Complex infections and sepsis
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
What is a complex infection?
Multi Resistant Infection (ESBL UTI, MRSA bacteraemia, TB)
Difficult to treat infections (eg. Endocarditis)
Deep seated infections (eg. bone infection)
Infections in a patient with underlying co-morbidities (eg. Resistant pseudomonas in a patient with cystic fibrosis)
Infection in more than one site
Ongoing infection with unknown origin source
Infection leading to a significant morbidity / mortality
Infection leading to sepsis
What is the pharmacist role in dealing with complex infections?
Procuring unusual antibiotics/antifungals/antivirals
Dosing advice to optimise treatment
Renal impairment – What if on dialysis?
Patient weight – Obesity
Type of infection – Pseudomonas
Critically unwell patient and altered drug handling – Low albumin
Route of treatment – What if no oral access?
Managing interactions (e.g. Voriconazole (inhibitor), Rifampicin (inducer) & DOACs)
Therapeutic Drug Monitoring and interpretation of levels – Taken at the correct times? When should we take levels?
Managing Outpatient Parenteral Antibiotics (OPAT/ NHS@HOME)→ IVs given at home
Managing Complex Oral outpatient Antibiotics (COPAT/ NHS@HOME)→ Long-duration orals with high risk profile e.g. Co-Trimoxazole
Patient counselling → TB regimes, Fluoroquinolones, Linezolid and Tyramine interactions etc.
Ask as a link with microbiologists
Providing / Monitoring adjunct treatments → e.g. steroids in meningitis, IV immunoglobulins in necrotising fasciitis
What medications do the following drugs have interactions with
Rifampicin
Voriconazole
Rifampicin = enzyme inducer. Common interaction with Apixaban – decreases exposure
Voriconazole = enzyme inhibitor. Common interaction with Atorvastatin – increases level/effect
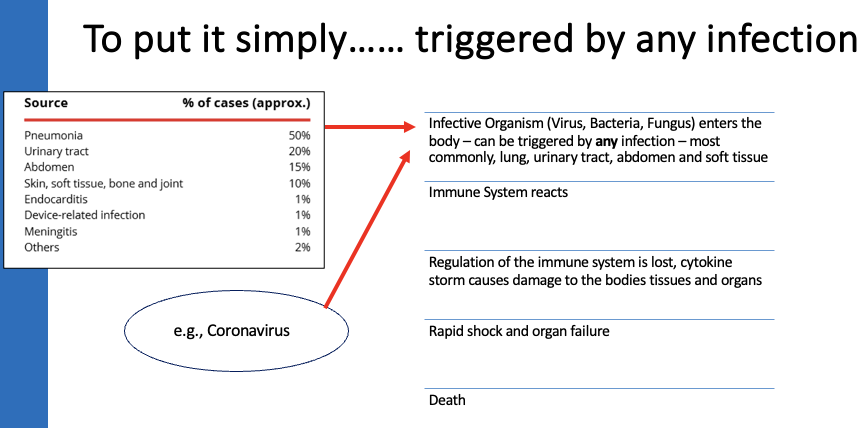
What is Sepsis?
Life-threatening organ dysfunction caused by a dysregulated host response to infection
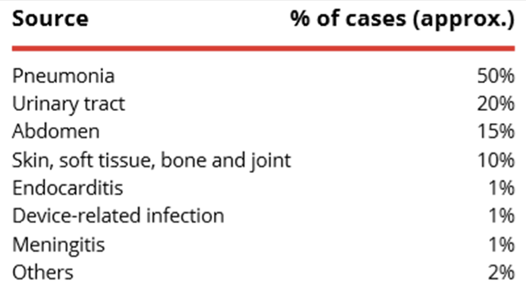
→ Can be triggered by any infection, but most commonly occurs following infection of lungs, urinary tract, abdomen, soft tissue.
What organs can sepsis affect?
ALL
Brain → confusion/ drowsiness/ coma
Kidneys → reduced urine / AKI
Lungs → hypoxia / respiratory failure
Heart → reduced cardiac output
Liver → metabolic dysfunction/ coagulopathy
What groups are high risk for sepsis?
Extremes of age: <1yr, >75yr or frail
Impaired immune systems (chemotherapy, diabetes, splenectomy, sickle cell, long term steroids (including long acting injections), immunosuppressants)
Surgery or invasive procedure in the last six weeks
Any breech in the skin integrity (cuts, burns)
Recent long courses of antimicrobials
IV drug use
Indwelling lines or catheters
Pregnant women, post-natal/termination/miscarriage in the past 6 weeks
→ Remember drug history à Long-acting steroid injections are immunosuppressant, as is recent MAb use for treatment of COVID-19 or multi-morbidity such as MS.
What are the six most common signs of sepsis?
Slurred speech or confusion
Extreme shivering or muscle pain
Passing no urine (in a day)
Severe breathlessness
"I feel like I might die"
Skin mottled or discoloured
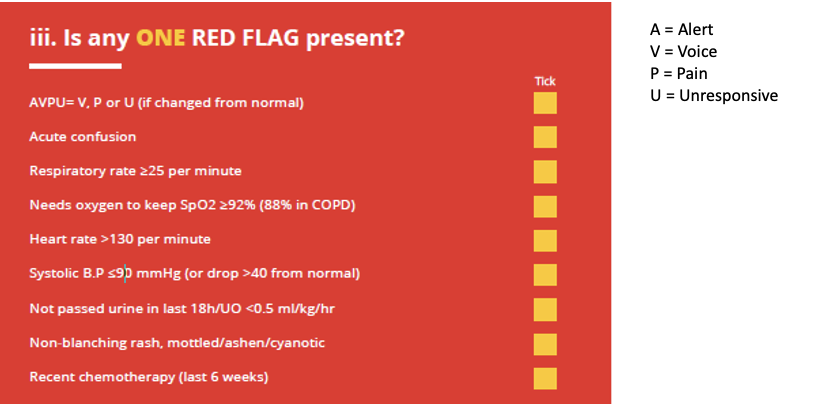
What red flags might indicate sepsis?
AVPU = Alert, Voice, Pain, Unresponsive
Alert: Patient is fully awake (though not necessarily orientated), will have spontaneously open eyes, and will respond to voice (thought may be confused). They will have bodily motor function.
Voice: The patient makes some sort of response when you talk to them. This could be through the eyes, which open when you speak to them, or by voice which may only be as little as a grunt. Or, it could be by moving a limb when prompted to do so by the rescuer.
Pain: A patient may respond by using any of the three components when pain stimulus is used on them (Eyes, Voice, Movement). Recognised methods for causing pain are pinching the ear or pressing into the bed of a fingernail. A fully conscious patient will locate the pain and push it away, whereas a patient who is not alert and not responded to voice may only manifest involuntary flexion or extension of a limb. Performing pain stimulus should be used with caution as in extreme circumstances this could be considered assault.
Unresponsive: This outcome is noted if the patient does not give any Eye, Voice or Motor response to voice or pain.
Although inflammation is an essential host response, excessive levels of pro-inflammatory cytokines can lead to…
systemic endothelial damage, and high levels of anti-inflammatory mediators can result in immune suppression.
Outline pathogenesis of sepsis.
Stimulation of the host immune response by toxins causes an inflammatory response that can lead to endothelial damage.
Pro-inflammatory cytokines, such as tumour necrosis factor (TNF), interleukin-1 (IL-1) and IL-6, are released in response to infection with the aim of destroying damaged tissue and promoting wound repair. Normally, anti-inflammatory mediators (e.g. IL-10, IL-13) are subsequently released to regulate the inflammatory response and restore homeostasis.
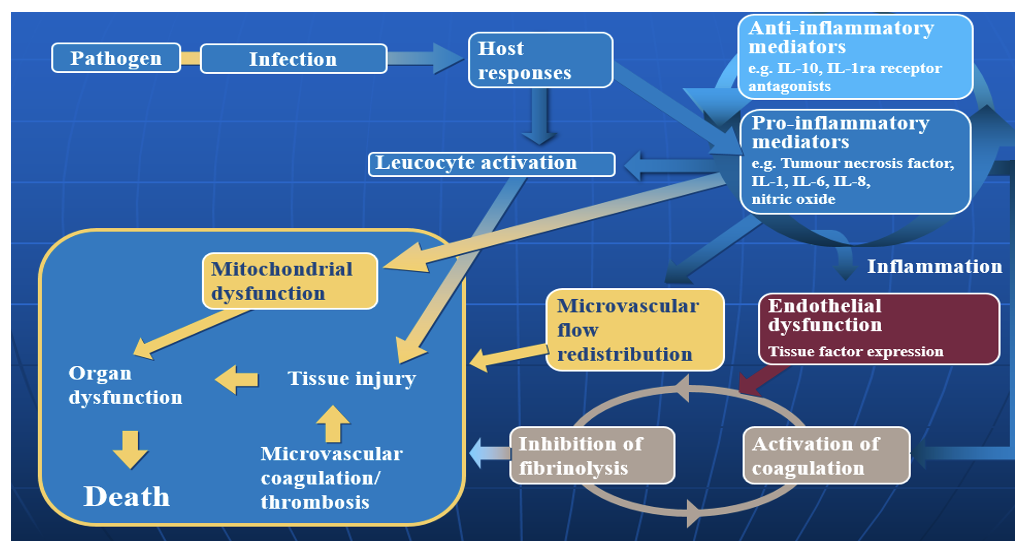
In sepsis, the imbalance between pro-inflammatory cytokines and anti-inflammatory mediators results in…
stimulated coagulation response
inhibited anticoagulant response
inhibited fibrinolytic response
These processes lead to endothelial damage and loss of equilibrium between the coagulation and fibrinolytic mechanisms.
As a procoagulant state develops, thromboses may form in the microvasculature, and in severe sepsis, the condition may progress to acute organ dysfunction and eventually death
Pro-inflammatory cytokines (including tumour necrosis factor, interleukin-1 and interferon-gamma) and thrombin are important in the…
up-regulation of adhesion molecules.
Therefore, in sepsis where there is excessive inflammation and thrombin production, there can also be increased expression of adhesion molecules, which leads to further inflammation, vascular endothelial injury and selectin expression
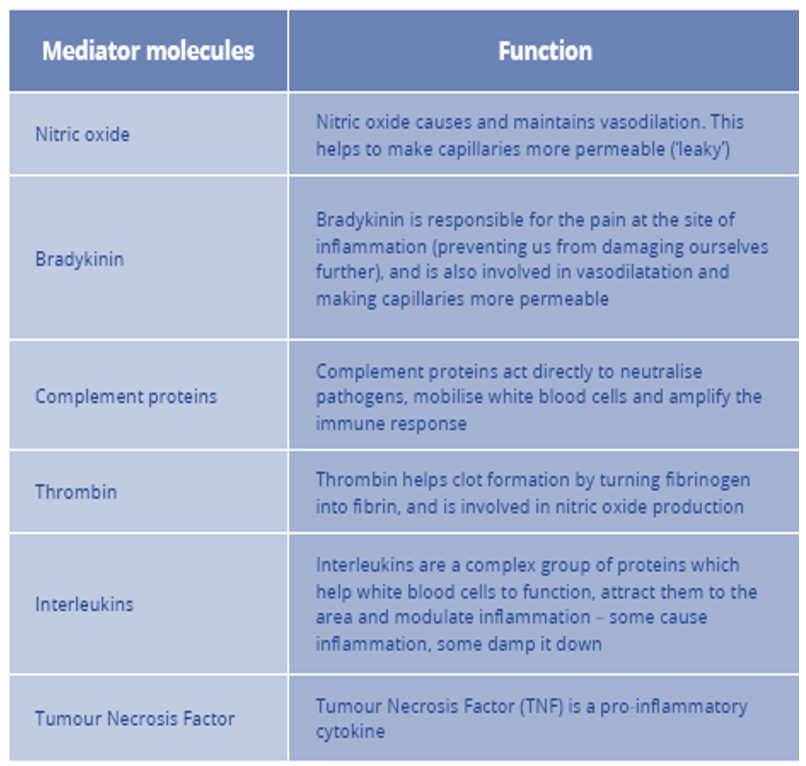
Summarise the pathogenesis of sepsis include the key mediator molecules.
Vasodilation and capillary leak – physiological response to infection
Lots of mediator molecules involved in the inflammation process
→ Balance of this inflammatory response goes “bad” in sepsis!
End result:
Hypovolaemia
Hypoperfusion at tissue/cellular level
Cell death
Organ dysfunction
Describe the process of Septic Shock.
“Septic Shock” Think about a hosepipe…..
Low water pressure in your hosepipe:
→ Not enough water (leaky capillaries - decrease circulating volume)
→ Diameter too wide (vasodilation)
Septic shock activates the coagulation system
Microthrombi in capillaries: this is from fibrinogen converting to fibrin, which binds to platelets > endothelial injury and release of inflammatory mediators
END RESULT: IMPAIRED BLOOD FLOW (AND OXYGEN) TO CELLS
Septic shock activates the coagulation system, causing sepsis-associated coagulopathy.
Fibrinogen converts to fibrin, which binds to platelets to form microvascular thrombi.
A marked or sustained procoagulant response to septic shock can lead to disseminated intravascular coagulation and widespread tissue injury, including loss of digits and limbs.
Microvascular thrombi amplify endothelial injury by the release of inflammatory mediators and by tissue hypoxia because of obstruction to blood flow.
What questions should you be asking if you suspect infection in a patient?
Can you identify the source?
Are there risk factors for sepsis?
Does the patients vital observations raise concern?
Breathing rate
Cold hands/feet
Increased pulse, decreased BP, decreased urine output
General appearance
In essence always think…. Could this be Sepsis?
What campaigns have been in place to help implement sepsis 6?
Hospital staff publicity campaign
Public awareness campaign
NHS 111 algorithims
Does sepsis 6 lead to increased antibiotic usage?
CQUIN on antibiotic usage at same time
Review of antibiotics within 72 hours
Overall antibiotic consumption
Broad spectrum IV antibiotic consumption
Importance of “Start Smart then Focus”
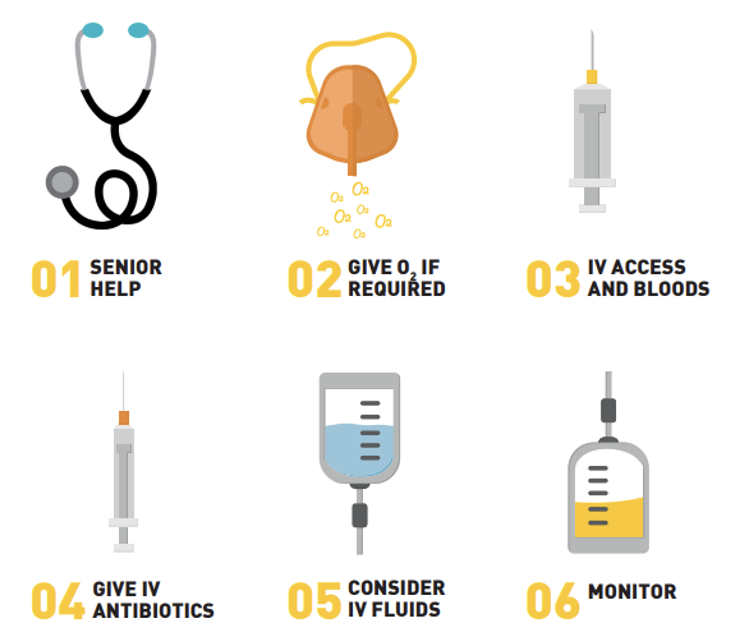
State the Sepsis 6
GIVE 3
Oxygen
Antibiotics
Fluids
TAKE 3
Blood cultures
Serum lactate
Urine output
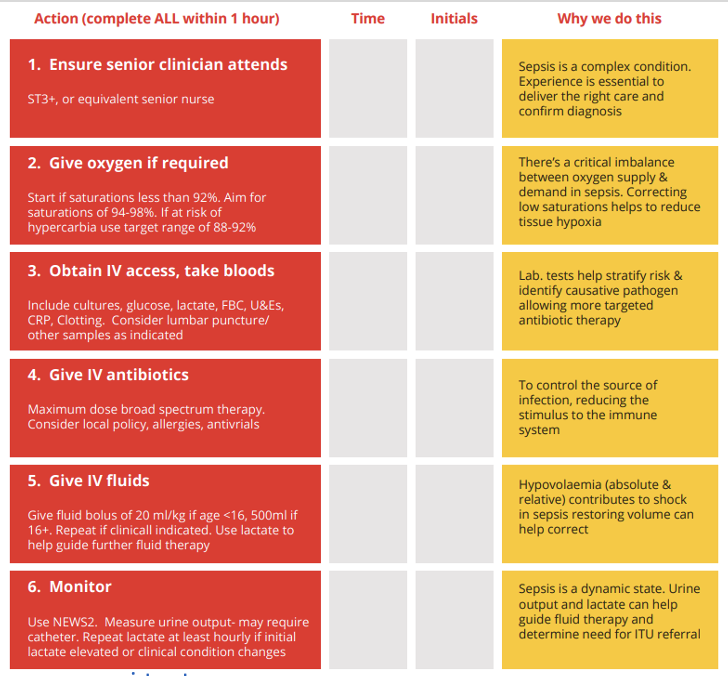
What are the keys point about Sepsis 6 - Ensure senior clinician attends?
New addition to Sepsis 6 in 2019
ST3+ or equivalent senior nurse
Ensure optimum collaborative care
Clinician experience is essential
Recent addition that they can verbally advice before attending, and senior involvement should not delay any other stages of the sepsis 6 management
What are the keys point about Sepsis 6 - GIVE Oxygen?
Imbalance between tissue oxygen supply and demand
- Reduced BP
- Tissue oedema
- Abnormal blood flow at capillary level
- Hyper-metabollic state – cellular oxygen demand increased
Start if 02 sats <92%
High flow oxygen initially
Enough to keep saturations >94% to reduce hypoxia and possible organ damage
→ Correcting low saturations helps reduce hypoxia and organ injury
What are the keys point about Sepsis 6 - Obtain IV access and take bloods?
Blood cultures
Help identify pathogen and direct antibiotic therapy (start SMART then FOCUS)
Aerobic and anaerobic bottles from peripheral site
Take before giving antibiotics if possible
Consider other samples (CSF, urine, sputum)
Lactate
Measured on arterial blood gases
Marker of tissue hypoperfusion. Indicates anaerobic respiration in cells
Helpful in initial diagnosis of sepsis and marker of effectiveness of therapy
Aim for ≤2mmol/L
Generally ≥4mmol/L concerning
Blood glucose
FBC, U&Es, CRP
What are the keys point about Sepsis 6 - GIVE IV Antibiotics?
According to guidelines – consider:
Likely source of infection
Allergies
Adequate levels at suspected site of infection
Broad is best…….???? Start SMART then FOCUS
Treat for most likely cause of infection if known (not just “sepsis”)
The GOLDEN hour
For each hour’s delay in administering antibiotics in septic shock, mortality increases by 7.6%*
What are the main causes of sepsis cases?
What are the keys point about Sepsis 6 - GIVE IV fluids
Improve pre-load to heart by correcting hypovolaemia
Improve blood pressure and cardiac output
500mL of crystalloid (e.g Hartmanns or Plasmolyte) quickly then further boluses according to response (Lactate, BP, clinical). More isotonic so remain in blood vessels
May opt for NaCl if lactate is elevated
Caution not to fluid overload
What needs to be monitored during sepsis?
Urine Output
Decreases in hypovolaemia
Used as an indicator of cardiac output
Target 0.5mL/kg/hr. May require catheterisation for accurate assessment
Use a fluid balance chart for accurate recording
Serial Lactates
If initial lactate >2, monitor hourly
NEWS2
State the Sepsis 6 checklist
The NEWS is based on a simple aggregate scoring system in which a score is allocated to physiological measurements, already recorded in routine practice, when patients present to, or are being monitored in hospital. Six simple physiological parameters form the basis of the scoring system:
respiration rate
oxygen saturation
systolic blood pressure
pulse rate
level of consciousness or new confusion
temperature.
For each overall news score what monitoring is required for each one…
NEWS 0
NEWS 1-4
NEWS >5
NEWS > 7
monitor 12hrly
monitor 4-6hrly
monitor minimum hourly
continuous monitoring of vital signs