L2- Acute Kidney Injury
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
What is the functional unit of the kidney?
The nephron.
What are the two main components of a nephron and what are their functions?
Glomerulus (filtration)
Tubule (reabsorption and secretion to modify the filtrate)
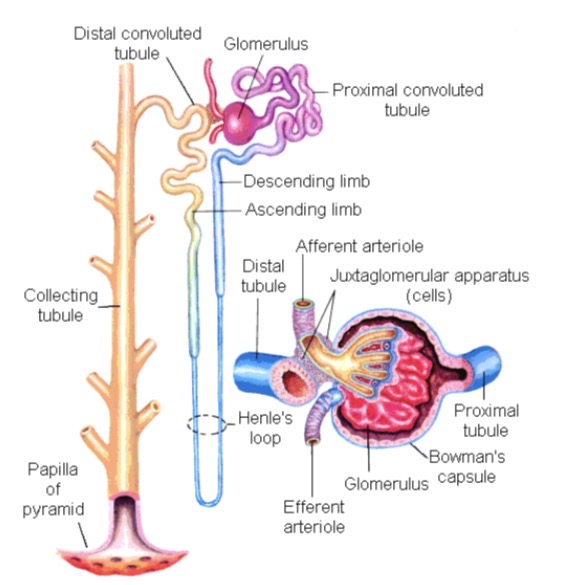
What regulates glomerular filtration in the nephron?
Afferent arteriole
Efferent arteriole
Approximately how many nephrons are present in each kidney?
~1 million nephrons.
What percentage of nephrons are located in the cortex vs medulla?
Cortex- About 85%.
Medulla- About 15%.
What 3 structures are located in the renal cortex?
Glomeruli
Bowman’s capsule
proximal and distal tubules of
the juxtamedullary nephrons
What structures are found in the renal medulla?
Renal pyramids
Renal columns
Loop of Henle
Vasa recta
Collecting ducts of
the juxtamedullary nephrons
Which part of the kidney is most susceptible to ischemia? Give 3 reasons why
The medulla.
Low oxygen tension
High metabolic activity
Countercurrent blood supply
What is acute kidney injury (AKI)?
A rapid decline in glomerular filtration rate (GFR) leading to retention of nitrogenous waste products (urea and creatinine).
What are the three major pathophysiological categories of AKI?
Pre-renal
Intrinsic renal
Post-renal
What is the basic pathophysiology of pre-renal AKI? Give 5 causes
Renal hypoperfusion due to
hypotension
Heart failure (Decreased CO)
Volume depletion (blood loss, vomiting)
Liver failure
Sepsis
What 4 hormonal systems are activated during renal hypoperfusion in pre-renal AKI? What is the purpose of these responses?
Noradrenaline
Angiotensin II
Endothelin
ADH
Reduce renal blood flow and preserve salt and water.
9 Clinical Features of Pre-renal AKI
Dry mouth
Dizziness
Hypotension (low BP)
Tachycardia
Slack skin (Reduced skin turgor)
Thirst
Weight loss
Reduced urine output (oliguria)
The patient also may have symptoms/signs of heart or
liver disease
What causes intrinsic renal AKI?
Structural damage to kidney tissue
What are 5 major causes of intrinsic renal AKI?
Glomerulonephritis
Atheroembolic disease
Acute interstitial nephritis's
Acute glomerulonephritis
Acute tubular necrosis
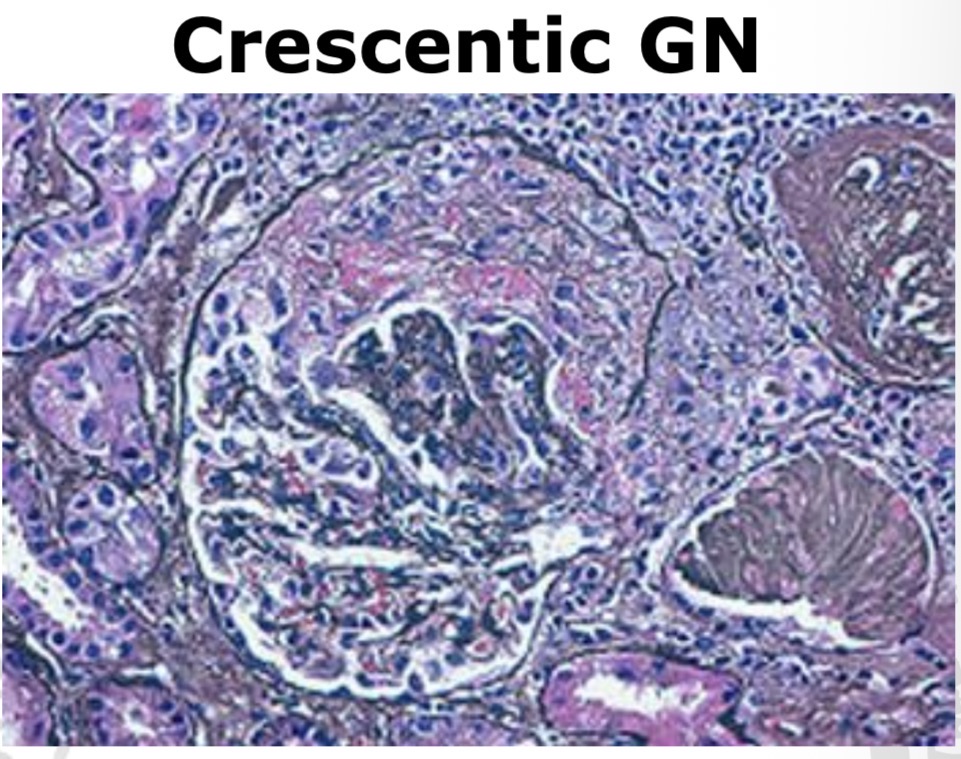
What pathological feature characterizes crescentic glomerulonephritis?
Crescent formation in Bowman’s space
What type of process causes acute interstitial nephritis?
Inflammatory reaction in renal interstitium.
What is the 4 classic features of AIN?
Fever
Rash
Eosinophiluria
Leukocyturia
What is AIN caused by?
Usually drug related
Antibiotics (especially penicillin)
Proton pump inhibitors
Spontaneous
Hereditary
What are the 2 treatments of AIN?
Withdrawal of offending drug & observation
Occasionally corticosteroids
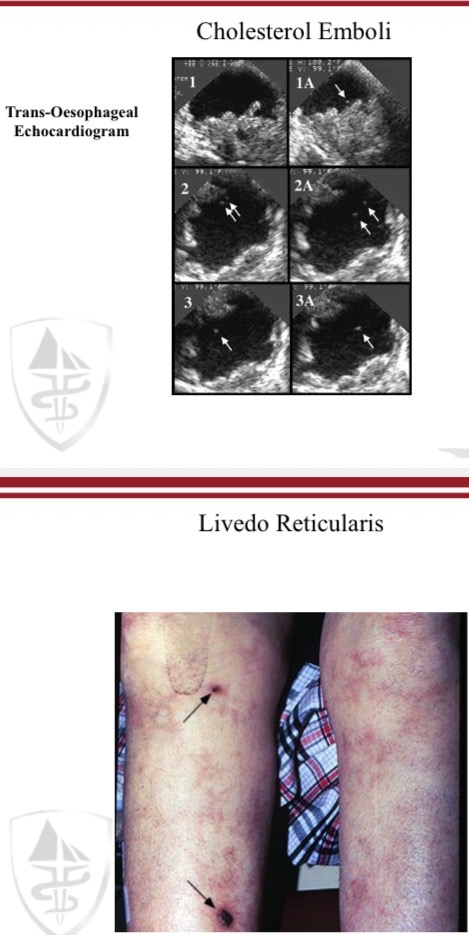
What causes renal atheroembolic disease?
Acute or Chronic Deterioration due to underlying atherosclerotic disease due to cholesterol emboli from atherosclerotic plaques.
What 2 patient groups are at risk of renal atheroembolic disease?
Peripheral vascular disease
Coronary artery disease
What 2 clinical findings suggest Atheroembolic Disease?
Livedo reticularis (skin)
Eosinophiluria (Eosinophiluria)
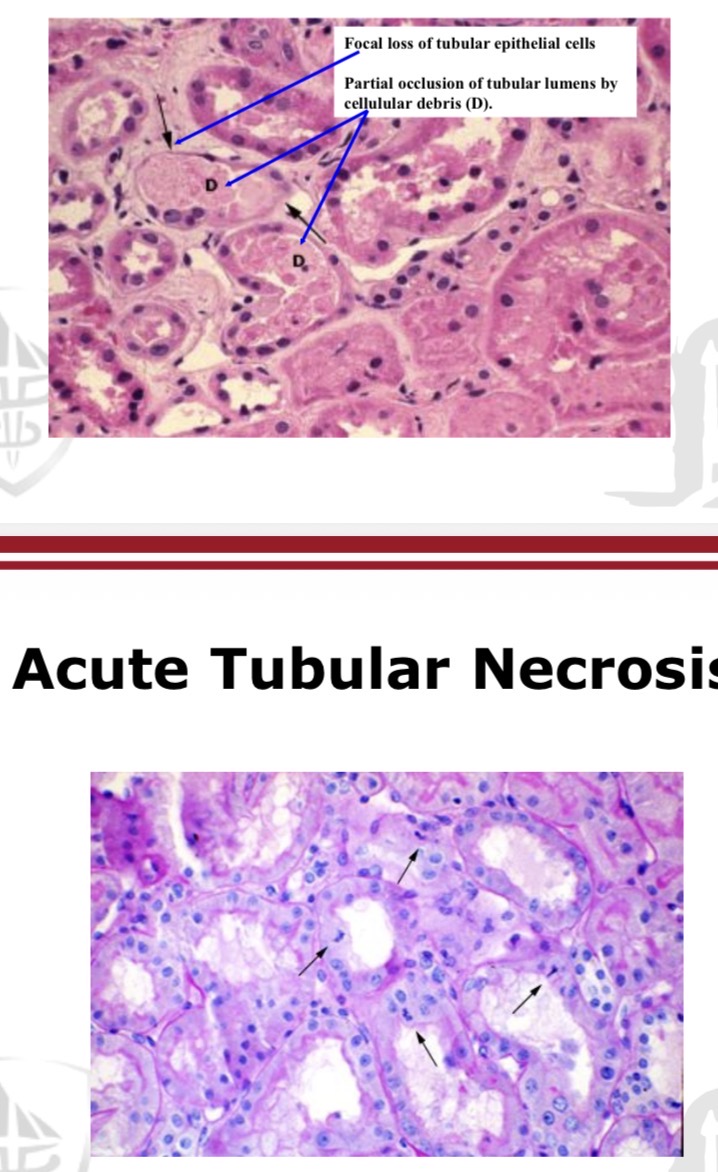
What is the most common cause of intrinsic AKI?
Acute tubular necrosis.
What are the 3 main pathological processes in ATN?
• Medullary Ischaemia
• Tubular damage
• Tubular Obstruction secondary to
sloughing of tubular cells and debris
What are common causes of ATN? (%)
Sepsis (48%)
Hemodynamic causes (32%)
Toxic causes (20%)
What are 6 toxic causes of ATN?
– ACE inhibitor
– NSAID
– Contrast Dye (perhaps less of a concern than originally thought)
– Antibiotics (gentamicin, amphotericin)
– Pigment Nephropathy (caused by rhabdomyolysis)
– DIC
CAPDAN
What is the mechanism of post-renal AKI?
Urinary outflow obstruction.
What 2 imaging findings suggest post renal AKI?
hydronephrosis → Dilatation of the renal pelvis due to obstruction.
hydroureter → Dilatation of the ureter due to distal obstruction.
What are 6 common causes of post-renal AKI?
Benign prostatic hyperplasia (BPH)
Urinary Retention (Drugs or Neurological Condition)
Pelvic malignancy
Nephrolithiasis (rare)
Retroperitoneal fibrosis
Urethral stricture
BURNUP
What 10 exposures may precipitate AKI?
Sepsis
Critical illness
Circulatory shock
Burns
Trauma
Cardiac surgery (especially with cardiopulmonary bypass)
Major non-cardiac surgery
Nephrotoxic drugs
Radiocontrast agents
Poisonous plants and animals
BCCCMNPRST
What 9 patient factors increase susceptibility to AKI?
Dehydration or volume depletion
Advanced age
Female gender
Black race
Chronic kidney disease (CKD)
Chronic diseases (heart, lung, liver)
Diabetes mellitus
Cancer
Anemia
BAD FAD CCC
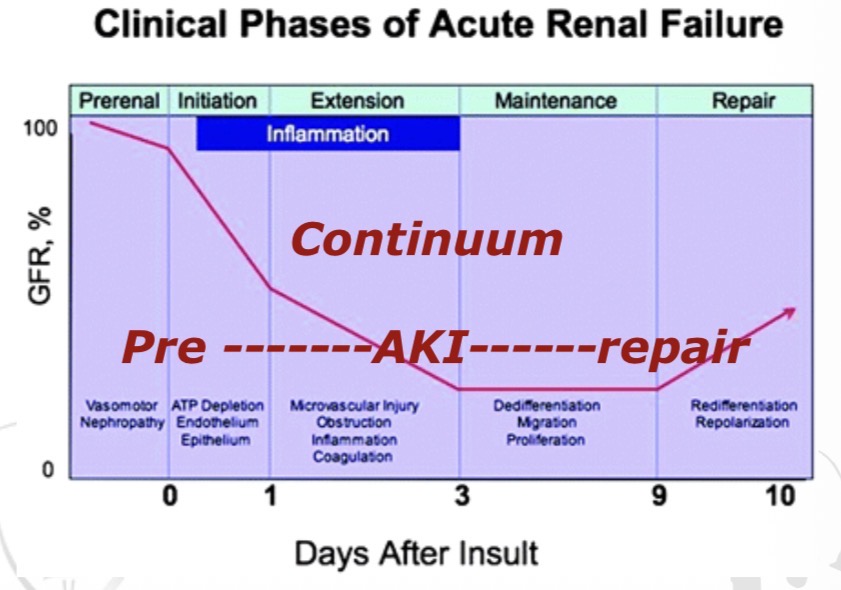
What is the continuum of acute kidney injury?
Pre-renal state (renal hypoperfusion)→ AKI → Recovery/ repair phase.
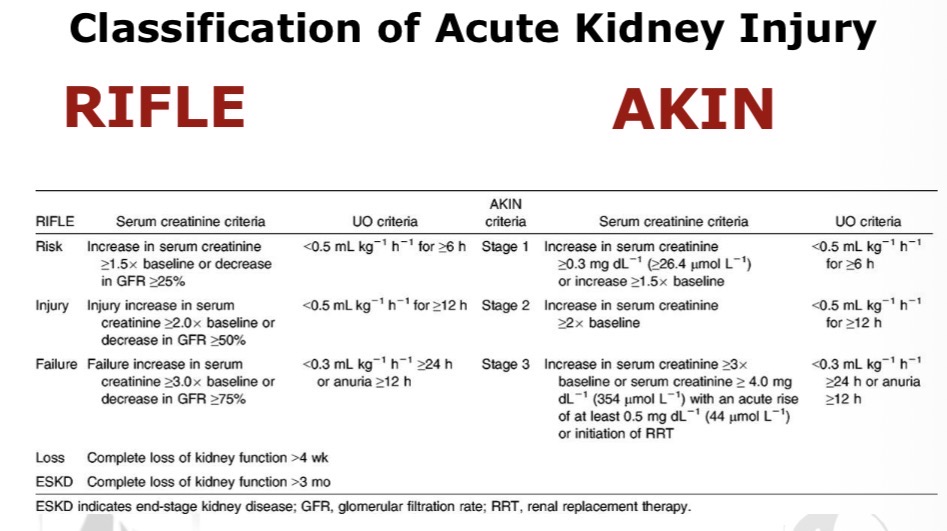
What are the two classification systems for AKI severity?
RIFLE classification
Risk
Injury
Failure
Loss
End-stage kidney disease
AKIN classification (Acute Kidney Injury Network)
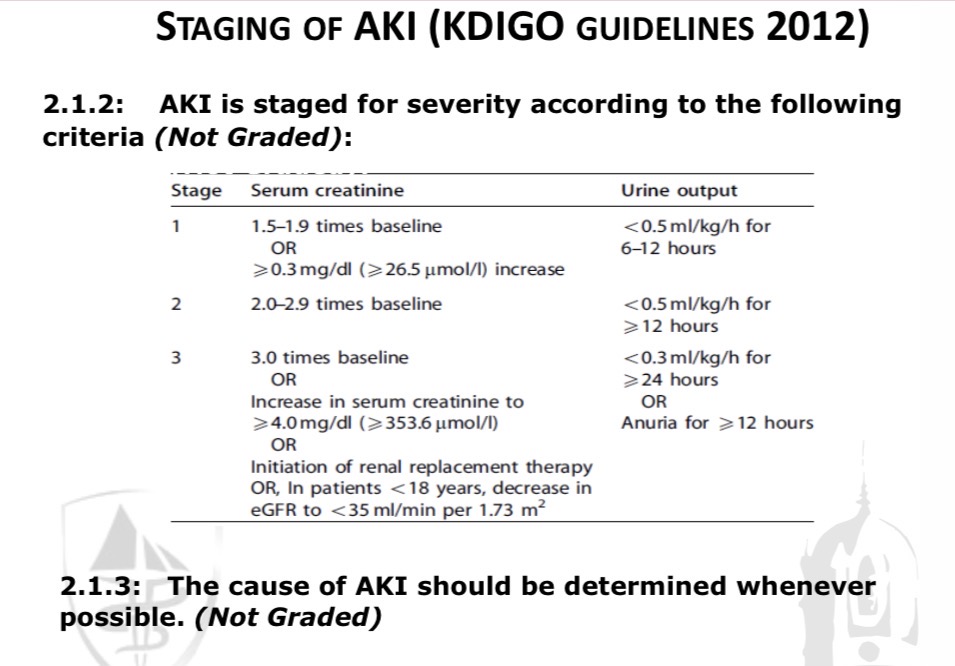
According to KDIGO guidelines (2012), how is AKI assessed?
By staging severity based on creatinine rise and urine output - The cause of AKI should always be determined whenever possible
What 9 investigations are used to diagnose AKI?
History
Physical examination
Urine microscopy
Serum chemistry
Urine sodium
Chest X-ray (CXR)
Renal ultrasound
Renal biopsy (in selected cases)
Additional laboratory tests
What 4 examination findings help assess AKI?
Pulse volume - Low-volume pulse
Blood pressure- lying and standing.
Neck veins- Volume status.
Skin rash
Drug reactions
Vasculitis
Is AKI usually symptomatic early?
No — it is often asymptomatic initially
What urine output change occurs in about half of AKI patients?
Oliguria (Urine output <400 mL in 24 hours)
What laboratory changes occur in AKI?
Rising urea
Rising creatinine
What 3 complications may develop in AKI?
Volume overload
Metabolic acidosis
Hyperkalemia
4 criteria in diagnosis of pre-renal AKI
• Hx of volume loss
• Elevated urea and creatinine
• Altered urea/creatinine ratio
ie. disproportionate elevation of urea
• Bland urinary sedimen
6 criteria for Diagnosis of Intrinsic Renal Disease
– Hx of volume loss/hypotension (anaesthetic note)
– Elevated urea and creatinine
– Ratio maintained
– Muddy brown casts - ATN
– Rbc, WBC, casts (red or white) on urinalysis
– Proteinuria – glomerular disease
What 3 conditions cause a bland urine dipstick?
Acute interstitial nephritis
Acute tubular necrosis
Some forms of myeloma
What 3 conditions cause blood only on dipstick?
IgA nephropathy
Post-infectious GN
Lupus nephritis
What 4 conditions cause protein only on dipstick?
Minimal change disease
Membranous nephropathy
Focal segmental glomerulosclerosis (FSGS)
Amyloidosis
What 5 conditions cause both blood and protein on dipstick?
Rapidly progressive GN
ANCA-associated vasculitis
Anti-GBM disease
IgA nephropathy
Lupus nephritis
What 8 symptoms suggest obstructive (post-renal) AKI?
Poor urinary stream
Frequency
Nocturia
Dribbling
Dysuria
Pain
Weight loss
Anorexia
What urine sodium level suggests pre-renal AKI vs intrinsic renal disease?
pre-renal AKI <20 mEq/L
intrinsic renal disease >40 mEq/L
What urine osmolarity suggests pre-renal AKI vs ATN?
pre-renal AKI >500 mOsm/kg (kidneys conserve water).
ATN <450 mOsm/kg (loss of concentrating capacity)
Why should previous laboratory tests be reviewed in AKI evaluation?
To identify previous chronic kidney disease.
What 3 lab abnormalities suggest chronic kidney disease?
Elevated phosphorus
Hypocalcemia
Anemia
What are the 2 key principles in AKI management?
Maintain intravascular volume.
Perfusion
What should be given when pre-renal AKI is suspected?
• Trial of Fluids If suspect a pre-renal
element.
• 5-10mls/kg bolus of Isotonic Fluid (saline or ringers lactate)
• Monitor for evidence of volume overload
What 3 drugs should be avoided in AKI?
NSAIDs
ACE inhibitors
SGLT2 inhibitors.
How do ACE inhibitors affect glomerular hemodynamics?
Efferent arteriole vasodilation.
How do SGLT2 inhibitors affect glomerular hemodynamics?
Afferent arteriole vasoconstriction → Reduce intraglomerular pressure and protect nephrons.
Is the kidney protective effect of SGLT2 inhibitors dependent on glucose lowering (T2D)?
No.
What 4 investigations are required for severe hyperkalemia?
ECG
Cardiac monitoring
Venous blood gas
Lab potassium measurement
Hyperkalemia Management- 5 steps
– Stabilise myocardium-30ml of 10%calcium gluconate IV, repeat ECG if changes
– 5-10 units iv insulin with 50ml of 50%
dextrose
– Salbutamol nebs
– +/- IV bicarbonate- may need renal input
– +/- Dialysis
3 steps when managing acidosis in AKI
Do an ABG
Confirm acidosis
Check respiratory compensation
Exclude mixed disorders
Determine if metabolic or respiratory
Calculate the anion gap
Identify cause of metabolic acidosis
Causes of Normal Anion Gap Acidosis
Hyperalimentation
Acetazolamide / Amphotericin B
Renal tubular acidosis
Diarrhea
Uretero-sigmoidostomy
Pancreatic fistula / post-hypercapnic state
(HARDUP)
Causes of High Anion Gap Acidosis
Glycols
Oxoproline
L-lactate
D-lactate
Methanol
Aspirin
Renal failure
Ketones
(GOLDMARK)
What are the 5 major indications for dialysis in AKI (Kidney Replacement Therapy-KRT)?
Refractory volume overload
Hyperkalemia (>6.5 mEq/L or rapidly rising)
Severe metabolic acidosis (pH <7.1)
Uremic complications (pericarditis, neuropathy, altered mental status)
Poisoning
Name 2 types (modalities) of KRT.
IHD (Intermittent Haemodialysis)
CRRT (Continuous Renal Replacement Therapy)- may improve patient outcomes
What is the duration of AKI recovery?
Variable
What usually happens to kidney function after recovery?
Often returns to baseline.
Which type of AKI has a better prognosis, oliguric or non-oliguric?
Non-oliguric
What long-term risk occurs after AKI?
Increased post-hospital mortality.
What is the overall mortality of AKI?
20–70%.
What is the mortality in ICU patients requiring dialysis? Why might modern outcomes appear better?
79% - modern outcomes appear better as dialysis started earlier due to lower thresholds.
A 56-year-old man with hypertension, type 2 diabetes, hypercholesterolemia, and osteoarthritis undergoes an elective laparoscopic cholecystectomy for cholelithiasis. His medications include diclofenac, ramipril, dapagliflozin, amlodipine, atorvastatin, and metformin.
Pre-operative labs show creatinine 121 µmol/L and eGFR 56 mL/min.
During surgery there is a bile leak requiring conversion to open surgery and severe hypotension (60/40 mmHg for ~15 minutes).
Post-operatively he develops fever (39°C), leukocytosis (WCC 20,000), and abdominal pain, and is transferred to the ICU. A contrast CT abdomen reveals a fluid collection which is drained. He receives gentamicin, metronidazole, and cefotaxime.
His urine output falls to 10 mL/hr then becomes anuric, with 210 mL total urine in 24 hours. Over the next few days creatinine rises from 257 → 321 → 467 → 550 µmol/L.
On day 4 he has:
pH 7.05
Potassium 6.9 mEq/L
Anion gap 25
Urine sodium 60 mEq/L
Chest X-ray: volume overload
O₂ saturation 85% on 100% FiO₂
What type of AKI is most likely?
Intrinsic AKI → Acute tubular necrosis
How can diclofenac cause renal failure?
NSAIDs inhibit prostaglandins → afferent arteriole vasoconstriction → reduced renal perfusion.
A 56-year-old man with hypertension, type 2 diabetes, hypercholesterolemia, and osteoarthritis undergoes an elective laparoscopic cholecystectomy for cholelithiasis. His medications include diclofenac, ramipril, dapagliflozin, amlodipine, atorvastatin, and metformin.
Pre-operative labs show creatinine 121 µmol/L and eGFR 56 mL/min.
During surgery there is a bile leak requiring conversion to open surgery and severe hypotension (60/40 mmHg for ~15 minutes).
Post-operatively he develops fever (39°C), leukocytosis (WCC 20,000), and abdominal pain, and is transferred to the ICU. A contrast CT abdomen reveals a fluid collection which is drained. He receives gentamicin, metronidazole, and cefotaxime.
His urine output falls to 10 mL/hr then becomes anuric, with 210 mL total urine in 24 hours. Over the next few days creatinine rises from 257 → 321 → 467 → 550 µmol/L.
On day 4 he has:
pH 7.05
Potassium 6.9 mEq/L
Anion gap 25
Urine sodium 60 mEq/L
Chest X-ray: volume overload
O₂ saturation 85% on 100% FiO₂
What 6 factors contributed to this patient’s AKI?
Intraoperative hypotension
Sepsis
Nephrotoxic drugs
Contrast CT
ACE inhibitor
NSAID use
Diabetes
A 56-year-old man with hypertension, type 2 diabetes, hypercholesterolemia, and osteoarthritis undergoes an elective laparoscopic cholecystectomy for cholelithiasis. His medications include diclofenac, ramipril, dapagliflozin, amlodipine, atorvastatin, and metformin.
Pre-operative labs show creatinine 121 µmol/L and eGFR 56 mL/min.
During surgery there is a bile leak requiring conversion to open surgery and severe hypotension (60/40 mmHg for ~15 minutes).
Post-operatively he develops fever (39°C), leukocytosis (WCC 20,000), and abdominal pain, and is transferred to the ICU. A contrast CT abdomen reveals a fluid collection which is drained. He receives gentamicin, metronidazole, and cefotaxime.
His urine output falls to 10 mL/hr then becomes anuric, with 210 mL total urine in 24 hours. Over the next few days creatinine rises from 257 → 321 → 467 → 550 µmol/L.
On day 4 he has:
pH 7.05
Potassium 6.9 mEq/L
Anion gap 25
Urine sodium 60 mEq/L
Chest X-ray: volume overload
O₂ saturation 85% on 100% FiO₂
What dialysis indications are present in this patient?
Severe hyperkalemia
Severe metabolic acidosis
Volume overload
Oliguria