Urinary system
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
Kidneys
Major excretory organs that maintain internal environment
How do kidneys maintain internal enviornent
Regulation H20 volume and solute concentrations
regulate ion concentrations in ECF,
acid-base balance,
excreting metabolic wastes,
produce erythropeitin and renin
How much o2 do the kidneys use at rest
20-25%
how many times a day do kidneys filter entire plasma vol
60
filtrate
blood plasma minus proteins <1% urine
medial renal hilum
marks where vasculature nerves and urinary tract enter/exit kidneys
Ureters(ext kidney)
urine from kidney to bladder
urinary bladder(ext kidney)
temporary storage for urine
urethra(ext kidney)
carries urine out body
cardiac output
renal arteries deliver 25% CO to kidneys every min
what kidney sits lower due to liver
right
because kidney’s are protected by inferior ribs they are prone to
damage from blunt trauma(esp. right)
3 distinct regions of internal kidneys
renal cortex, renal medulla, renal pelvis
Renal cortex
superficial region
renal medulla
deep to cortex composed of cone-shaped renal pyramids
renal pelvis
continuous with ureter
structures in renal pelvis
minor calyces, major calyces
minor calyces
cup shaped, collect urine from pyramids
major calyces
collect from minor calyces and empty into renal pelvis
pyelonephritis
infection or inflammation of entire kidney(fecal bacteria into urinary tract)
what causes pyelonephritis
untreated UTI
symptoms of pyelonephritis
fever, back pain, chills, painful urination, bloody(hematuria) or cloudy urine
servere pyelonephritis
cause kidney to swell, abscess formation, pus may fill renal pelvis
nephron
structural and functional units responsible for urine formation( actual filtration unit)
how may nephron
more 1 million
cortical nephrons
entirely inside renal cortex space, 85% of nephrons
juxtamedullary nephrons
long, nephron loops of tubule network extend deep into renal medulla, important for formation of concentrated urine
Nephron structure
Renal corpuscle, renal tubule
What does the renal corpuscle consist of
Glomerulus, Glomerular capsule, afferent arteriole, efferent arteriole
Renal corpuscle process( what you cannot lose)
blood enters glomerulus through afferent arteriole, filtration begins, filtrate collects in glomerular capsule, blood exits glomerulus through effect arteriole to capillaries, filtrate goes to proximal convoluted tubule(PCT)
Renal tubule proximal convoluted tubule( could keep or lose(selective))
Gets filtrate from renal corpuscle
Renal tubule nephron loop
continue with PCT, perm with H20
renal tubule distal convoluted tubule
drains filtrate into collecting duct goes into renal medulla
Renal tubule peritubular capillaries
low pressure pours capillaries adept at h20 and solute absorption
juxtaglomerular apparatus
regulates rate of filtrate formation and blood pressure( each nephron has 1)
JGA made of of modified prtions of:
Distal convoluted tubule: refeeds afferent arteriole and glomerulus, contains macula densa Afferent arteriole renal corpuscle: contains granular cells, recpeptor monitor BP, contain and secrete renin triggering mechanism Extraglomerular mesangial cells: allow for communication between macula densa and granular cells
Glomerular filtration
1st step of urine formation and blood composition adjustment
Glomerular filtration process
passive, hydrostatic(pushing) pressure forces fluids and solutes through membrane into capsular space
What can pass glomerular filtration
h20, glucose, amino acids, and nitrogenous wastes
What can NOT pass glomerular filtration
Cells and proteins( exit glomerulus through efferent arteriole, peritublar capillaries, circulation)
Glomerular filtration rate(GFR)
vol. of filtrate formed per min by both kidneys( Normal=120-125 mL/min)
GFR is directly proportional to:
Net filtration pressure: change diameter of afferent arterioles, Total SA available for filtration: Glomerular cap. have huge SA, Filtration permeability membrane: Glom. cap. much more permeable that other capillaries
How is GFR measured
Renal clearence
Renal clearance
Vol. of plasma the kidneys can clear of a particular substance in a given time
Chronic renal disease
GFR<60 mL/min for 3 mos
Renal failure
GFR <15 mL/min
Tubular reabsorption
reclamation of contents from filtrate into particular capillaries, mostly organic nurtrients, h20 and ion reabsorption hormonally regulated
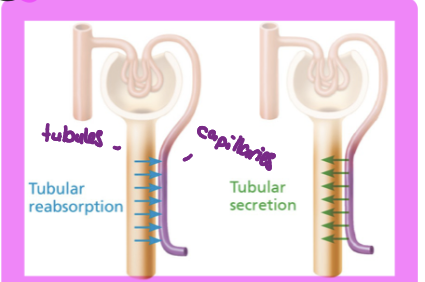
Tubular secretion
contents form peritubular capillaries are added to filtrate into tubules, important for waste disposal
Transport maximum
limit how much of a substance can be reabsorbed
Where does tubular reasoption and secretion mainly occur
PCTA
Atrial natriuretic peptide
increase Na secretion, results in decreased blood volume and BP
Parathyroid hormone
Increase Ca reapportion at DCT
Antidiuretic hormone
Increase water reabsorption at DCT and collecting duct
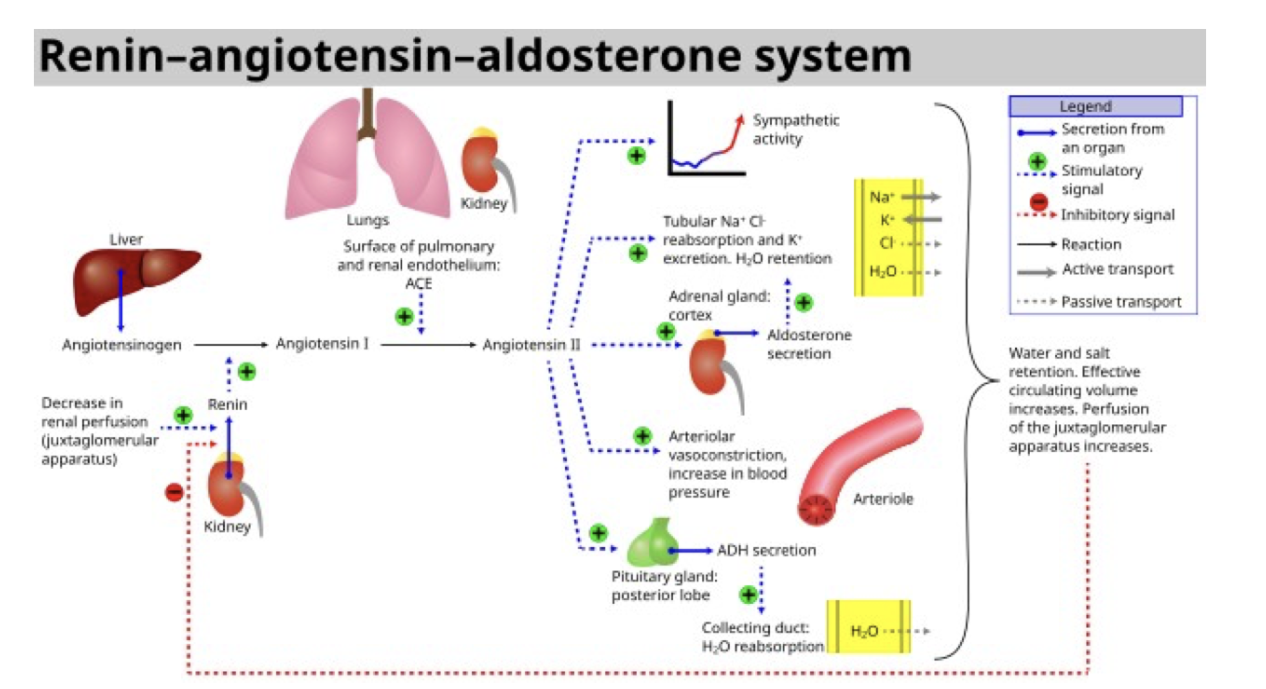
Renin-angiotensisn-aldosterone mechanism
main mechanism for increasing BP
Stimulates increased ion reabsorption for increased BV and BP
Renin mechanism steps
Renin secretion from kidney and angiotensinogen from liver
make angiotensin 1
ACE from lungs coverts ^ to angiotensin II
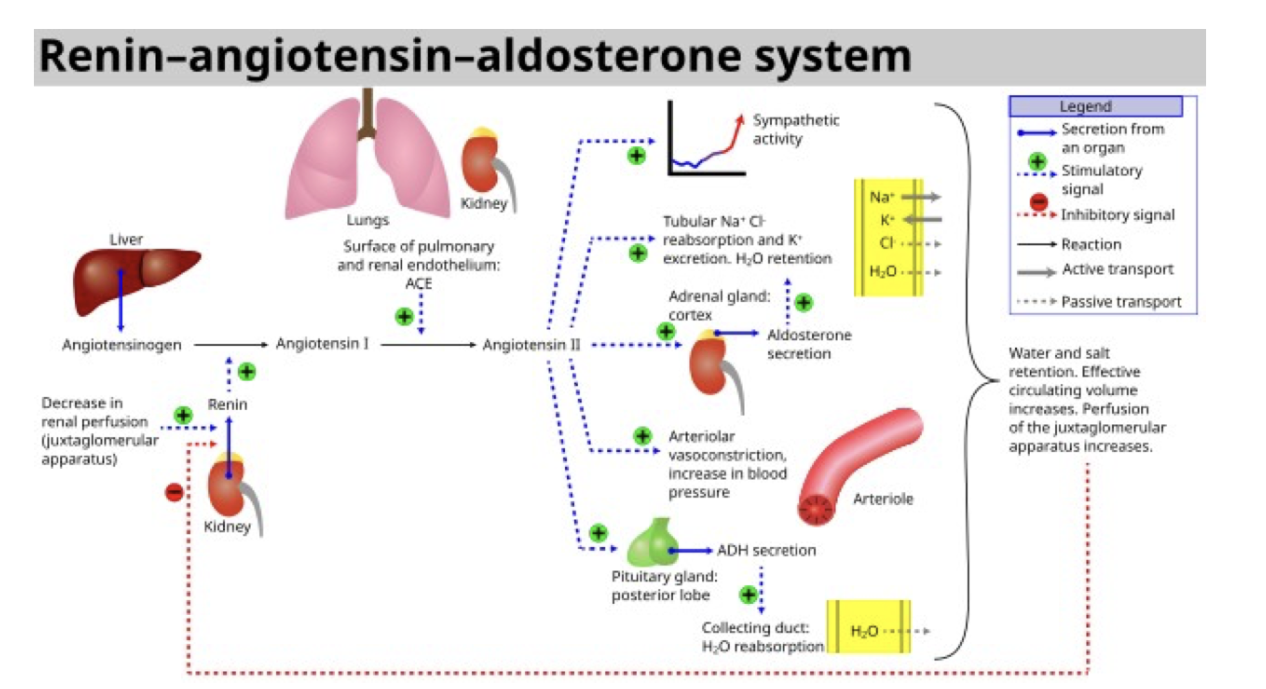
What does angiotensin II stimulate the release of
ADH= increased BV and BP
aldosterone release=Na reabsorption K secretion
Loop of Henle
Descending limb and ascending limb
water and solute reabsorption are not coupled
critical role in regulating urine concentration
Descending limb(loop)
Water CAN be reabsorbed (many aquaporins)
Solute CANNOT be reabsorbed
Ascending limb(loop)
Water CANNOT be reabsorbed (few aquaporins)
Solute CAN be reabsorbed
Urine make up
95% h20 5% solute
Solutes
nitrogenous wastes
Urea(solute)
from amino acid breakdown
most prevalent
Uric acid(solute)
from nucleic acid metabolism
Creatinine(solute)
metabolite from phosphocreatine breakdown
Excess or abnormal solutes=
diagnostically significant
Urine concentration
kidneys need to adjust urine concentration and volumes to maintain body fluids’ osmotic concentrations
Anuria
abnormally low urine output(<50mL day)
may indicate glomerular BP is too low for filtration
may arise from lack of nephron function(renal failure)
Diuretics
chemicals enhancing urine output
ADH inhibitors
Na reabsorption inhibitors
Osmotic diuretics: substances that don’t get reabsorbed
Urinalysis
examination of urine for signs of disease
Diabetes mellitus urine smell
acetone
urine pH
slightly acidic (4.5-8.0)
specific gravity
ratio of mass solute to mass of equal volume water (urine>water due to solutes)
used to assess hydration
passage of urine
ureters
urinary bladder
urethra
urinary bladder
storage vessel
collapses when empty
lined with rugae
male capacity> women
Internal urethral sphincter
bladder urethra junction
involuntary