular rejection after cardiac transplant?
Occurs in 20-40% of transplants.
How is acute cellular rejection after cardiac transplant treated?
Most occurrences are self limited. Advanced grades treated with pulse dose steroids and non respondent grades get thymoglobulin (hemodynamic compromise or treatment failure)
When do you repeat biopsy after findings of acute cellular rejection after heart transplant?
Repeat biopsy at 2-4 weeks.