Looks like no one added any tags here yet for you.
Goal of immunization
to protect against disease upon subsequent exposure to the infection
Passive immunity
transfer of immunity produced by one human or animal to another
implications for immunization - drug interaction with live vaccines
Transplacental transfer
mode of passive immunity
active transport of IgG during last 1-2 months of gestation (weeks 32-40)
go across concentration gradient
baby will get antibodies
good protection from some diseases - measles, rubella, tetanus
poor protection from some diseases - polio
interferes with response to live vaccines as maternal antibodies neutralize vaccine before infant mounts an immune response
active immunity
stimulate the host to produce a protective response to an antigen
natural infection
immunizations
relies on immunologic memory
makes its own memory
makes their own response
vaccine formulations
live attenuated
whole inactivated
polysaccharide
conjugate
recombinant DNA
toxoid
mRNA
general recommendations for vaccines
timing of immunization
childhood and adult immunization schedules updated frequently and published each year
vaccine timing
any commonly used vaccines can be administered during the same encounter
inactivated vaccines and inactivated and live vaccines can be administered at intervals without regard to each other
live vaccines must be separated by 4 weeks if not administered simultaneously
live vaccine timing
on or after the first birthday
delay following administration of antibody-containing product
separated by at least 4 weeks
live vaccine administered second should not be counted
repeat that vaccine at least four weeks after it was administered as an invalid dose
vaccine dosing intervals
increasing the interval between doses does NOT diminish the effectiveness
no need to restart ANY vaccine series
decreasing the interval between doses may interfere with vaccine response
immunization of immune individuals
no evidence of harm
MMR, varicella, HiB hepB, polio
increased incidence and severity of local reactions
PPSV23 administered <4 years
Td too frequently
pain, swelling, redness
hence, can’t find on records, REIMMUNIZE
vaccine contraindications (general)
severe allergy to vaccine component
for future pertussis containing vaccines: encephalopathy without known cause within seven days of pertussis vaccine
very uncommon
temporary contraindications
pregnancy
immunosuppression
decreased response to immunization
live attenuated vaccines contraindicated
severe illness (not terrible but worse things to worry about)
recent receipt of blood and immune globulin products
herd immunity
community immunity, community protection, indirect protection
protection conferred to susceptible individuals when sufficient proportion of the population is immune
depends on reproduction number, Ro
on how transmissible it is
number of people to which an infected person transmits the infection
assumes equal mixing of an entirely susceptible population
for sars-cov2 estimated Ro=2-3
measles was Ro=18
Threshold = 1-1/Ro
approach to herd immunity
herd immunity describes immunization strategies
no infection has ever achieved herd immunity
likely unable to protect the vulnerable
NEED IMMUNIZATIONS TO GET TO HERD IMMUNITY
immunization to herd immunity
need community immunity at 60%
assume
estimate that 10% has been infected
vaccine confers 70% protection
to achieve herd immunity, need vaccine uptake at least 70%
measles
highly infective viral disease
most contagious disease known
transmitted primarily by larger respiratory droplets
fever, cough, coryza (runny nose), conjunctivitis
complications include otitis media, pneumonia, encephalitis
estimated that 10% of cases involve complications
death rate 1-3/1,000
measles elimination
goal of healthy people 2010
WHO, Pan American Health Organization formulated plans for elimination and eradication
measles eliminated from US
importations frequent
threats from vaccine hesitancy and delay
must keep immunizing
measles outbreaks
immunization rates sufficient to prevent widespread
transmission within unimmunized communities
85% of cases in unimmunized due to philosophical or religious belief (from 2014 outbreak)
other 15% were too young
measles vaccine
live attenuated viral vaccine
usually administered in combination with mumps and rubella
combination of measles, mumps, rubella, and varicella available
vaccine administered at 12-15 months of age with a second dose prior to entering school
evaluate travelers for immune status
vaccination strategies for measles
two dose strategy implemented in early 1990s
second dose is not a “booster”
second chance to get immune
two doses recommended for healthcare workers and college students
can consider those before 1957 immune
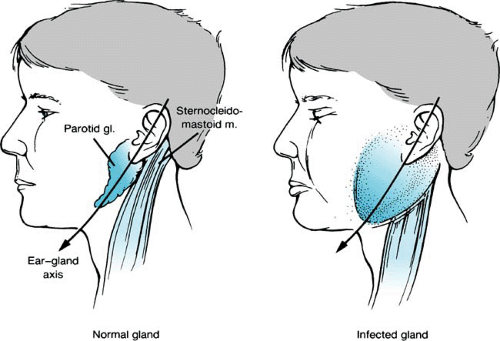
mumps
acute self-limited parotitis
transmitted by large respiratory droplets
complications include gastritis, meningoencephalitis, orchitis, mastitis, and oophoritis
death 1-3.4/10,000 (much smaller)
mumps immunization
live attenuated viral vaccine
administered with measles and rubella (MMR)
combination of measles, mumps, rubella, and varicella available
recommended for 12-15 months olds, susceptible adolescents and adults
can consider immune if born before 1957
two doses for school aged children and high risk adults
healthcare workers
international travelers
students at post-high school educational institutions
third dose recommended for outbreak response
rubella
mild exanthematous (rash) viral infection
transmitted via respiratory route
congenital rubella syndrome if infection during pregnancy
deafness, cataracts, heart defects, intellectual disabilities, liver and spleen damage, low birth weight
rubella elimination
rubella and congenital rubella syndrome eliminated from Western Hemisphere
immunization continues to be required because threat of transportation
rubella immunization
live attenuated viral vaccine
administered with measles and mumps (MMR) or varicella (MMRV)
recommended for 12-15 months, susceptible adolescents and adults
rubella vaccine cautions
do not immunize pregnant individuals
no evidence for congenital rubella syndrome from vaccine
avoid pregnancy for 28 days
routine pregnancy screening not recommended
don’t need a pregnancy test
vaccinations of adults who may become pregnant for rubella
vaccination of susceptible people of childbearing age
routine general medical and gynecologic outpatient care
all family planning settings
before discharge from hospital, birthing center, or other medical facility
prenatal assessment and post partum immunization
will be screened for rubella immunity
pregnant people should not get live vaccines
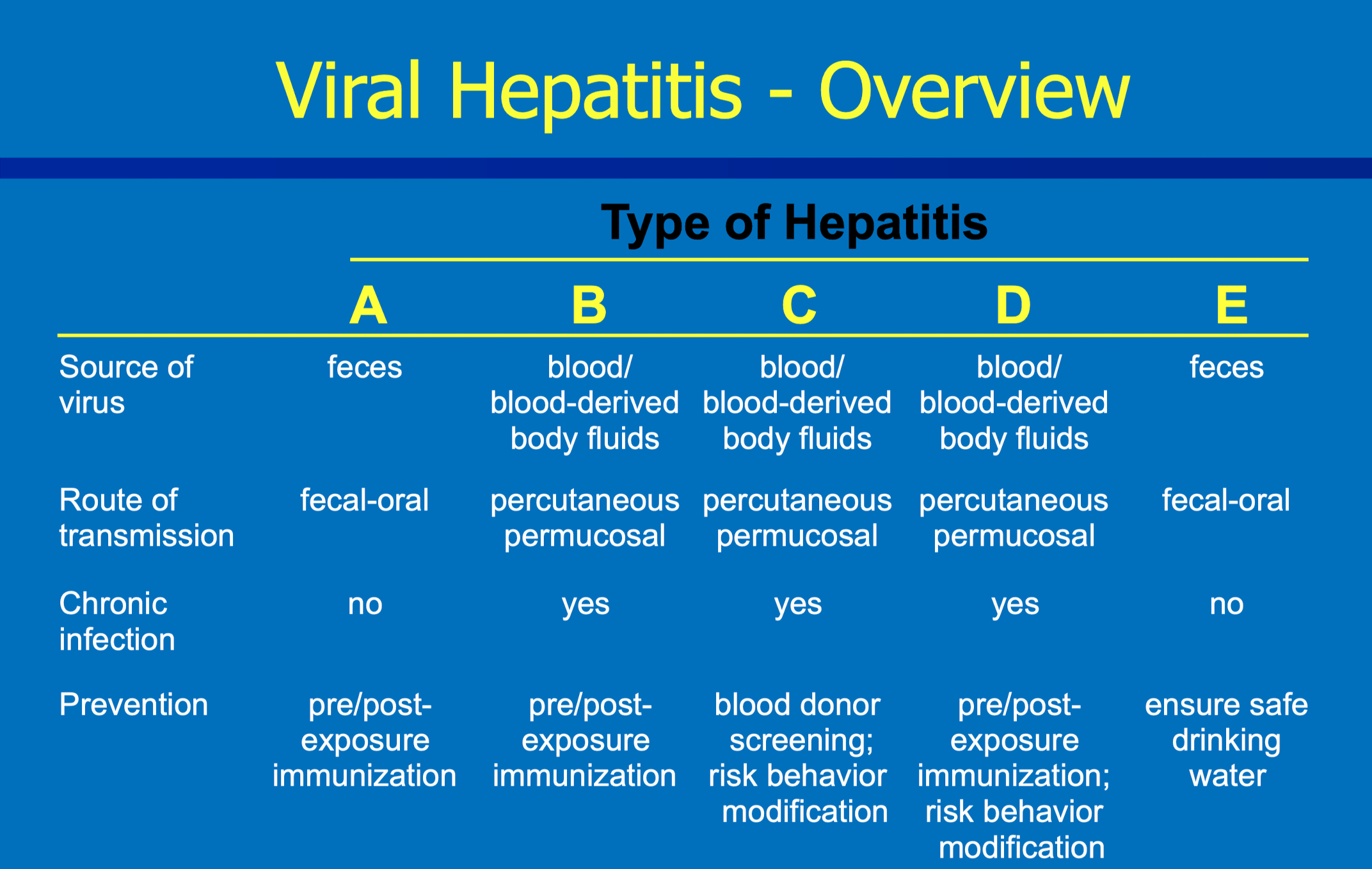
Viral hepatitis - overview
Hepatitis A infection
viral disease caused by hepA virus
transmitted by fecal-oral route
immune mediated liver injury
relatively mild illness in children
more serious illness in adults
elevated LFT (live function test)
jaundice
rare fulminant hepatitis (makes you so sick you end up in ICU)
no chronic carrier state
no specific treatment; supportive care
Hepatitis A outbreak
as of 2023 61% of people had hospitilizations
this is really high
if you get it as a child you may be asymptomatic and won’t be as sick
Hepatitis A Vaccine Indications
travelers to countries with high or intermediate endemicity
men who have sex with men
people who use drugs
persons with occupational risk
perons with chronic liver disease
if they do get it, their liver may fail
experiencing unstable housing or homelessness aged 1 and older
currently or recently incarcerated
all children 12 months of age and catch up for unimmunized 18 years and younger
Haemophilus influenzae type b
small gram negative organism causing infections ranging from colonization to meningitis
meningitis has 10% mortality rate and 40% have neurological deficits
Haemophilus influenzae type b vaccine
conjugate vaccines
recommended at 2,4, (6), and 12-15 months of age
recommended for those >5 years if immunocompromised
sickle cell, splenectomy, HSCT (hematopoietic stem cell transplantation)
hepatitis b virus
affects liver
viral disease caused by hepb virus
transmitted by parenteral routes (injected/not oral)
blood transfusion
sharing of needels
sexual contact
mother to neonate
must have chronic infection at the time of pregnancy
hepatitis b infection in US
the groups from 0-19 and 20-29 are very low numbers for infections since they were immunized as babies
similarly, ages 60+ have a low rise
reported risks for hepatitis B infections
injection drug use most commonly reported rise
note that no risk identified/reported in about 2/3 of cases
hepatitis b immunization of adults
routine immunizations for all adults aged <60 years
doesn’t work great for people older than 60 since they don’t respond well
routine immunization of infants since 1991
routing immunization of adolescents since 1997
not a huge ordeal since many people are immunized
hepB vaccines
recombinant hepatitis b surface angtigen with aluminum adjuvant
energix (pediatric or adult)
recombivax (pediatric or adult)
both require 3 doses for immunity: 0, 1, and 6 months
recombinant hepatitis b surface antigen with CpG 1018 adjuvant
cool new adjuvant
heplisav-b (ages 18 and older)
two doses separated by one month
recombinant vaccine with multiple surface antigens with aluminum adjuvant
prehevbrio (ages 18 and older)
three dose series: 0, 1, and 6 months
post vaccination testing for hepb
post vaccine antibody testing in healthcare workers at risk for sharp injury
measure antiHBs (antibody to hepatitis B surface antigen)
antiHBS > 10 mlUml protective
100% effective in those who develop an antibody response
older individuals (age >40 years), chronic conditions, immunosuppression at risk for nonresponse
repeat series
choose hepB with CPG
heplisav b or prehevbrio
polio
acute viral illness which in its serious form affects the central nervous system
fecal-oral transmission
complications include flaccid paralysis
death rate as high as 10%
polio vaccines
live attenuated vaccine - no longer used (hasn’t been for 23 years)
OPV (stockpile with CDC for public health emergency)
enhanced-potency inactivated vaccine
IPV
No wild type polio cases in the western hemisphere since 1991
Vaccine associated poliomyelitis occurs in approximately 1 in 2.4 million doses
become infectious after receiving the vaccine
polio case in NY
unvaccinated young adult developed symptoms in June 2022
caused by VDPV2
vaccine deprived
wastewater monitoring shows vaccine virus present in April 2022
low immunization rates in Rockland County
high vaccine coverage rates absolutely needed
polio vaccine scheduling
polio vaccine recommended at 2, 4, 6-18 months and again at 4-6 years
any immunized adult; however if person received any childhood vaccines, almost certainly vaccinated for polio
varicella
highly contagious disease due to varicella zoster virus
spread by directed contact or the respiratory route
characteristic pruritic vesicular rash with fever
complications include bacterial infection of lesion, pneumonia, encephalitis, and cellulitis
varicella epidemiology
children
3.5 to 4 million cases each year
generally mild disease with rare complications
adults
5% of all cases occur in those >15 years
complications much more common
varicella vaccine
varivax licensed april 1995
a live attenuated viral vaccine
contraindicated in these situations:
immunosuppression
pregnancy
receipt of blood products - dose dependent
active and untreated TB
evidence of varicella immunity
born in US before 1980
physician documented clinical history of chicken pox or zoster
laboratory evidence of immunity
two doses of varicella vaccine after first birthday separated by at least 4 weeks
evidence of varicella immunity for healthcare worker
physician documented clinical history of chicken pox or zoster
laboratory evidence of immunity
two doses of varicella vaccine after first birthday separated by at least 4 weeks
*birth before 1980 doesn’t count*
varicella vaccine indications
all infants at age 12 months with second dose prior to entering school
minimum 3 month interval between doses
second dose recommended for anyone who has received only one dose
when first licensed, it was only one dose
children entering child care facilities or schools (or evidence of immunity)
assume immune in US before 1980 unless healthcare worker, pregnant woman, or immunocompromised
varicella vaccine indications
routine immunization of all adolescents and adults without evidence of immunity
prenatal assessment + postpartum immunization
varicella vaccine adverse effects
fever
rash
at injection site: median number of lesions = 2
generalized: median number of lesions = 5
rotavirus infection
half million childhood deaths worldwide
serious infection
one third of hospitalizations for diarrhea
w/o immunization
incidence similar in developing AND developed countries
rotavirus vaccines
live oral vaccine stores refrigerated
two preparations
rotateq (merck)
pentavalent bovine reassortment viruses
must be reconstituted with supplied diluent
three oral doses
rotarix (GSK)
attenuated human rotavirus
liquid preparation
two oral doses
recommended at 2, 4, and (6 if merck used) months
vaccine schedule for rotavirus
first dose between 6 and 14 weeks of age
if inadvertently started, complete series
second and third doses spaced by 4 to 10 weeks
series must be completed by 8 months of age
DON’T FINISH IF IT’S PAST EIGHT MONTHS
initiate or complete series for infant who have had rotavirus infection
RV and intussusception
with the old vaccine there was an increase in intussusception (bowel obstruction)
pain, inflammation, sometime surgery needed
no evidence that risk is different between vaccines
about 45-213 cases per birth cohort
prevents 53,000 hospitalizations and 170,000 ED visits per birth cohort
risk is worth the benefit
RV vaccine impact
dramatic reductions in disease
decreased hospitalization by 42-63%
decreased lost workdays by 87%
tetanus diptheria pertussis abbreviation
upper case means higher doses
bigger dose for smaller people
pertussis
whooping cough
bacterial respiratory infection caused by bordetella pertussis
direct transmission from close contact
major manifestation is severe paroxysms of cough
severe complications include pneumonia, encephalopathy, malnutrition
pertussis vaccine
administered in combination with diptheria and tetanus
recommended at 2, 4, 6, and 15-18 months with boosters at 4-6 years
routine Tdap for 11-12 years
use for 7-10 year olds with incomplete childhood series
Tdap for next dose of adults
pertussis vaccine scheduling
adacel license for booster after 8 years
Td or Tdap can be administered every 10 years
late 2nd or 3rd trimester of each pregnancy
transfer immunity to baby
vaccine products for TDAP
DTaP for children <7 years
several brands and combinations
pertussis antigens and doses included in the vaccine vary among manufacturers
Tdap
Adacel (sanofi-pasteur)
Boostrix (GSK)
ACIP recommended use in under-immunized 7-10 year olds and no upper age limit
cocooning
strategy from protecting very young infants from pertussis
Tdap recommended for pregnant females in late 2nd or 3rd trimester
immunization of parents, siblings, grandparents, out of state home care providers
Tdap immunization at hospital discharge for mother
Key role for pharmacy based immunization services
diptheria
Bacterial infection caused by Corynebacterium diphtheriae
Person to person transmission through direct contact
Must be pretty close
Major manifestation is membranous inflammation of respiratory tract
May damage myocardium, nervous system, and kidney
diptheria vaccine
Toxoid, adsorbed inducing immunity to the bacterial exotoxin
Administered in combination with tetanus and pertussis
Recommended at 2, 4, 6, 16-18 months and at 4-6 years
Routine boosters (Td or Tdap) every 10 years
tetanus
All muscles are in contracted state
Acquired through environmental exposure
Mediated via bacterial toxin
Not contagious
Get from environment
Worse for diabetics since they can get bad wounds
Clinical presentation / clinical syndroms tetanus
Clinical syndromes
Localized: painful contractions, generally mild
Generalized: spasm of facial muscles, hyperreflexia, opisthotonos, tonic tetanic seizure-like activity
Cephalic: atonic cranial nerve palsies, may progress to generalized
Muscle constraints so strong you may break bones
Tetanus vaccine
Toxid, adsorbed from Clostridium tetani
Administered in combination with diphtheria and pertussis
Recommended at 2, 4, 6, and 15-18 months and 4-6 years
Routine boosters (Td or Tdap) every 10 years
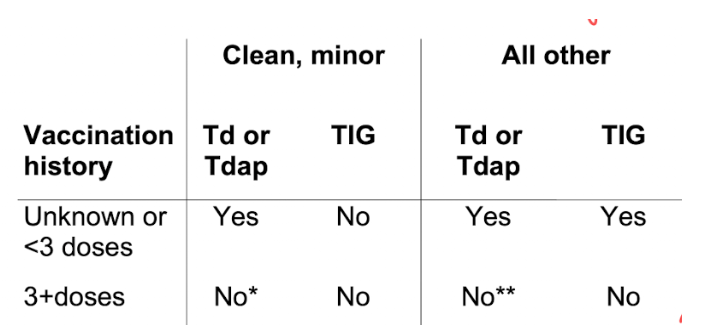
Wound management
If wound and its been >5 years immunize
If wound and it’s been <5 years no need to immunize
pneumococcal disease
Infection caused by the bacteria Streptococcus pneumonia
Otitis media
20 million office visits (28-55% strep)
Pneumonia
175,000 cases annually
Meningitis
Leading cause 3,000-6,000 cases annually
Bacteremia
50,000 cases annually
invasive pneumococcal disease
Defined as S. pneumoniae in normally sterile body site
Incidence >65 years 24 cases/100,000 population
Pneumococcal pneumonia
<age 65 years: 126-422 per 100,000
> 65 years: 847-3365 per 100,000
Much larger
pneumococcal vaccines
Pneumococcal conjugate 15 valent (vaxneuvance)
Pneumococcal conjugate 20 valent (prevnar 20)
Pneumococcal polysaccharide 23 valent (pneumovax23)
When we vaccinate kids we see way decrease because herd immunity
PCV15 or PCV20 recommendations for children
Universal immunization for infants
2, 4, 6, and 12-15 month schedule
Immunocompromised children aged 6-18 years
Single dose of PCV15 or PCV20 if no history of previous conjugate vaccine
If at least one PCV20, no additional doses
If PCV13 or PCV15 administer either PCV20 or PPSV23
So must have 20 at some point
pneumococcal vaccines for immunosupressed
Congenital or acquired immunodeficiency
HIV
Chronic renal failure
Nephrotic syndrome
Leukemia
Lymphoma
Hodgkin disease
Generalized malignancy
Iatrogenic immunosuppression
Solid organ transplant
Multiple myeloma
other conditions that are indications
Chronic heart disease (REAL not hypertension)
Chronic lung disease (asthma >19)
Diabetes
Cerebrospinal fluid leak
Cochlear implant
Sickle cell disease other hemoglobinopathy
Alcoholism
Cigarette smoking (>19 year)
All adults aged 65 years and older
for those aged 65 and older
PCV20 or PCV15 + PPSV23 later (PCV20 can be substituted for PPSV23)
If adults received PCV13 and/or PPSV23 prior, PCV20 may be considered
for those 19-64 years old
PCV15 or PCV20
If PCV15 used this should be followed up with PPSV23
Chronic conditions, immunocompromised
patient has PCV13 history
Used for adults who were immunocompromised
Used by shared clinical decision making for those aged 65 years and older who were NOT immunocompromised
Followed by PPSV23
Additional dose of conjugate vaccine not routinely recommended
Healthcare professionals may recommend PCV20 for those 65+ years of age who were previous immunized (PCV13 +- PPSV23)
Pneumococcal polysaccharide vaccine (PPSV23)
Vaccine composition
Capsular polysaccharide inducing type-specific antibodies
Used for those who receive PCV15
Immunocompromised: 8 weeks after PCV15
Chronic conditions: >1 year after PCV15
Aged 65 years and older: >1 year after PCV15
65+ years who received PPSV23 only, PCV15 or PCV20 recommended >1 year later
Using ACIP pneumococcal vaccine recommendations
Infants and immunocompromised children straightforward
Adults
Use the table posted on canvas
Do the problems posted on canvas
Human papillomavirus infection
Most common sexually transmitted infection
Highest rates among sexually active young adults
Nearly everyone will get HPV at some point
Spread through intimate skin to skin contact
Infection often asymptomatic; clincial pathology diagnosed by Pap test
Screening tests not available for other cancers caused by HPV
HPV infection
Oncogenic viruses associated with cervical, vulvar, vaginal, anal, oropharyngeal, penile cancer
Types 6 and 11 are associated with anogenital warts and respiratory papillomatosis (wart like growth on vocal cords)
Besides cervical we don’t have screening
Low HPV immunizations
Very low numbers although Tdap and meningitis are much higher
They should be given at the same time
HPV vaccine
9vHPV containing VLP 6, 11, 16, 18, 31, 33, 45, 52, 58
If age 9-14 years, two doses 0, 6-12 months
i f age 15-26 years, three doses 0, 1-2, 6 months
Recently expanded licensure for 27-45 years old
ACIP HPV vaccine recommendations
Recommended for all adolescents aged 11-12 years
Also recommended for all aged 13-26 years
Immunization prior to sexual debut preferred
Can initiate series in individuals as young as 9 years if clinician deems appropriate
HPV vaccine for 27-45 year olds
Acip recommended vaccine for use in 27-45 years by shared clinical decision making
New partner, immunosuppression
HPV vaccine limitations
Duration of protection unknown, but more than a decade of follow-up shows little indication of waning
No change in recommendations for pap test frequency
opportunities for pharmacists and HPV
Unacceptably low rates of series completion
Partner with clinic
Series initiated at annual visits
Finish series at pharmacies
Communication
Between clinicians
Personal immunization record
Immunization registry
Meningococcal disease
Five major serogroups A, B, C, Y, and W - 135
Transmission via direct contact with respiratory secretions of a nasopharyngeal carrier
Most common cause of bacterial meningitis in individuals 2-18 years
Mortality rates 10-13%
10% of survivors with severe morbidity
Mental retardation
Hearing loss
Loss of limbs
Meningococcal vaccines
Meningococcal conjugate vaccine covering serogroups A, C, Y, and W-135
Repeat doses for high risk
License for use in individuals aged 9 months to 55 years (Menactra) and 2 months - 55 years (menveo)
Recommended for routine use in 11-12 year olds and repeat dose at age 16
Meningococcal vaccine also recommended for
Individuals with complement deficiency or receiving complement inhibitor
Eculizumab or ravulizumab
Those with HIV infection
Individuals with asplenia
Travelers to endemic areas
Microbiologists with occupational exposure
Those who live in residence halls or military recruits if incompletely immunized
Revaccination with MenACWY
Revaccinate individuals at prolonged risk of invasive disease
Complement deficiencies
Anatomic or functional splenectomy
Prolong exposure (microbiologist, travelers, resident of epidemic areas)
Revaccination schedule for meningococcal ACWY
Revaccinate adolescent at 16 years of age
Revaccinate after 5 years if age >7 years
Revaccinate after 3 years of age 2-6 years
Continue to revaccinate at 5 year intervals if remain in high risk group
Meningococcal immunization for infants
MeACWY recommended for infants at high risk of invasive meningococcal disease
Four dose series in infant immunization schedule
Use age-appropriate vaccine product
Meningococcal serogroup B vaccine
Trumenba: recombinant serogroup B fHBP protein
H binding protein
Induces complement dependent antibody responses
2 dose series at 0 and 6 months for 16-23 year olds under shared clinical decision-making
3 dose series 0, 2, 6 months for high risk and outbreaks
Bexsero: multicomponent; recombinant
Big increases in antibody concentrations
2 dose series at least one month apart for 10-25 year olds
ACIP recommendations for meningococcal b
Either vaccine for individuals at high risk for invasive meningococcal disease starting at age 10 years
No upper age limit
Complement deficiency or inhibitor
Asplenia
Microbiologists with occupational exposure
Either vaccine may be used in an outbreak
16-23 year olds may be vaccinated to provide short-term production
Influenza
Acute febrile illness caused by varying strains of influenza virus
Transmitted by respiratory droplets
Rarely by contact with contaminated objects
characterized by headache, fever, myalgia, dry cough, pharyngitis
Complications due to secondary bacterial infection or involvement of the myocardium or central nervous system
It can be the tipping point for chronic conditions
Super onset (know exactly when it happened)
influenza vaccine
Influenza viruses representing circulating viral strains
All vaccines are quadrivalent (2A strains and 2B strains)
Vaccine formulation strategies
Grown in eggs
Live (flumist) (LAIV4)
Inactivated split or subunit (various)
Everything else is eggs
Grown in MDCK cells (Flucelvax) (ccIIV4)
Mammalian cells
Recombinant DNA grown in transfected insect cells (Flublok) (RIV)
Contains strains that experts think will arise)
influenza vaccine preparations abbreviations
IIV4: quadrivalent inactivated influenza vaccine
LAIV4: quadrivalent live attenuated influenza vaccine
Nasal spray
ccIIV4: quadrivalent cell culture based inactivated influenza vaccine
RIV4: quadrivalent recombinant influenza vaccine
enhanced influenza vaccines
High dose
4x more antigen
Adjuvantated
Makes vaccine work better
Recombinant
RIV4
No standard definition of enhanced influenza vaccine
Preferentially recommended for those aged >65 years
high dose inactivated influenza vaccine
Licensed for individuals >65 years of age
More antigen than regular influenza vaccine
60 mcg HA vs. 15 mcg HA
Vaccine volume is 0.7 mL (higher)
Higher antibody concentrations
Clinical trials endpoint higher Ab titers to two vaccine viruses
Higher antibody responses in nursing home residents
Higher rate of injection side reactions
More antigen duh
Not really a deferent for people
Older people make poorer responses to vaccines and they are at higher risk for complications from influenza