Haemostasis & Thrombosis
1/136
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
137 Terms
Hemostasis
the process by which blood clots form at the site of vascular injury
4 steps of response to vessel injury
1. Vasoconstriction to reduce blood flow
2. Platelet plug formation (von Willebrand factor binds damaged vessel and platelets)
3. Activation of clotting cascade with generation of fibrin clot formation
4. Fibrinolysis (clot breakdown)
Roel of endothelin at site of injury
Causes Vasoconstriction & stops release of Nitric Oxide and prostacyclin
What triggers primary haemostasis
Disruption of the endothelium exposing collagen and von Willebrand factor (vWF)
How do platelets form a platelet plug
Platelets adhere via vWF
Platelets activate and change shape
Granule release recruits additional platelets
Aggregation forms the platelet plug
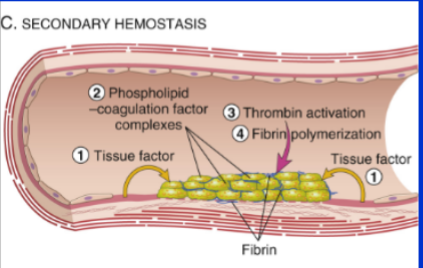
What initiates secondary haemostasis in vivo
Exposure of Tissue Factor (TF) from vascular injury
4 steps of secondary haemostasis
Tissue factor exposed → activates Factor VII → thrombin generation → fibrin mesh & platelet plug form
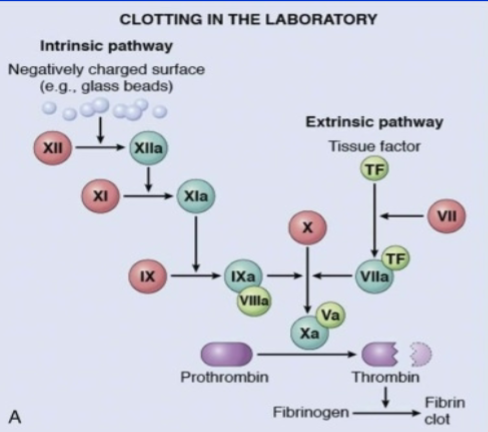
Differentiate between activating the extrinsic & intrinsic pathways of coagulation
Intrinsic - negative charged substance such as glass beads
Extrinsic - source of tissue factor (main one in vivo)
What factors are involved in intrinsic vs extrinsic clotting cascades
Role of t-Pa
tissue plasminogen activator is a counterregulatory mechanism made by endothelial cells that limit clotting to the site of injury and eventually lead to clot resorption & tissue repair
What enzyme is responsible for fibrinolysis
Plasmin
Plasmin is generated by enzymatic catabolism of the inactive circulating precursor …
plasminogen
most important plasminogen activator
t-PA
t-PA; it is synthesized principally by endothelium and is most active when in what state
bound to fibrin
What about the way it works makes t-PA a useful therapeutic agent
its fibrinolytic activity is largely confined to sites of recent thrombosis
What prevents platelet aggregation & coagulation & promotes fibrinolysis in endothelium with no injury
anticoagulant factors
Endothelium is activated by what
trauma, sepsis, bacteria, cancer, cytokines, …
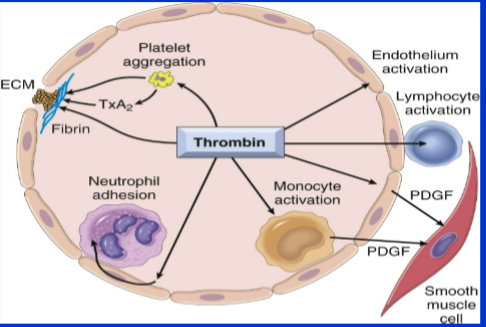
Role of thrombin
Generates cross-linked fibrin (cleaves fibrinogen & activates factor XIII)
Activates several other coagulation factors
Modulates several cellular activities
Directly induces platelet aggregation
Directly induces TxA2 production
Activates endothelial cells
Directly activates leukocytes
Through what receptors does thrombin modulate cellular activities
Through protease-activated receptors (PARs)
When endothelial cells are activated by thrombin, they release what
They respond by expressing adhesion molecules and cytokine mediators (e.g., PDGF ).
True/False platelets are anucleate
True
What type of receptor do platelets have
Glycoprotein receptor
True/False platelet cytoskeleton is rigid
False - it’s contractile
What is contained within platelet α granules
selectin, fibrinogen, vWF, Factor V, PF4, PDGF
What is contained within platelet δ granules
ADP, ATP calcium, serotonin, adrenaline
Main role of platelets
Platelets provide surface that binds and concentrates coagulation factors
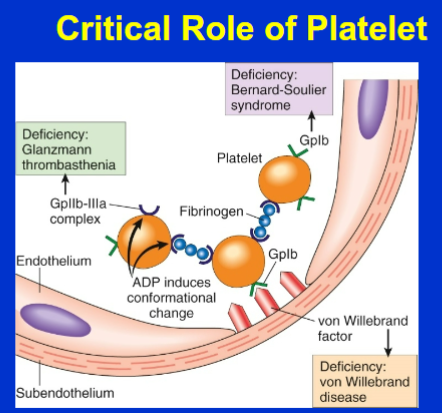
What do platelets do when an endothelial injury exposes the underlying basement membrane ECM
platelets adhere to the ECM primarily through the binding of platelet GpIb receptors to VWF
We know that platelets adhere to the ECM in endothelial injury but what could cause them not to do this (2)
Von Willebrand Disease
Bernard Soulier
Adhesion of platelets to the ECM leads to platelet activation → secretion of platelet granule contents. Give 2 examples of what is secreted
Calcium
ADP
What could prevent the release of platelet granule contents such as calcium & ADP
Storage Pool Disorders
Function of calcium in coagulation
cofactor for several coagulation proteins
Function of ADP in coagulation
mediator of further platelet activation
Activation of platelets from adhesion to ECM leads to what structural changes
dramatic changes in shape and membrane composition
Activation of platelets from adhesion to ECM leads to activation of what receptors
activation of GpIIb/IIIa receptors
What happens once GpIIb/IIIa receptors are activated on platelets
They form bridging cross-links with fibrinogen, leading to platelet aggregation
What could interfere with the formation of cross-links with fibrinogen from GpIIb/IIIa receptor activation
Glanzmanns Thrombasthenia
Fibrin deposition cements the platelet plug in place. What promotes fibrin deposition
Activation of thrombin via Protease Activated Receptor (PAR1) promotes fibrin deposition
Name the 3 disorders that can affect platelets in coagulation
Bleeding disorders are generally due to a defect in 3 things. Name the 3 things & their accompanying disorders
Vessel wall: Ruptured aorta/aortic dissection - Ehlers Danlos syndrome
Platelets: Glanzmanns thromasthenia
Coagulation factors: Haemophilia
True/False Bleeding disorders are all inherited
False - inherited/Acquired
Name a Collagen vascular disorder that affects haemostasis
Ehlers Danlos syndrome
Name a disorder that leads to inflammation of blood vessels that affects haemostasis
Vasculitis “palpable purpura”
Name a disorder that can make Blood vessels fragile & affects Haemostasis
Amyloidosis
Primary Haemostasis
How do patients present? (what’s the hallmark sign among the signs)
Hallmark is Mucocutaneous bleeding
– Purpura
– Epistaxis
– Menorrhagia
– Post partum Haemorrage
– GI bleed
– Bleeding post dental extraction
– Post operative bleeding
– Iron deficiency anaemia
Name 3 inherited Disorders of Primary Haemostasis
– Bernard Soulier Gp1b IX
– Glanzmann Thromasthenia GP IIb/IIIa
– Storage pool disorder
Most common inherited bleeding disorder
Deficiency of VWF
Name 3 acquired Disorders of Primary Haemostasis
– Uraemia/renal Failure
– ASPIRIN inhibits cyclooxygenase
– Clopidogrel/Prasugrel/ P2Y12
True/False VWD is a disorder of secondary haemostasis
False - It’s a disorder of Primary Haemostasis
VWF roles (2)
Von Willebrand factor VWF is involved in primary haemostasis and also protects factor VIII from destruction.
True/False Muscle or joint bleeds are rare in VWD
True - only found in severe forms (due to reduction of Factor VIII)
VWD treatment (3 options)
Tranexamic acid
DDAVP
Von Willebrand concentrate
3 steps to a Von Willebrand Disease Diagnosis
1. Personal history of muco-cutaneous bleeding
2. Family history of muco-cutaneous bleeding
3. Laboratory studies consistent with VWD
Differentiate between the 3 different types of VWD
Type 1 VWD: Quantitative Reduction in VWF
Type 2 VWD: Qualitative mutants of VWF
Type 3 VWD: Absence /Severe Reduction in VWF
By what inheritance pattern is VWD inherited
Autosomal Dominant
True/False Defects in platelet function lead to severe bleeding
False - Bleeding usually mild outside of surgery or
dental extractions
How are Platelet function defects diagnosed
– Assess platelet function in Laboratory
– Measure glycoprotein on surface of cells
Platelet function defects treatment options (4)
Tranexamic acid (antifibrinolytic)
DDAVP
Platelet transfusion
Activated Factor VIIa
Name 2 Disorders of secondary haemostasis
B. Coagulation abnormalities
Haemophilia
What causes haemophilia
Factor VIII and IX deficiency.
Disorders of secondary haemostasis also include bleeding disorders from Fibrinogen (Factor I) Factor II, Factor V, Factor VII, Factor X, Factor XI and Factor XIII deficiency. Are these common/rare
Rare
Symptoms of Fibrinogen (Factor I) Factor II, Factor V, Factor VII, Factor X, Factor XI and Factor XIII deficiency
• Muscle bleeding
• Intracerebral Bleeding
• GI Bleeding
• Dental bleeding
• Bleeding at time of surgery
• Joint bleeding
By what pattern are Haemophilia A & B inherited
X linked
Haemophilia A is a deficiency in what factor
Factor VIII
Haemophilia B is a deficiency in what factor
Factor IX
Haemophilia __ is approx. 5x more common than haemophilia _
Haemophilia A is approximately five times more common than haemophilia B
How to differentiate between Haem A/B
Blood test only
Due to its inheritance pattern, severe haemophilia affects only males/females
Males
Method of administration for treatment of bleeds
Treatment given IV through vein or port
Haemophilia treatment (for prevention of bleeds) (& method of administration)
Gene therapy
Mimetic products (Haemlibra, aka Emicizumab)
Subcutaneous administration
Emicizumab brings baseline clotting factors up to what % by mimicking what factor
15%
Mimics Factor VIII
A father has Haemophilia. Will his son/daughter be affected
Daughter will be a carrier
Son will not be affected (as it is X linked and Dad will pass on Y to son)
A mother has Haemophilia. Will her son/daughter be affected
Daughter has 50:50 chance being a carrier
Son has 50:50 chance of having haemophilia
What % of haemophilia patients have no known family history of haemophilia
30%
Explain how the PT Coagulation Screening Test is carried out & what it assesses & what the normal range is
Prothrombin Time (PT)
Process: Tissue Factor TF, calcium & phospholipid added to plasma and measure time to clot
Assesses: Factor VII in Extrinsic Pathway, & I, II, V, X in Common Pathway
Normal Range: 10-13 seconds
What standardised test is the PT value used in
INR - used to monitor anticoagulant effect of Warfarin
Explain how the APTT Coagulation Screening Test is carried out & what it assesses & what the normal range is
Method: Initiated by negatively charged particles (ground glass/silica) to activate Factor XII in presence of Phospholipid and Calcium. Measure time taken for clot to form.
Assess: Intrinsic Pathway Factors XII, XI, IX and VIII & may also be used to assess Common Pathway Factor II, V, X and Fibrinogen (Factor I)
Normal Range: 20-30 seconds
What would cause an Isolated Prolonged PT
Factor VII deficiency
What would cause a prolonged APTT (4)
• Factor VIII deficiency
• Factor IX deficiency
• Factor XI deficiency
• Factor XII deficiency
What would cause a Prolonged PT & APTT (4)
• Factor I (Fibrinogen) deficiency
• Factor II (prothrombin) deficiency
• Factor V deficiency
• Factor X deficiency
True/ False: A Normal Coagulation Screening can bee seen in all 3 of these diseases
• von Willebrand’s Disease
• Platelet Disorders
• Factor XIII deficiency
True
Outcome of severe factor II deficiency
Severe factor II deficiency (prothrombin) is incompatible with life
Treatment required for people with Severe Fibrinogen (Factor I), X, XIII deficiency
It is present as a neonate & replacement is required from diagnosis
Outcome of Severe V and VII deficiency
variable bleeding
Outcome of severe Factor XI deficiency
Severity of deficiency doesn’t matter - level does NOT correlate with bleeding risk
Outcome of Severe XII deficiency
No bleeding & may contribute to thrombosis
Thrombosis
Blood clot that forms within intact blood vessel or in chambers of the heart
Embolism
detached intravascular solid, liquid or gaseous mass that is carried by blood from its point of origin to a distant site where it often causes tissue dysfunction or infarction
What type of embolism is most common
Pulmonary Embolism is most common
Symptoms and signs of a Pulmonary Embolism
Dyspnoea on exertion
Haemoptysis
Chest pain
Tachypnoea
Hypotension
Tachycardia
Leg symptoms or signs
Collapse
Sudden death
What % patients with DVT also have PE
50%
What % of PE originate in leg veins as a Deep Vein Thrombosis (DVT) (hence term Venous Thromboembolism VTE)
95%
Pulmonary Embolism treatment
anticoagulation
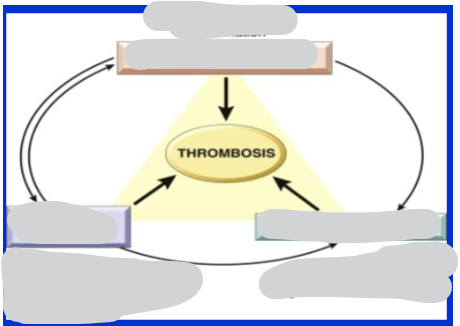
Fill in Virchow’s triad for the causes of thrombosis
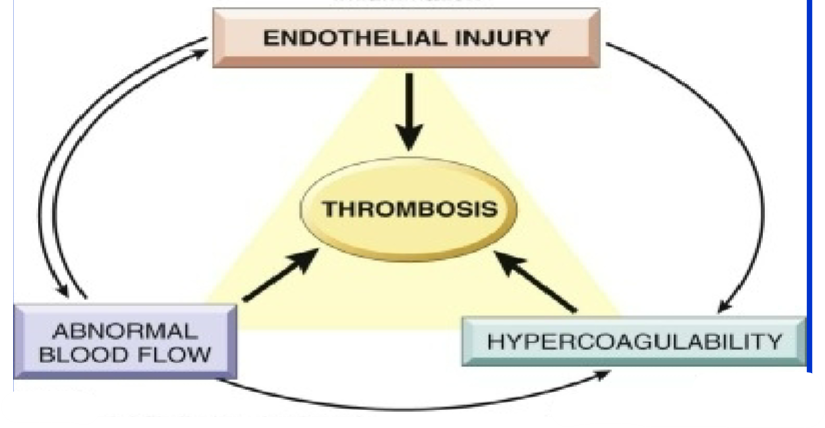
Give 2 examples of Endothelial Injury
Plaque rupture in atherosclerosis
Endothelial injury post MI
Give 5 possible causes of Endothelial Injury
It doesn’t need to be physically disrupted
– Increased procoagulant factors
– Decreased anticoagulant factors
– Turbulent flow
– Bacterial endotoxin
– Cigarette smoke
Name 3 causes of Alterations to blood flow
– MI stasis due to reduced contractility
– Aneurysm local stasis
– Atrial fibrillation
Hypercoagulability Definition
• Acquired or inherited abnormality of haemostasis predisposing to thrombosis
Or
• Haemostasis in the wrong place at the wrong time
Venous Thromboembolic Disease includes what 2 things
Deep Venous Thrombosis and Pulmonary Embolism