APEX FCs Combined
1/1858
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
1859 Terms
which muscle tense & relax the vocal cords?
CricoThyroid :Cords Tense/Elongate
SLN-ext
ThyroaRytenoid: They Relax/Shorten and ADD/Narrow
which muscles abduct + adduct the VC?
Lateral CricoArytenoid = "Let's Close Airway"
ADD/narrow
Posterior CricoArytenoid = "Please Come Apart"
ABD/widen
sensory innervation of the upper airway
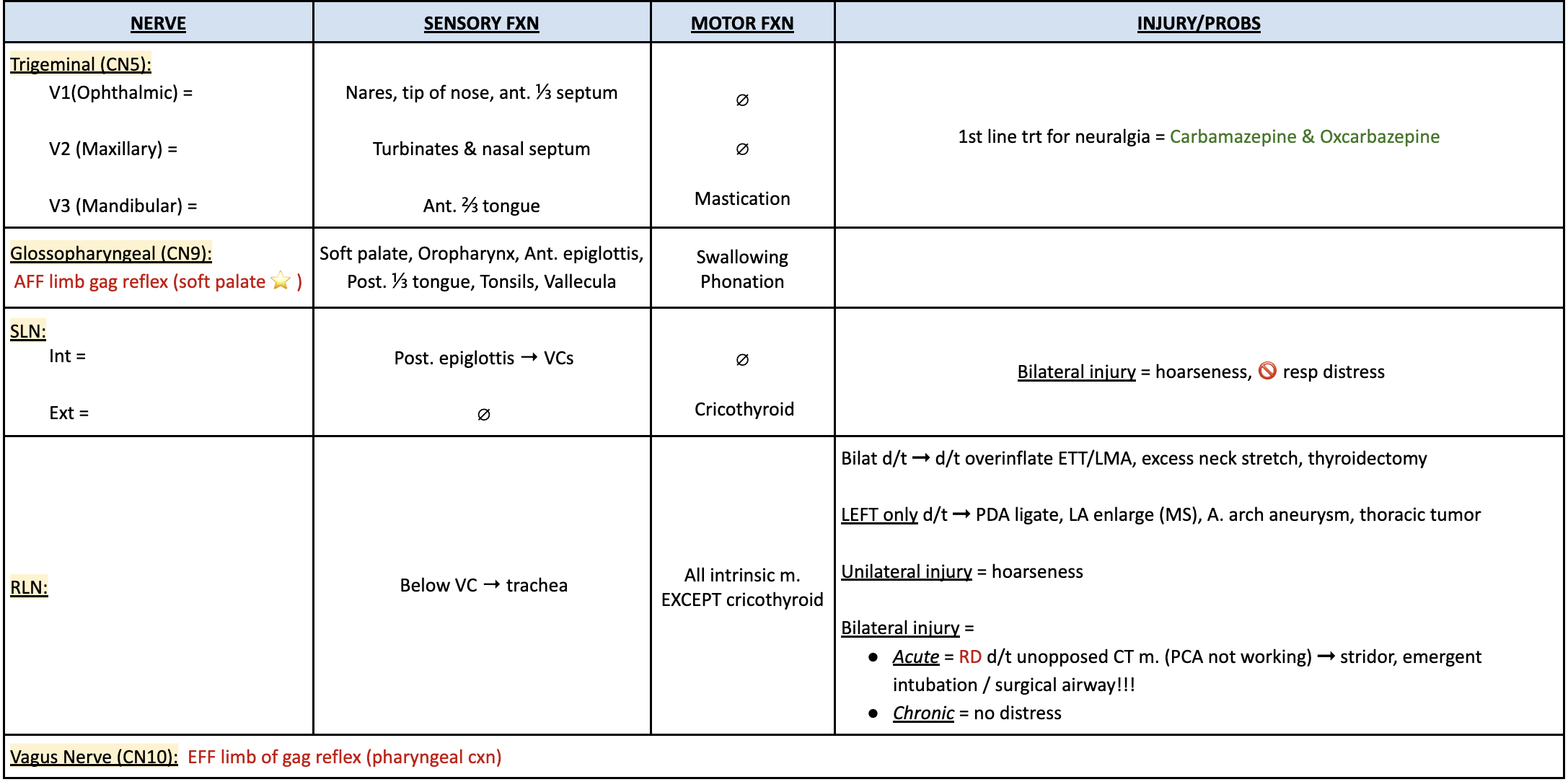
Bilat RLN injury is d/t?
overinflation of cuff
excessive neck stretch
neck sx (thyroidectomy)
LEFT sided RLN injury is d/t?
PDA ligation
LAE (MS)
aortic arch aneurysm
thoracic tumor
3 airway blocks: key landmarks, techniques, and risks?
GP = base of palatoglossal arch (ant. tonsillar pillar), 0.25-0.5 cm deep, 1-2 ml
risk sz if intracarotid injection
SLN = inf. border of greater cornu (hyoid), 1 ml outside THM, 2 ml deep to THM
aspirate air = too deep
Transtracheal (RLN) = CTM, caudally, 3-5 ml → pt coughs
what is the risk of benzocaine spray for topical anesthesia for UAW?
met-Hgb-nemia → methylene blue 1-2 ml/kg
what spinal level is the adult larynx?
C3-C6
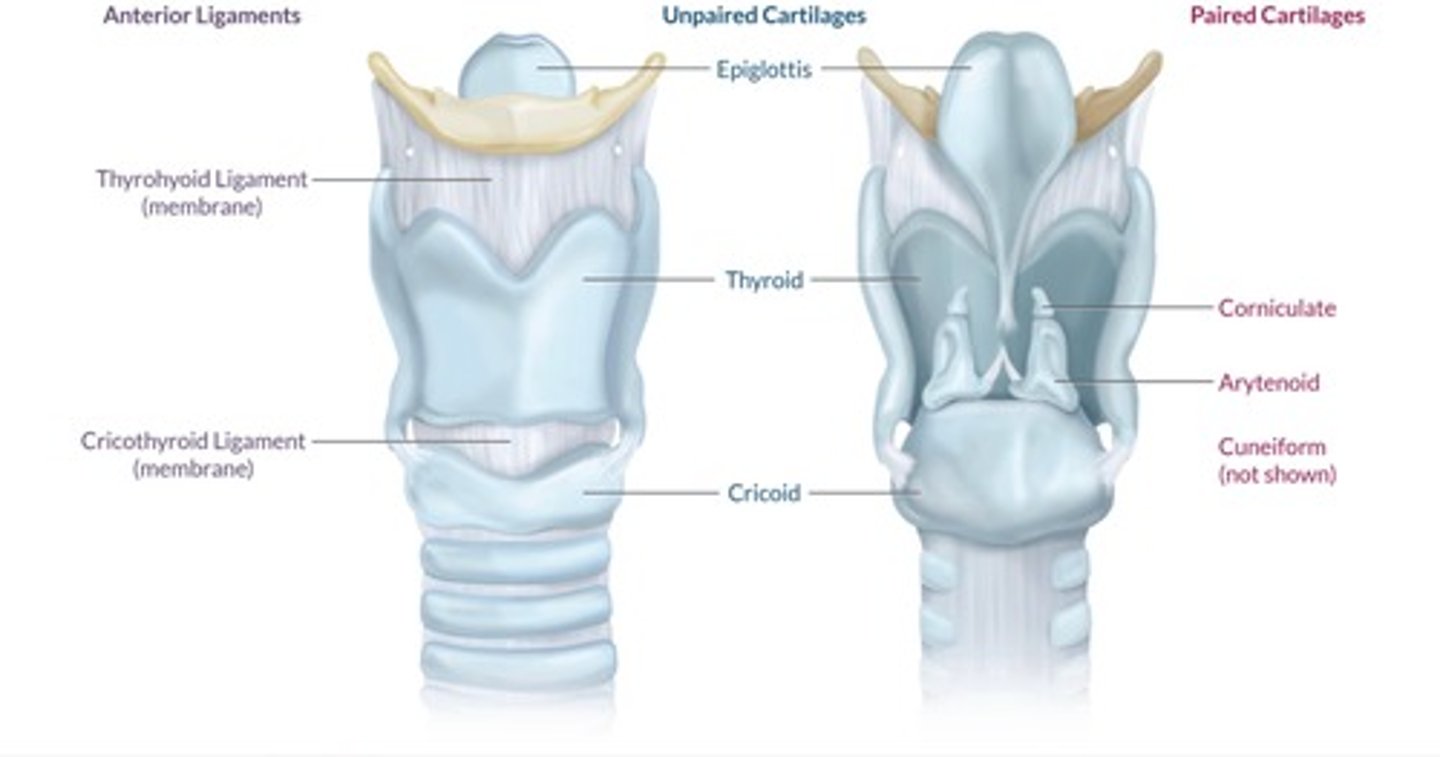
what are the 3 paired and 3 unpaired cartilages of the larynx?
Paired = arytenoids, corniculate, cuneiform
Unpaired = epiglottis, thyroid, cricoid
adult vs peds larynx anatomy?
adult = cylinder
narrowest → glottic opening
peds < 5yr = funnel
narrowest fixed → cricoid ring
narrowest dynamic → VCs
laryngospasm nerve innervation?
What are 2 significant consequences of laryngospasm?
Hypoxia
NPPE
What is the treatment for laryngospasm?
100% FiO2
Remove noxious stimulation
Deepen anesthesia
CPAP 15-20cmH2O
Open AW (head extension, chin lift)
Sch
Regarding Sch:
infants & small children should receive atropine (0.02mg/kg) w/Sch
no IV access: fastest onset - submental
no IV access & pt cannot have Sch: Roc is only other NMB that can be given IM
Describe how the respiratory muscles function during the breathing cycle.
Contraction of inspiratory muscles ↓ thoracic P & ↑ thoracic V (Boyle's law)
Inspiration:
diaphragm & external intercostals contract during inspiration (tidal breathing)
diaphragm ↑ superior-inferior dimension of the chest
external intercostals ↑ anterior-posterior diameter
accessory muscles include the SCM & scalene muscles
Exhalation:
exhalation usually passive, driven by recoil of chest wall
abd musculature (rectus/transverse abdominis, internal/external obliques) assist in active exhalation
internal intercostals serve a secondary role in active exhalation
exhalation becomes active when MV ↑ or in Pts w/ lung disease (COPD)
forced exhalation is required to cough & clear AW of secretions
What is the difference between minute ventilation (Ve) and alveolar ventilation (VA)?
Ve = Vt x RR
alveolar ventilation (VA): fraction of Ve that is available for gas exchange - removes anatomic dead space from the MV equation.
VA = (Vt - anatomic dead space) x RR
VA is directly proportional to CO2 production
VA is indirectly proportional to PaCO2
Define the 4 types of dead space.
Anatomic Vd: Air confined to the conducting AW
Alveolar Vd: Alveoli that are ventilated but not perfused
Physiologic Vd: Anatomic Vd + Alveolar Vd
Apparatus Vd: Vd added by equipment
Provide an example for each type of dead space.
Anatomic Vd: nose/mouth → terminal bronchioles
Alveolar Vd: ↓ pulm BF (↓ CO)
Physiologic Vd: anything that ↑ anatomic or alveolar Vd
Apparatus Vd: FM, HME, limb of circle system if incompetent valve present
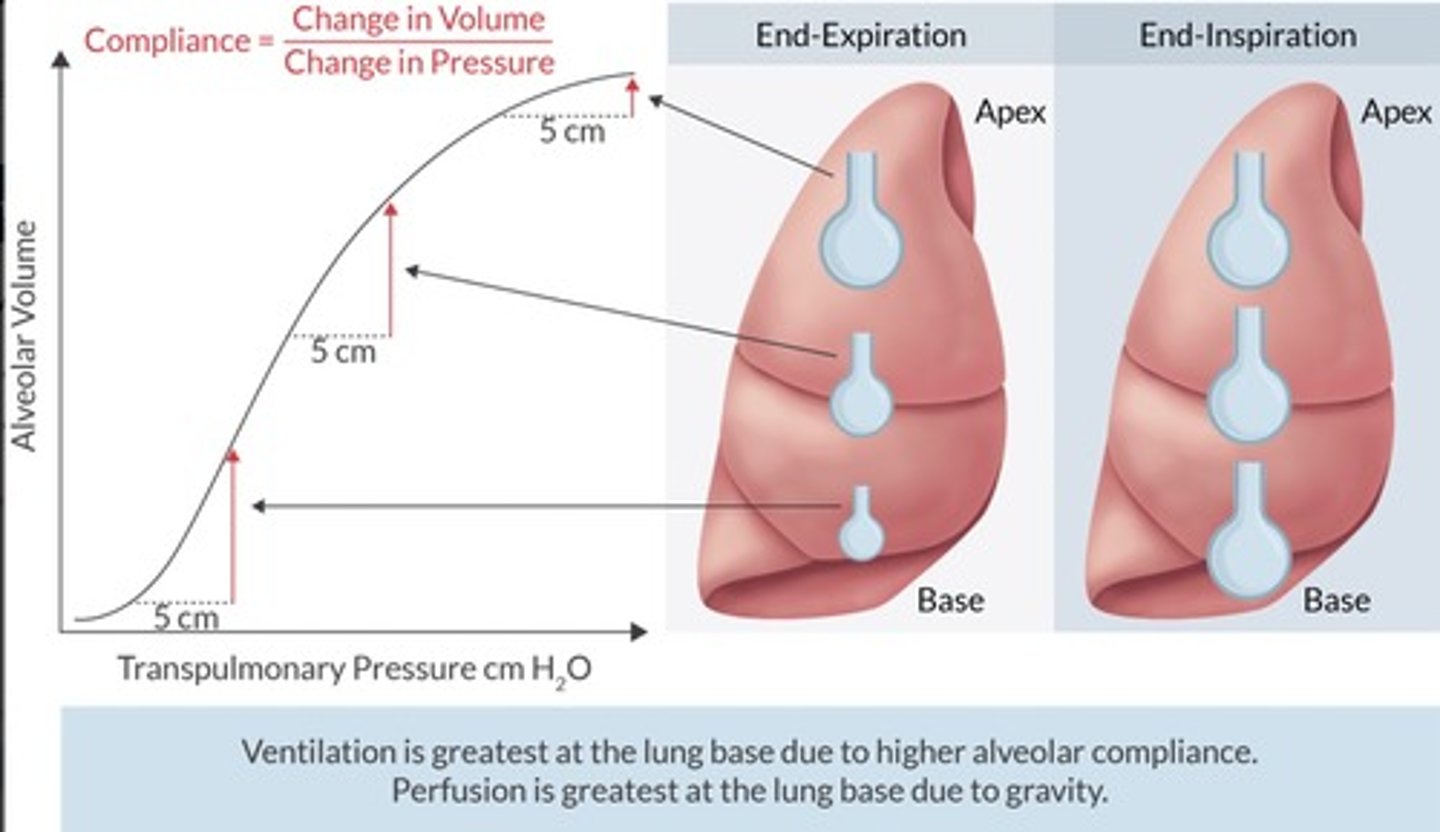
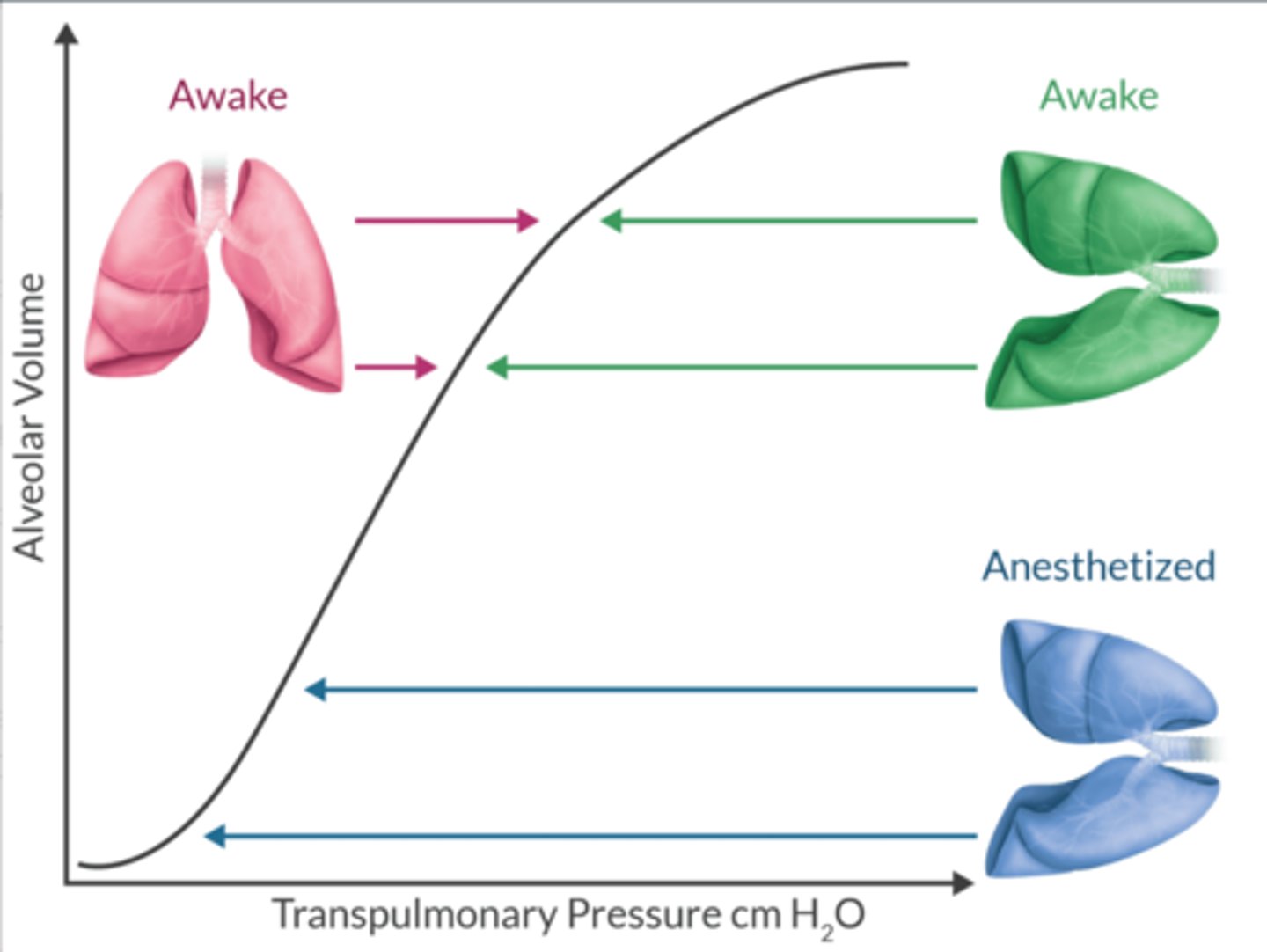
What does the alveolar compliance curve tell you?
VA is a function of alveolar size & its position on the curve.
Best ventilated alveoli are most compliant (steep slope of the curve)
Poorest ventilated alveoli are least compliant (flat portion of the curve)
What does the V/Q ratio represent?
Ratio of ventilation to perfusion (Ve/CO)
Normal Ve = 4L/min
Normal CO = 5 L/min
Normal V/Q ratio = 0.8
Absolutes:
Dead space: V/Q = infinity (10/0 = infinity)
Shunt: V/Q = 0 (0/10 = 0)
V/Q mismatch occurs when the ratio is disturbed.
If > 0.8 → dead space
If < 0.8 → shunt
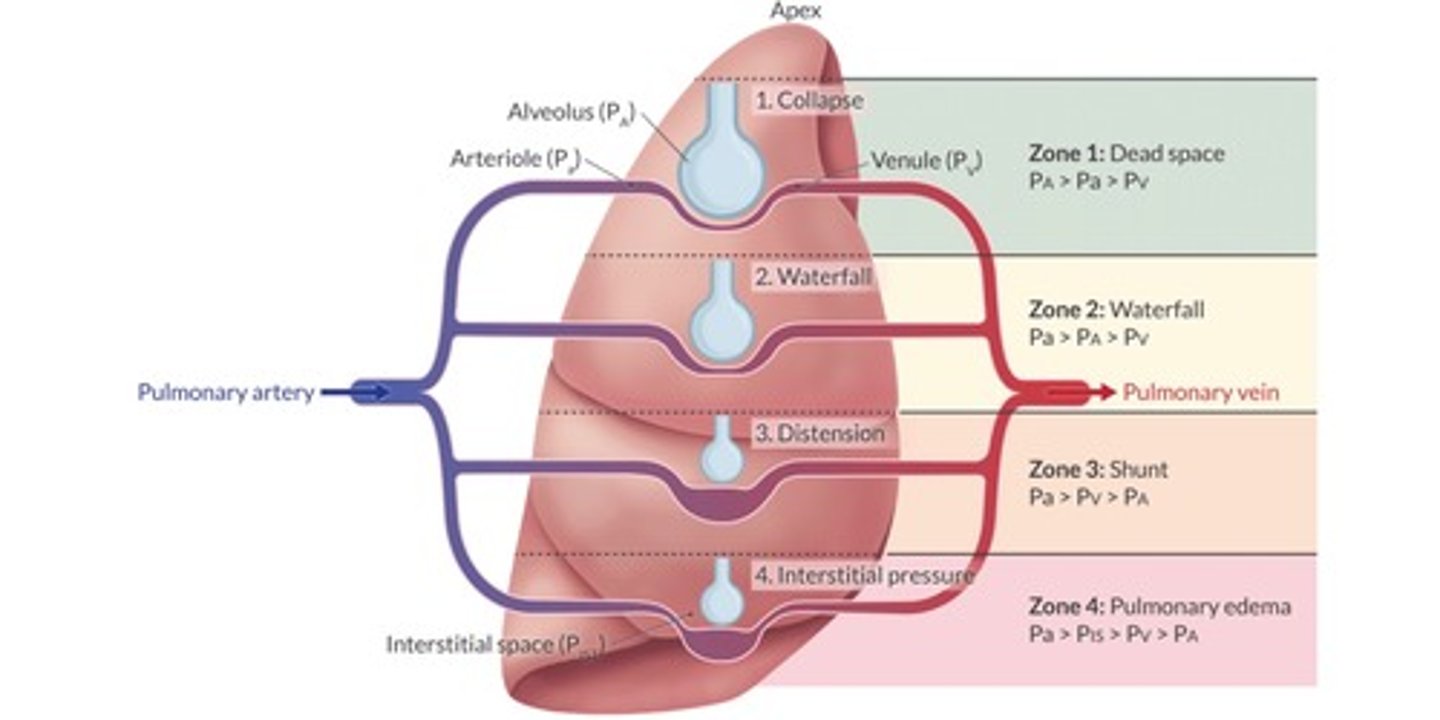
Define the West zones of the lung.
Zone 1
PA > Pa > Pv
dead space
Zone 2
Pa > PA > Pv
waterfall, normal physiology
Zone 3
Pa > Pv > PA
shunt
Zone 4
Pa > Pist > Pv > PA
pulmonary edema
Recite the alveolar gas equation.
Hypoventilation can → ↑ CO2 & ↓ O2.
Explains supp O2 reverses hypoxemia, but does nothing to reverse hypercarbia.
VA = FiO2 x (Pb - PH2O) - (PaCO2 / RQ)
Pb = atmospheric pressure
PH2O = 47mmHg
RQ = Respiratory quotient = 0.8
RQ = (CO2 elimination / O2 consumption) = (200mL / 250mL)
Alveolar O2 in healthy adult Pt breathing RA at sea level is ~ 105.98mmHg
What is the A-a gradient?
Difference between alveolar (PAO2) + arterial oxygen (PaO2).
Helps us diagnose the cause of hypoxemia by quantifying the amount of venous admixture
NORM = < 15mmHg
What factors ↑ the A-a gradient?
High FiO2
Aging
Vaso-d’s
R → L shunt
Diffusion limitation
List the 5 causes of hypoxemia.
Normal A-a gradient
1. Reduced FiO2: not enough O2 in inspired gas
2. Hypoventilation: inadequate air transfer in & out of lungs
Increased A-a gradient
3. Diffusion limitation: capillary thickening hinders O2 diffusion
4. V/Q mismatch
5. Shunt: pulmonary blood bypass alveoli
Which causes of hypoxemia are fixed with supplemental O2?
YES:
1. Reduced FiO2
2. Hypoventilation
3. Diffusion limitation
4. V/Q mismatch
NO
1. Shunt
w/shunt there is no way for O2 to access the pulmonary capillary. All the other causes will allow O2 to transfer b/t the alveolus and the pulmonary capillaries.
Define Inspiratory Reserve Volume + give its reference value.
V that can be forcibly inhaled after a tidal inhalation
3000 mL
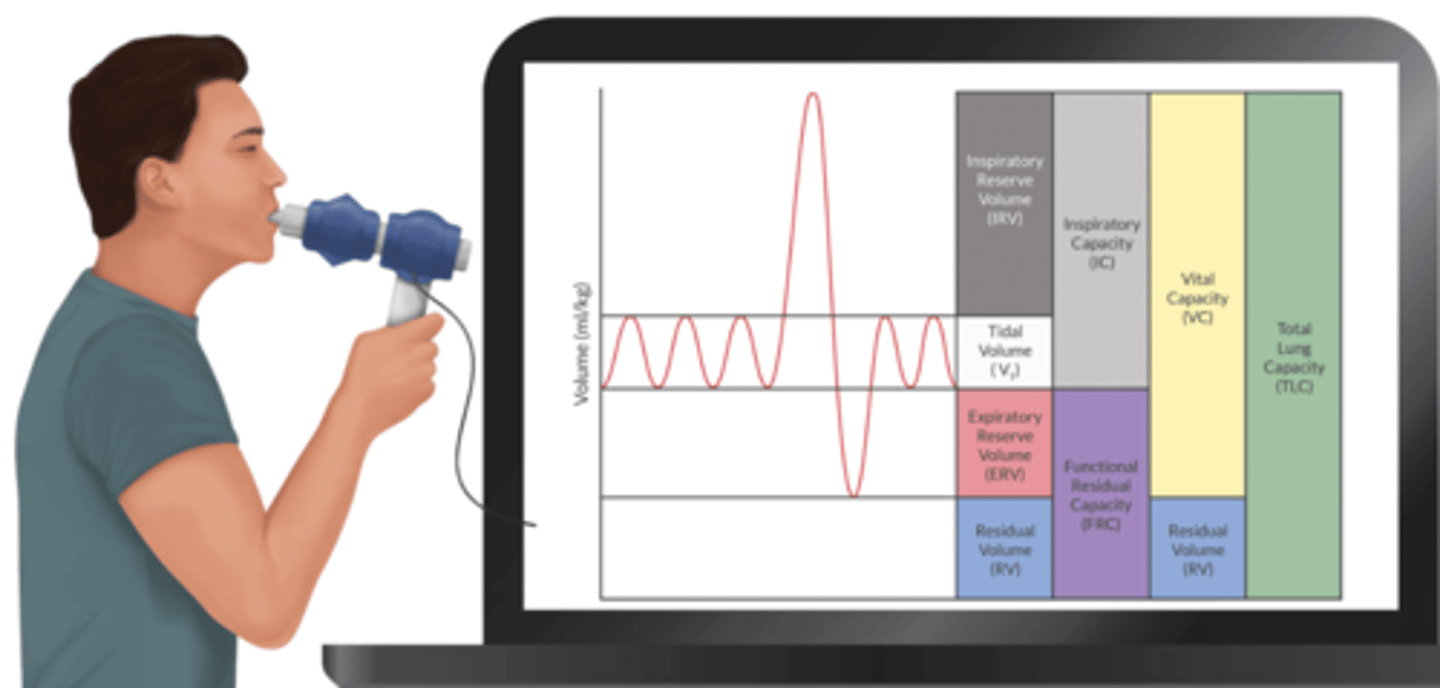
Define Tidal Volume and give its reference value.
V that enters + exits lungs during tidal breathing
500 mL
Define Expiratory Reserve Volume + give its reference value.
V that can be forcibly exhaled after a tidal exhalation
1100 mL
Define Residual Volume + give its reference value.
V that remains in the lungs after a complete exhalation
1200 mL
Define Closing Volume + give its reference value.
V above RV where the small a.w. begin to close
Variable
~ 30% TLC @ age 20
~ 55% TLC @ age 70
Define TLC + give its reference value.
IRV + TV + ERV + RV
5800 mL
Define Vital Capacity + give its reference value.
IRV + TV + ERV
4500 mL
Define Inspiratory Capacity + give its reference value.
IRV + TV
3500 mL
Define FRC and give its reference value.
RV + ERV
V at end expiration
2300 mL
Define Closing Capacity + give its reference value.
RV + CV
Absolute V of gas contained in lungs when small a.w. close
Variable
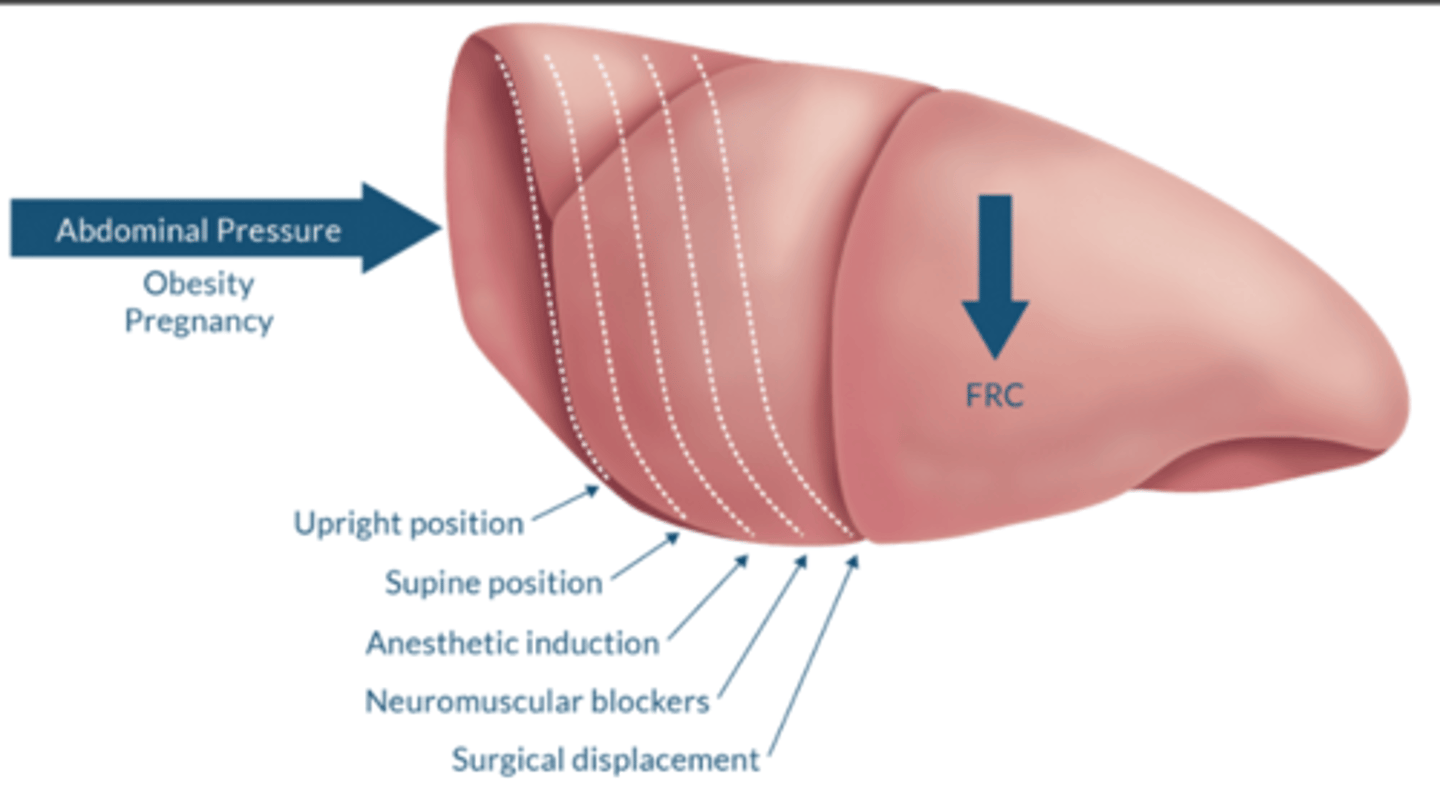
What factors influence FRC?
↓ FRC→ ↑ intrapulmonary shunt (zone 3). PEEP acts to restore FRC by ↓ zone 3.
↑ FRC: COPD or any condition that causes air-trapping
↓ FRC: obesity, pregnancy, supine position, anesthetic induction, NMB, surgical displacement
-↓ lung expansion or compliance
Why can't spirometry measure FRC?
FRC = RV + ERV (35mL/kg)
Conventional spirometry can't measure FRC because it includes RV.
What tests can measure FRC?
Indirectly by:
-nitrogen washout
-helium wash in
-body plethysmography
What increases Closing Volume?
"CLOSE-P"
COPD
LVF
Obesity
Surgery
Extreme age
Pregnancy
State the equation + normal value for oxygen-carrying capacity.
CaO2 = (1.34 x Hgb x SaO2) + (PaO2 x 0.003)
Normal: 20 mL O2/dL
State the equation and normal value for oxygen delivery.
DO2 = CaO2 x CO x 10
Normal: 1000 mL O2/min
Discuss the factors that alter the oxyhemoglobin dissociation curve.
Tells us how Hgb binds to oxygen.
Normal P50 is 26.5mmHg.
Left shift (love) - ↑ affinity
occurs in the lungs
↑ pH
↓ temperature
↓ 2,3 DPG
↓ CO
↓ [H+]
↑ HgbMet
↑ HgbCO
↑ HgbF
Right shift (release) - ↓ affinity
occurs near metabolically active tissue
↓ pH
↑ temperature
↑ 2,3 DPG
↑ CO
↑ [H+]
![<p>Tells us how Hgb binds to oxygen. </p><p>Normal P50 is 26.5mmHg. </p><p>Left shift (love) - ↑ affinity </p><p>occurs in the lungs</p><p>↑ pH</p><p>↓ temperature </p><p>↓ 2,3 DPG</p><p>↓ CO </p><p>↓ [H+]</p><p>↑ HgbMet</p><p>↑ HgbCO </p><p>↑ HgbF</p><p>Right shift (release) - ↓ affinity</p><p>occurs near metabolically active tissue </p><p>↓ pH </p><p>↑ temperature </p><p>↑ 2,3 DPG</p><p>↑ CO</p><p>↑ [H+]</p>](https://knowt-user-attachments.s3.amazonaws.com/5fe4557e-dc1d-4c00-9086-57e03875e54f.png)
How is carbon dioxide transported in the blood?
-Bicarbonate = 70%
-Bound to hemoglobin = 23%
-Dissolved in the plasma = 7%
What does the rxn that converts CO2 to HCO3 require?
Carbonic anhydrase (CA) enzyme
CA converts H2O + CO2↔︎ H2CO3 ↔︎ H + HCO3
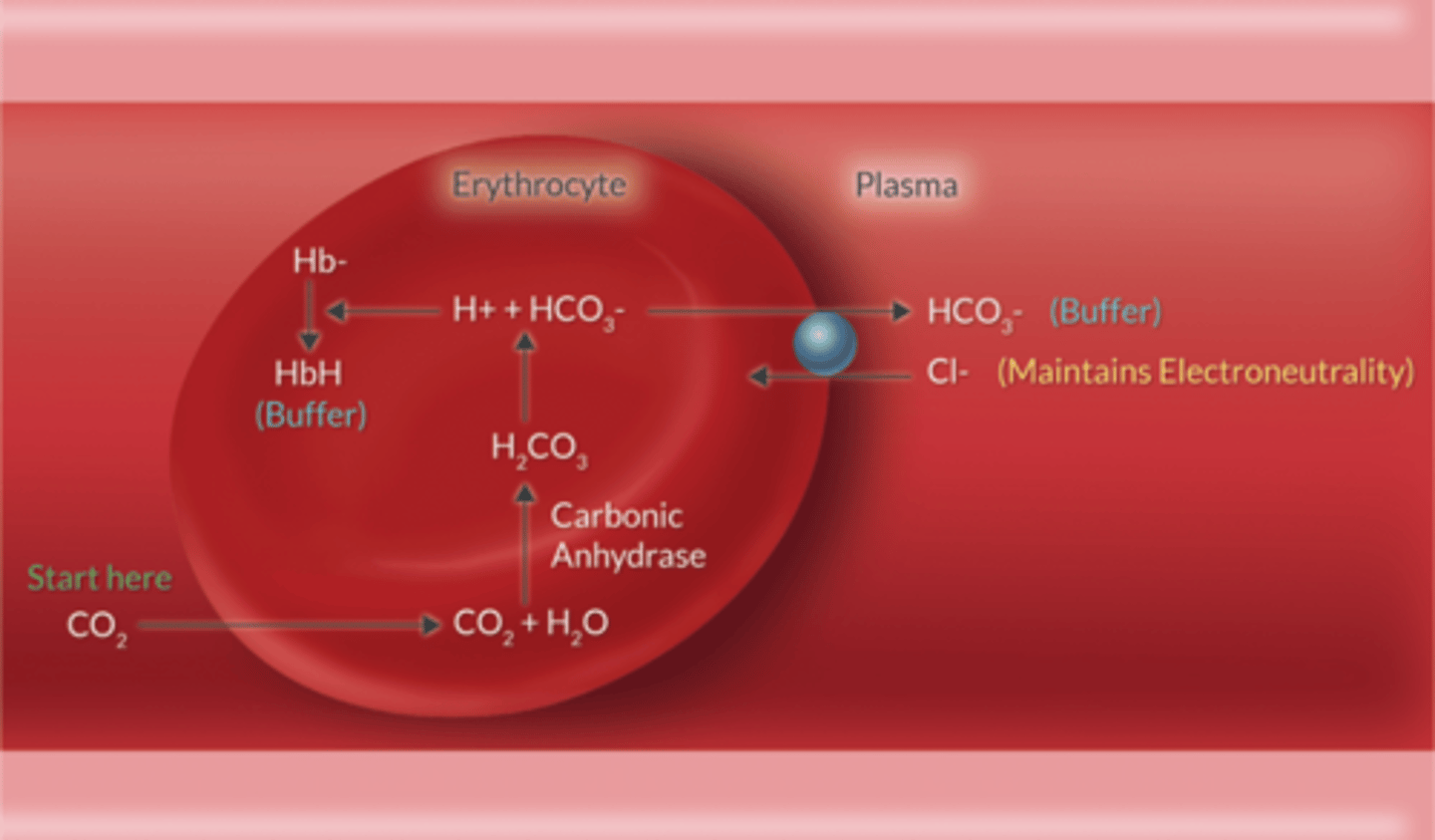
Describe the Hamburger Shift.
Chloride Shift
RBC releases HCO3 into plasma
+
Cl is transported into RBC to maintain neutrality
Describe the Bohr effect.
Describes O2 carriage.
↑ CO2 + ↓ pH cause the erythrocyte to release O2.
Describe the Haldane effect.
Describes CO2 carriage.
↑ O2 causes the erythrocyte to release CO2 (in lungs).
Said another way, deoxygenated (v) blood can carry more CO2, than oxygenated (a) blood.
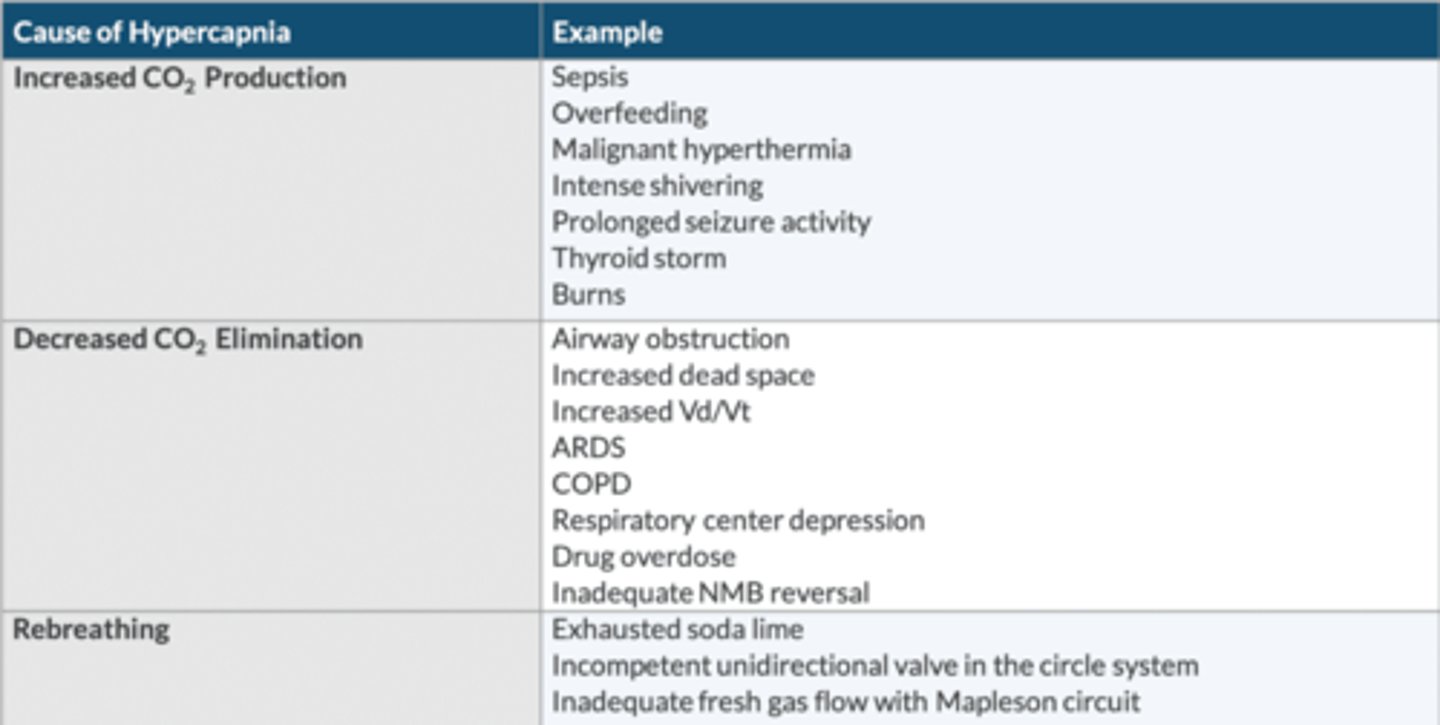
List the 3 primary causes of hypercapnia, and provide examples of each.
↑ CO2 production:
-sepsis
-overfeeding
-MH
-intense shivering
-prolonged seizure activity
-thyroid storm
-burns
↓ CO2 elimination:
-AW obstruction
-↑ dead space
-↑ Vd/Vt
-ARDS
-COPD
-respiratory center depression
-drug OD
-inadequate NMB reversal
Rebreathing:
-exhausted soda lime
-incompetent unidirectional valves in the circle system
-inadequate FGF w/Mapleson circuit
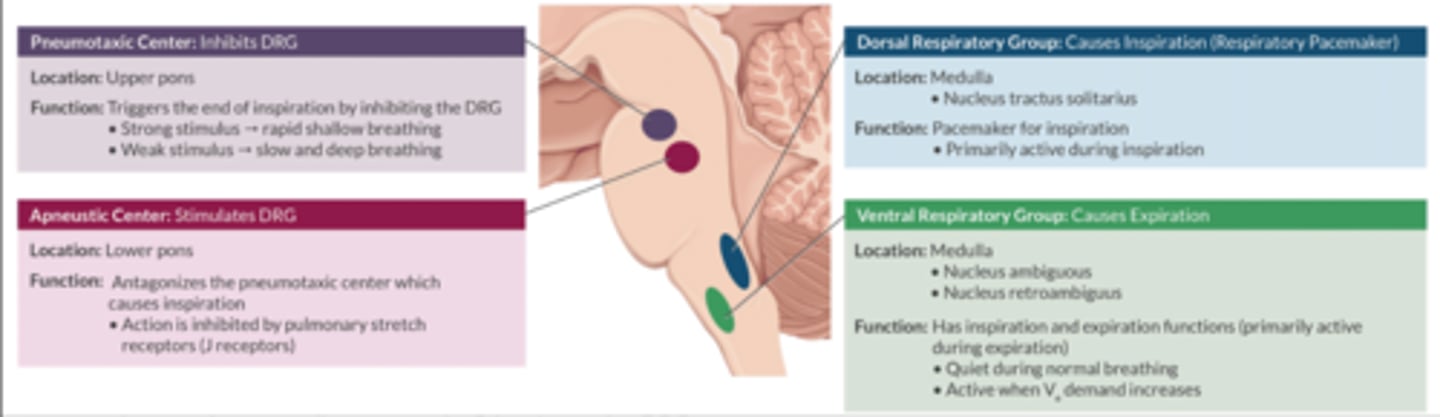
Describe the 4 areas in the respiratory center.
Resides in the brainstem (reticular activating system)
Medullary Respiratory Centers
-Dorsal respiratory center: active during inspiration (respiratory PM)
-Ventral respiratory center: active during expiration
Pontine Respiratory Centers
-Pneumotaxic center (upper pons): inhibits the DRC
-Apneustic center (lower pons): stimulates the DRC
Contrast the location and function of the central and peripheral chemoreceptors.
Central Chemoreceptor:
-medulla
-responds to the H [ ] in the CSF
-H in the CSF is a fxn of PaCO2 in the blood (PaCO2 is the primary stimulus to breathe)
Peripheral chemoreceptors:
-carotid bodies: nerves of Hering → glossopharyngeal n. (CN IX)
-aortic arch: Vagus n. (CN X)
-respond to ↓ O2, ↑ CO2, ↑ H
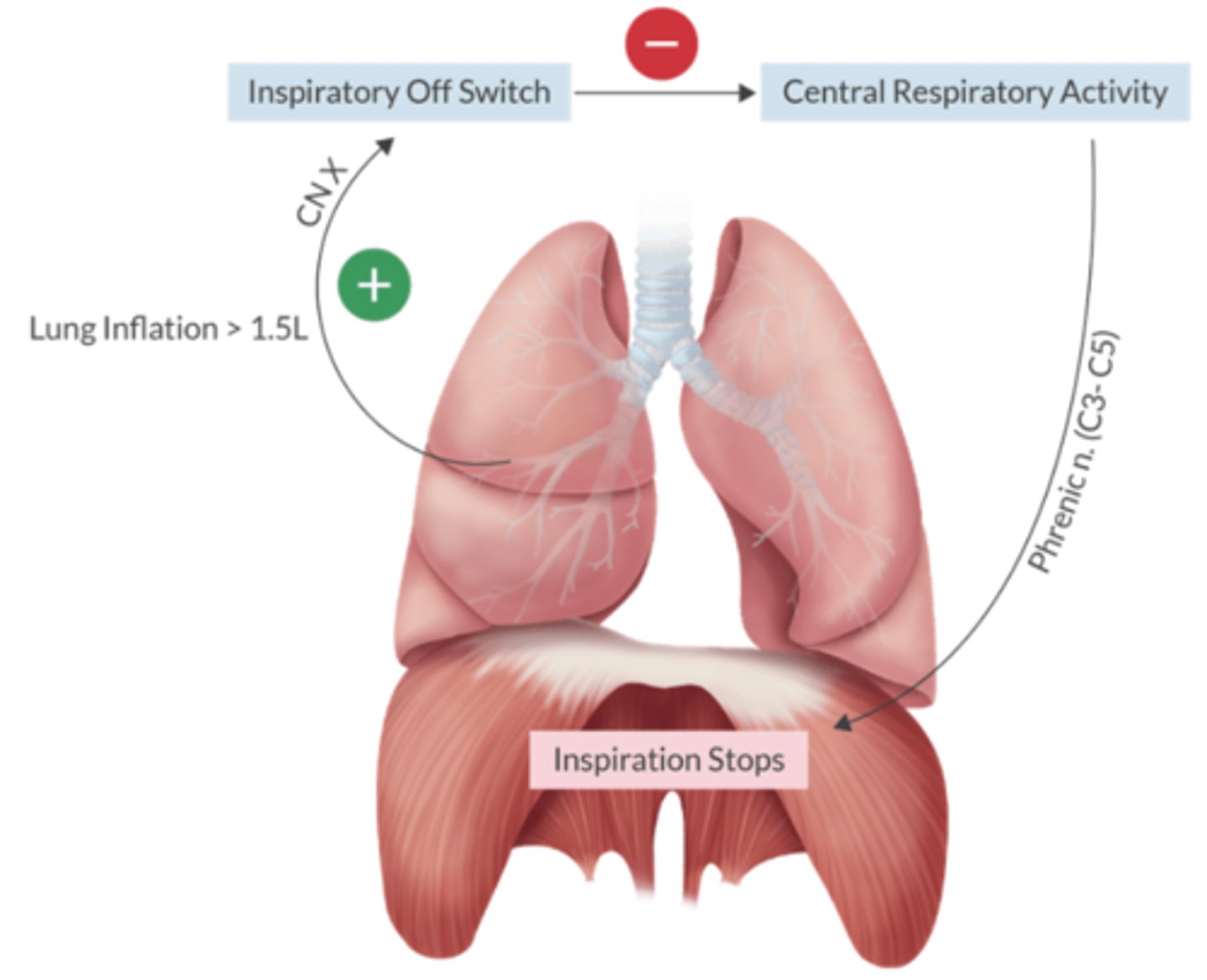
Which reflex prevents overinflation of the lungs?
Hering-Breuer inflation reflex
Inflation > 1.5L
→ CN X (inspiratory off switch)
→ inhibition of central respiratory activity + Phrenic n. manipulation of diaphragm
What is hypoxic pulmonary vasoconstriction (HPV)?
Minimizes shunt by ↓ BF through poorly ventilated alveoli → better ventilated alveoli
Trigger: ↓ PAO2 (not PaO2)
-begins immediately
-peaks after 15 min
What things impair HPV, and what are the consequences of this?
-VA > 1-1.5 MAC
-Phosphodiesterase inhibitors
-Dobutamine
-Vasodilators
IV anesthetics do NOT inhibit HPV.
Consequence: ↑ shunt
What does the diffusing capacity for carbon monoxide tell us?
DLCO assess how well the lung can exchange gas.
Normal = 17-25 mL/CO/min/mmHg
Using Fick's law of diffusion, the DLCO tells us 2 key characteristics about the alveolar-capillary interface:
-surface area (↓ by emphysema)
-thickness (↑ by pulmonary fibrosis and pulmonary edema)
How is tobacco smoke harmful?
↑ SNS tone
↑ sputum production
↑ carboxyhemoglobin [ ]
↑ infection risk
Describe the short term benefits of smoking cessation.
Does NOT ↓ risk of PPC
-↑ SNS effects of nicotine dissipate after 20-30 minutes
-P50 returns to near normal in 12 hr (CaO2 improves)
Describe the intermediate term benefits of smoking cessation.
Normal fxn req at least 6 weeks
-a.w. fxn
-mucociliary clearance
-sputum production
-pulmonary immune fxn
-hepatic enzyme induction subsides
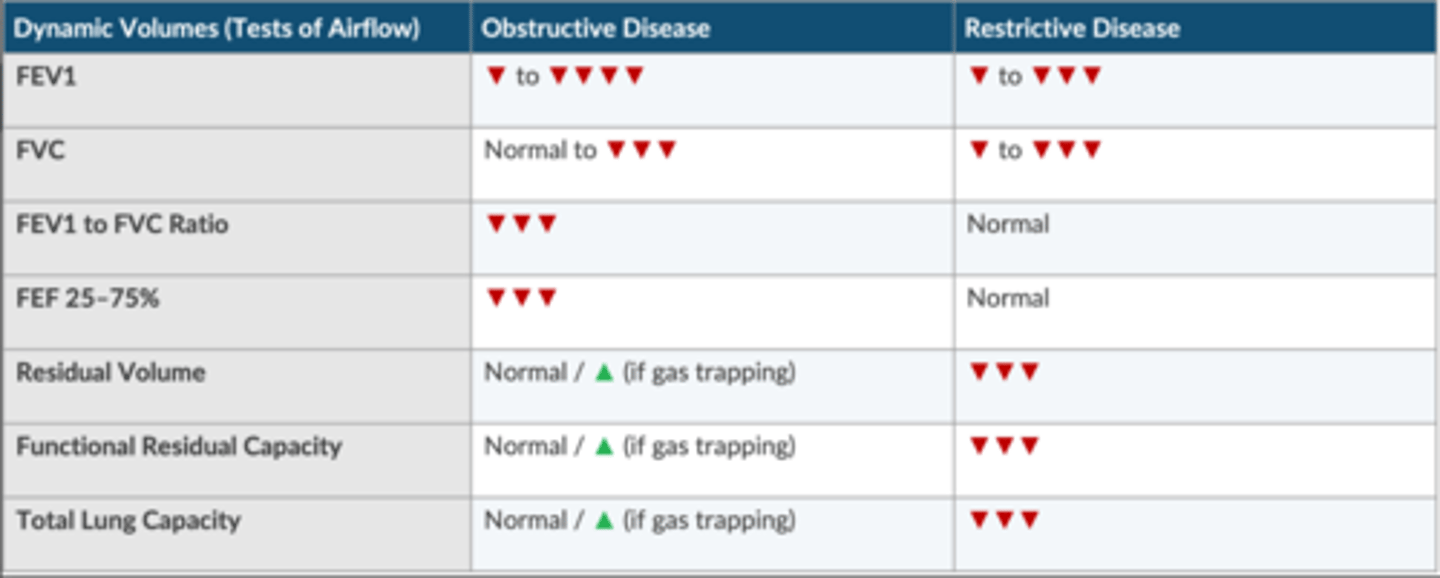
Compare and contrast PFTs in obstructive and restrictive disease.
Obstructive disease
↓ : FEV1, FVC, FEV1/FVC ratio, FEF 25-75%
normal/ ↑ (if gas trapping): RV, FRC, TLC
Restrictive disease
↓ : FEV1, FVC, RV, FRC, RLC
normal: FEV1/FVC ratio, FEF 25-75%
Discuss the following pulmonary flow-volume loops: normal, obstructive, restrictive, fixed obstruction.
Normal: upside down ice cream cone.
Obstructive: normal inspiration with expiratory obstruction.
Restrictive: shape is similar to normal loop, but the restrictive loop is smaller and right-shifted.
Fixed Obstruction: inspiration and expiration are affected. An extra thoracic obstruction is abnormal during inspiration and normal during expiration. An intra thoracic obstruction is normal during inspiration and abnormal during expiration.
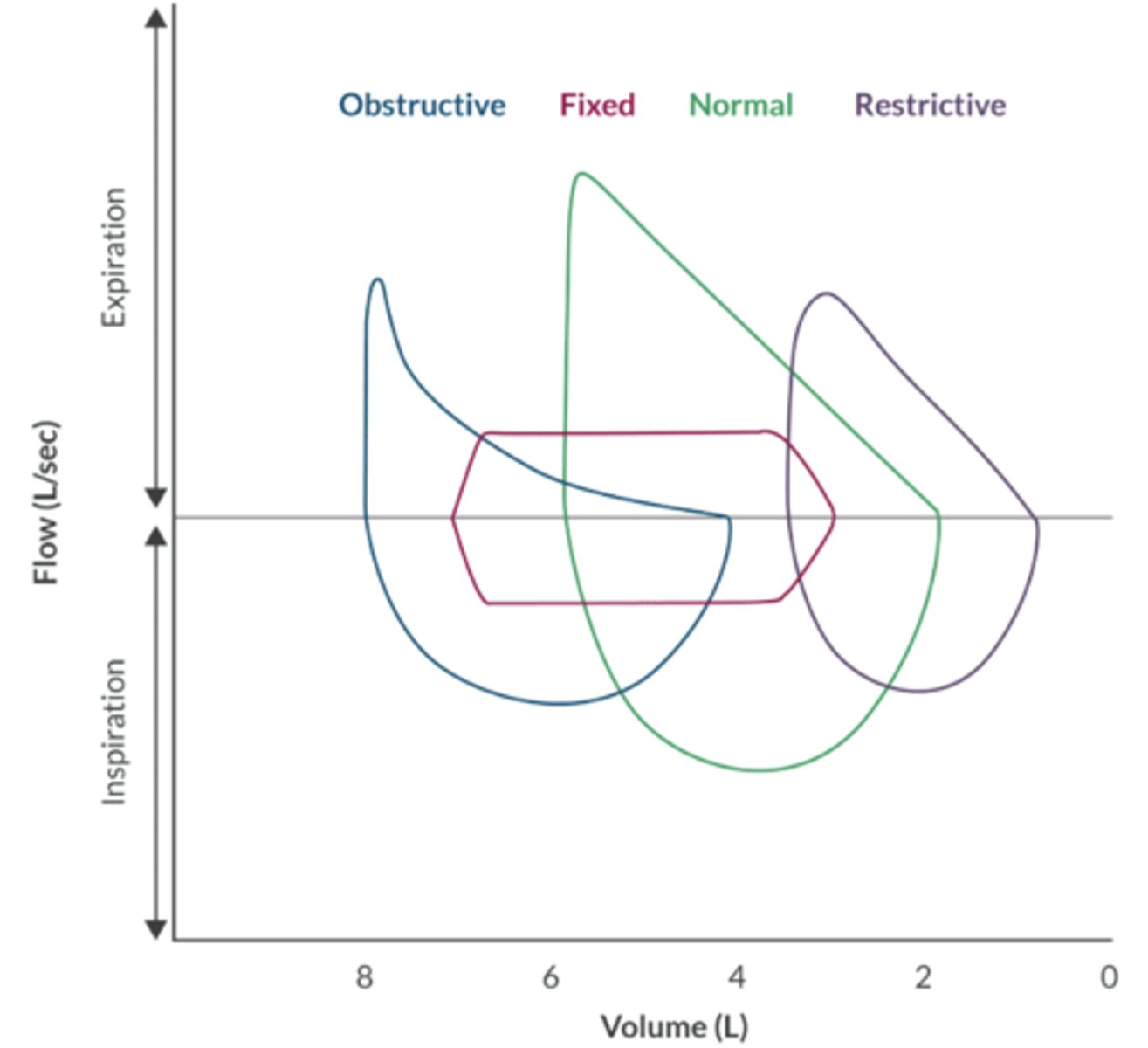
Give an example of a disease that produces the following pulmonary flow-volume loops: obstructive, restrictive, and fixed obstruction.
Obstruction: COPD
Restrictive: pulmonary fibrosis
Fixed Obstruction: tracheal stenosis
What is the treatment for acute bronchospasm?
1. 100% FiO2
2. Deepen anesthetic
3. Inhaled β2 agonist (albuterol)
4. Inhaled anticholinergic (ipratropium)
5. Epinephrine 1 mcg/kg IV
6. Hydrocortisone 2-4 mg/kg IV (takes several hours to have an effect)
7. Aminophylline
8. Helium-oxygen reduces airway resistance
*Montelukast is not used in the treatment of acute bronchospasm
What is alpha-1 antitrypsin deficiency?
-Alveolar elastase is a naturally occurring enzyme that breaks down pulmonary connective tissue. This enzyme is kept in check by alpha-1 antitrypsin (produced in the liver).
-Deficiency: alveolar elastase is free to wreak havoc on pulmonary connective tissue. Ultimately → panlobular emphysema.
-Liver transplant is the definitive treatment
Describe the goals and strategies for mechanical ventilation in the patient with COPD.
Goal: prevent barotrauma + ↓ air trapping.
This is accomplished by:
-low TV (6 - 8 mL/kg IBW)
-↑ expiratory time to minimize air trapping
-slow inspiratory flow rate optimize V/Q matching
-low levels of PEEP are ok, so long as air trapping does not occur
Define restrictive lung disease
-↓ lung volumes and capacities
-↓ compliance
-intact pulmonary flow rates
Give examples of intrinsic lung diseases (acute and chronic).
Affects lung parenchyma:
-Acute: aspiration, negative pressure pulmonary edema
-Chronic: pulmonary fibrosis, sarcoidosis
Give examples of extrinsic lung diseases (acute and chronic).
Affects areas around the lungs:
-chest wall/mediastinum: kyphoscoliosis, flail chest, neuromuscular disorders, mediastinal mass
-↑ intraabdominal pressure: pregnancy, obesity, ascites
List the risk factors for aspiration pneumonitis.
-Trauma
-Emergency surgery
-Head injury
-Seizures
-Difficult AW management
-Cricoid pressure
-Impaired AW reflexes
-Residual NMB
-Pregnancy
-Ascites
-GI obstruction
-GERD
-PUD
-Hiatal hernia
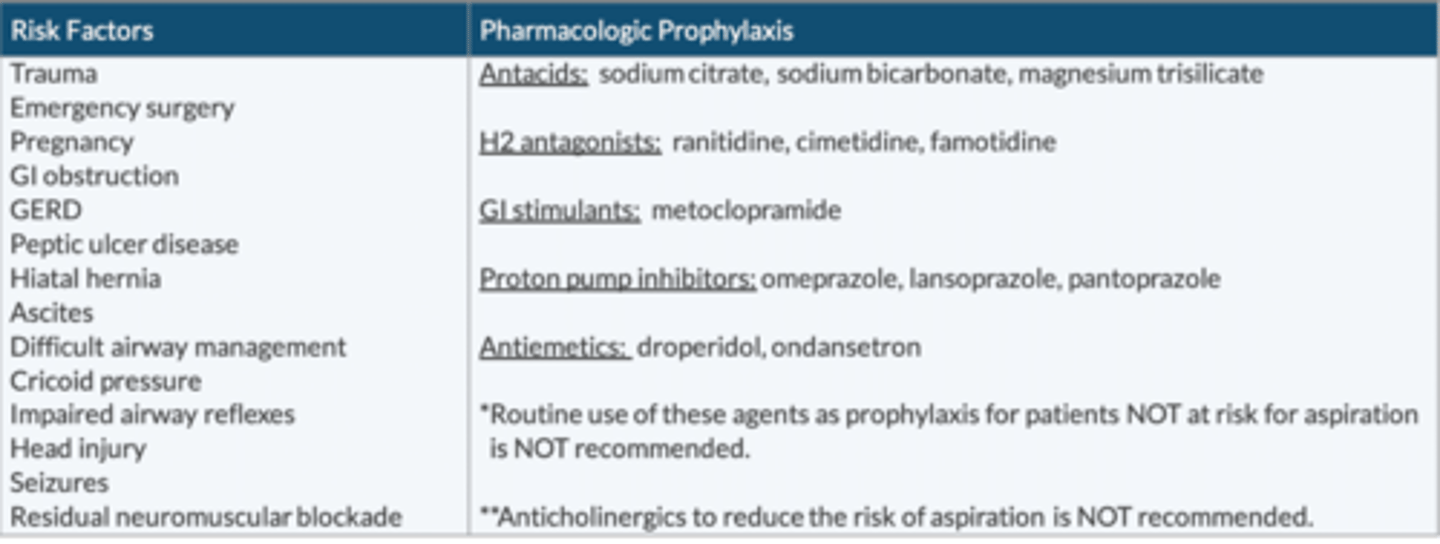
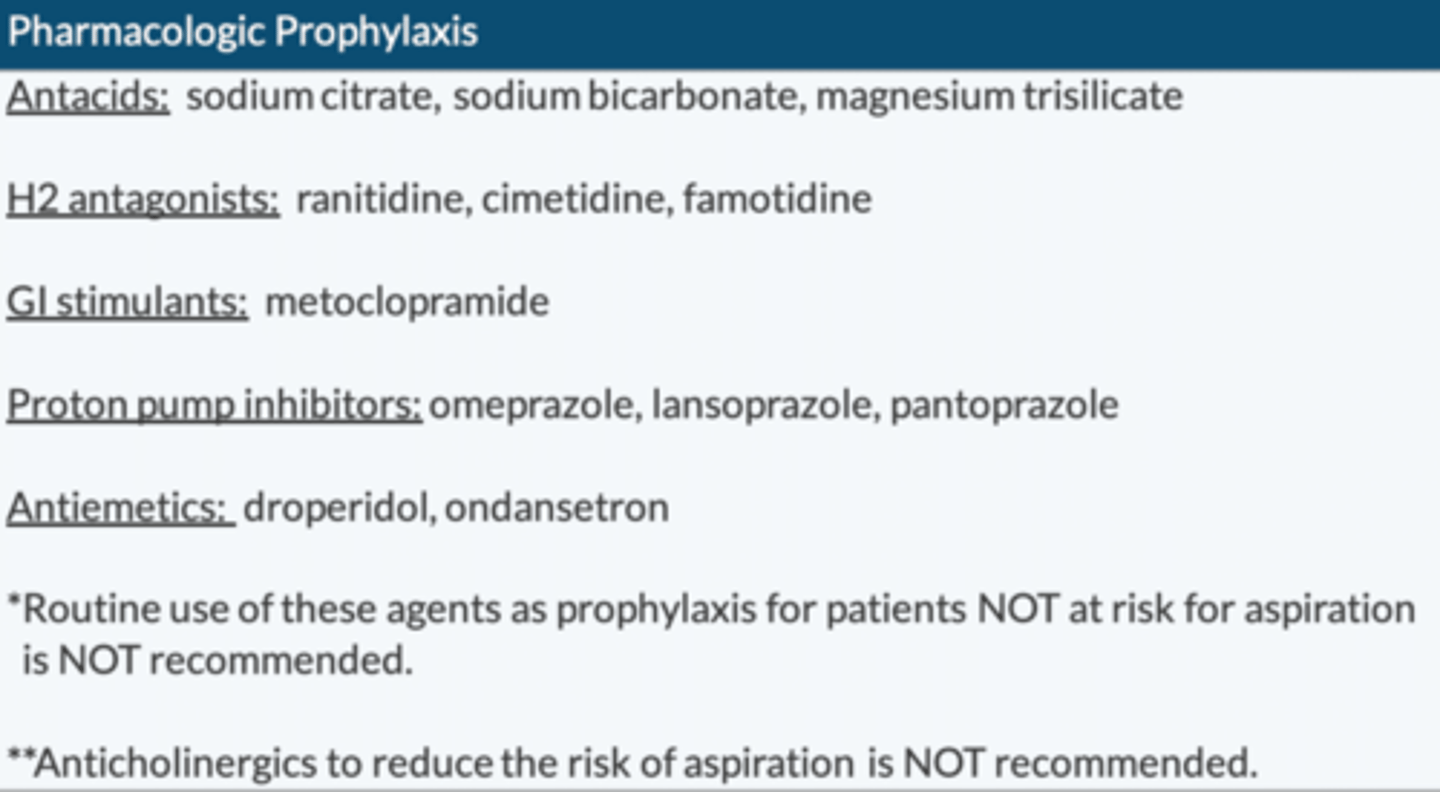
Describe the pharmacologic prophylaxis of aspiration pneumonitis.
Antacids: sodium citrate, sodium bicarbonate, magnesium trisilicate
H2 antagonist: ranitidine, cimetidine, famotidine
GI stimulants: metoclopramide
PPI: omeprazole, lansoprazole, pantoprazole
Antiemetics: droperidol, ondansetron
*Routine use of these agents as prophylaxis for patients NOT at risk for aspiration is NOT recommended
**Anticholinergics to ↓ risk of aspiration is NOT recommended
What is Mendelson's syndrome?
Chemical aspiration pneumonitis
-1st described in OB w/inhalation anesthesia
Risk factors include:
-Gastric pH < 2.5
-Gastric volume > 25 mL (0.4 mL/kg)
Describe the treatment of aspiration.
1. Tilt head downward or to the side
2. Upper AW suction to remove particulate matter
3. Lower AW suction is only useful for removing particulate matter (doesn't help chemical burn from gastric acid)
4. Secure AW to support oxygenation
5. PEEP to ↓ shunt
6. Bronchodilators to ↓ wheezing
7. Lidocaine to ↓ neutrophil response
8. Steroids probably don't help
9. ABX are only indicated if patient develops a fever or an ↑ WBC count > 48 hrs
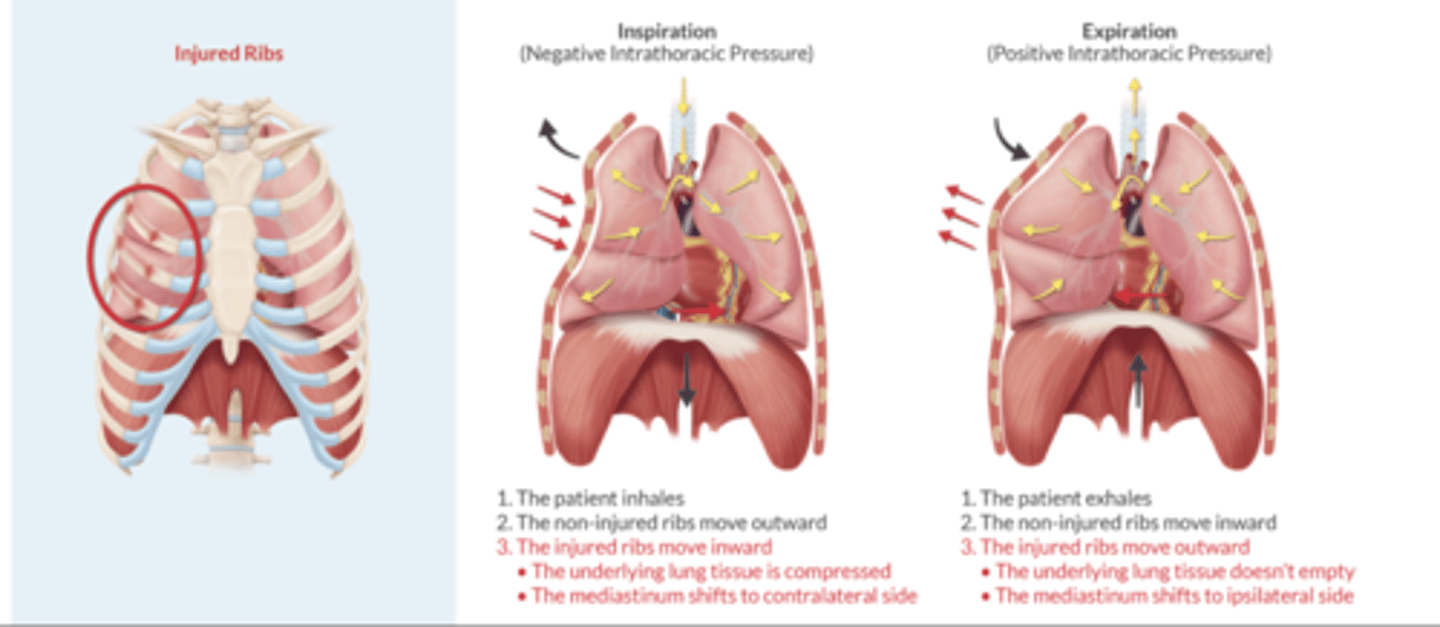
Discuss the pathophysiology and treatment of flail chest.
Consequence of blunt chest trauma with multiple rib Fx.
Key characteristic: paradoxical movement of chest wall at the site of the fractures
Inspiration (Negative Intrathoracic pressure)
injured ribs move inward & collapse the affected region, mediastinum shifts to contralateral side
Expiration (Positive Intrathoracic Pressure)
injured ribs move outward & affected region doesn't empty, mediastinum shifts to ipsilateral side
Treatment = epidural catheter or intercostal nerve blocks (higher risk of LA toxicity)
Define Pulmonary HTN, + discuss the goals of anesthetic management.
PAP > 25 mmHg
Causes: COPD, Left Heart Disease, connective tissue disorders
Goals: optimize PVR
↑ PVR (avoid/correct):
-hypoxemia
-hypercarbia
-acidosis
-SNS stimulation
-pain
-hypothermia
-↑ intrathoracic pressure
-Coughing/straining
-PEEP
-atelectasis
-MV
-N2O
-ketamine
-Des
The patient with cor pulmonale (RHF) is also sensitive to ↑ PVR, so keep the same principles in mind.
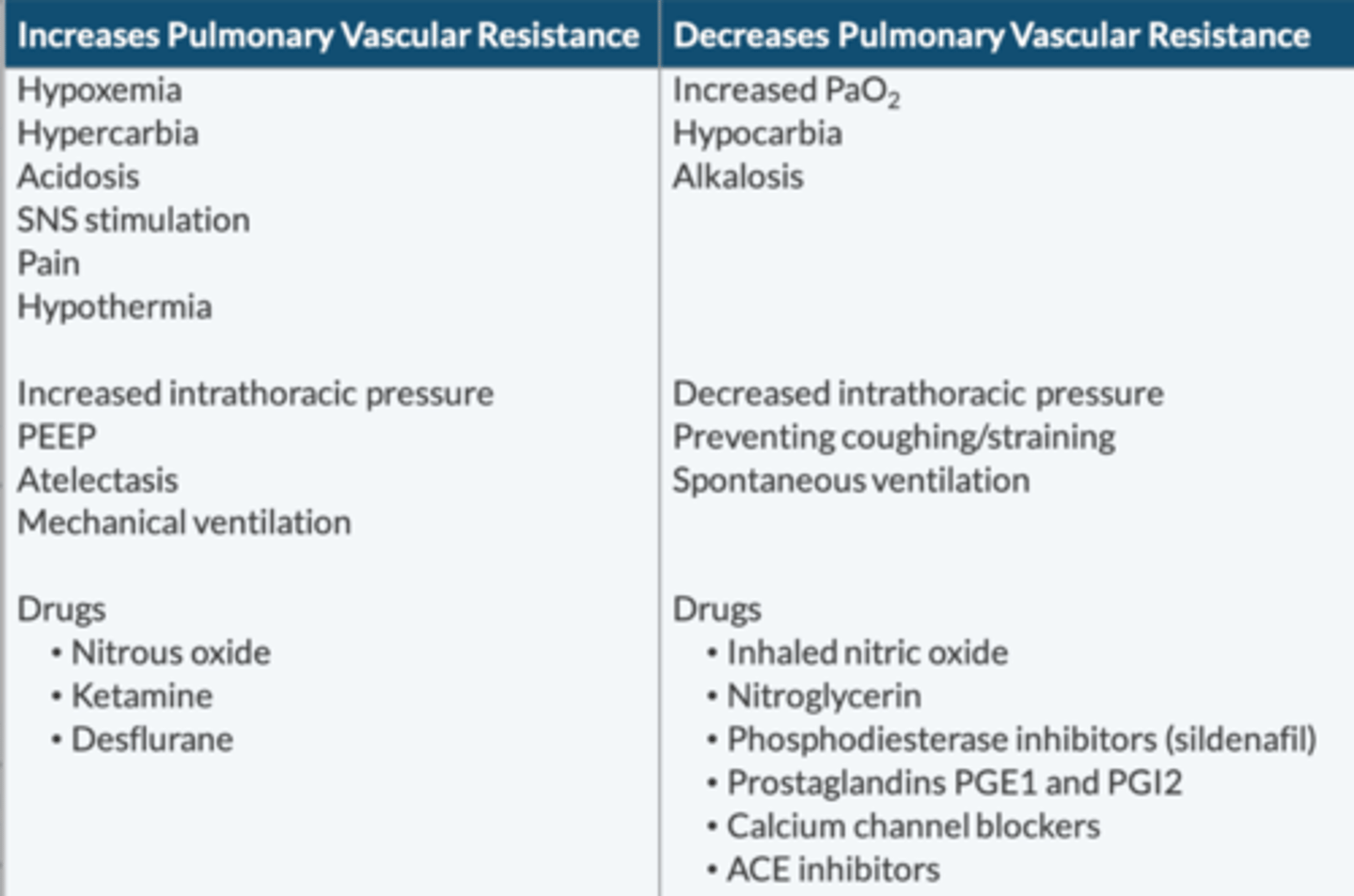
What drugs help ↓ PVR?
iNO
Nitroglycerin
Phosphodiesterase inhibitors
-sildenafil
Prostaglandins PGE1 + PGI2
CCB
ACEI
Discuss the pathophysiology of carbon monoxide poisoning.
↓ oxygen carrying capacity (left shift).
Affinity 200x that of oxygen.
Oxidative phosphorylation is impaired → metabolic acidosis
-A co-oximeter (not SpO2) measure CO
-Cherry red appearance (not cyanosis)
-SNS stimulation may be confused with light anesthesia or pain
-If soda lime is desiccated, then VA can produce CO (Des > Iso >>> Sevo)
Discuss the treatment of carbon monoxide poising.
100% FiO2
until CoHgb is < 5% for 6 hrs
Hyperbaric oxygen if CoHgb > 25% or Pt is symptomatic
List the absolute indications to OLV
Avoid contamination:
-infection
-massive hemorrhage
Control of distribution of ventilation:
-BPF
-surgical opening of major AW
-large cyst or bulla
-life threatening hypoxeima
Unilateral bronchopulmonary lavage:
-pulmonary alveolar proteinosis
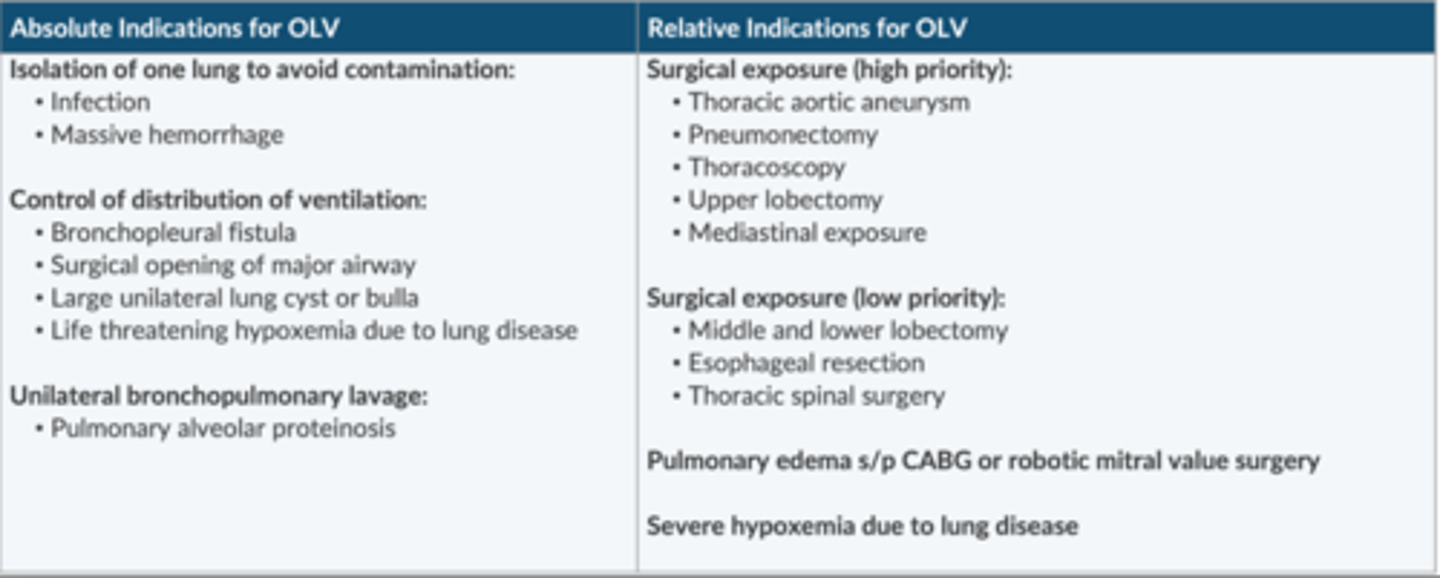
List the relative indications for OLV.
Surgical exposure (high priority):
-TAA
-pneumonectomy
-thoracoscopy
-upper lobectomy
-mediastinal exposure
surgical exposure (low priority):
-middle/lower lobectomy
-esophageal resection
-thoracic spinal surgery
pulmonary edema s/p CABG or robotic MV surgery
Severe hypoxemia d/t lung disease
Discuss how anesthesia in the lateral decubitus position affects the V/Q relationship.
Nondependent lung:
-moves from a flatter region (less compliant) to an area of better compliance (slope)
-ventilation is optimal
Dependent lung:
-moves from the slope to the lower, flatter area of the curve (less compliant)
-perfusion is best in this lung (gravity)
-↓ of alveolar V contributes to atelectasis
The net effect: ventilation is better in the nondependent lung.
-creates V/Q mismatch + ↑ risk of hypoxemia during OLV.
Discuss the management of hypoxemia during OLV.
1. 100% FiO2
2. Confirm DLT position w/FOB (most common complication)
3. CPAP 2-10 cmH2O to nondependent (nonventilated) lung
4. PEEP 5-10 cm H2O to dependent (ventilated) lung
5. Alveolar recruitment maneuver
6. Clamp PA to the nondependent (non-ventilated lung)
7. Resume TLV
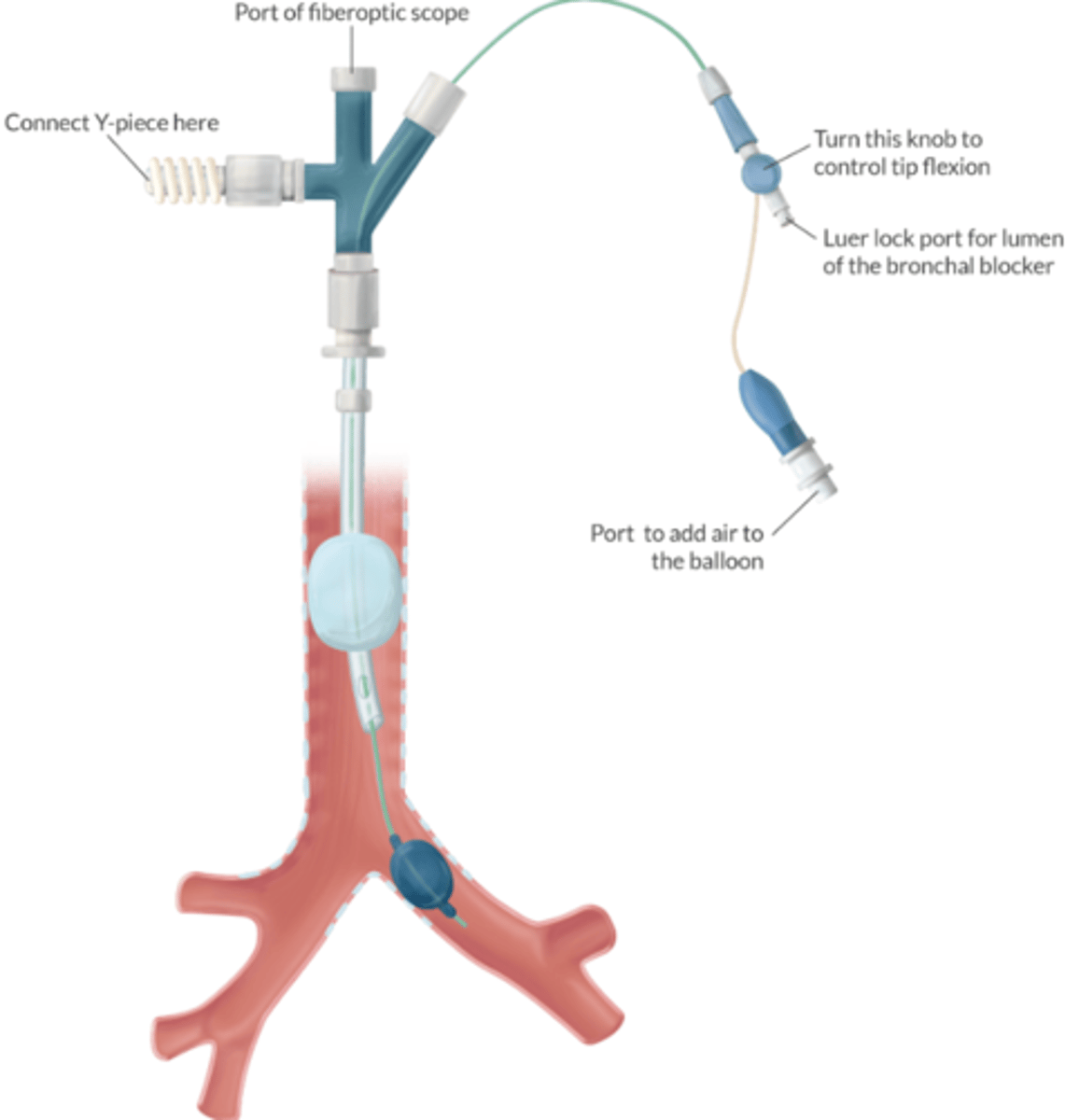
List 5 indications for the use of a bronchial blocker.
-< 8 y/o (smallest DLT = 26 Fr for 8-10 y/o)
-require nasal intubation
-have a trach
-have a SLT in place
-require post op intubation (avoids changing DLT to SLT)
How can the lumen of the bronchial blocker be used during OLV?
USE:
-insufflate O2 into nonventilated lung
-suction air from nonventilated lung (improves surgical exposure)
DO NOT USE:
-ventilate
-suction blood, pus, or secretions from the non-ventilated lung
What is mediastinoscopy, and why is it performed?
Performed to obtain biopsy of the paratracheal lymph nodes at the level of the carina.
Helps the surgeon stage the tumor prior to resection.
What are potential complications of mediastinoscopy? What is the most common?
-Hemorrhage (#1 - major vessels near scope)
-PTX (#2 - R side)
-Thoracic aoarta (hemorrhage + reflex ↓HR)
-Innominate artery (↓ carotid BF & CBF)
-Trachea (AW obstruction)
-Thoracic duct (chylothorax)
-Nerve paresis: Phrenic, RLN
Where you should place the pulse oximeter and NIBP for mediastinoscopy?
RUE
-SPO2 (or A-line) waveform will dampen or disappear w/innominant a. compression
LUE
-BP reading on the LUE won't be affected w/innominant a compression.
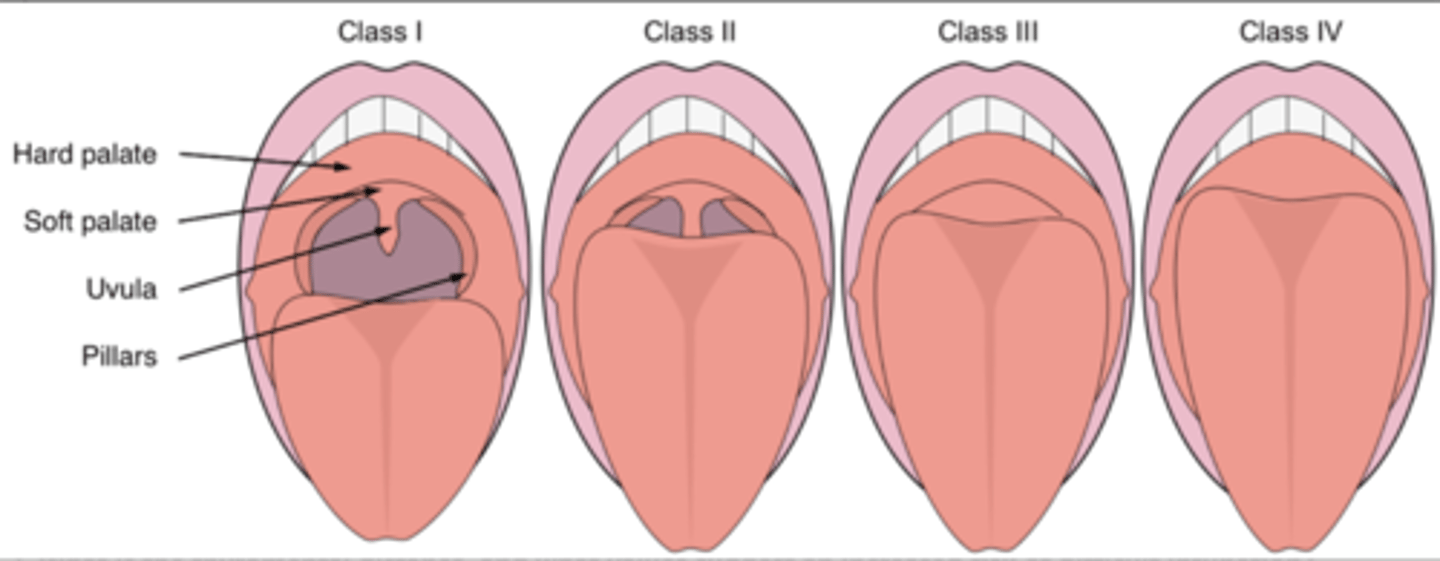
Describe the Mallampati score.
"PUSH"
Class I:
Posterior pillars
Uvula
Soft palate
Hard palate
Class II:
Uvula
Soft palate
Hard palate
Class III:
Soft palate
Hard palate
Class IV:
Hard palate
Describe the inter-incisor gap. What is normal?
Ability to open the mouth directly affects ability to align the oral, pharyngeal, laryngeal axes.
Small inter-incisor gap creates a more acute angle b/t oral + glottic openings
-↑ difficulty of intubation.
Normal = 2-3 FB or 4 cm
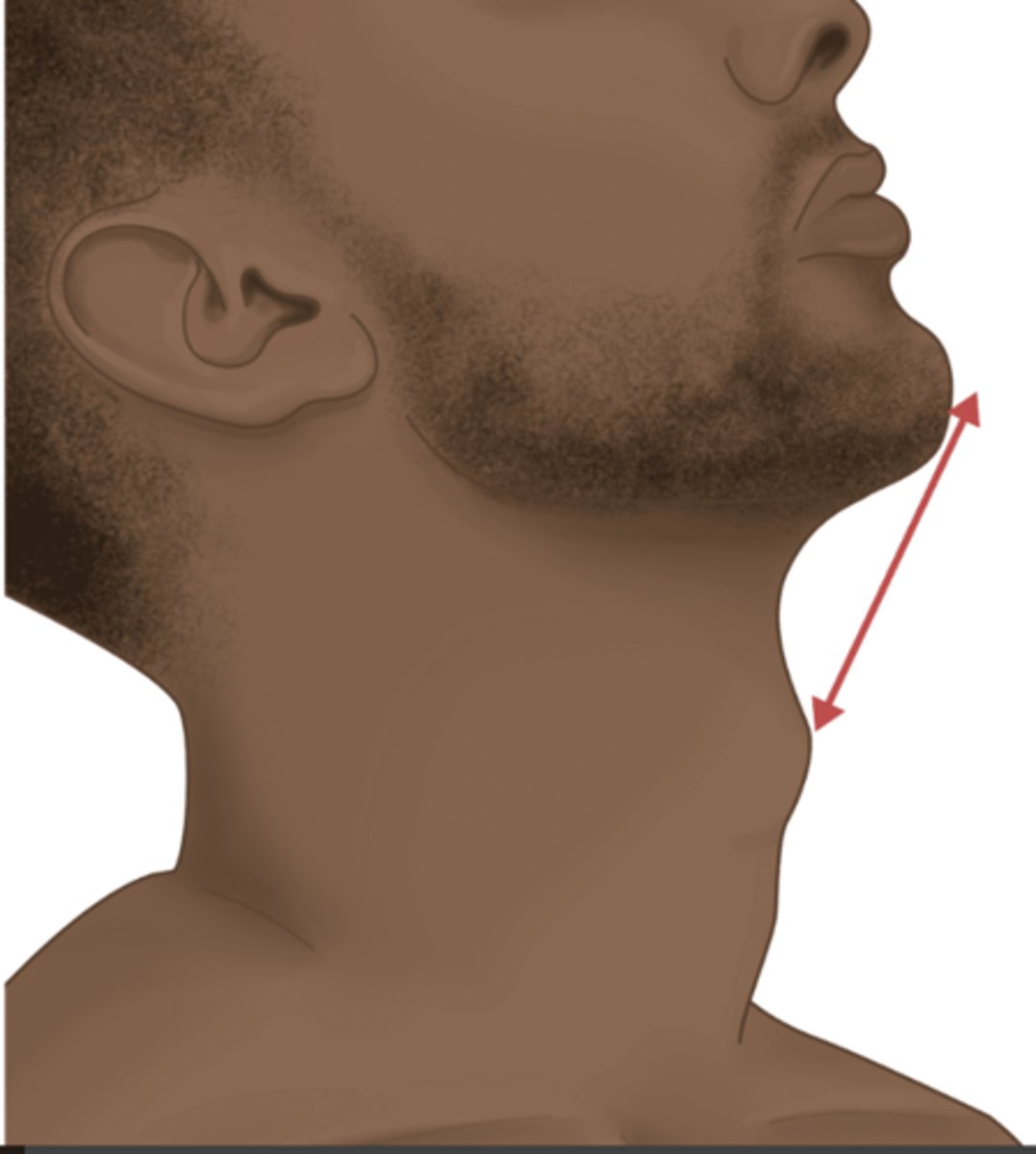
What is the thyromental distance, and what values suggest an increased risk of difficult intubation?
Helps estimate the size of the submandibular space.
With the neck extended and mouth closed, you can measure the distance from the tip of the thyroid cartilage to the tip of the mentum.
DL ↑ difficulty if
< 6 cm (3 fingerbreadths) or
> 9 cm
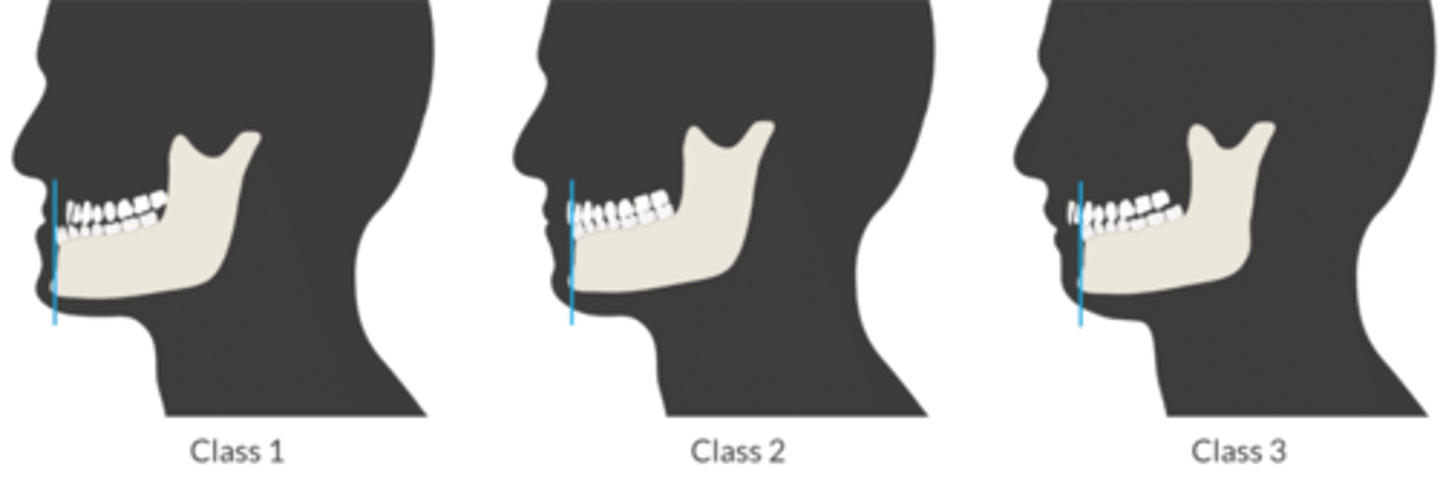
What is the mandibular protrusion test, and what values suggest an increased risk of difficult intubation?
Assesses fxn of TMJ.
Ask Pt to sublux jaw
-Compare position of the lower incisors to the upper incisors
Class 1: moves LI past UI + bite the vermilion of the lip (where the lip meets the facial skin).
Class 2: LI + UI inline
- Class 3: cannot move LI past UI (↑ risk of difficult intubation).
What conditions impair atlanto-occipital joint mobility?
-Degenerative joint disease
-Rheumatic arthritis
-Ankylosing spondylitis
-Trauma
-Surgical fixation
-Klippel-Feil
-Down syndrome
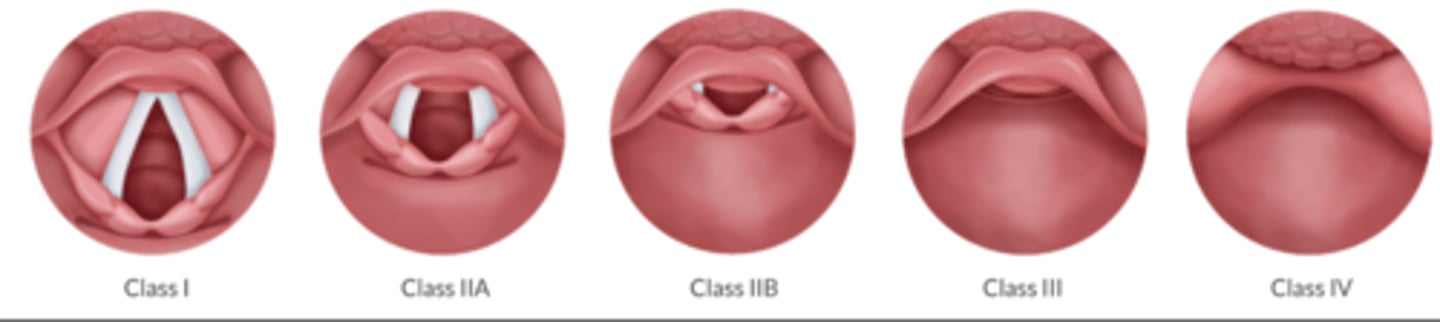
Describe the Cormack and Lehane score.
Helps us measure the view we obtain during DL
"AW, PAW, E, NAW"
Class 1: AW structures seen
Class 2: Posterior AW
-2a posterior glottis
-2b: arytenoids only
Class 3: Epiglottis
Class 4: No AW structures
List 5 risk factors for difficult mask ventilation.
"BONES"
Beard
Obese (BMI > 26)
No teeth
Elderly (>55)
Snoring
List 10 risk factors for difficult tracheal intubation.
1. Small mouth opening
2. Narrow palate w/high arch
3. Long Upper Incisors
4. Inter-incisor distance < 3 cm
5. Mallampati class 3 or 4
6. Mandibular Protrusion Test class 3
7. Poor compliance of submandibular space
8. Thyromental distance < 6 cm (< 3 FB) or > 9 cm
9. Thick + short neck
10. Limited AO joint mobility (can't touch chin to chest and/or can't extend the neck)
List 6 risk factors for difficult supraglottic device placement.
1. Limited mouth opening
2. Upper AW obstruction (prevents passage of device into pharynx)
3. Altered pharyngeal anatomy (prevents seal)
4. Poor AW compliance (requires excessive PIP)
5. ↑ AW resistance (requires excessive PIP)
6. Lower AW obstruction
List 5 risk factors for difficult invasive airway placement.
1. Abnormal neck anatomy (tumor, hematoma, abscess, hx of radiation)
2. Obesity (can't ID CTM)
3. Short neck (can't ID CTM)
4. Limited access to CTM (halo, neck flexion deformity)
5. Laryngeal trauma
Describe the Practice Guidelines for Preoperative Fasting and Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration.
2 hours = clears
4 hours = breast milk
6 hours = nonhuman milk, infant formula, solid food
8 hours = fried or fatty food
Ingestion of clear liquids 2 hours before surgery ↓ gastric volume and ↑ gastric pH.
What is angioedema?
result of ↑ vascular permeability that can lead to swelling of the face, tongue, and AW.
AW obstruction is an extreme concern.
What are two common causes of angioedema? What is the treatment for each?
1. Anaphylaxis
Tx:
-epinephrine
-antihistamine
-steroids
2. ACEI or C1 esterase deficiency
Tx:
-icatibant
-ecallantide
-FFP
-C1 esterase concentrate.
What is Ludwig's angina?
A bacterial infection characterized by a rapidly progressing cellulitis in the floor of the mouth.
Most significant concern is a posterior displacement of the tongue resulting in complete, supraglottic AW obstruction.
What is the best way to secure the AW in the patient with Ludwig's angina?
Awake nasal intubation
Awake tracheostomy
List the 4 types of oropharyngeal AW. Which are best suited for fiberoptic intubation?
1. Guedel
2. Berman
3. Williams
-blind orotracheal
-fiberoptic intubation
4. Ovassapian:
-fiberoptic intubation
