MIDI3 M2L1: Wound Management/ Suture 101
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
What are the MC types of mechanisms of wound creation?
- Shearing
- Tension
- Compression
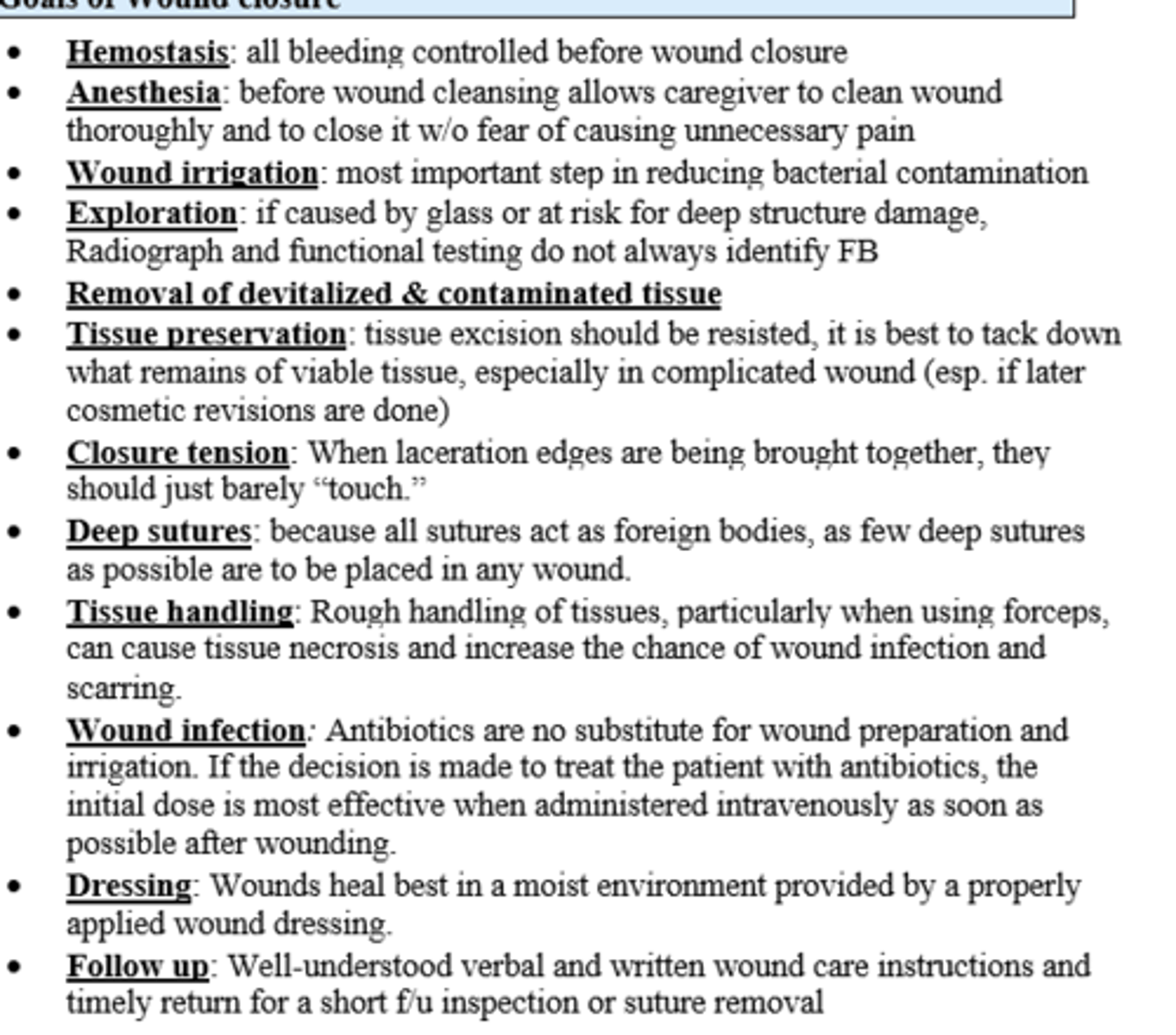
Superficial skin lacs that extend deep into the SubQ tissue should be considered for closure. What are the goals/indications of wound closure?
- Reduce healing time
- Reduce risk of infections
- Reduce scarring
- Repair the loss of structure/function
- Improve cosmetic outcome / cosmesis
What are the stages of wound healing & when do they occur from onset of injury?
1) Coagulation (hemostasis) - onset to 24 hours
2) Inflammatory - 6hrs - 7 days
3) Proliferative - 4days-3 weeks
4) Maturation & Remodeling - 3 weeks to 1 year
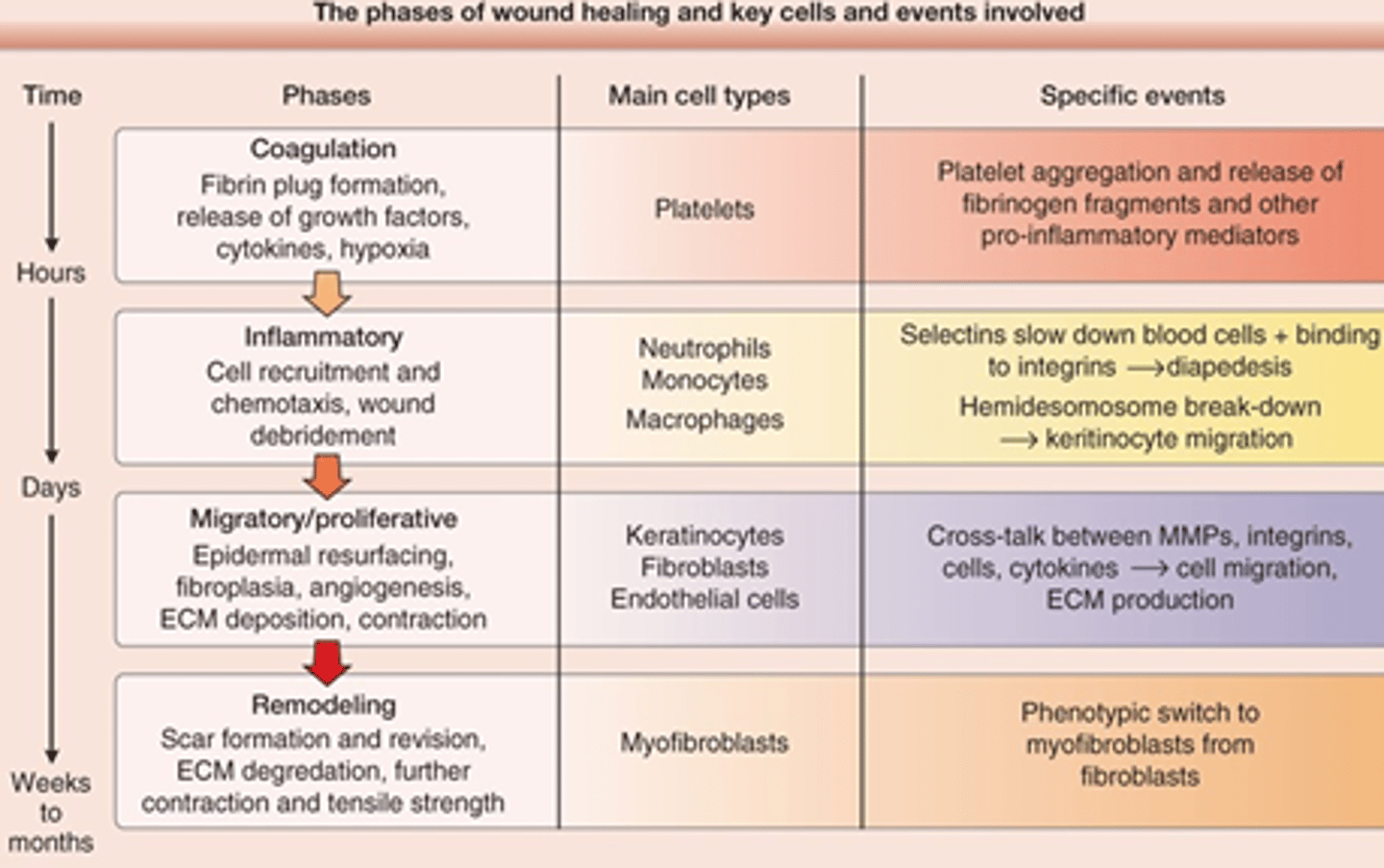
What are the key cells of each stage of wound healing?
1) Coagulation: Platelets
2) Inflammatory: Neutrophils, Monocytes, Macrophages
3) Proliferative: Keratinocytes, Fibroblasts, Epithelial cells
4) Maturation/Remodel: Myofibroblasts
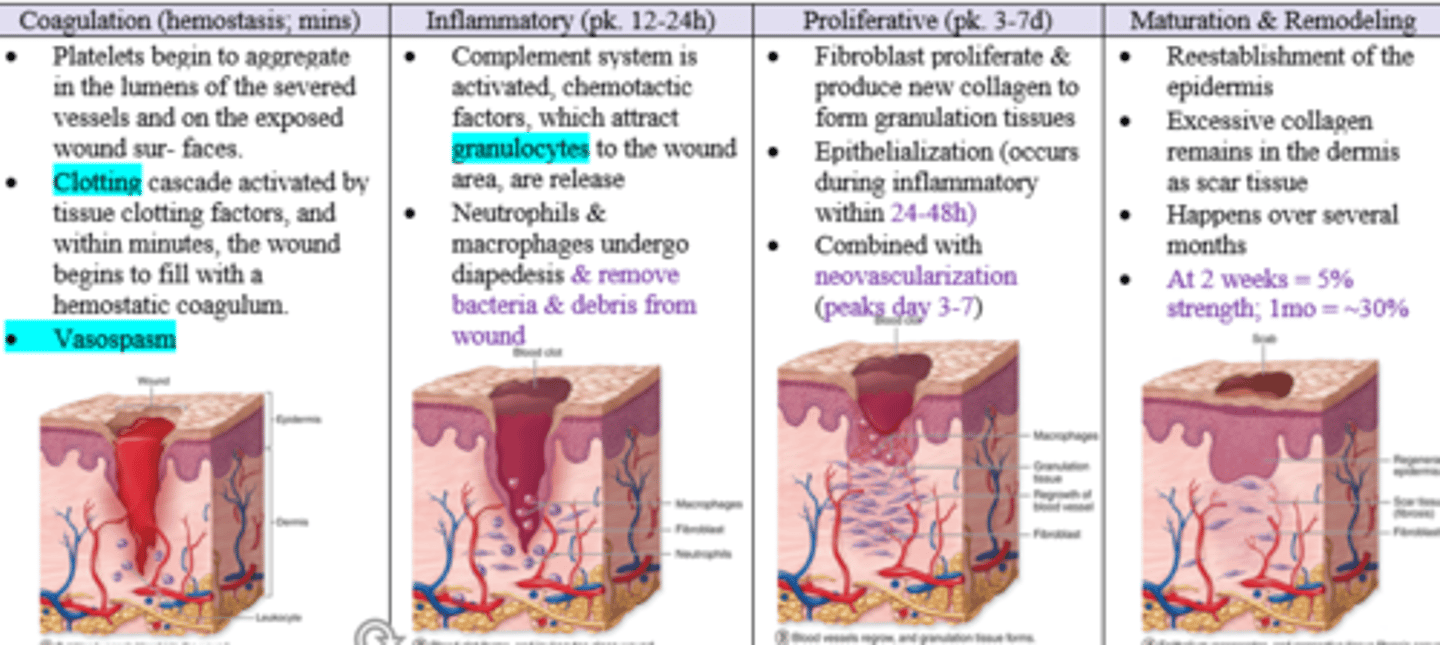
What are the key events that take place in the 1) Coagulation Phase that occurs from onset of injury to up to 6 hours?
- platelets aggregate and release fibrinogen fragments
- fibrin plug / clot formation
- platelets also release pro-inflammatory mediators, growth factors, and cytokines
- hypoxia and vasospasm
- Hemostasis achieved
What are the key events that take place in the 2) Inflammatory Phase that occurs from hours to days from onset ?
- Selectins slow down blood cells (Neutrophils, Mono/Macros) + binding to integrins --> Diapedesis
- Cell recruitment and chemotaxis
- Wound Debridement
- Hemidesomosome break-down
- Keratinocyte migration
What are the key events that take place in the 3) Proliferative / Migratory Phase that occurs from days to weeks from onset ?
- Epidermal resurfacing
- Fibroplasia
- Angiogenesis / Neovascularization
- ECM production / deposition
- contraction
What are the key events that take place in the 4) Remodeling Phase that occurs from weeks to months / 1 year from onset ?
- Fibroblasts --> Myofibroblasts
- Scar formation and revision
- ECM degradation
- further contraction and tensile strength
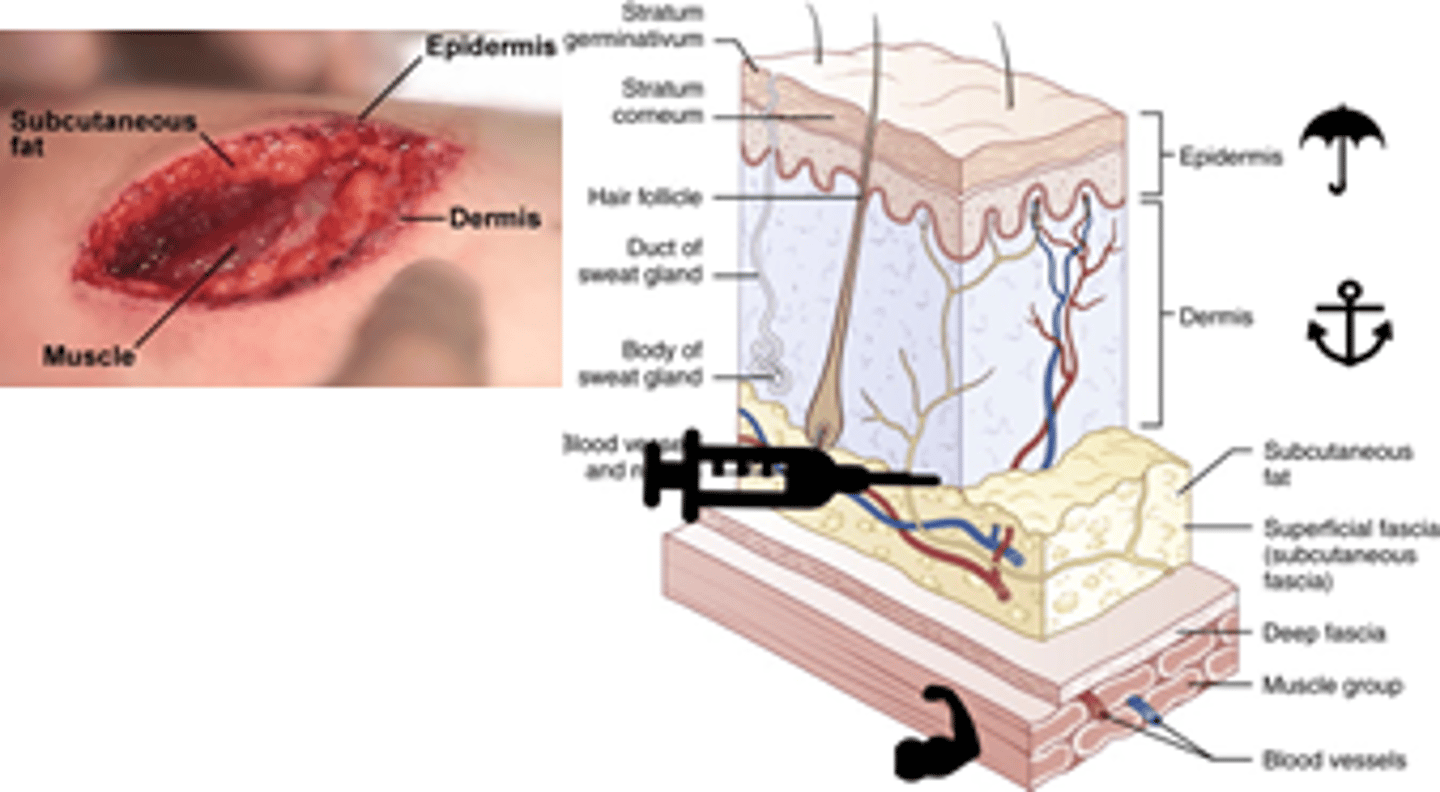
Describe epidermis, dermis, and subcutaneous layers and their role in wound healing
1. Epidermis (outermost layer) protective & prevents loss h2o & electrolytes
2. Dermis: connective tissue, key layer for proper wound repair
3. Subcutaneous (yellow/globular); where nerve fibers are and preferred delivery site for local anesthetics
What are the 3 types of wound closure intention classifications ?
1) Primary - epithelialization, connective tissue repair
2) Secondary - contraction, epithelilialzation
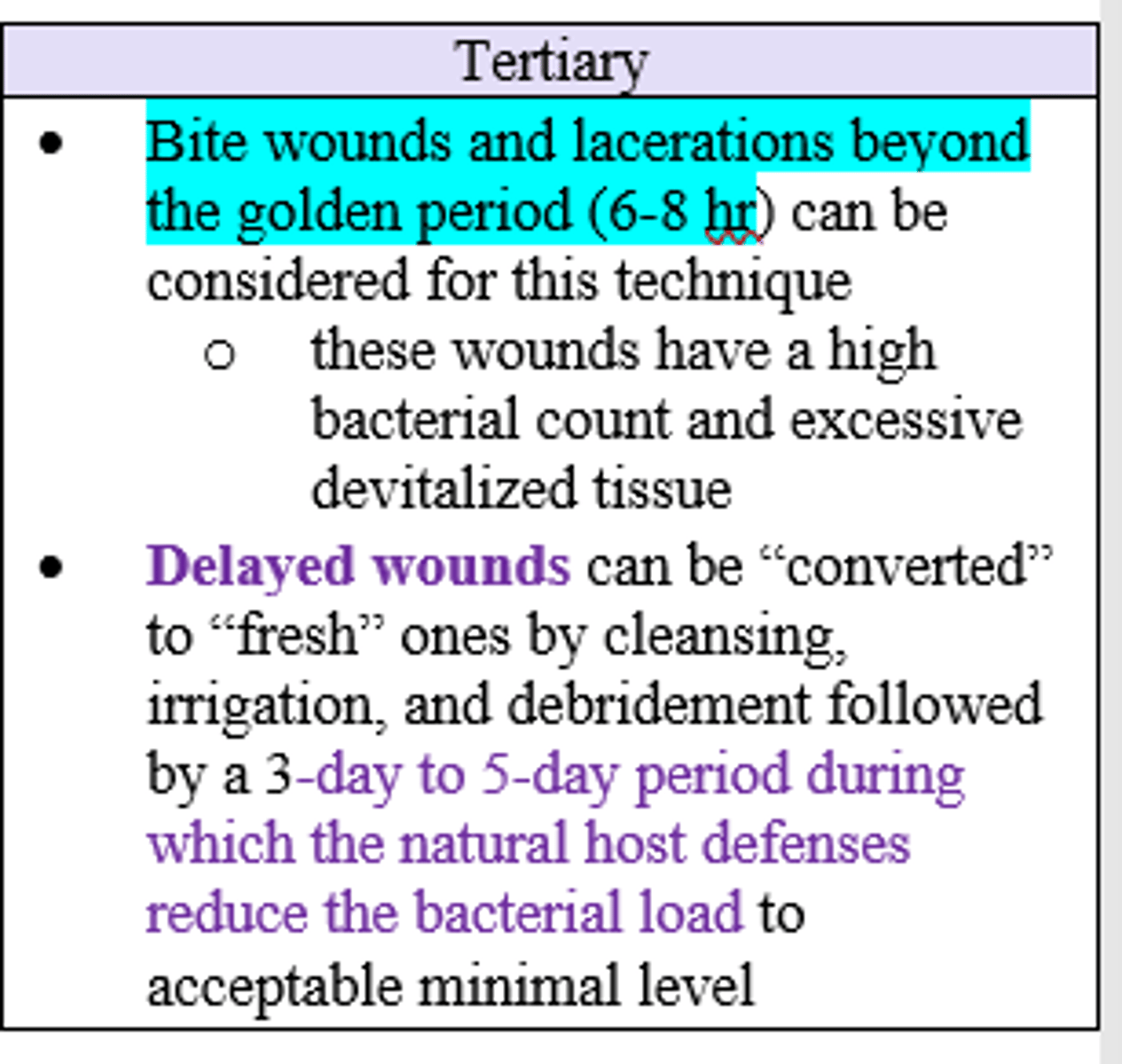
3) Tertiary - contraction, connective tissue repair
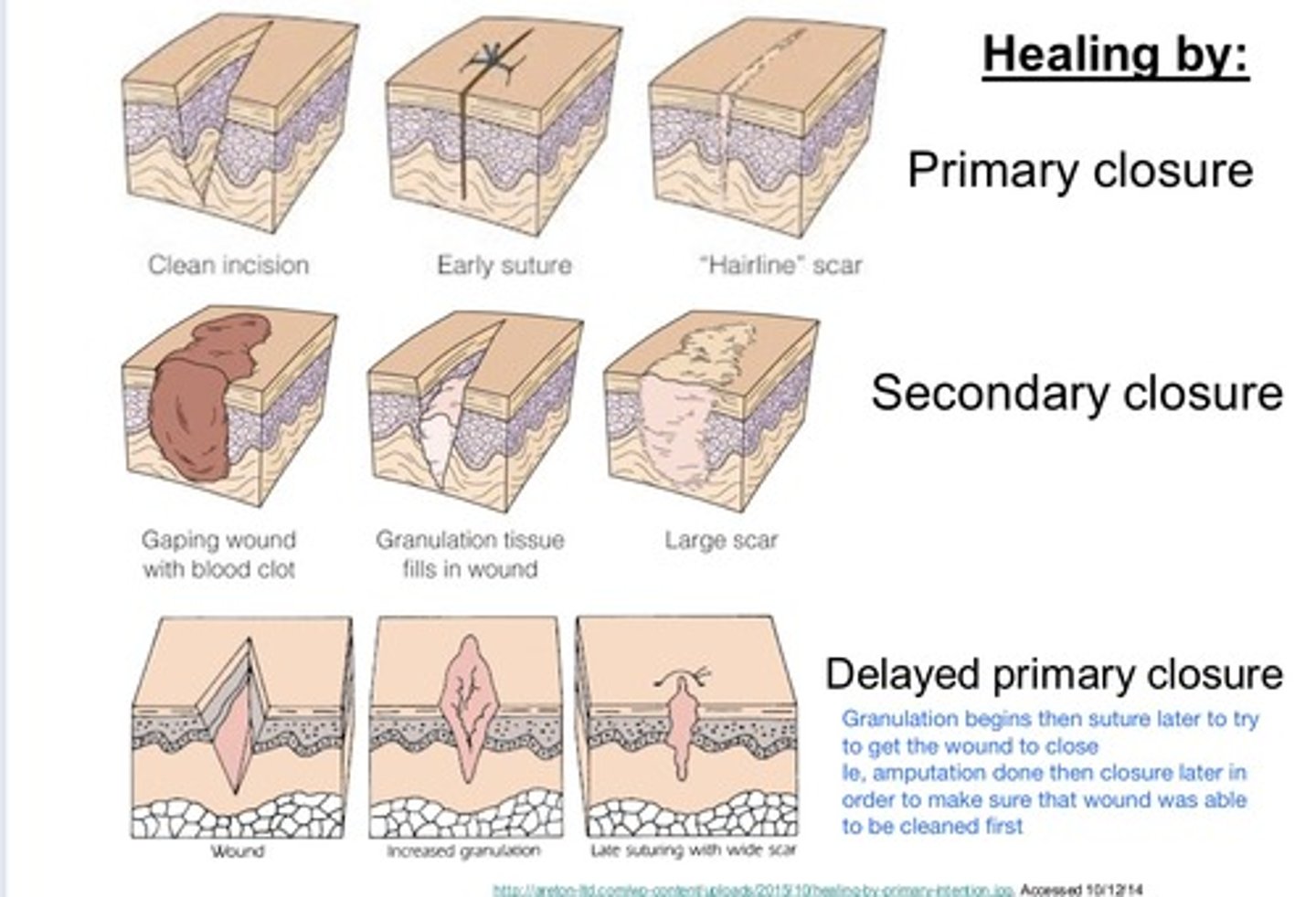
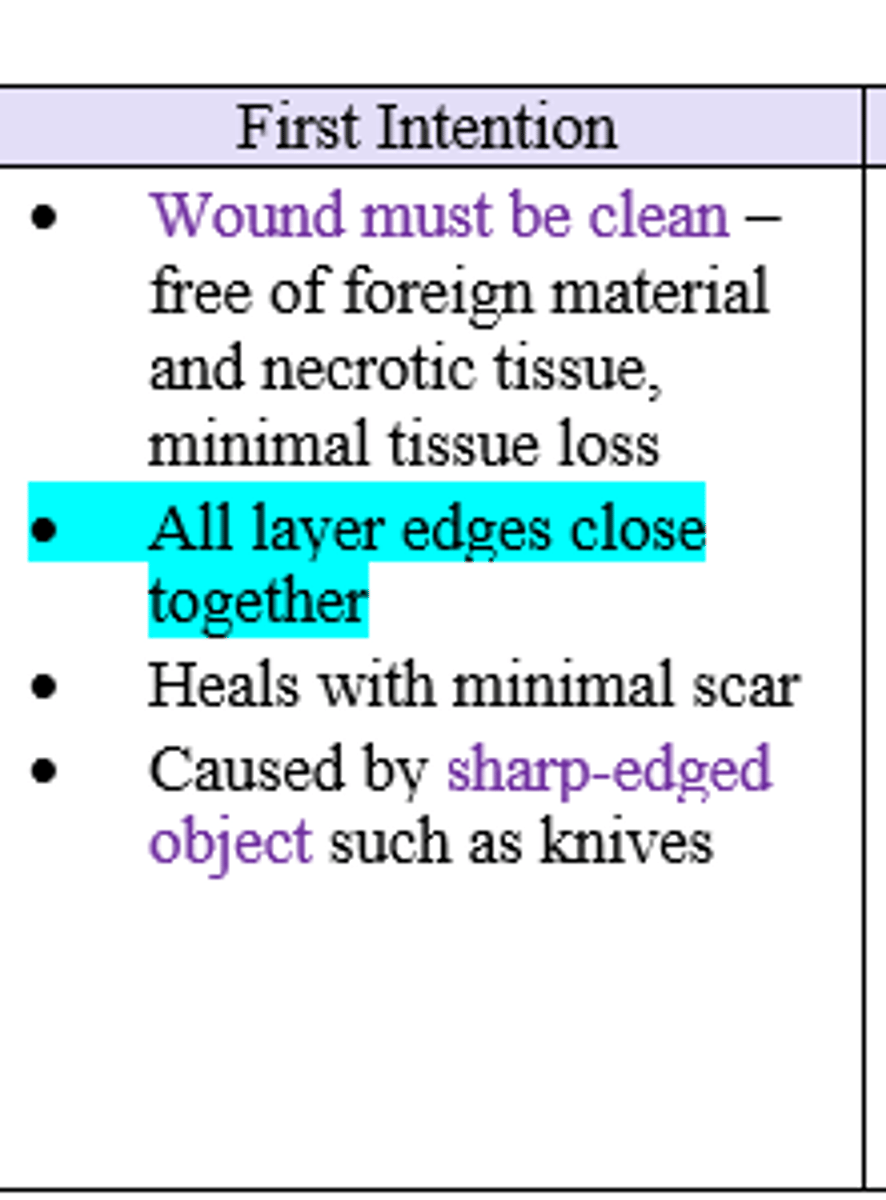
Which wound closure classification is optimal for a clean wound that was caused by sharp-edged object (ex. knife) and has the best chance for minimal scarring bc it is fully sutured/closed ?
First / Primary Intention
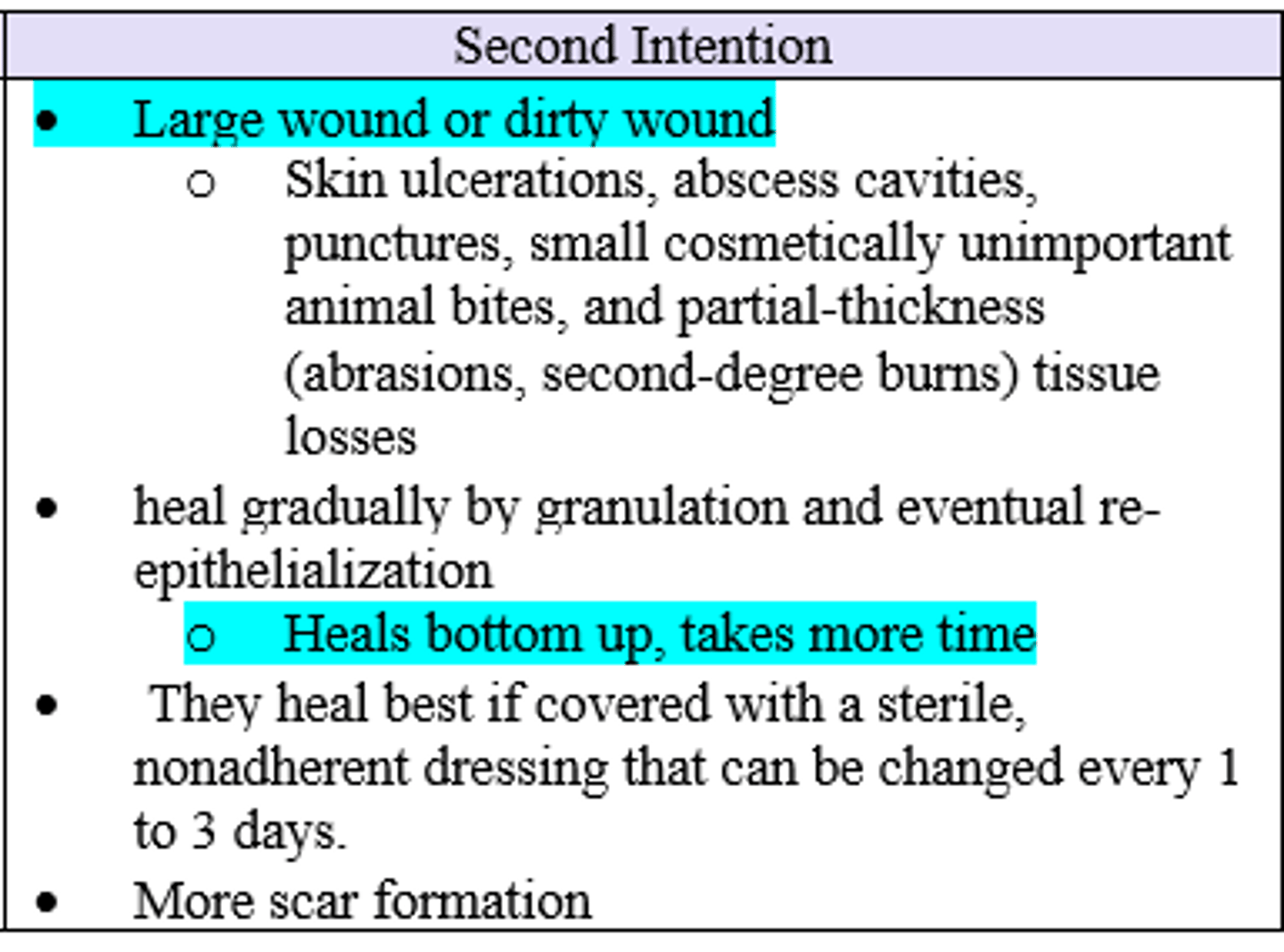
Which wound closure classification is optimal for a large (or dirty) wound where the deep layers are sutured closed but superficial layers are left to heal from inside out often leading to excessive tissue loss, infection, and a wide scar (ex. skin ulcer, abscess, cavities, punctures, small animal bites, partial thickness burns, tissue loss)?
Second / Secondary Intention
Which wound closure classification is optimal for a contaminated bite wound or lac that is >6-8hrs old, deep and has high bacterial count / excessive devitalized tissue, where deep layers are primarily sutured closed but superficial layer is left open to heal and reassessed after 4-5 days ?
Tertiary (or delayed primary closure) Intention
What are the 5 factors affect cosmetic outcome of a wound?
- Mechanism of Injury (MOI)
- Anatomic location (i.e. tension, oil, region)
- Infection
- poor technique (cleaning, excessive tension, materials, etc.)
- Disease/Drugs
(T/F) Sutures can produce permanent marks in the skin if left in for 5 days
False (but true if longer than 7-14 days)
What is the best chemical/surgical method to eliminate scars?
None available to eliminate
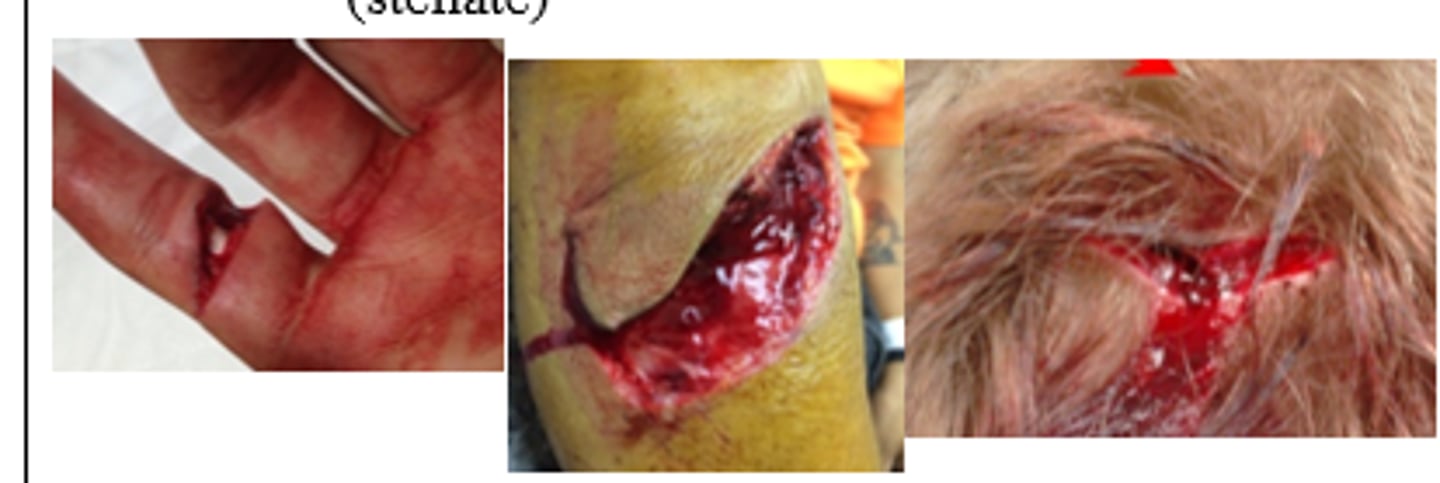
Patient has linear, clean wound. What type of MOI does this describe?
Shearing (simple cut caused by knife or glass dividing of tissue)

Patient has a wound shaped like a triangular flap (partial avulsion). What type of MOI does this describe?
Tension (blunt/semi blunt object striking skin at a glancing angle)

Patient has a wound that is satellite-shaped with ragged/shredded edges. What type of MOI does this describe?
Compression (blunt object striking skin at right angle)

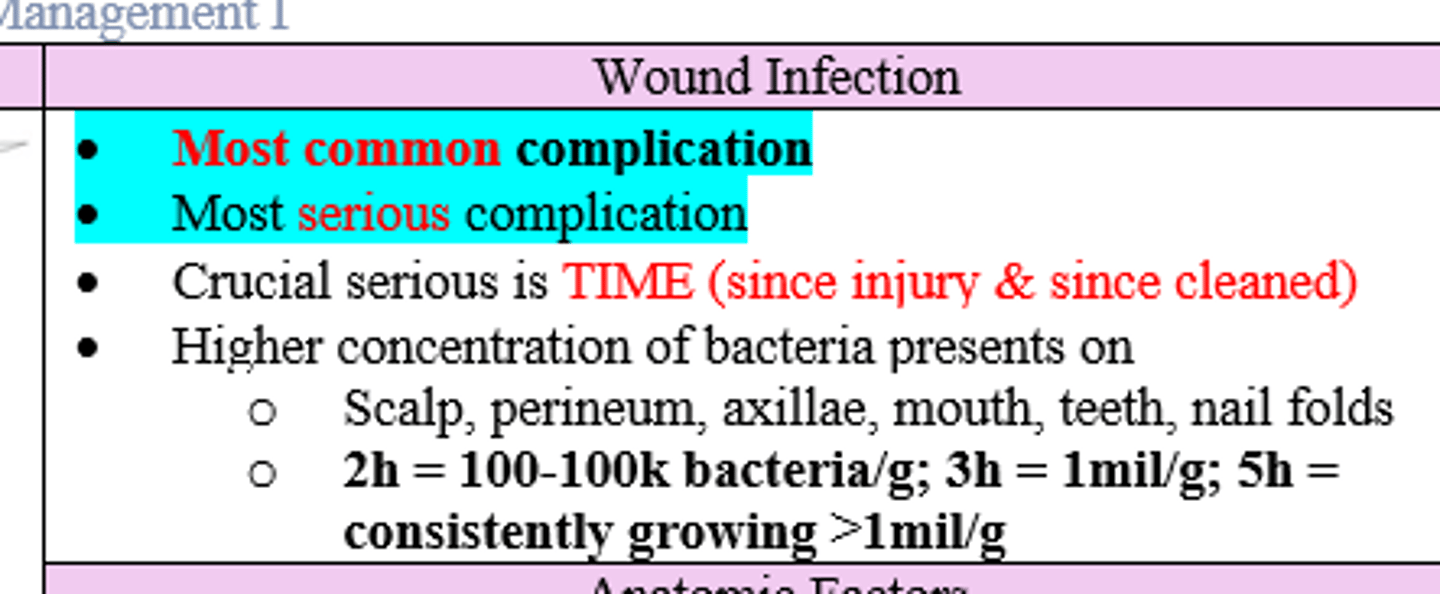
What is the most common and most serious complication of a wound? What is the most crucial factor for this?
- Wound Infection and disruption of underlying nerves, arteries, and tendons;
- Time
**High risk locations (more germs): scalp, perineum, axillae, mouth, feet, nail fold
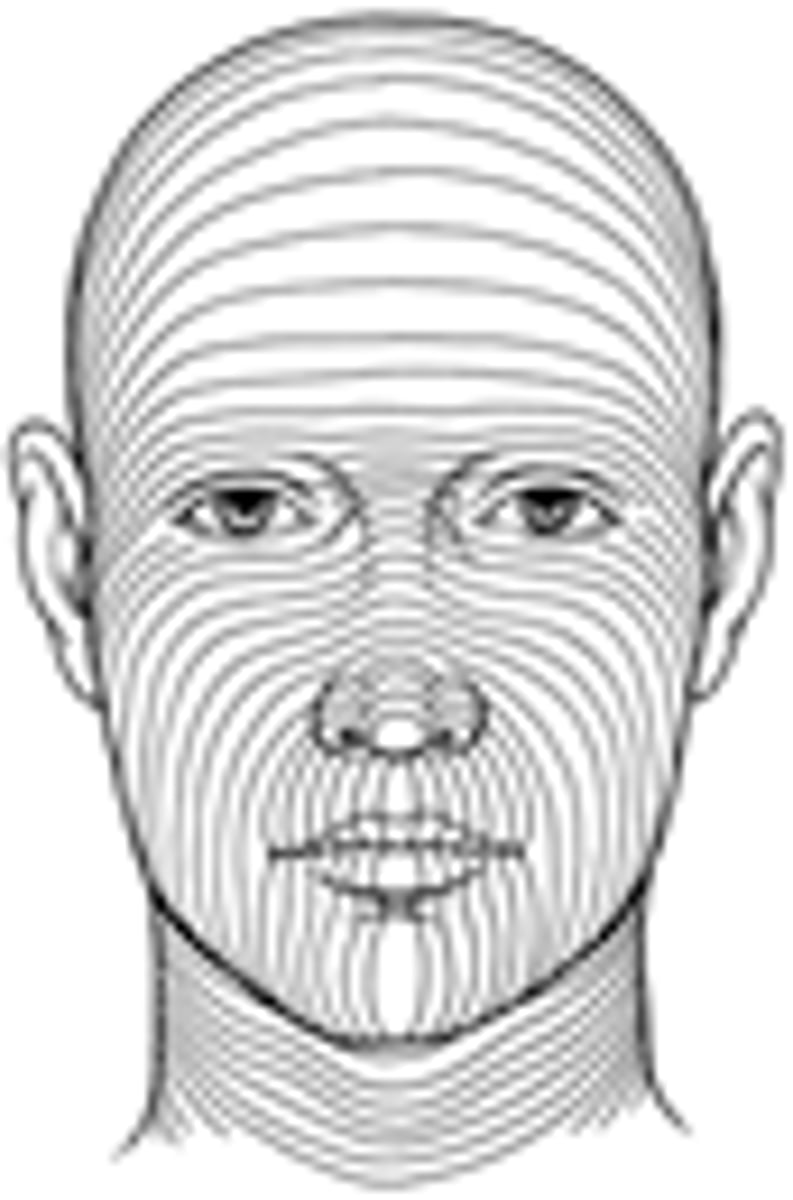
Lacs & incisions (perpendicular/parallel) to skin tension lines leave thinner and less visible scars
parallel
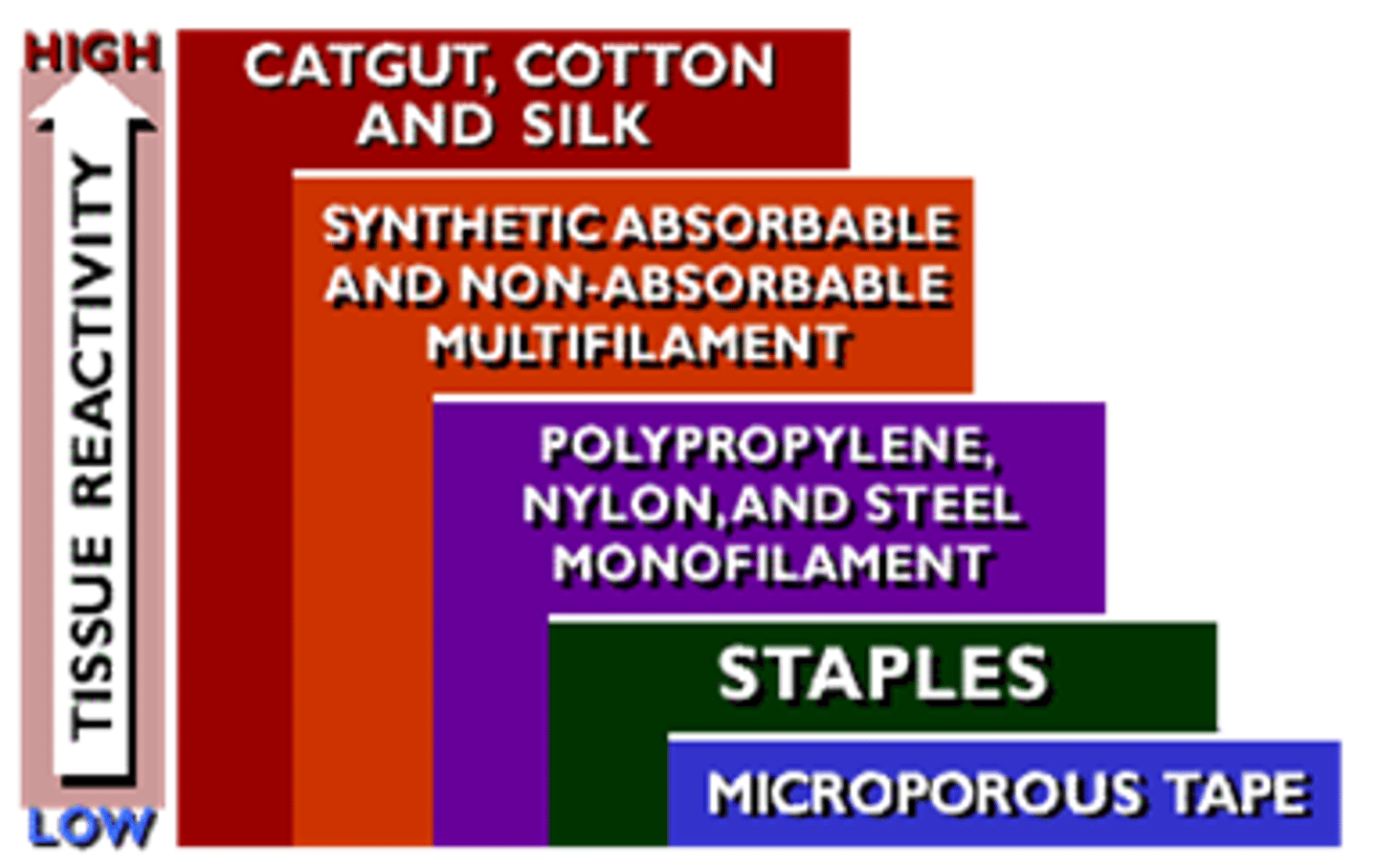
Which suture material is the least reactive and thus less likely to to cause an inflammatory reaction and poor cosmetic outcome (vs. Silk that causes more reactivity and absorbable sutures that can risk infection and provoke more scar response)?
Nylon & Polyprolene
Which drug has the most profound effect on wound healing / cosmetic outcome?
Long Term Corticosteroids - alters inflammatory response:
- decreases fibroblast, neovascularization / epithelialization
- leads to paper thin skin
Out of the following drugs/ supplements, which are the most helpful for wound healing?:
NSAIDs
Vitamin C
Vitamin A
Colchicine
Steroids
Zinc
Steroids
- Vitamin C
- Vitamin A
- Zinc
Pigmented & oily skin has (more/less) probability of scar formation
more
What are the Diseases (AAUDEHAPM) that can affect Cosmetic outcome of a wound / scar formation d/t persistent inflammation and thus slowing of angiogenesis, epithelialization, connective tissue deposition, and turnover (overall decreases quality of repair response)?
- Aging (everything slows)
- severe Alcoholism (slows protein synthesis)
- acute Uremia (dec. fibroblasts growth/strength of wound)
- DM (infection prone and dec. collagen synthesis and neovasc.)
- Ehlers-Danlos (abnormalities w/ collagen)
- Hypoxia
- severe Anemia
- PVD / Venous Ulcers
- Malnutrition
What are some different causes for suture marks?
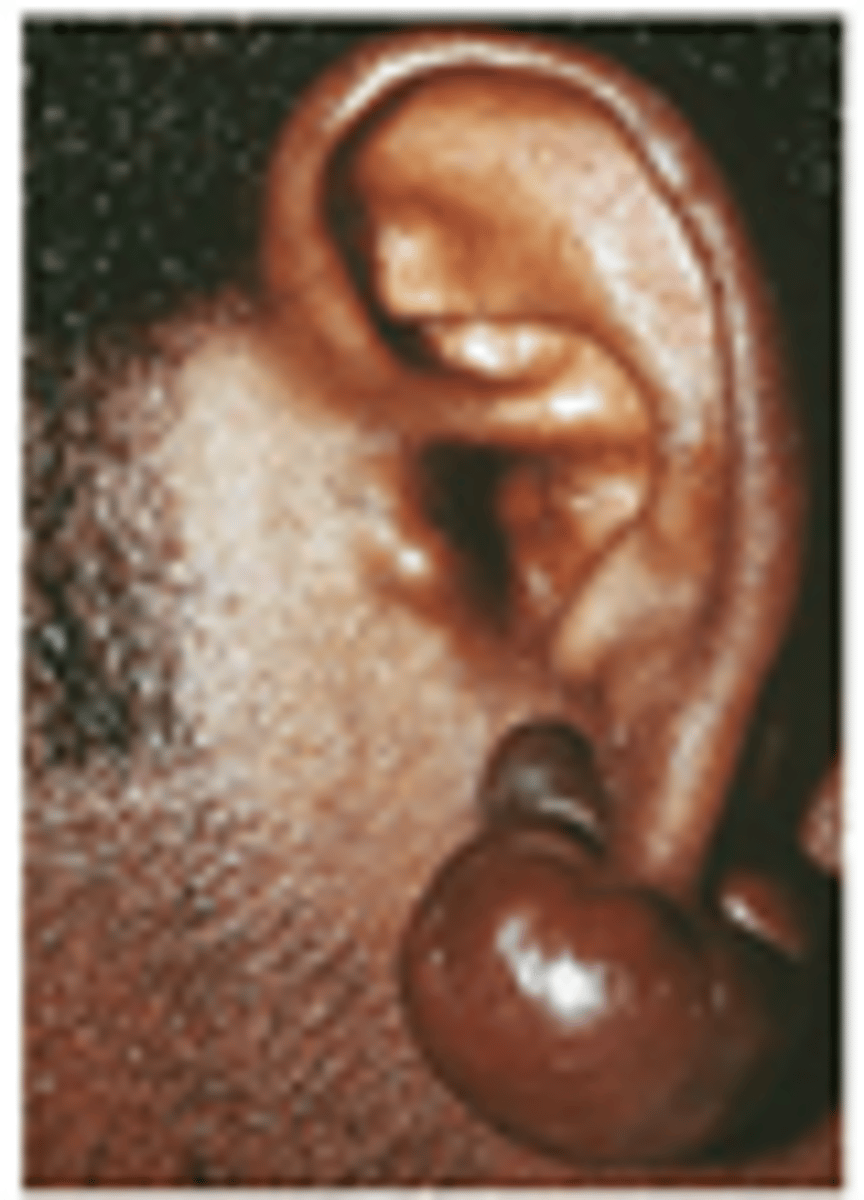
- Skin type (darker pigment --> prominent scar)
- Keloid/Hypertrophic tendency
- Suture Tension
- Stitch Abscess
- Duration of sutures
The tensile strength of a repaired laceration is only ___% of normal skin at the time of suture removal.
5
Potential complications of wound closure:
- infection (MC and most important)
- scarring / keloid formation
- loss function or structure
- loss of cosmesis
- dehiscence (reopens)
- tetanus infection
What are the key components of a general wound history that you need to ask about?
- MOI? possible FB?
- When / age of wound?
- Associated Sx's? (systemic, neovascular intact ?)
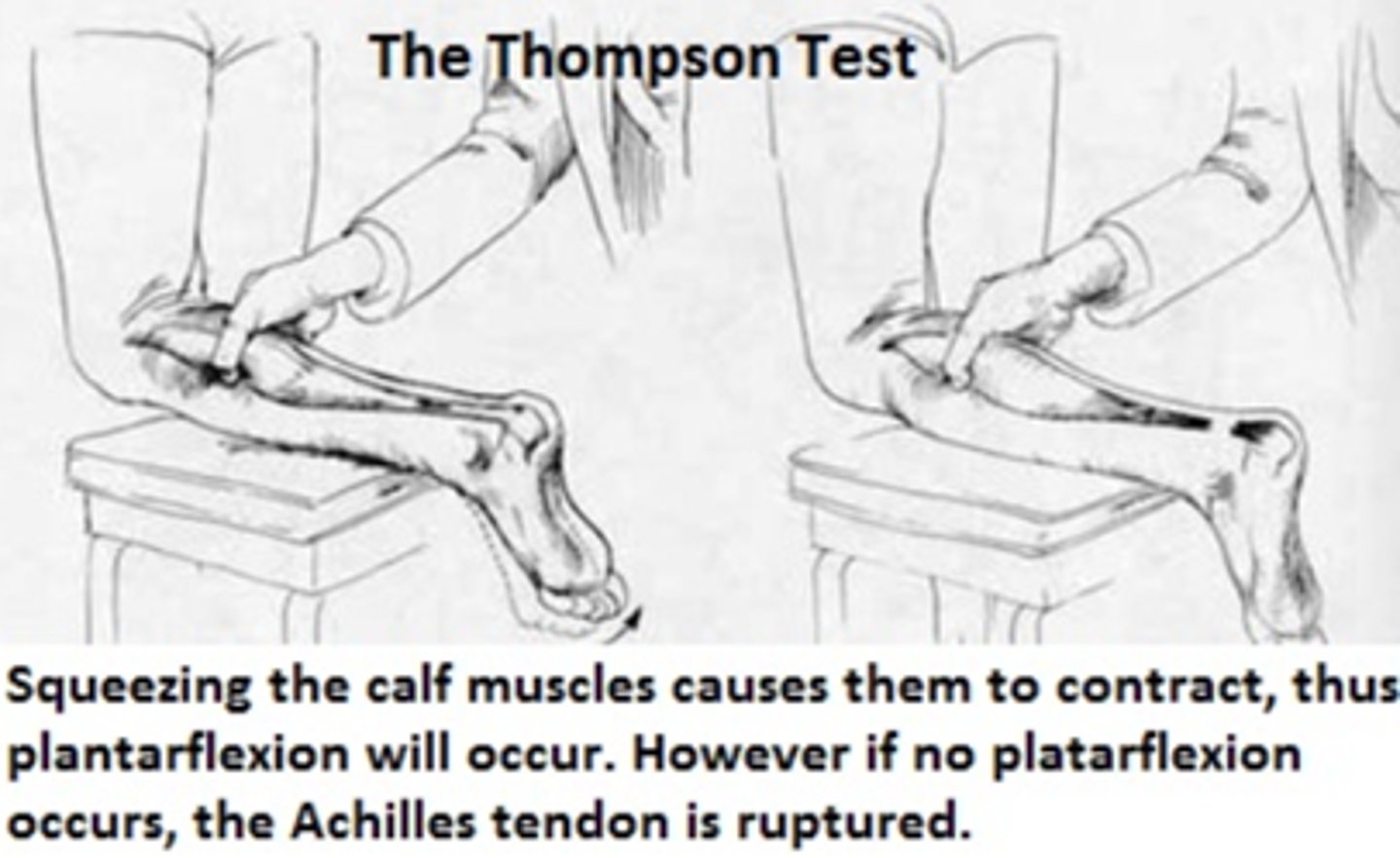
How can you assess Neovascular status in lower extremities that have sustained a wound?
The Thompson Squeeze Test
What are the golden period(s) to implement wound management / closure?
- within 6-8h from time of injury
- within 24h if clean or highly vascularized lesions (i.e. face, scalp)
** but if +12-18h, depending on MOI & contamination, consider leaving for 2ny intention healing
What are some initial decisions that should be made when a patient comes in needed a wound closure?
- Timing (within golden period?)
- Tetanus (UTD?)
- ABX (needed?)
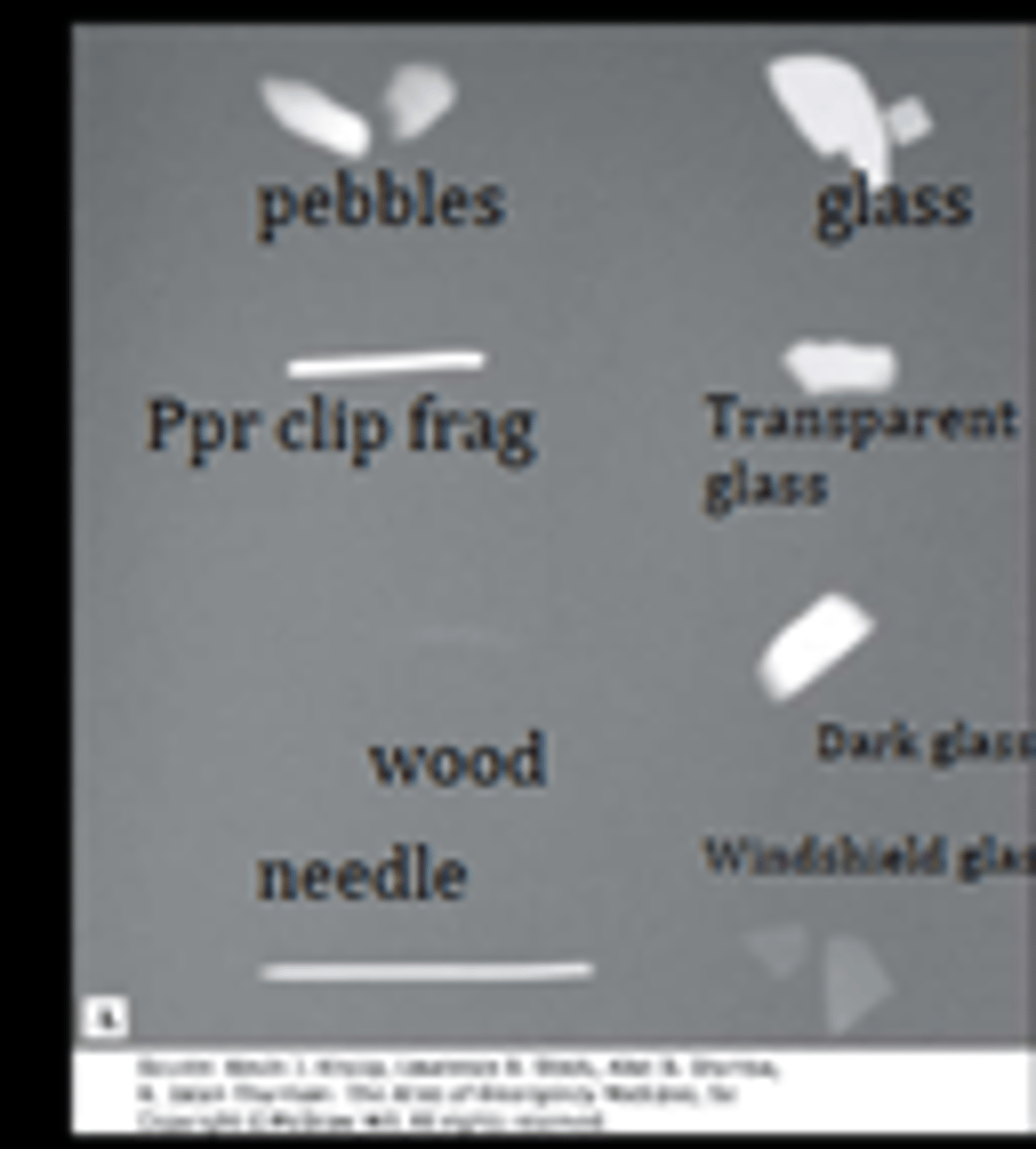
95% glass is radio(lucent/opaque)
radiopaque (x-ray every wound from glass)
What are some ways wounds can be classified?
1. Thickness (superficial vs. partial vs. full)
2. Complexity (simple vs. combined)
3. Age (fresh vs. old)
4. Origin (MOI)
5. Clean (vs. Clean-contam. vs. Contaminated vs. Infected)
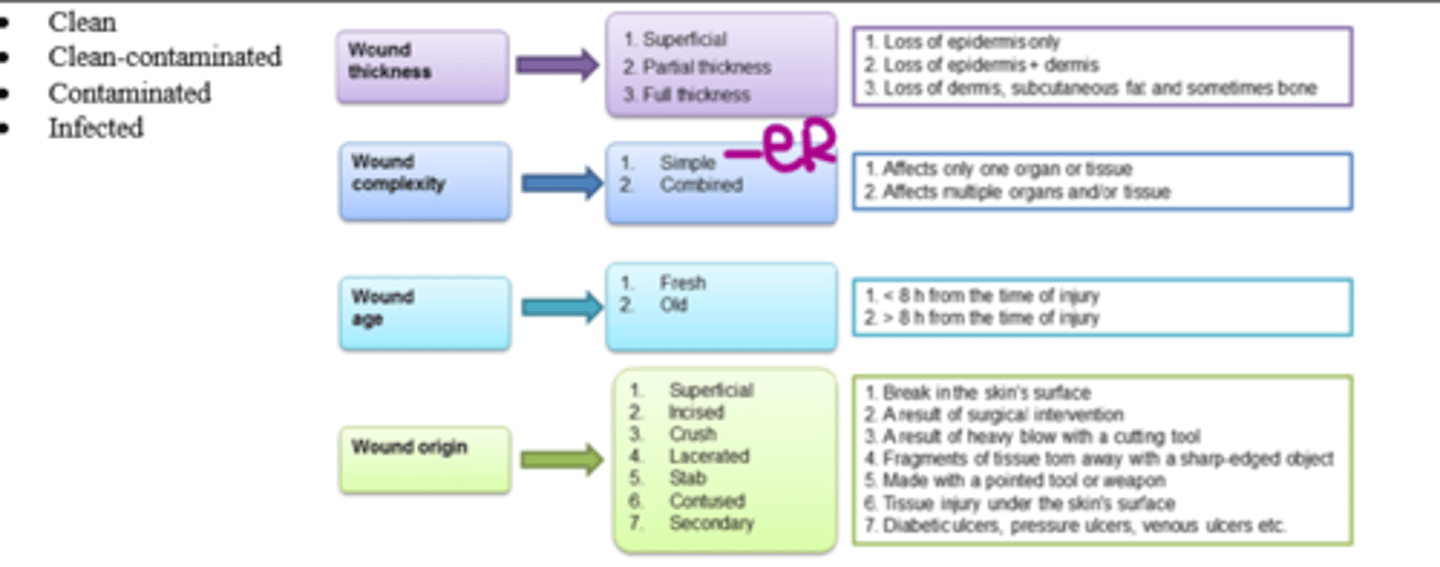
What is the MC wound complexity seen in the ER?
Simple (affects only one organ or tissue)
(vs. combined = affects 1+ organ/tissues system)
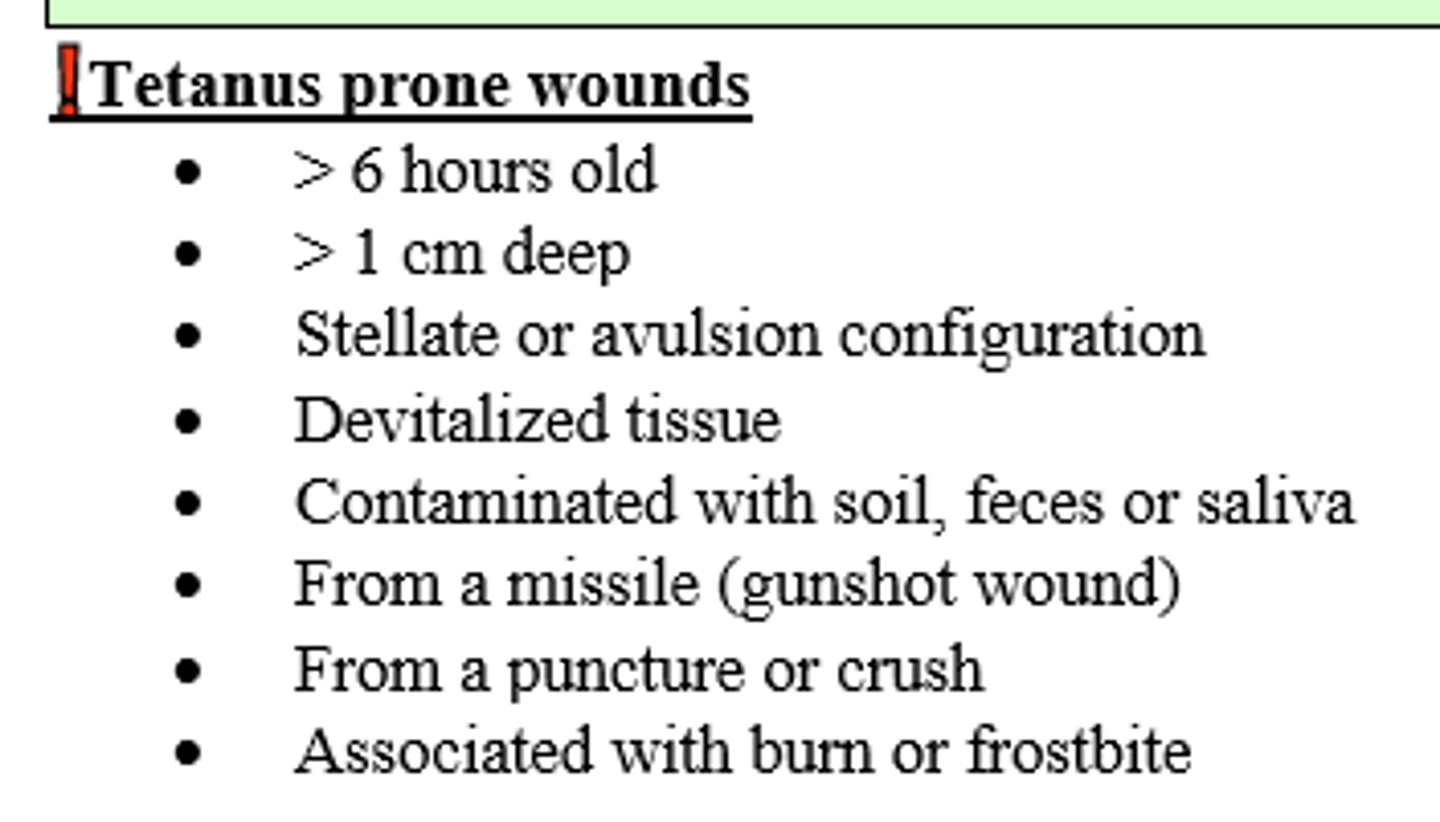
What is a description of a wound that would be the most prone to tetanus?
- Missile(gunshot) wound
- puncturing or crushing devitalized (ischemic) tissue
- w/ associated burn or frostbite
- ~6+ hours ago
- contaminated with soil, feces, and saliva
- > 1 cm deep
- stellate or ragged/avulsed edges
If a patient of any age has a contaminated wound (dirt, feces, saliva, soil, puncture, avulsion from flying/crushin object, animal bite, burn, or frost bite) and either never finished their 3 Tdap series vaccines or is unsure, what should you do?
- either Tdap vaccine or Td booster (if prev. vaxed)
- TIG anti-toxin
- if they refuse, then document !
Patient with gunshot wound that is contaminated with dirt is unsure if he finished his primary tetanus series. What should be done?
Admin Tdap Vaccine and TIg (Tet Human immunoglobulin anti-toxin) now
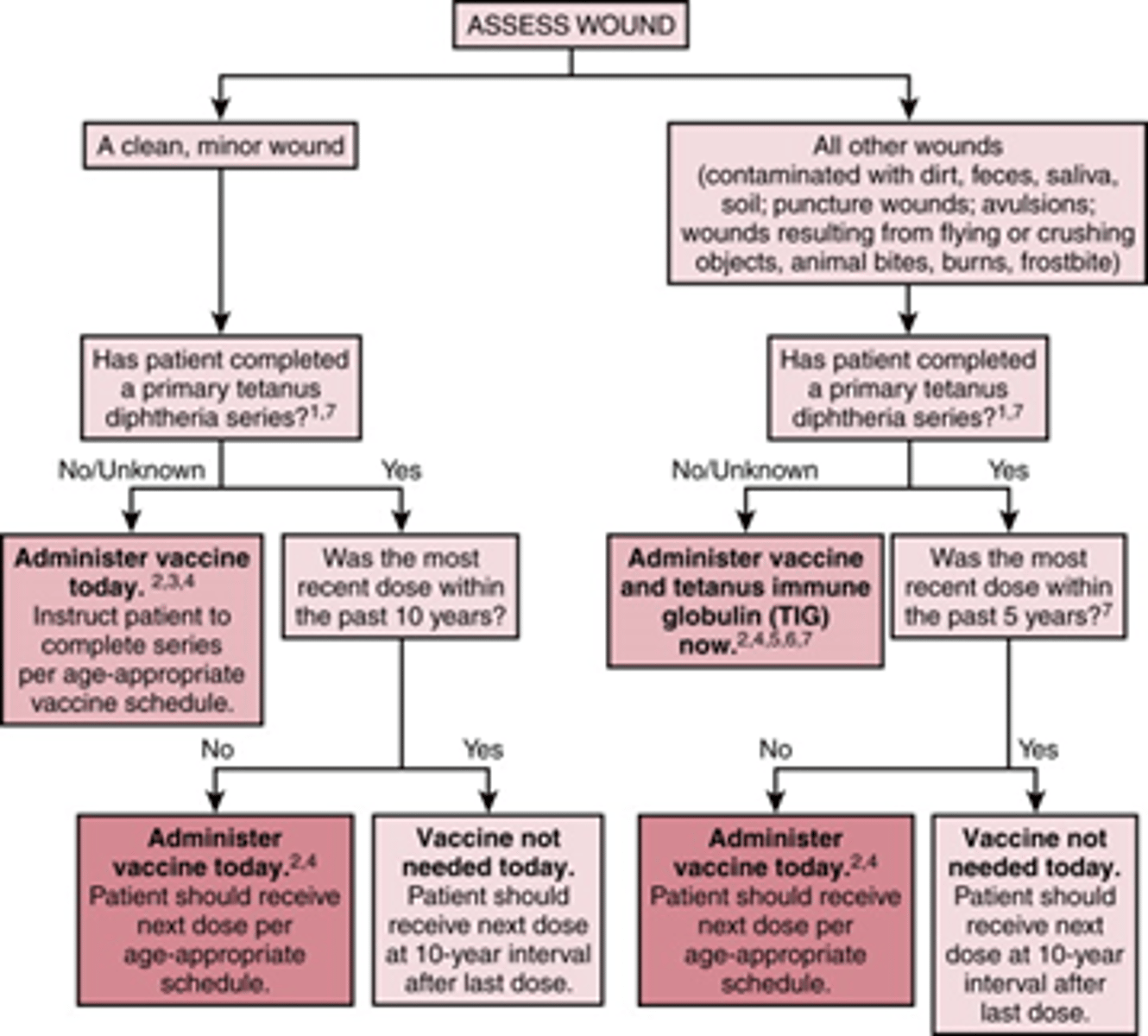
Patient has burn that occurred > 6 hrs ago. She has received her primary tetanus vaccination and had her booster a more than 5 years ago. What should be done?
Administer vaccine today
(wouldn't have to do it if < 5 years since prior dose)
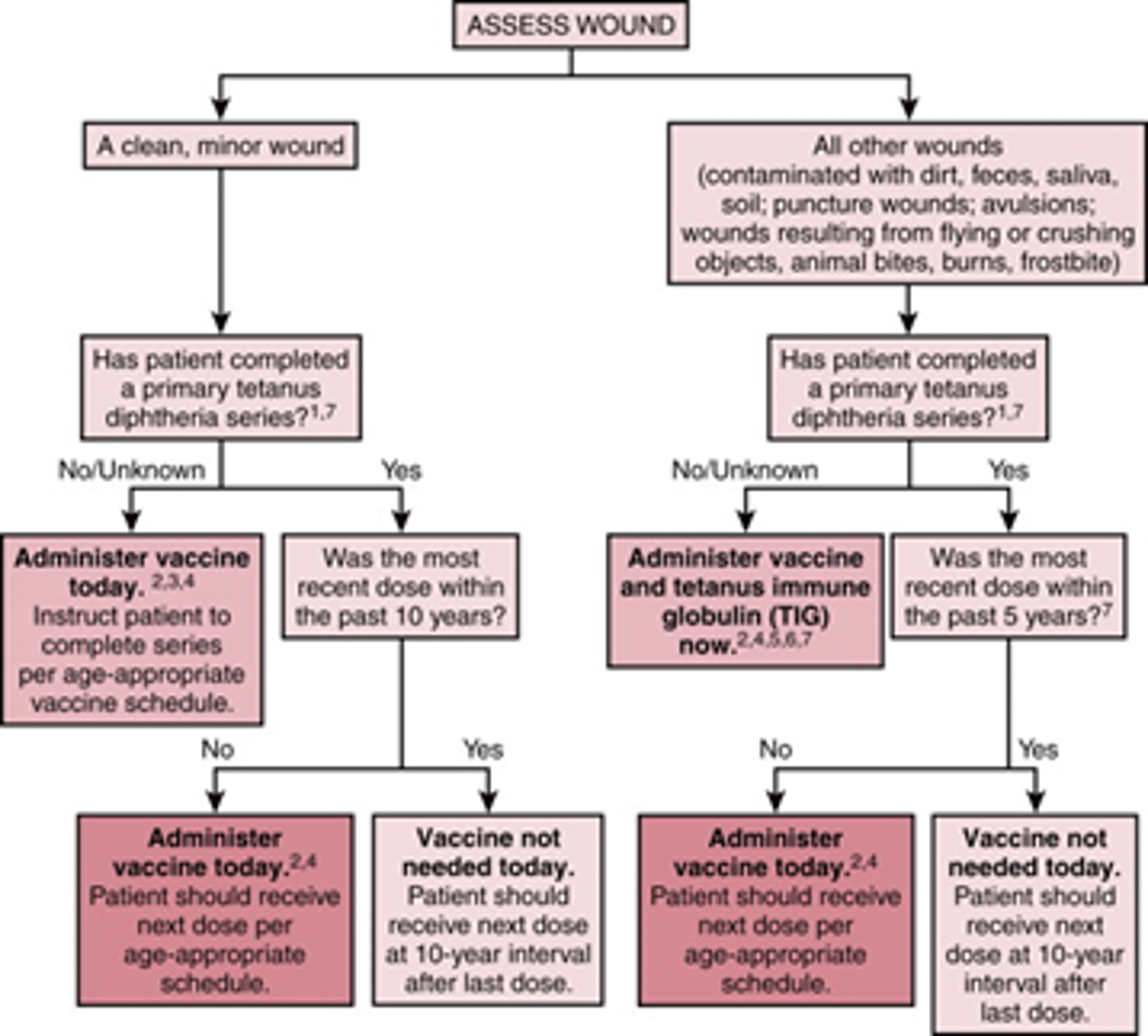
Pt comes into ER with a clean, minor wound. They are unsure if they completed their > 3 vaccine series and had their last dose a little over 10+ years ago. What should be done?
Admin vaccine today
(wouldn't have to do it if < 10 years)
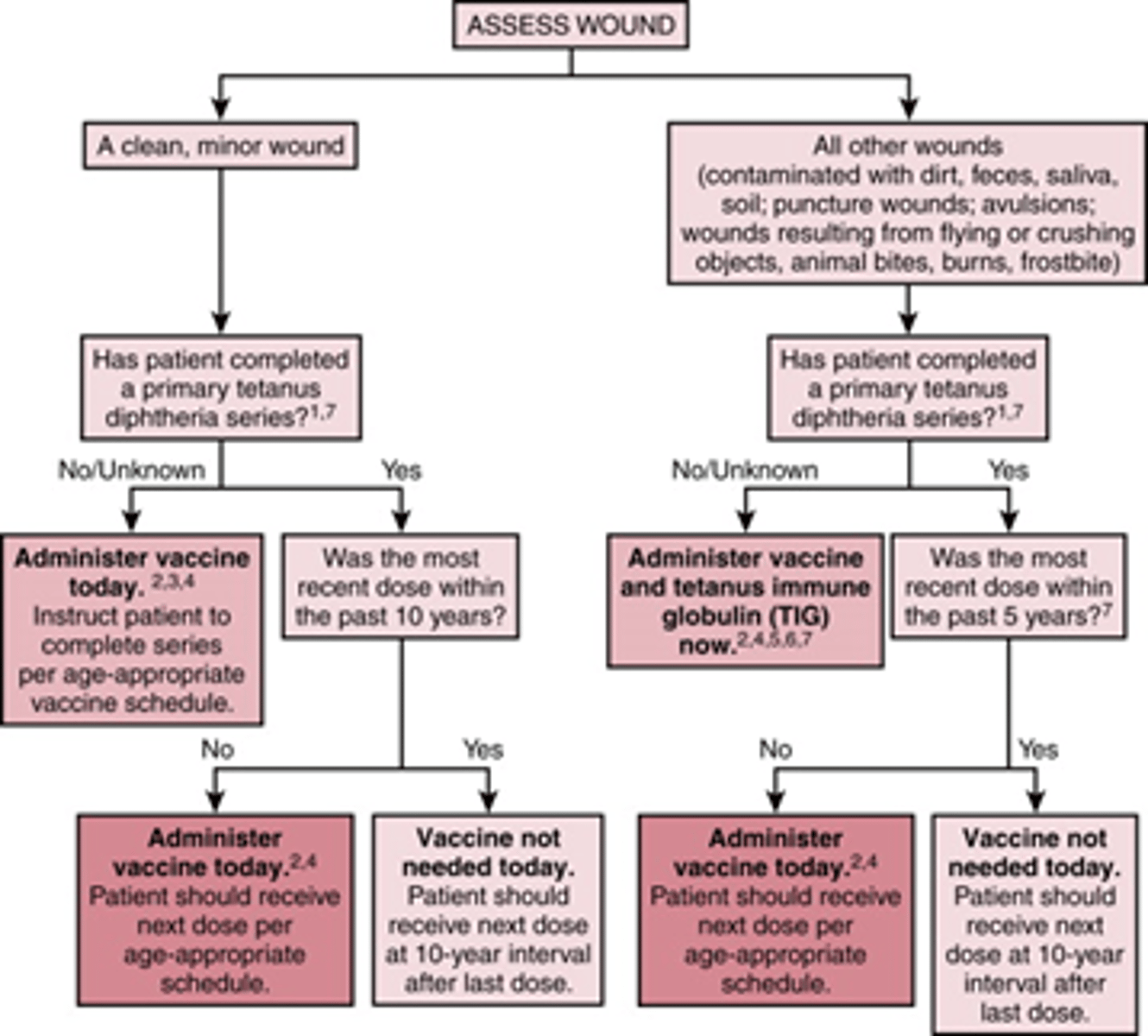
A non-tetanus prone wound (simple and clean) in an adult (19-64yo) pt with UTD immunizations does REQUIRE immunization with Tdap or Td booster IF it has been how long since completion of series?
10 years
** Tdap is recommended once a lifetime, if already received or if 65+yo, Td booster should be given
A tetanus prone wound (contaminated, etc.) in a patient with UTD immunizations does REQUIRE immunization with either Tdap or Td booster IF it has been more than how long since completion of series?
5 years
** Tdap is recommended once a lifetime, if already received or if 65yo+, Td booster should be given
T/F Most wounds do not require antibiotics
True (most are small & uncomplicated)
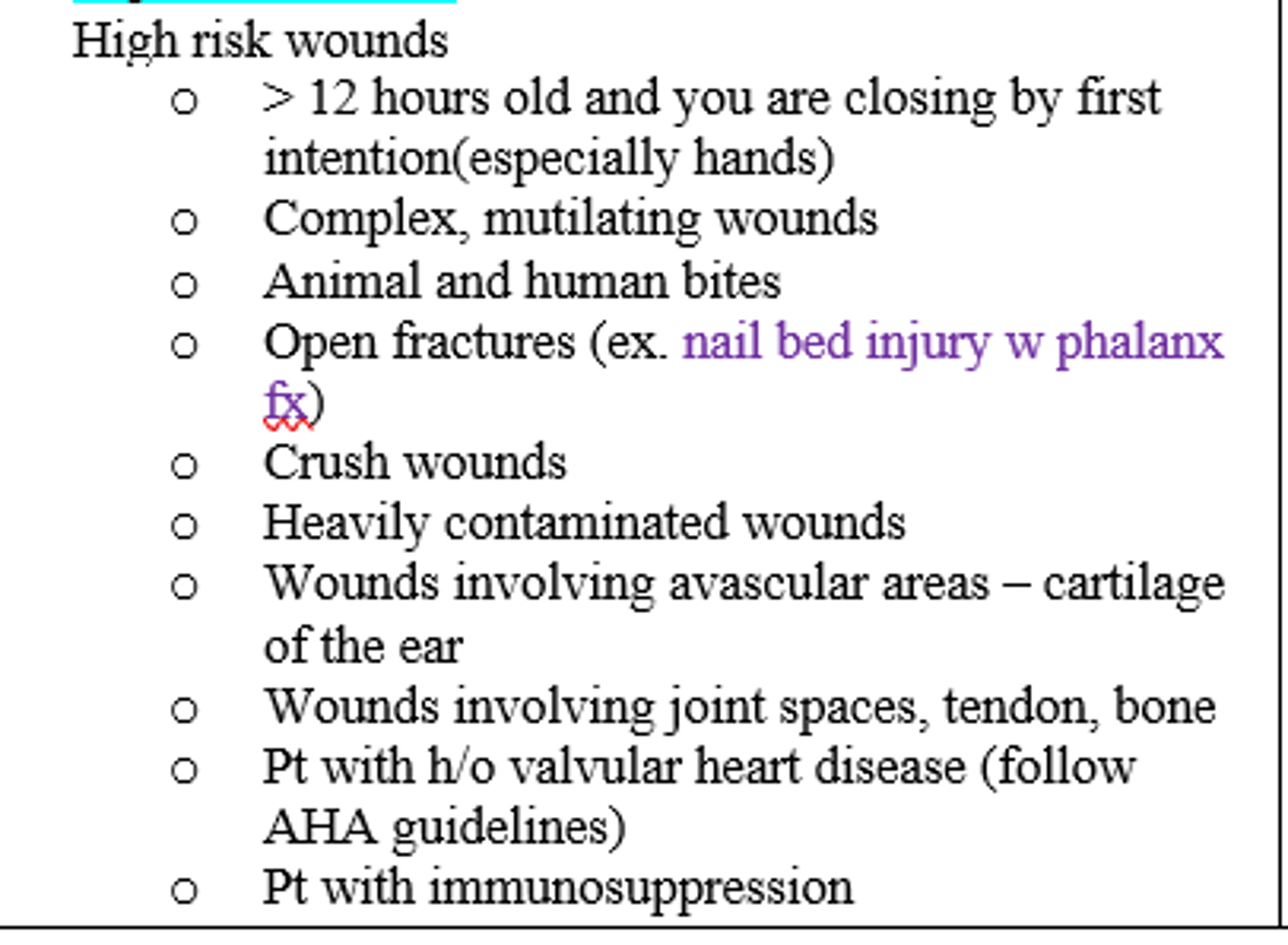
Which wounds should be considered for antibiotics?
high risk wounds (see pic)
What ABX is recommended for a contaminated dog bite wounds (high risk)?
Augmentin (Amoxicillin-clauvonate)
What ABX is recommended for contaminated NON-bite wound ?
TMP-SMX (Bactrim)
w/ Cefalexin or Clindamycin
What ABX is recommended for your patient who is tourist at Virginia Beach and sustained a foot lac while walking on the beach / ocean by stepping on a sharp sea shell (salt-water wound / concerns of Vibrio vulnificus)?
Doxycycline (broad spectrum Tetracycline)
What is the most important step in Wound closure?
Irrigation, irrigation, irrigation!
When irrigating a wound prior to closure you should be using minimally _________ mL and ~_____PSI (but rule of thumb to use ____mL/cm)
- 250-500;
- 5-7;
- 100
You are repairing a wound over a lip of a moustached patient. What should be done to keep hair out of the lac while suturing?
- Clean hair and utilize lubricant or abx ointment to keep out of the way
- avoid shaving hair d/t increase incidence of infection
- FYI NEVER SHAVE AN EYEBROW
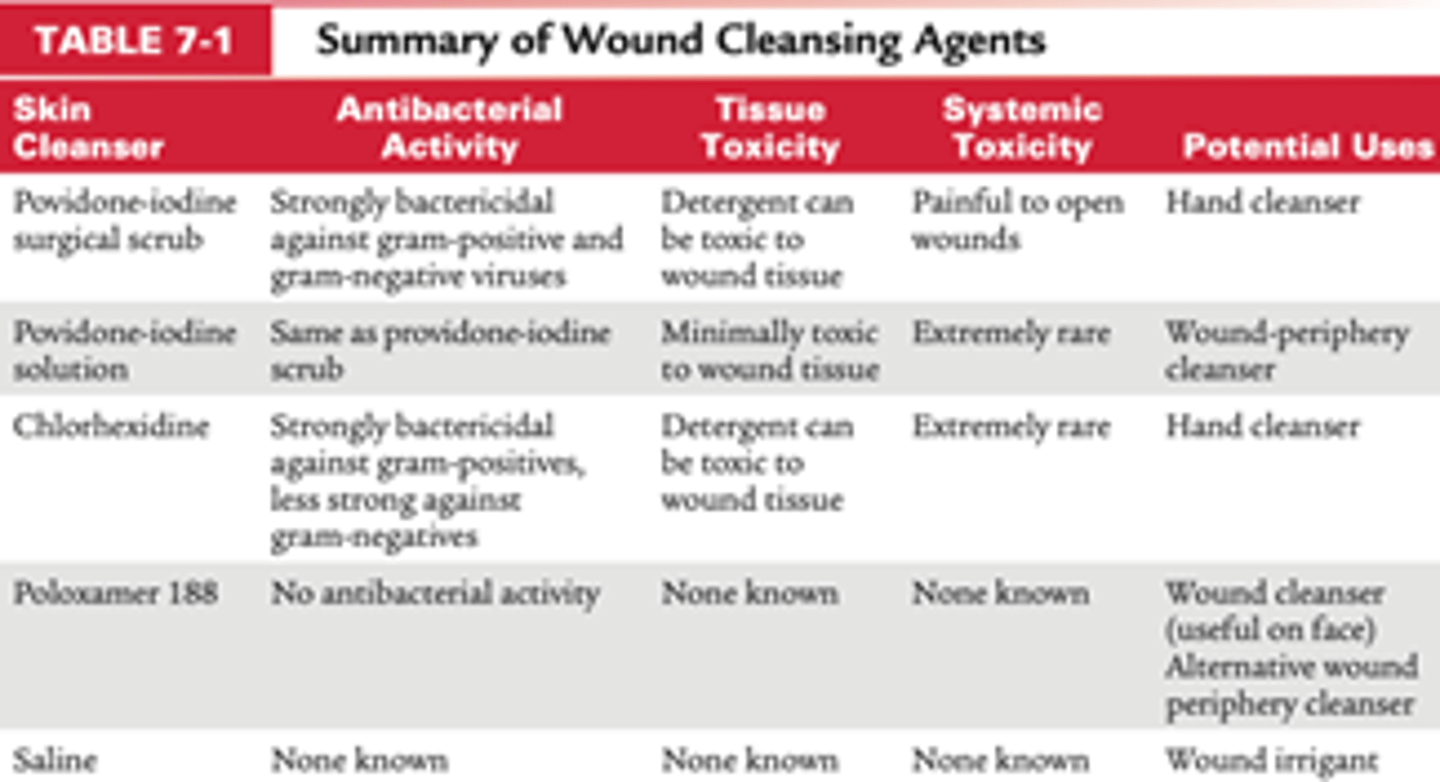
Which wound cleansing agents have antibacterial activity and also known to be somewhat toxic to wound tissues but rarely cause systemic toxicity (bactericidal against gram positive and gram negative)?
- Povidone-Iodine / Betadine (surgical scrub and solution)
- Chlorhexidine / Hibacleanse
Wound Closure procedure:
1) confirm UTD on immunizations
2) confirm timing w/n golden period
3) anesthesia
4) wound cleansing
5) Irrigation, irrigation, irrigation!
6) switch gloves from non sterile to sterile
7) Exploration (Neurovasc. status, FB, etc.)
8) Debridement (of subQ fat)
9) suture
Which layer of injured skin can be liberally debrided before suturing a wound: epidermis, dermis, or subcutaneous fat?
Subcutaneous fat
*spare as much of the other layers as much as possible
Scar visibility is minimized when it runs ______ to skin tension lines / Langer Lines, but is more prominent when placed ________ to them.
- parallel
- perpendicular/oblique
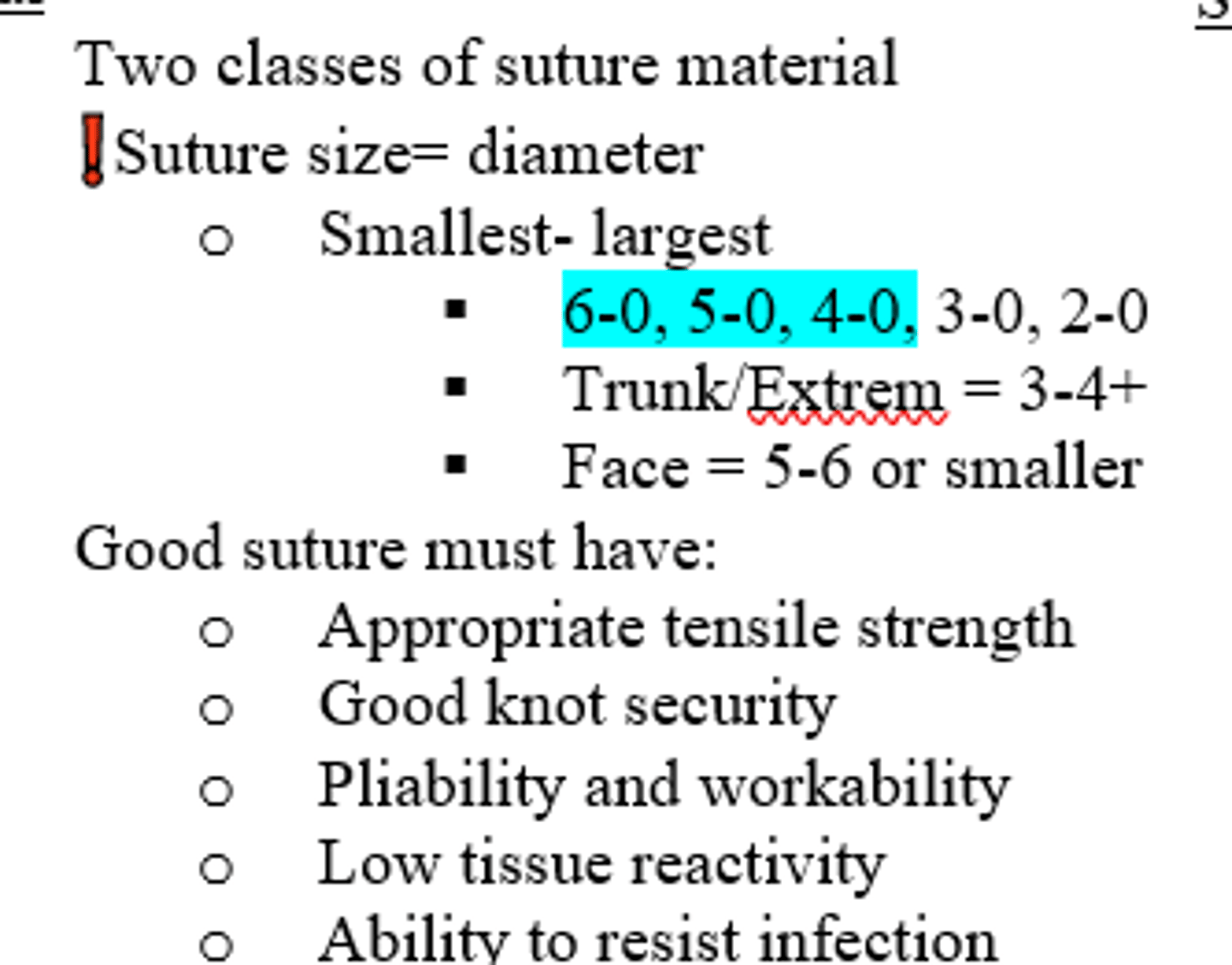
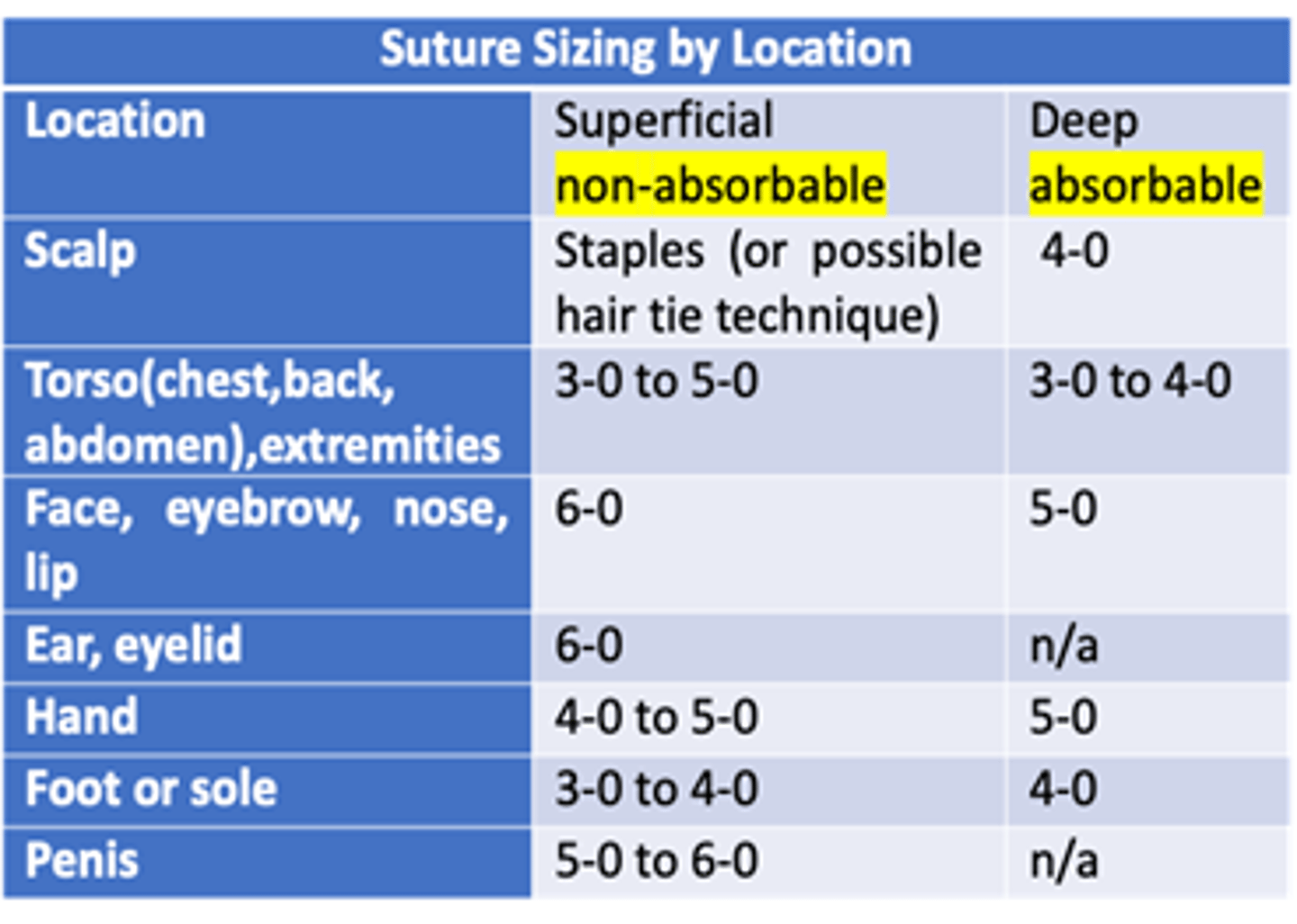
Which size suture is best for the face due to its good cosmetic outcome?
5-0 to 6-0 or smaller (bigger the #, the smaller the diameter needle)
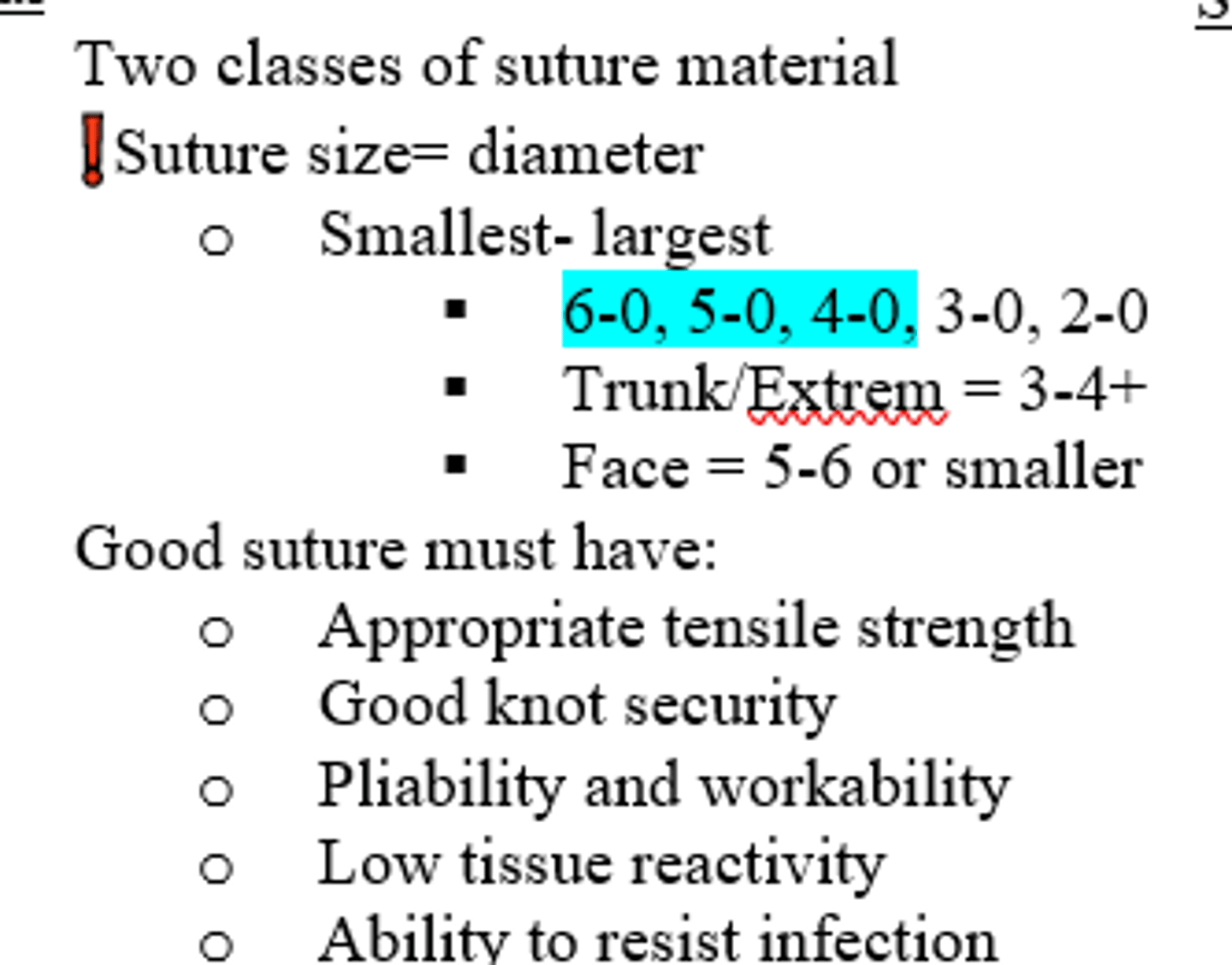
Which size suture is best for the trunk/extremities?
3-0 to 5-0 or larger (smaller the #, the larger the diameter needle)
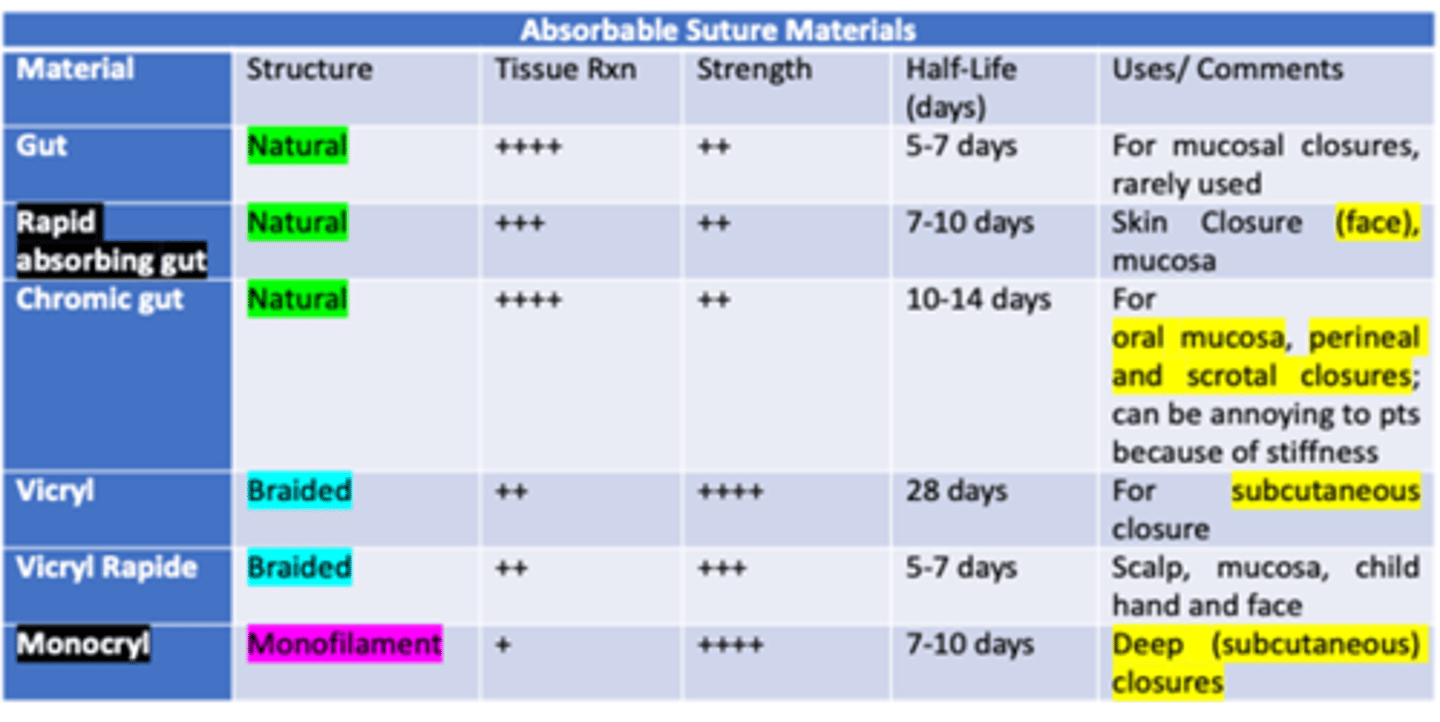
Which types of sutures causes a more inflammatory process, absorbable or non-absorbable?
Absorbable
Which type of Absorbable suture is best for skin closure of the face, oral mucosa, lips, and tongue, because it heals the fastest?
Rapid absorbing gut
- Natural structure / monofilament
- severe tissue rxn
- moderate strength
- t1/2: 7-10 days
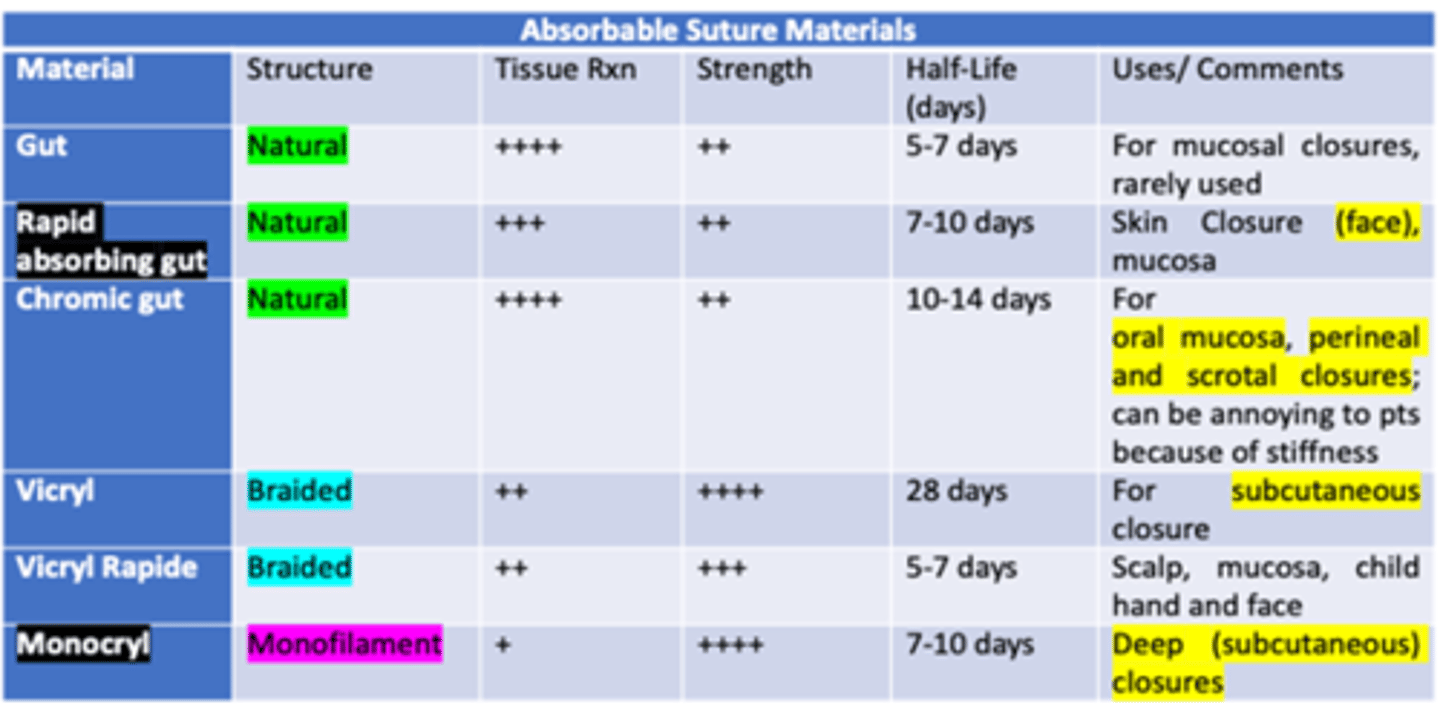
Which type of Absorbable Monofilament suture is best for deep (subcutaneous) closure, has the least amount of tissue reaction, and greatest amount of strength?
Monocryl
- low tissue rxn
- great strength
- t 1/2: 7-10 days
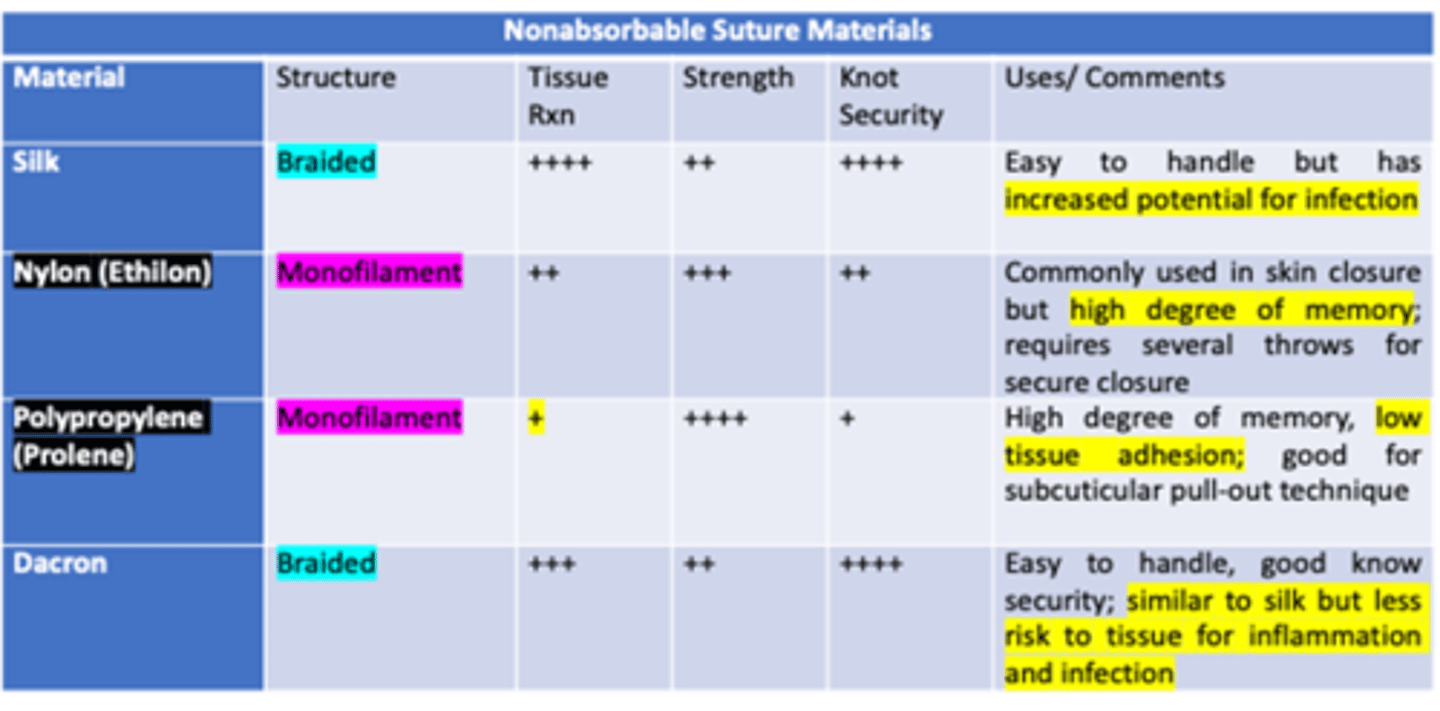
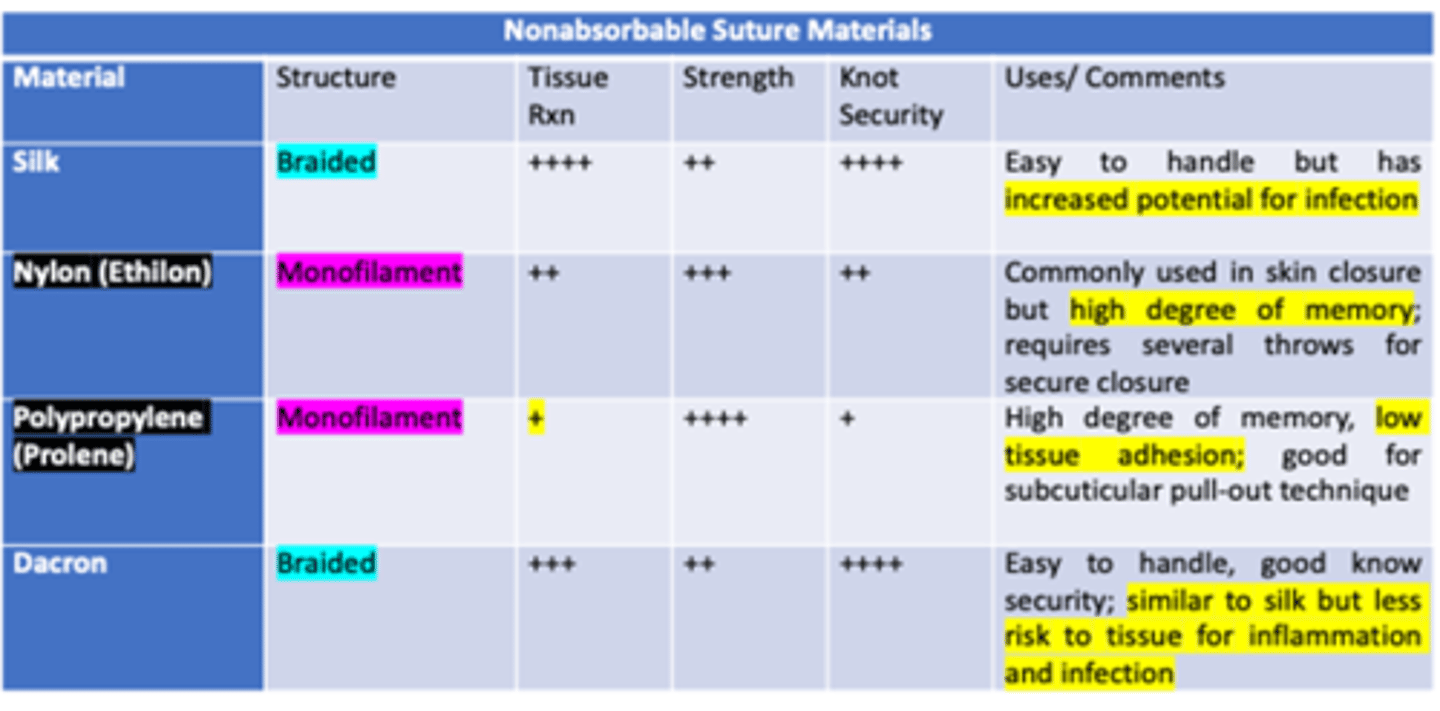
Which type of non-absorbable monofilament suture has the least amount of tissue reaction & knot security, but the highest strength?
Prolene / Polypropylene
- commonly used
- high memory
- low tissue adhesion, glides well
- good for subcuticular pull-out technique (i.e. eyebrow)
Superficial wounds should be given __________ sutures and deep should be given ___________
non-absorbable; absorbable
Which type of non-absorbable monofilament suture has equal tissue reaction & knot security, and almost a high amount of strength?
Nylon / Ethilon
- commonly used
- high degree of memory
- requires several throws for secure closure
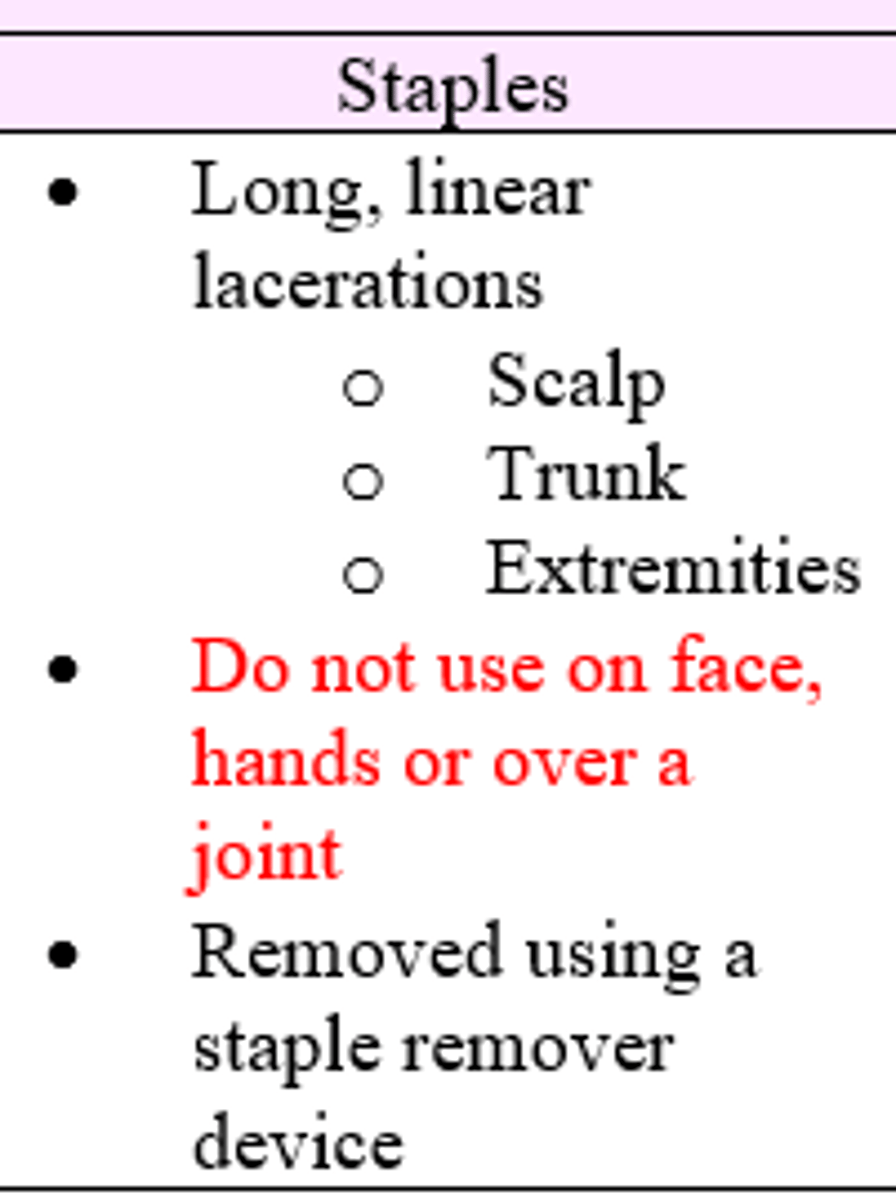
What can be done to close a wound on the scalp?
Staples or possible hair tie technique superficially; 4.0 if deep
Staples & microporous tape have (more/less) tissue reactivity than polypropylene and nylon sutures
less
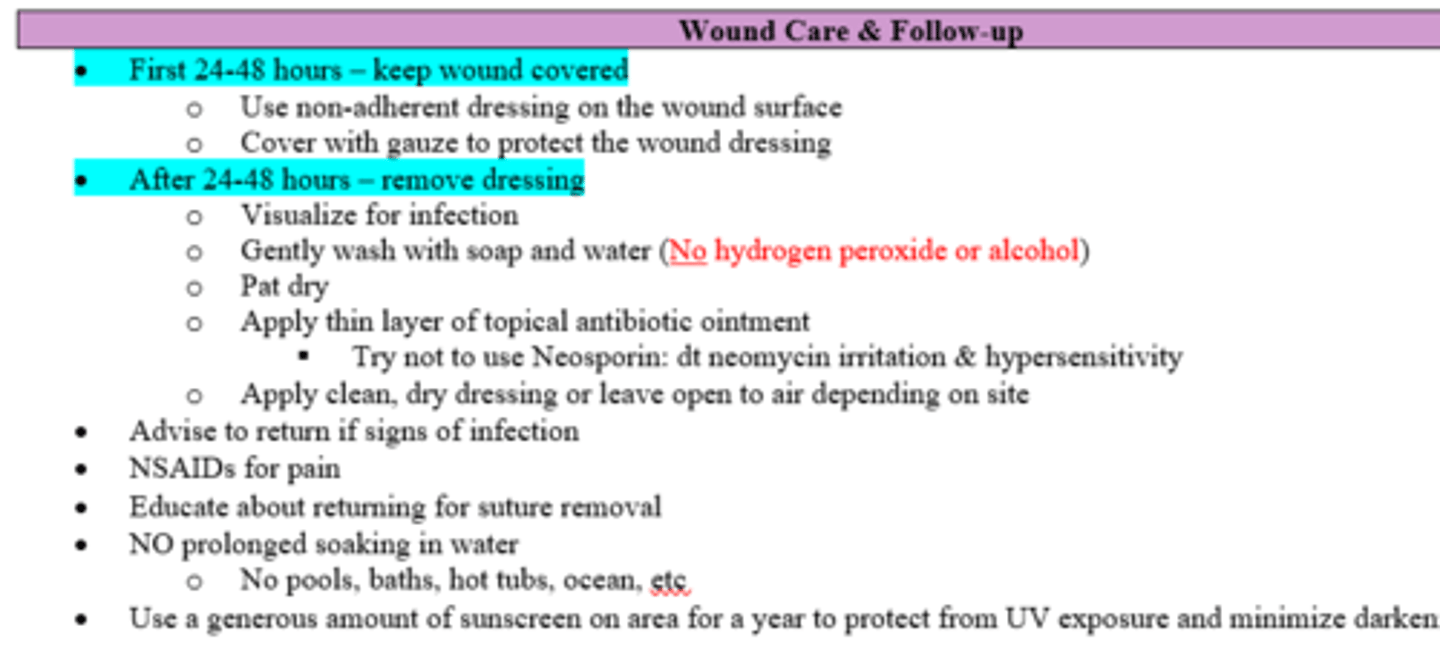
When should the wound be covered and when should dressing be removed?
First 24-48h; after 24-48h
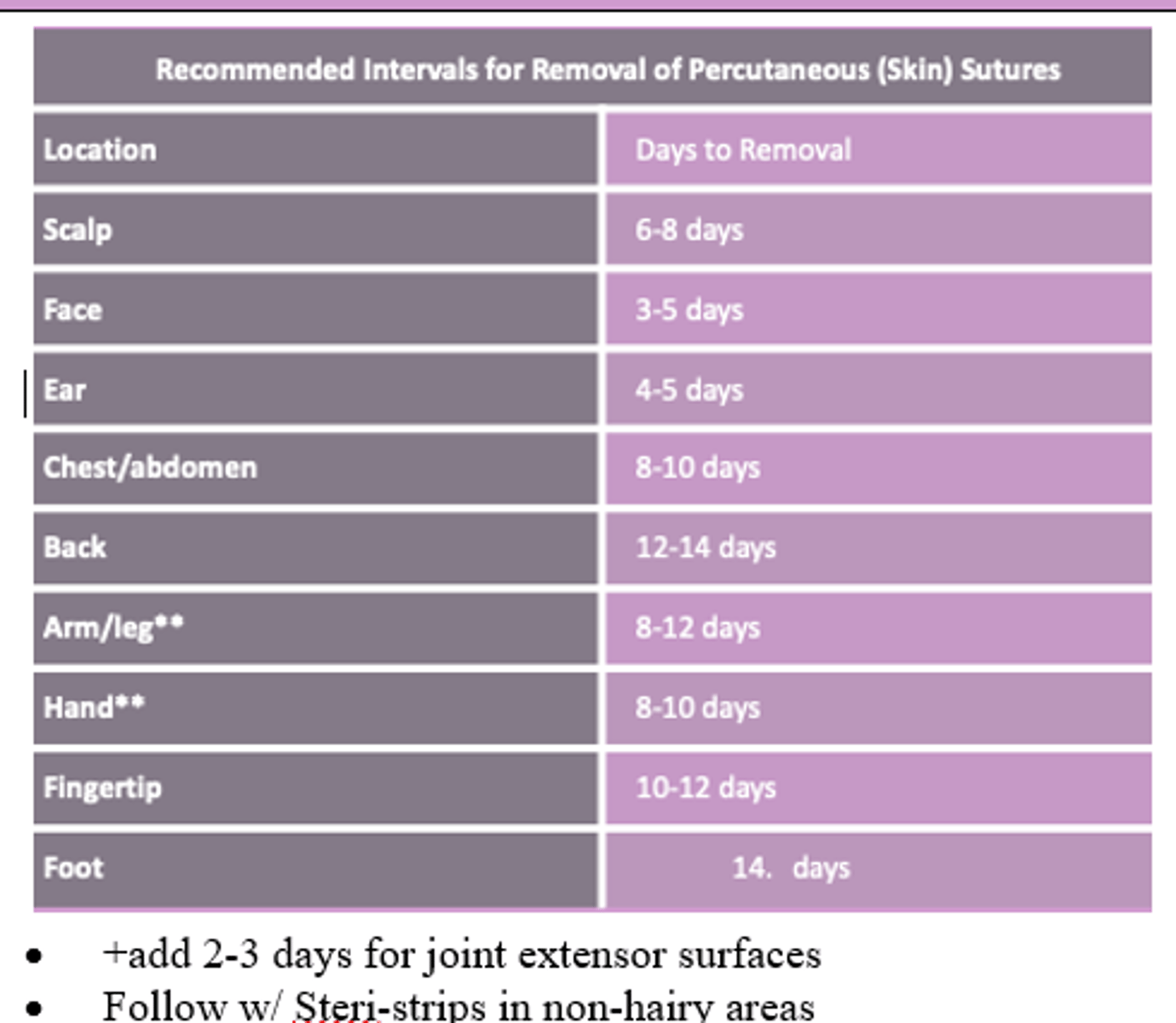
Face, ear, and scalp wounds should have sutures kept in (shorter/longer) vs. chest, abdomen, back, and extremities?
Shorter (~3-8 days)
**trunk/extremeties (8-14 days)
What surfaces should not be closed with staples?
face, hands or over joint
T/F Glued wounds have decreased tensile strength vs. sutured wounds by day 7
False (no difference by day 7)
What alternative for sutures is good in elderly or steroid dependent patients who get superficial straight lac under little tension?
Wound tape
You should suture (towards/away from) you
towards
What are the various types of sutures and suture needles?
what are the principles to follow when to choosing what type of suture and suture needle for specific wounds?
- Use smallest diameter acceptable (the bigger there # the smaller the diameter)
- keep interrupted sutures properly spaced
- keep # of sutures to a minimum
- "halving"/bisecting technique
What are the rationale and principles of safe needle handling?
- Limit handling
- Limit passing/ Announce moves ("sharp down")
- Clean after self
What are the various suturing techniques?
- Simple
- Continuous
- Interrupted
- Subcuticular
- Vertical / Horizontal Mattress
What are the general principles of knot tying?
- Simple is better
- Never less than 2 knots
- if multifilament = 2 knots (4 throws)
- if monofilament = 3 knots (6 throws)
- Avoid "sawing" through tissue
What are the 3 methods of tying knots?
- Instrument (simple vs. surgeon's throw)
- Two-hand
- One-Hand
How many throws is 1 square knot?
2 throws
- 2 knots = 4 throws
- 3 knots = 6 throws
Things to include on a wound closure procedure note:
- Date
- consent
- time wound open
- MOI
- Anatomic location/associated injuries
- Length and Depth
- Wound classification (clean, dirty, etc.)
- cleansing method/irrigation volume and type
- anesthesia and method
- suture size and type
- Closure method/technique
- Dressing method
- pt response / complications
- disposition/follow up
- pt education instructions
- signature