LAB: ROOT CANAL ANATOMY
1/36
Earn XP
Description and Tags
from lab manual
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
parts of the root canal system
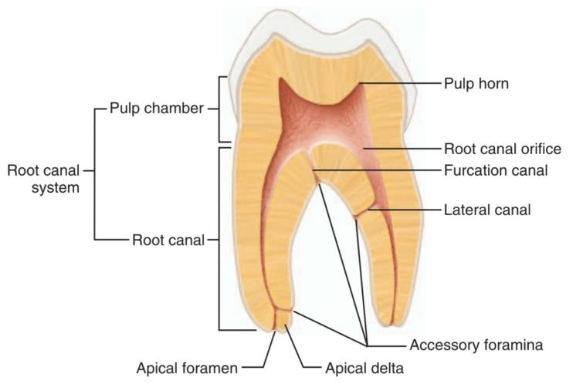
canal bifurcation
(splitting into two canals)
indicates when a root canal disappears or becomes indistinct partway down the root
apical constriction
the narrowest part of the canal
→ root canal gradually narrows as it approaches the apex
1.0 – 1.5 mm from the root apex
diameter of apical constriction
shape of the narrowest area
round
oval
serrated
apical foramen
often exits at an angle to the main canal
is not usually in a straight line with the main canal
forms after the narrowest point which widens again
0-3 mm from the root apex
diameter where apical foramen is located
Frank Weine (1982)
he classified the basic classification of root canal morphology
Type 1
Single canal from pulp chamber to apex
1

Type 2
(2-1)
Two separate canals leaving the pulp chamber but merging short of the apex to form only one canal
type 3
(2)
two separate canals leaving the pulp chamber and exiting from the root in separate apical foramina
Type 4
(1-2)
one canal leaving the pulp chamber but dividing short of the apex into two separate canals with separate apical foramina

lateral canals
present in about 50% of permanent teeth
branch off from the main root canal at right angles
can be:
blind-ending sacs
or open channels that reach the root surface (most common)
can occur:
anywhere along the root
size varies:
from very small (microns)
sometimes as large as the main canal
relevance of lateral canals in endodontics
act as communication pathways between:
main canal (inside the tooth)
periodontal tissues (around the tooth)
this means:
pulp infection → periodontal damage
periodontal disease → pulp irritation or infection
irritation or secondary dentin formation
causes the root canal system to gradually reduce in size
factors that hasten the process::
caries (tooth decay)
trauma
excessive wear
dental procedures (preoperative work)
younger patients → larger access cavities
older patients → smaller access cavities needed due to narrower canals
canal obliteration process
canals never fully sclerose (block completely)
hard tissue deposition occurs:
first fills the pulp chamber
then moves into the coronal part of the canal
changes in pulp tissue
becomes more fibrous
less vascular (reduced blood supply)
in some cases, pulp dies
apical portion of the canal often remains open (patent)
Vertucci
he classified the complex of root canal morphology
Vertucci’s Classification Type I
(1-1)
A single canal extends from pulp chamber to apex

Vertucci’s Classification Type II
(2-1)
Two separate canals leave the pulp chamber and join short of the apex to form one canal

Vertucci’s classification type III
(1-2-1)
one canal leaves the pulp chamber and divides into two in the root: the two then merge to exit as single canal

Vertucci’s Classification Type IV
(2-2)
Two separate, distinct canals extend from the pulp chamber to apex

Vertucci’s Classification Type V
(1-2)
one canal leaves the pulp chamber and divides short of apex into two separate, distinct canals with separate apical foramina

Vertucci’s Classification Type VI
(2-1-2)
two separate canals leave the pulp chamber; merge in body of the root, and redivide short of the apex and exits as two distinct canals

Vertucci’s Classification Type VII
(1-2-1-2)
one canal leaves the pulp chamber; divides and then rejoins in the body of the root, and finally divides into two distinct canals short of the apex

Vertucci’s Classification Type VIII
(3-3)
three separate distinct canals extend from the pulp chamber to apex

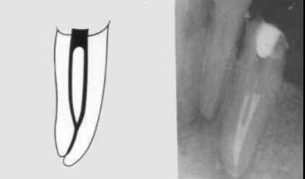
canal anatomy of mx incisors
inclination: labial
root shape:
central: usually straight [fig. 7]
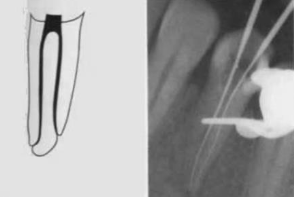
lateral: often has a distal curve at apex [fig. 8]
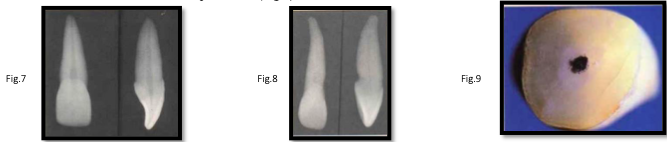
canal cross-section:
oval in coronal and middle thirds
becomes round in apical third
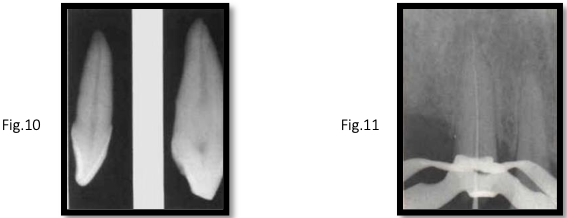
canal anatomy of mx canine
apical portion may be thin → only small instruments can be used to avoid perforation
inclination: Labial [fig. 10]
root shape: Straight or slightly distal curve near apex
canal shape:
middle third: broad labio-palatal (forms a bulge)
apical third: round [fig. 11]
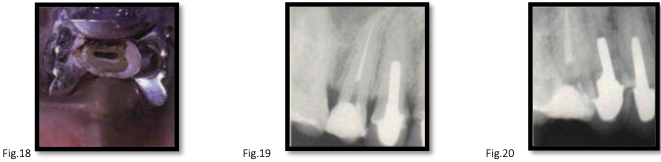
canal anatomy of mx 1st premolar
roots:
62% have 2 roots
38% have 1 root
rarely, 3 roots
canals:
majority (85%) have 2 canals
pulp chamber floor extends into roots, wide bucco-palatal
special cases:
3-rooted premolars are hard to detect radiographically
can have 3 canal orifices: 2 buccal, 1 palatal
canal anatomy of mx 2nd premolar
roots: usually 1
2 roots in 15%
canals:
usually 1, broad bucco-palatal
2 canals occur in 25%
note: buccopalatal extent may be visible only in oblique radiographs
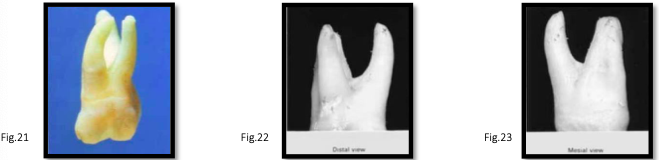
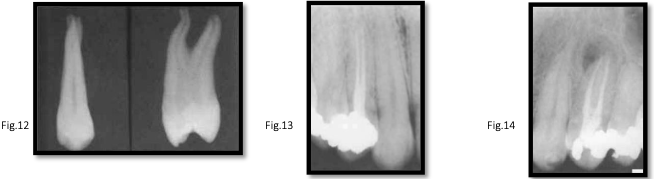
canal anatomy of mx 1st molar
roots: 3 (2 buccal, 1 palatal)
distobuccal root: straight, round cross-section
mesiobuccal root:
curved distally, broad bucco-lingual
usually has a groove mesially and distally
2 canals in 60% of cases
if only one canal → broad bucco-lingual, narrow mesio-distal
main mesiobuccal canal → larger, buccally positioned
palatal root:
curves buccally, oval mesio-distally
opens under mesiopalatal cusp

canal anatomy of mx 2nd molar
similar to first molar
pulp chamber: flattened mesio-distally (reflects crown shape)
mesiobuccal root: lower incidence of second canal than first molar
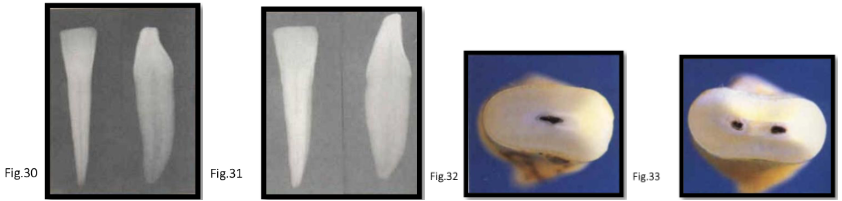
canal anatomy of mn incisors
canals:
40% have 2 canals
configurations:
type 1 → 60% [fig. 30]
type 2 → 35% [fig. 31]
type 3 → 5%
shape:
single canal: broad bucco-lingually, narrow mesio-distally [fig. 32-33]
2 canals: rounder in cross-section
ovoid throughout root length [fig. 35]
root features:
shallow vertical grooves on mesial and distal surfaces
narrow root width → higher risk of lateral perforation during enlargement
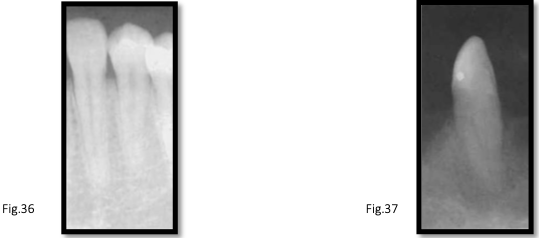
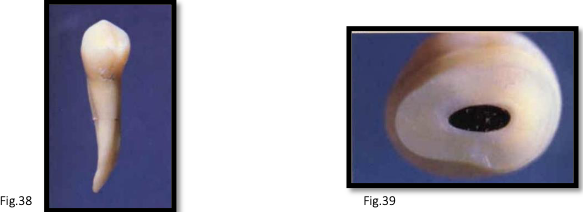
canal anatomy of mn canines
roots: usually 1; rarely 2 [fig. 36]
canal configurations: type 1, 2, or 3
length: longest mandibular tooth, variable length
canals: 2 canals in 18% of cases [fig. 37]
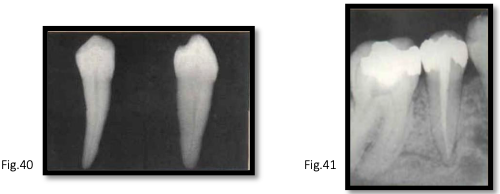
canal anatomy of mn 1st premolar
canals:
usually 1
2 canals in 27% of cases, rarely 3
when two canals present → lingual canal is second
shape: wide bucco-lingually
configuration: mainly type 4
canal anatomy of mn 2nd premolar
high incidence of lateral canals
canals:
usually 1 (type 1 most common)
wide bucco-lingually
apical portion often curves distally
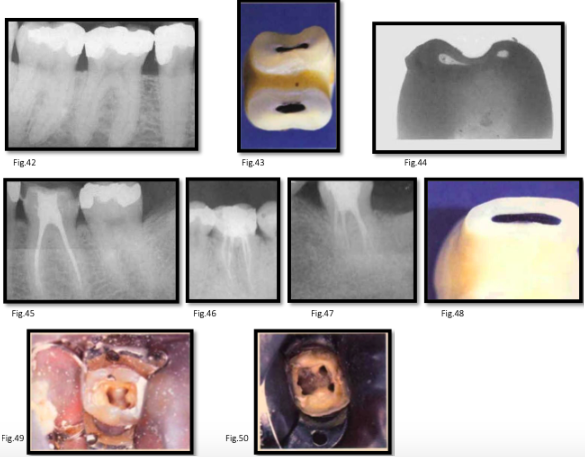
canal anatomy of mn 1st molar
roots: usually 2 (mesial and distal)
mesial root:
2 canals in 87% [fig. 42]
about half merge at apical foramen
canals curve mesially then gradually distal
mesiobuccal canal more curved than mesiolingual
canals may communicate along their length [fig. 43]
grooves on midline wall increase perforation risk [fig. 44]
distal root:
canal centrally located, slightly behind middle bucco-lingual fissure [fig. 45-47]
single canal cases: Broad bucco-lingually [fig. 48]
canal openings:
mesiobuccal → beneath mesiobuccal cusp
mesiolingual → nearer midline
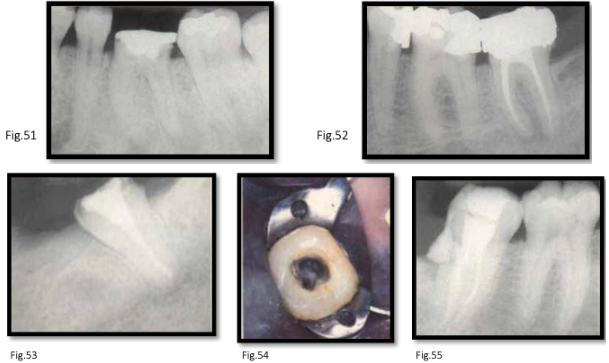
canal anatomy of mn 2nd molar
similar to first molar
distal root: lower incidence of two canals
roots: tend to be closer together [fig. 51-52]
mesial root: usually 2 canals, occasionally 1 (broad bucco-lingually)
rare variations:
single root with single canal [fig. 53]
c-shaped canals → distal canal extends mesially, sometimes including mesiobuccal and mesiolingual canals [fig. 44-45]
difficult to detect on preoperative radiographs