Lecture 5: continuing regulation of pH, regulation of blood Ca2+ levels, renal failure
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
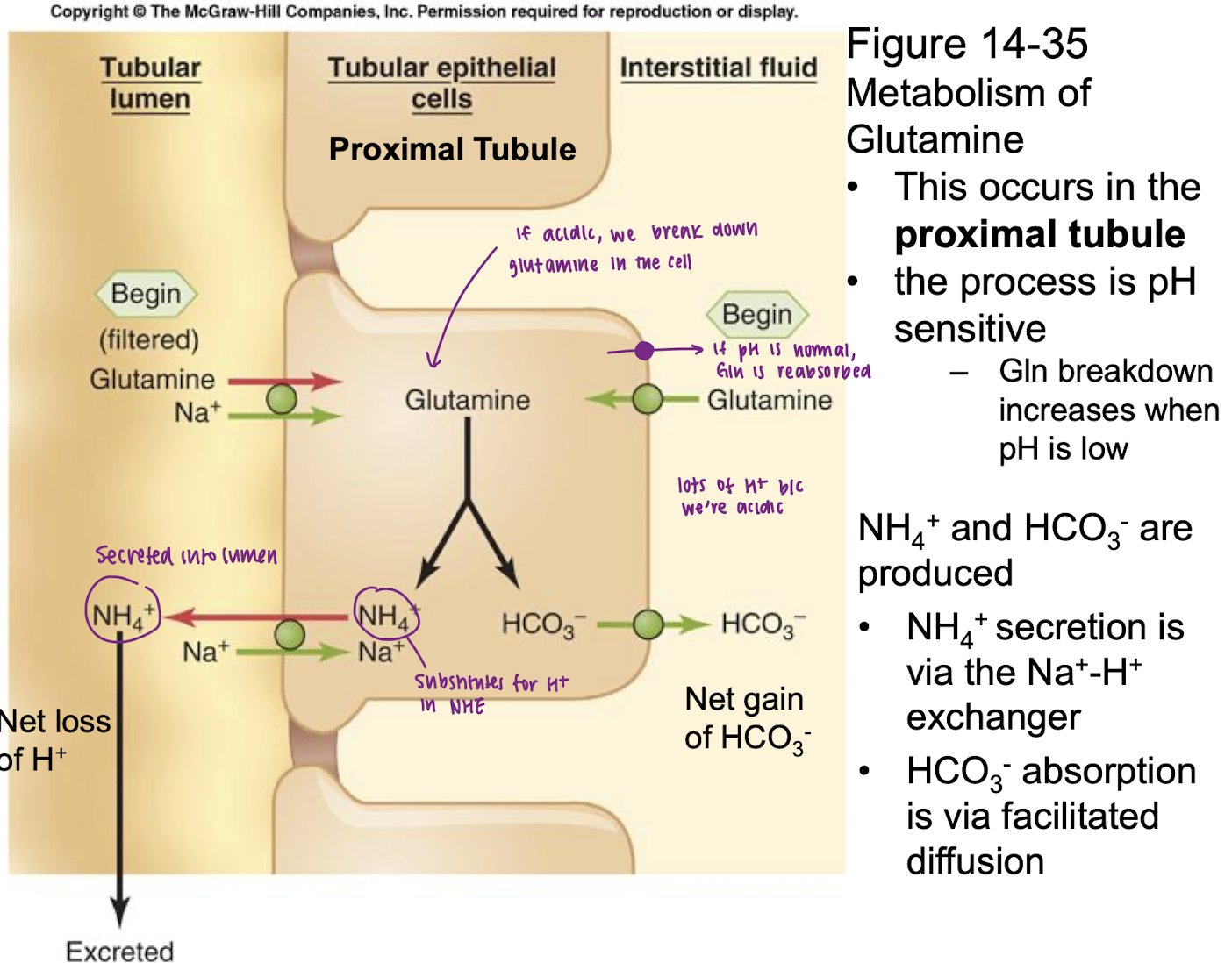
explain mechanism of adding new HCO3- in proximal tubule
glutamine enters proximal tubule via apical membrane via facilitated diffusion or secondary Na+ active transporter on basolateral membrane
glutamine breaks down into NH4+ and HCO3-
(1) HCO3- absorbed (2) NH4+ secreted via Na/H exchanger and excreted
Result is net gain of HCO3- and net loss of H+
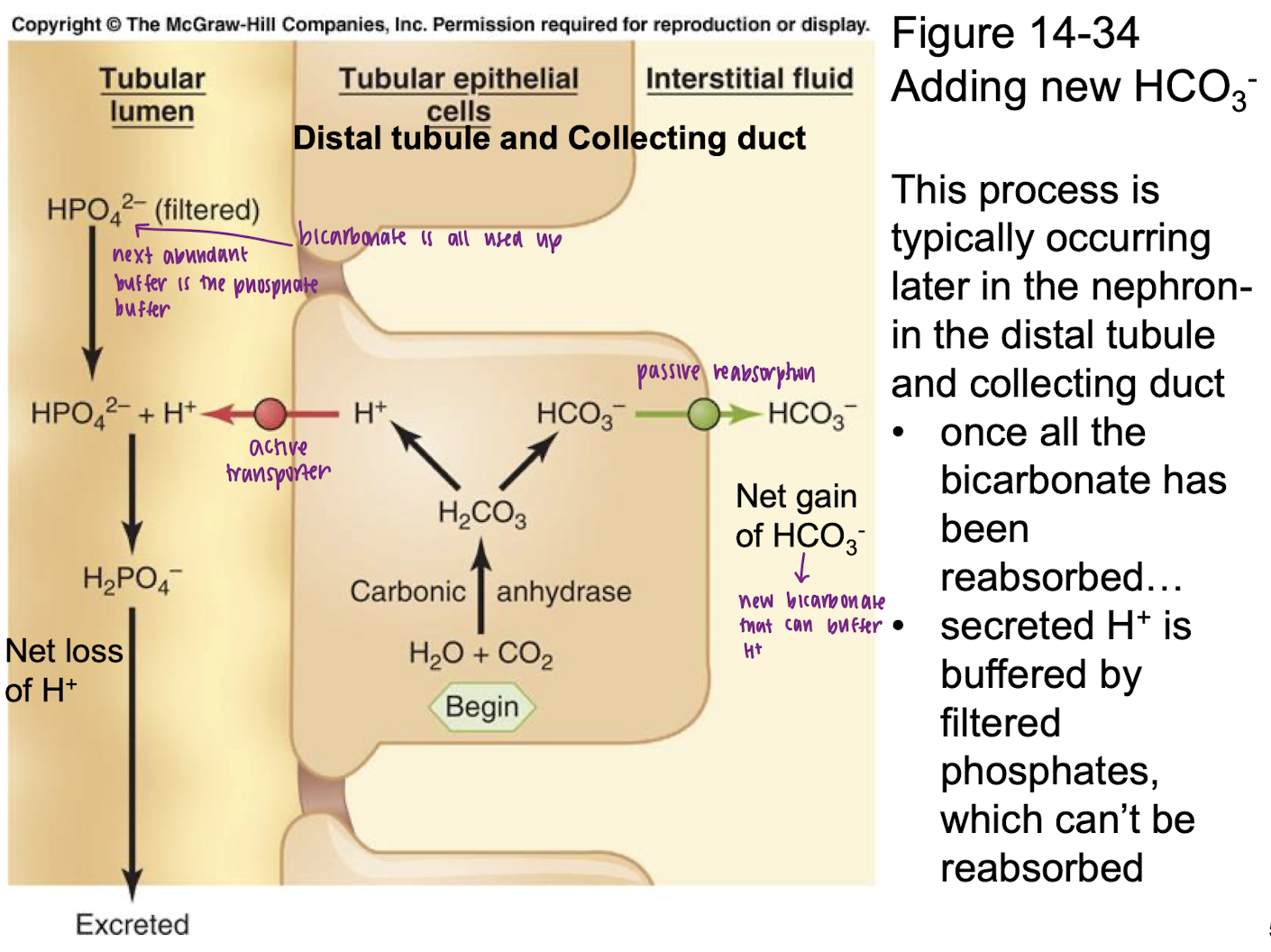
explain mechanism of adding new HCO3- in distal tubule and collecting dut
H2O + CO2
carbonic anhydrase
H2CO3 splits into HCO3- and H+
HCO3- passively absorbed into ISF (net gain of HCO3-); H+ actively transported into tubular lumen
H+ + HPO4 (filtered) → H2PO4 excreted
Once all the bicarbonate has been reabsorbed, secreted H+ is buffered by filtered phosphates, which can’t be reabsorbed
P cell (what gets secreted and absorbed?)
Na+ and H2O reabsorbed, K+ secreted
alpha intercalated cell (what gets secreted and absorbed?)
HCO3- absorbed, H+ secreted
active most of the time b/c we’re usually under an acid loud
beta intercalated cell (what gets secreted and absorbed?)
H+ absorbed, HCO3- secreted
only active if we are alkalotic
kidneys adjust pH by
altering absorption or secretion of HCO3- (plasma [HCO3-])
effect of adding lactic acid to the blood on pH, H+, HCO3-, Pco2
pH decreases
H+ increases
HCo3- decreases
Pco2 no change
effect of adding Hco3 to the blood on pH, H+, HCO3-, Pco2
pH increases
H+ decreases
Hco3 increases
Pco2 no change
effect of hypoventilation on pH, H+, HCO3-, Pco2
pH decreases
H+ increases
Hco3 no change
Pco2 increases
effect of hyperventilation on pH, H+, HCO3-, Pco2
pH increases
H+ decreases
Hco3 no change
Pco2 decreases
respiratory acidosis
primary defect
how do kidneys respond
compensatory response
primary defect: increased Pco2
alpha intercalated cells secrete H+ and reabsorb HCO3-
compensation occurs via renal responses and will result in increased HCO3- in blood level and pH that is increased toward normal
metabolic alkalosis
primary defect
what receptors sense the change and what is the respiratory response
how does respiratory response affect pH?
primary defect: decreased H+ (or increased Hco3-)
sensed by peripheral chemoreceptors and causes decreased ventilation
respiratory response → decreased pH
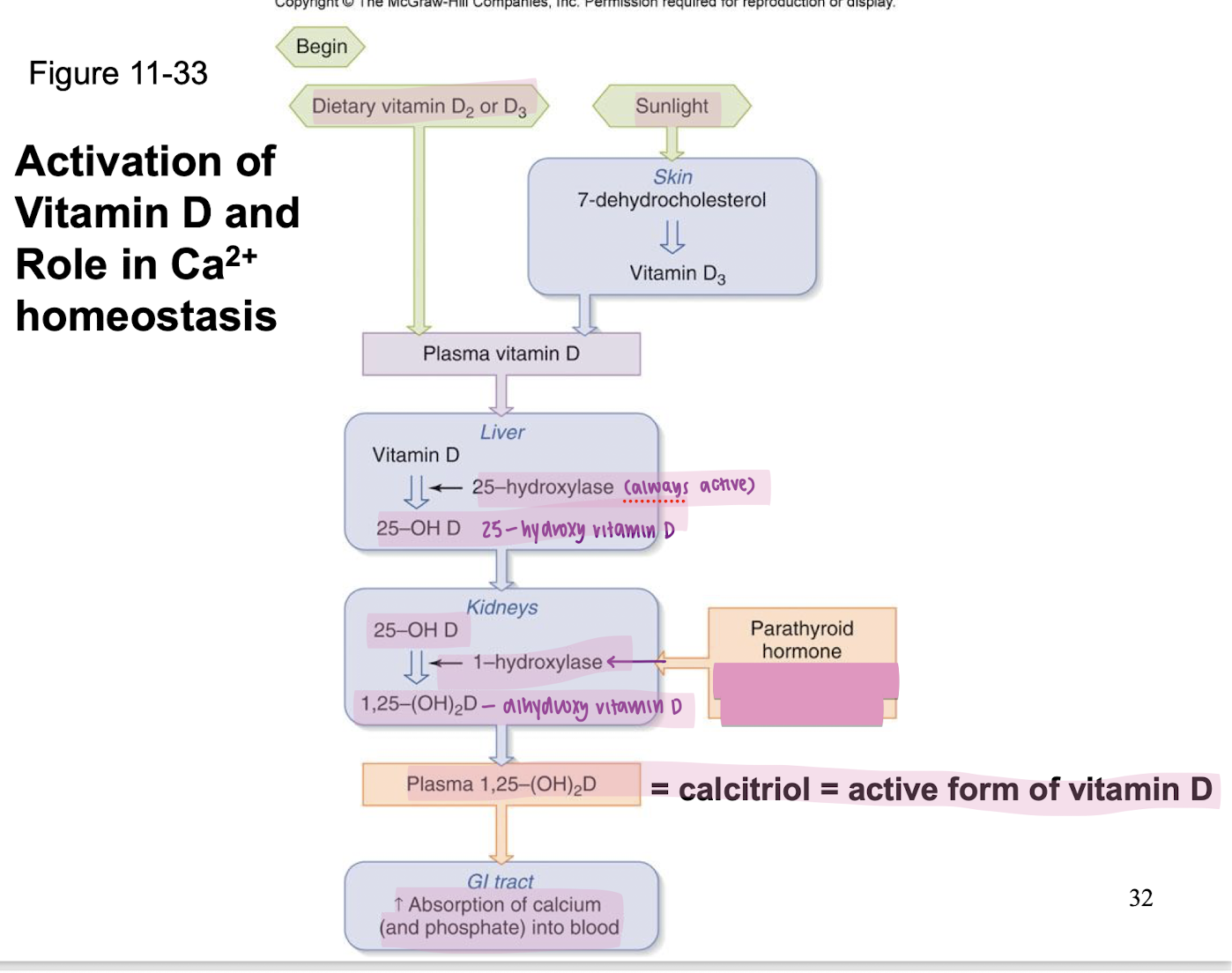
PTH
released by the parathyroid glands in response to decreased plasma Ca2+
PTH stimulates (3 things)
increased bone breakdown
formation of calcitrol (active form of vitamin D3) by the kidney
increased Ca2+ reabsorption by the kidney
calcitrol
active form of vitamin D3; stimulates Ca2+ (and phosphate) absorption by the intestine
PTH inhibits
phosphate reabsorption by the kidney → increased urinary excretion of phosphate
fill this out
if PTH induces bone resorption thus increased plasma Ca2+ and PO4, then why does PTH decrease PO4 reabsoprtion?
because PTH also stimulates PO4 absorption by the intestine
and high plasma PO4 promotes Ca2+ deposition in bone
so decreasing PO4 absorption by kidney blunts the increase in plasma PO4 and helps keep the released Ca2+ in the plasma compartment rather than driving it to be deposited back into bone
erythropoietin
released by the kidney in response to decrease O2 delivery to kidney and stimulates production of RBC and increases blood Hb concentration
chronic renal failure
a progressive disease process consisting of loss of filtration (decreased GFR)
effect of chronic renal failure on plasma K+
hyperkalemia: K+ secretion/excretion is impaired
effect of chronic renal failure on arterial pH
acidosis: HCo3- reabsorption/addition is impaired
effect of chronic renal failure on hematocrit
anemia: low RBC, due to decreased erythropoietin secretion
effect of chronic renal failure on waste excretion? plasma [waste products]?
wastes are not removed so waste products increase in blood (plasma urea and creatinine levels go up, for example)
effect of chronic renal failure on bone density
decreases due to increased bone breakdown
decreased ability to reabsorb filtered Ca2+ AND decreased calcitriol activation (so decreased Ca2+ absorbed from GI tract) → decreased plasma Ca2+ → increased PTH → increased bone breakdown
effect of chronic renal failure on urinary excretion of protein
protein appears in urine
glomerular filtration barrier breaks down and proteins are filtered and excreted
effect of chronic renal failure on blood pressure
Na intake must be monitored. If increased intake, increase volume and BP (and vice versa)
increased renin secretion from damaged nephrons due to low GFR → increase Ang II and TPR → increase BP
effect of chronic renal failure on plasma osmolarity
ability to dilute and concentrate urine is diminished. therefore, ability to excrete or retain water is diminished.
if increase water intake, can decrease osmolarity (and vice versa)
calcitonin
stimulated by increased plasma Ca2+
reduces bone breakdown or stimulates bone formatiob
decreases renal absorption of Ca2+ and phosphate.