All Adjustment Set Ups
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Listing:
• T5 transverse process (TP) palpates posterior on the right
• T5 has a left rotation restriction
• T5 spinous is deviated to the left
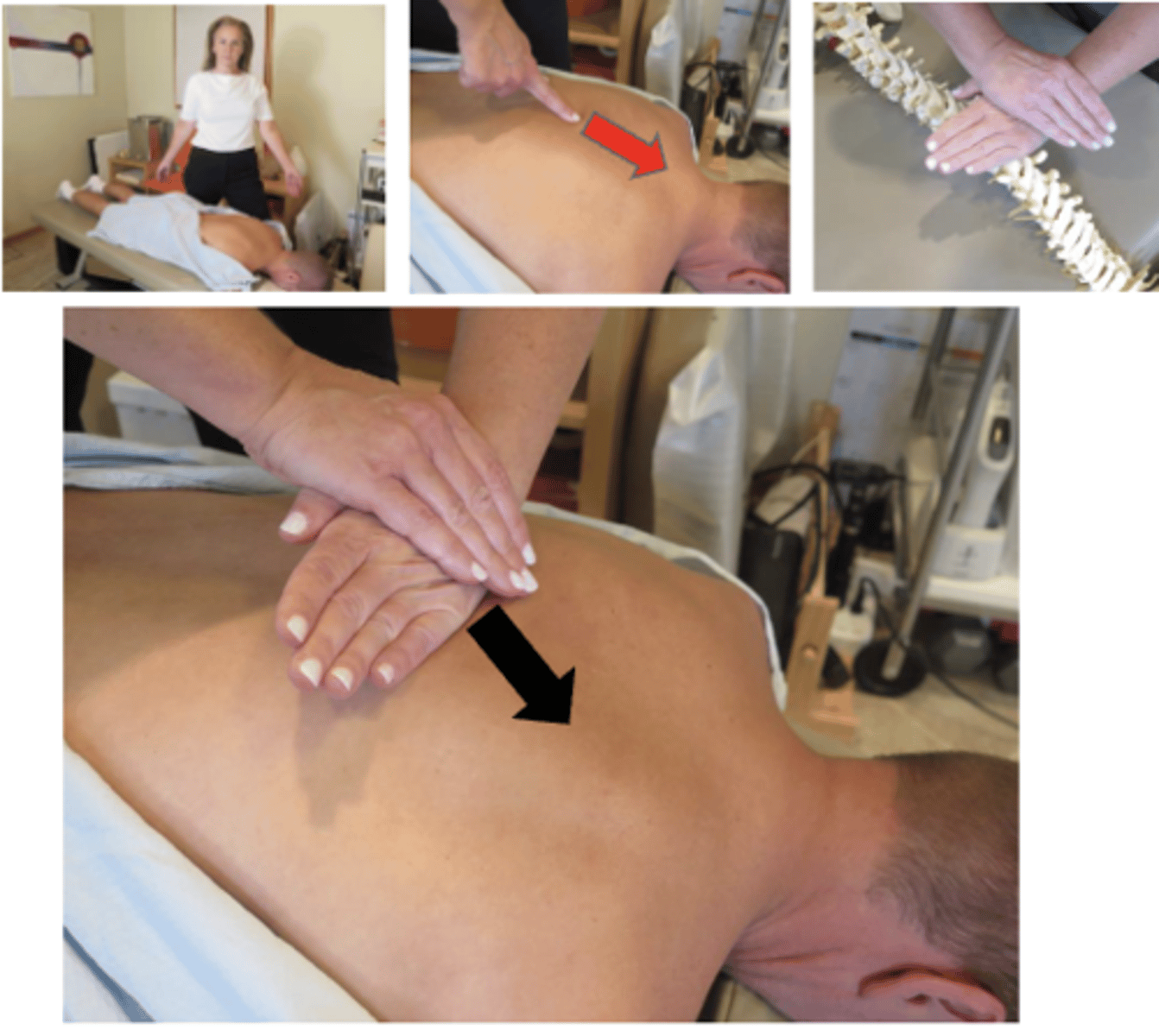
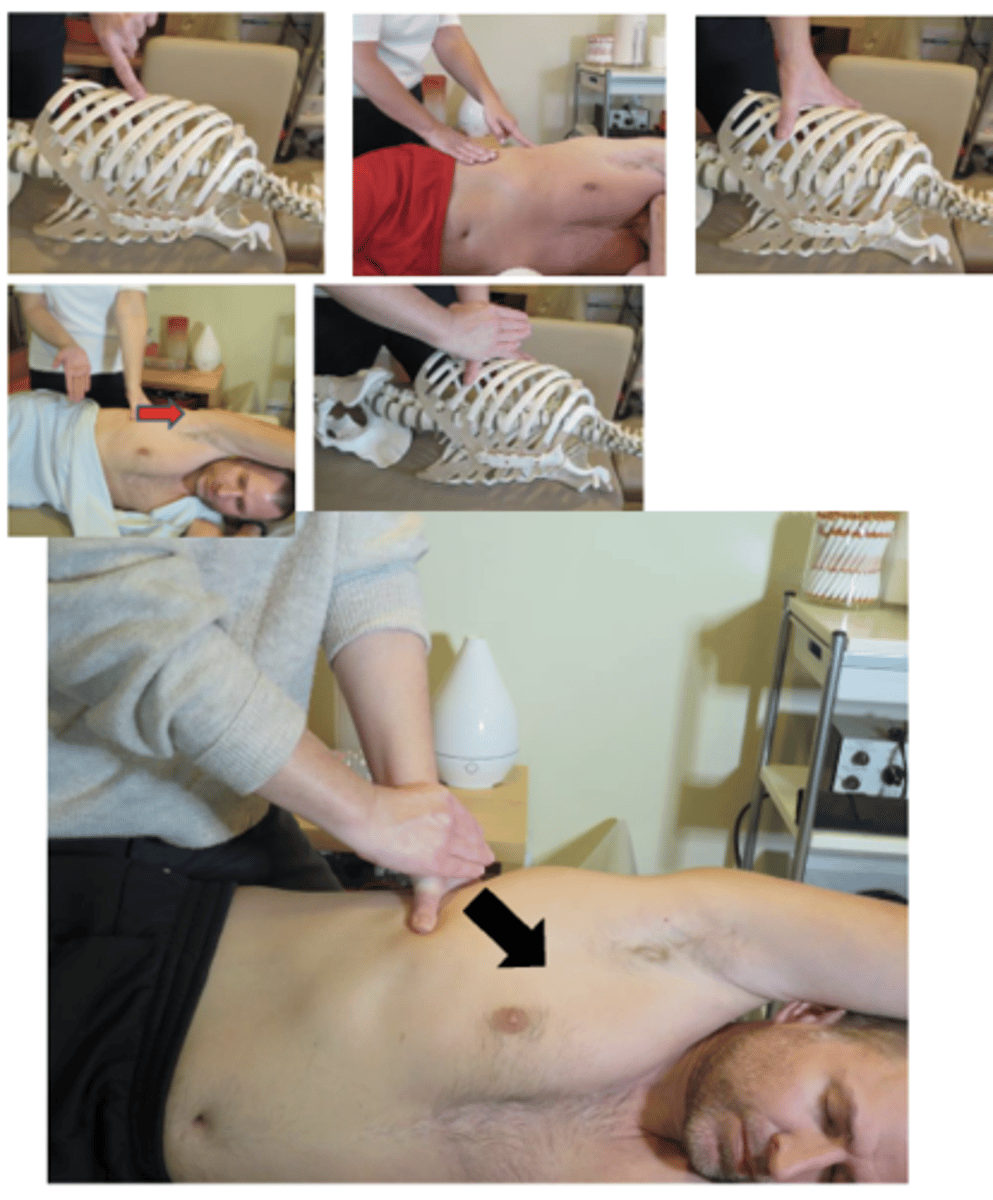
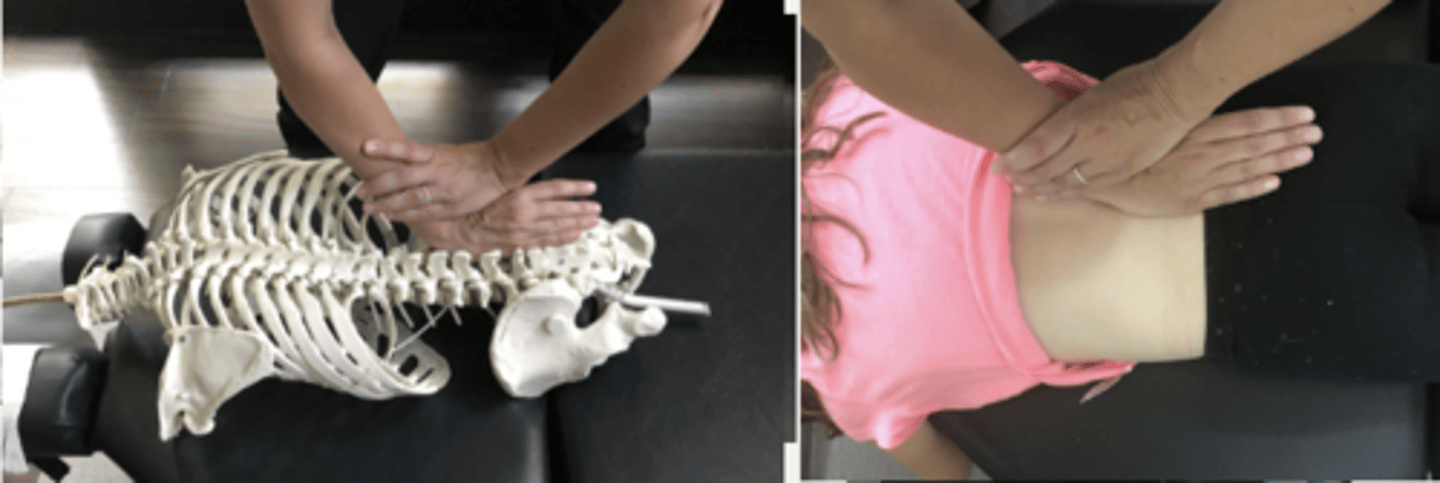
Technique:Prone (Unilateral) Hypothenar/Transverse Push
• PP: Prone, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Fencer or square stance facing cephalad, side of adjustive contact, tissue slack M-L
• CH: Hypothenar of caudal hand on Transverse Process (TP) (fingers running parallel to the spine)
• IH: Pisiform in anatomical snuff box ofCH, with fingers around wrist.
• Vector: P-A
Listing:
Left T4 TP palpates inferior in relationship to the left T5 TP
T4 has a right lateral flexion restriction
T4-T5 has an open wedge on the right side
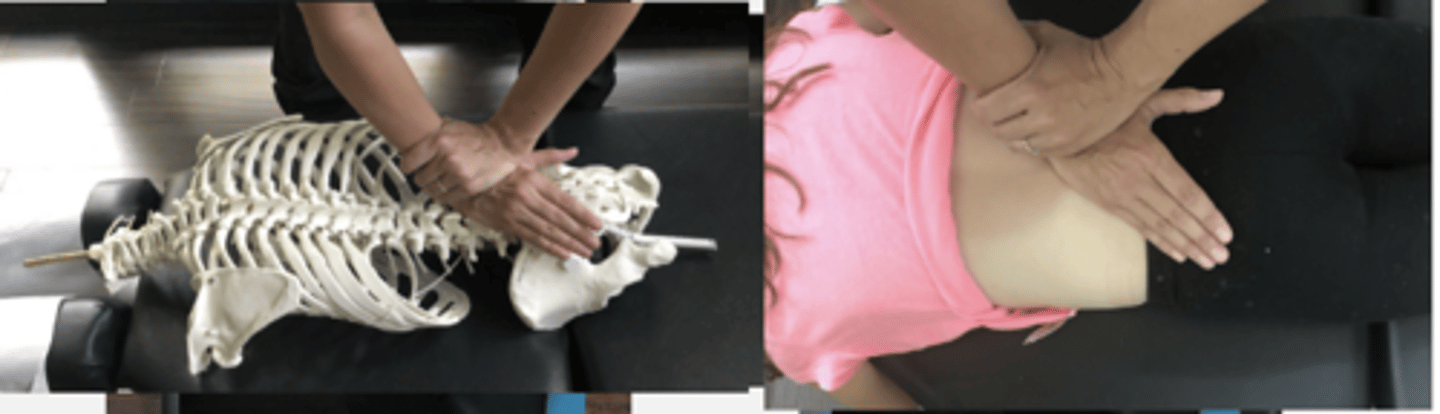
Technique:Prone (Unilateral) Hypothenar/Transverse Push
• PP: Prone, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Fencer or square stance facing caudal, side of adjustive contact, tissue slack M-L
• CH: Hypothenar of cephalic hand on Transverse Process (TP) (fingers running parallel to the spine)
• IH: Pisiform in anatomical snuff box, with fingers around wrist.
• Vector: P-A and S-I
• CLOSING THE WEDGE
Listing:
• T7 spinous process (SP) palpates closer to the T8 spinous process
• T7 has a flexion restriction
• T7 spinous is deviated inferior
Technique:Prone Bilateral Thenar/Transverse Push
• PP: Prone, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Modified fencer stance, facing cephalad, thumbs running parallel to the spine, a bolster can be placed under the adjustive contact to flexion preadjustive tension, tissue slack I-S
• CH: Thenar contact over superior TransverseProcess (TP)
• IH: Thenar contact over superior TransverseProcess (TP)
• Vector: P-A and I-S
**contact can be modified to bilateral hypothenar(knife-edge)
Listing:
• T8 transverse process (TP) palpates posterior on the right
• T8 TP palpates closer to the T9 TP on the right
• T8 has a left rotation and left lateral flexion restriction
• T8 spinous is deviated to the left and superior
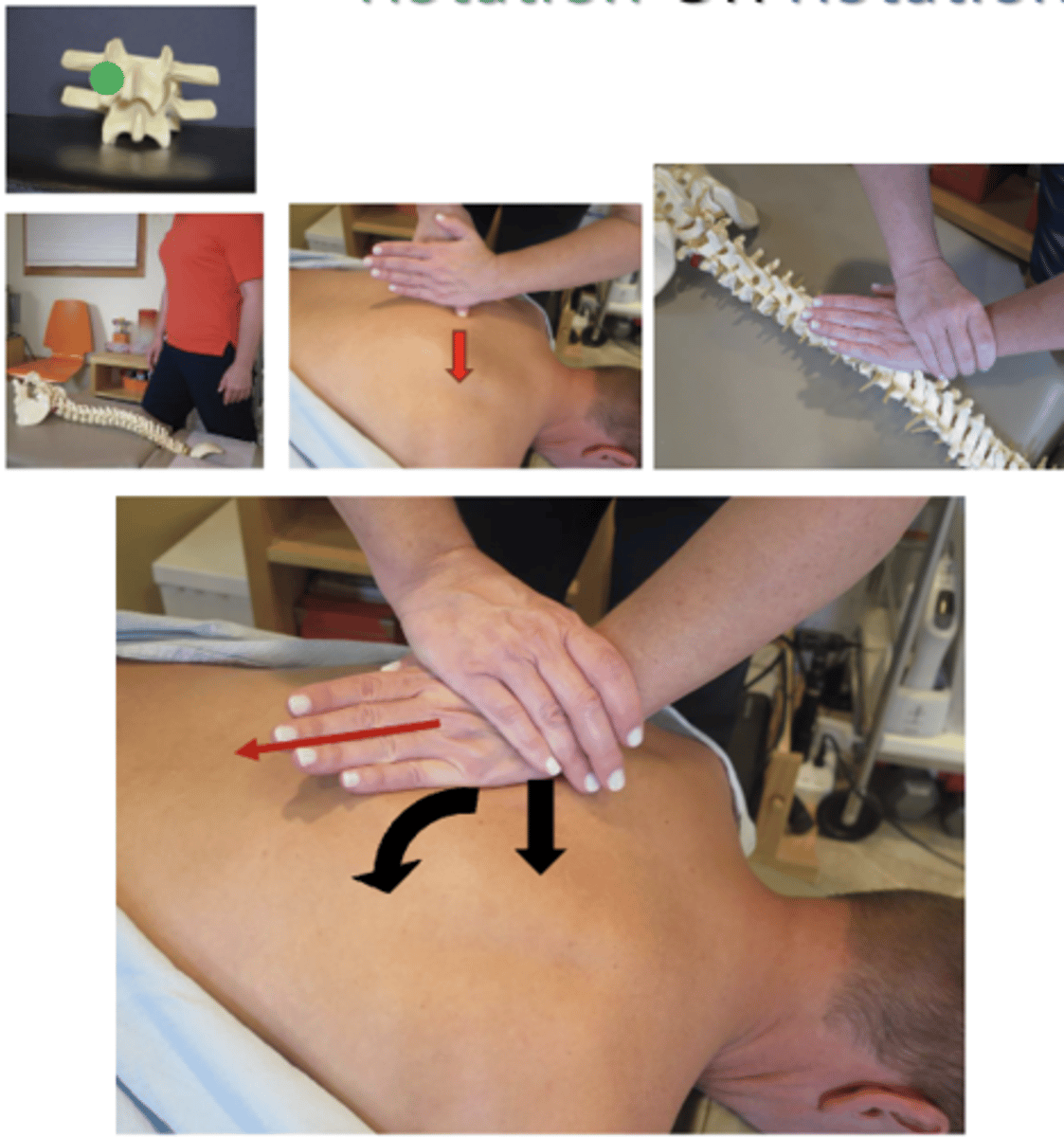
Technique:Prone (Unilateral) Hypothenar/Spinous Push
• PP: Prone, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Square or fencer stance facing caudal, side of contact, at cephalad end of the table, tissueslack L-M
• CH: Hypothenar of cephalad hand on lateral surface of superior Spinous Process (SP) on the side of rotation. Then, torque hand 45 degrees so that little finger CROSSES the Spine.
• Left hand counterclockwise torque, righthand clockwise torque
• IH: Hypothenar in anatomical snuff box, stabilize contact.
• Vector: P-A and L-M with torque (or S-I)
Listing:
• T4 spinous process (SP) palpates closer to the T5 spinous process (SP)
• T4 has a flexion restriction
• T4 spinous deviates is inferior
Technique: Prone Knife Edge/Spinous Push
• PP: Prone, headrest in flexion, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Fencer stance, facing cephalad, center of gravity caudal to contact, drawing tissue slack inferior to superior
• CH: Mid-knife edge contact on the inferior edge of the superior spinous process
• IH: Calcaneal reinforcement with fingers pointing cephalad
• Vector: I-S with enough P-A to stay onSpinous Process (SP)
Listing:
• A gap palpates between the T6 spinous process and T7 spinous process
• T6 has an extension restriction
• T6 spinous deviates superior
Technique: Prone Knife Edge/Spinous Push
• PP: Prone, head piece lowered, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Fencer stance, facing caudal, at cephalad end of the table, center of gravity over contact, draw tissue slack superior to inferior
• CH: Mid-knife edge contact on superior edge of superior spinous process
• IH: Calcaneal reinforcement with fingers pointing caudal
• Vector: P-A and S-I

Listing:
• T4 transverse process (TP) palpates posterior on the right
• T4 has a left rotation restriction
• T4 spinous is deviated to the left
Technique: Supine Opposite-Side Thenar/Transverse Drop
• PP: Supine, arms crossed on shoulders, patient in flexed position , asks permission to open gown, verbalize finding the segment
• DP: Modified fencer, opposite side of contact, tissue slack from below
• CH: Unilateral thenar contact on superior segment
• IH: Contacts the patient's crossed arms
• Vector: A-P to induce rotation

Listing:
• A gap between T6 spinous process (SP) and the T7 spinous process (SP)
• T6 has an extension restriction
• T6 spinous is deviated superior
Technique: Supine Opposite-Side Thenar/Transverse Drop
• PP: Supine, arms crossed on shoulders, NO FLEXION, asks permission to open gown, verbalize finding the segment
• DP: Modified fencer, opposite side of contact, tissue slack from above
• CH: Bilateral thenar contact onINFERIOR segment
• IH: Contacts the patient's crossed arms
• Vector: A-P to induce extension•
*we are avoiding putting the patient in flexion because we want to induce EXTENSION
Listing:
• T5 spinous process (SP) palpates closer to the T6 spinous process (SP)
• T5 has a flexion restriction
• T5 spinous is deviated inferior
Technique: Supine Opposite-Side Thenar/Transverse Drop
• PP: Supine, arms crossed on shoulders, patient in flexed position ,asks permission to open gown, verbalize finding the segment
• DP: Modified fencer, opposite side of contact, tissue slack from below
• CH: Bilateral thenar OR spinous contact on superior segment
• IH: Contacts the patient's crossed arms
• Vector: A-P and I-S to induce flexion
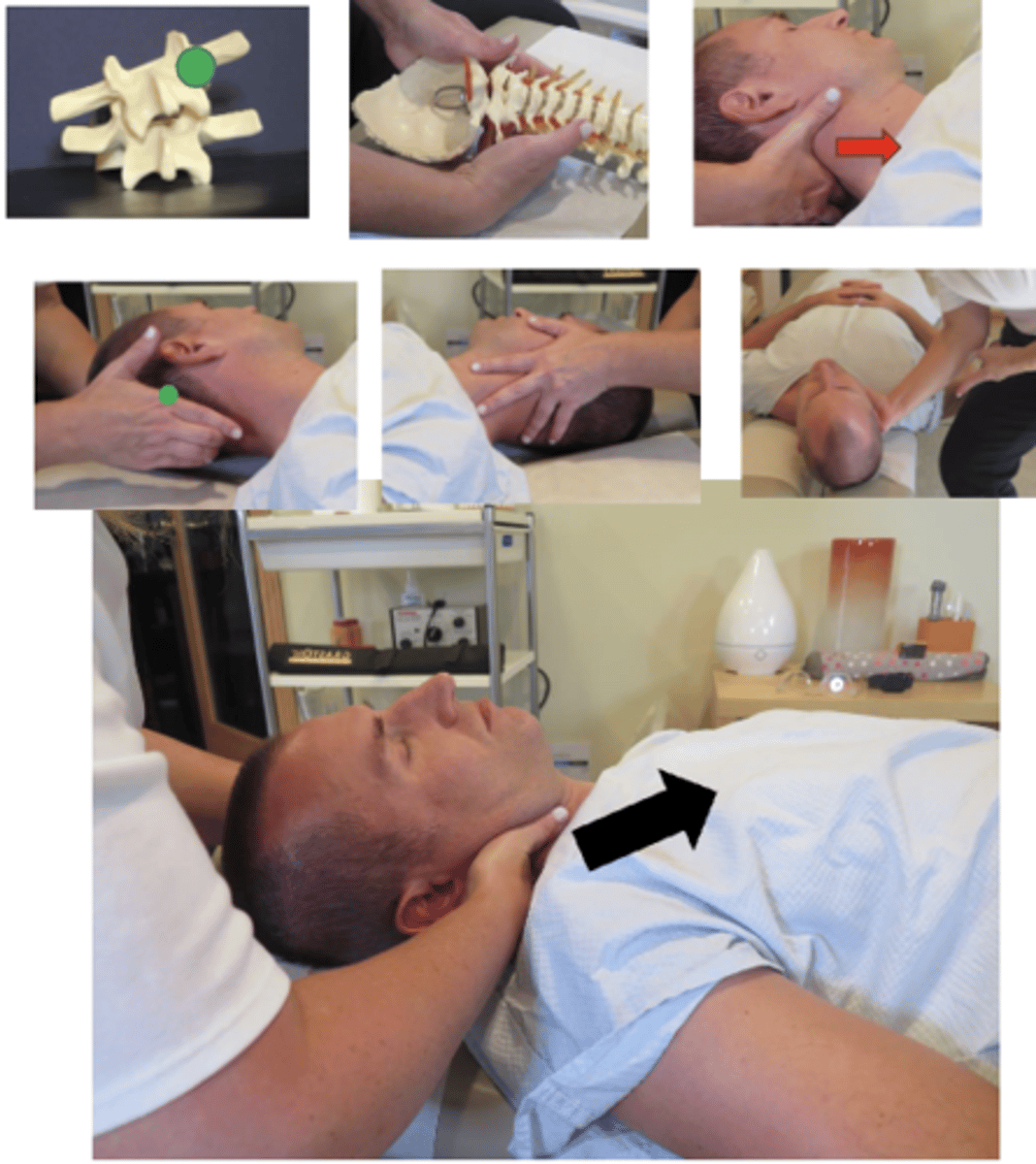
Listing:
• C5 articular pillar (AP) palpates posterior on the right
• C5 has a left rotation restriction
• C5 spinous is deviated to the left
Technique:Supine Index/Pillar Push
• PP: Supine, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Towards head of table, on side of contact, angled 45°-90° to the patient, tissue slack M-L
• CH: Proximal metacarpophalangeal index of the hand corresponding to the side of segmental contact, on posterolateral articular pillar of superior vertebrae, fingers reinforce
• IH: #1-cradles patients head, supports contralateral occiput and upper cervical spine
• VEC: P-A with counterclockwise rotation ( or clockwise depending on direction

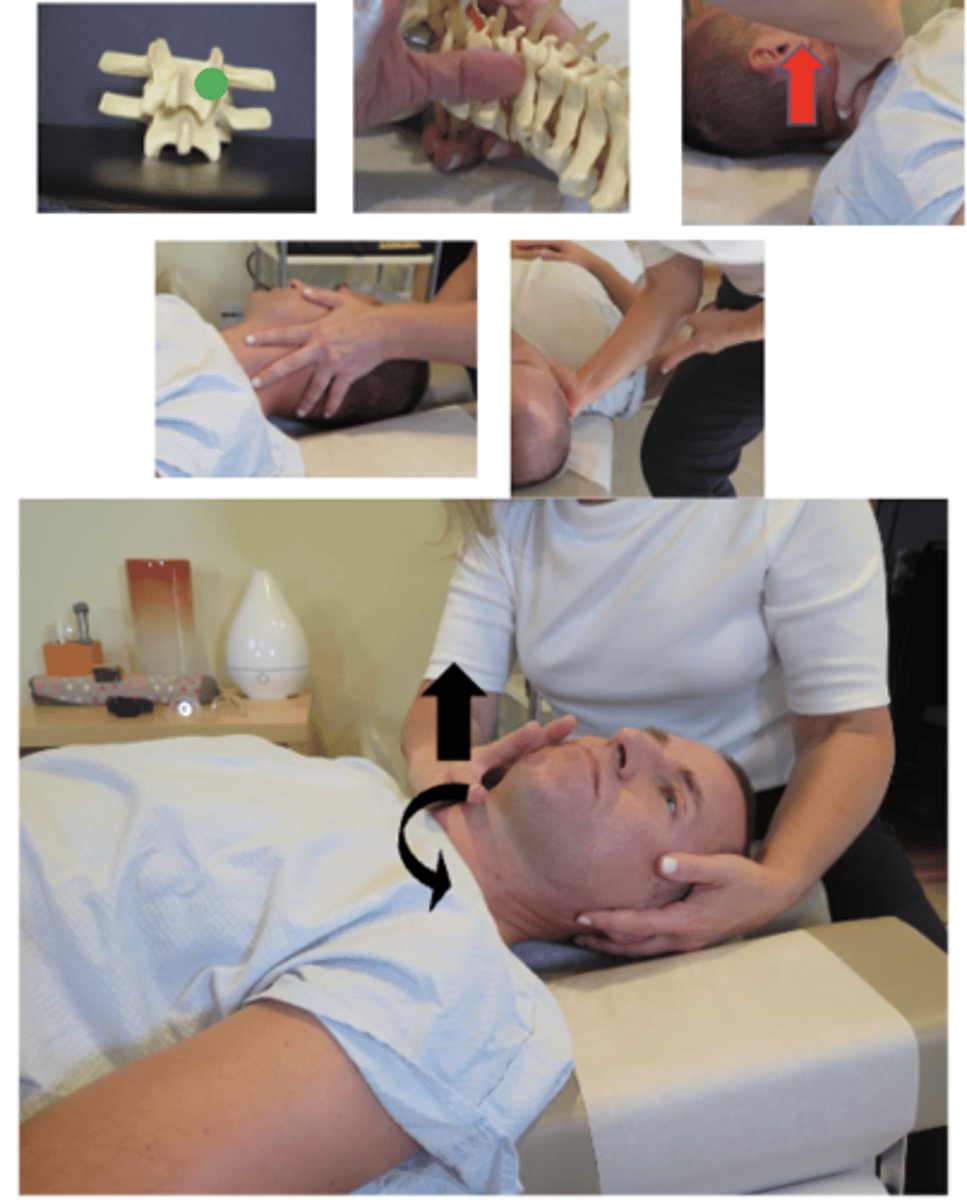
Listing:
On a APLC x-ray endplate lines converge on the left for C6 and C7
C6 has a right lateral flexion restriction
C6-C7 has an open wedge on the right side
Technique:Supine Index/Pillar Push
• PP: Supine, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Towards head of table, on side of contact, laterally flexing head toward contact, minimizing rotation, tissue slack S-I
• CH: Proximal metacarpophalangeal index of the hand corresponding to the side of segmental contact, on posterolateral articular pillar of superior vertebrae, fingers reinforce
• IH: #1-cradles patients head, supports contralateral occiput and upper cervical spine
• VEC: L-M and S-I• CLOSING THE WEDGE
Listing:
• C4 articular pillar (AP) palpates posterior on the right
• C4 has a left rotation restriction
• C4 spinous is deviated to the left
Technique:Supine Thumb/Pillar Push
• PP: Supine, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Towards head of table, on side of contact, approximately 90° to patient, tissue slack M-L
• CH: Palmar surface of thumb of the hand corresponding to the side of segmental contact, on posterolateral articular pillar of superior vertebrae, palm turned down, finger rest on cheek
• IH: #1-cradles patients head, supports contralateral occiput and upper cervical spine
• VEC: P-A and slight I-S (think up and over)with counterclockwise (or clockwise rotation depending on the direction)
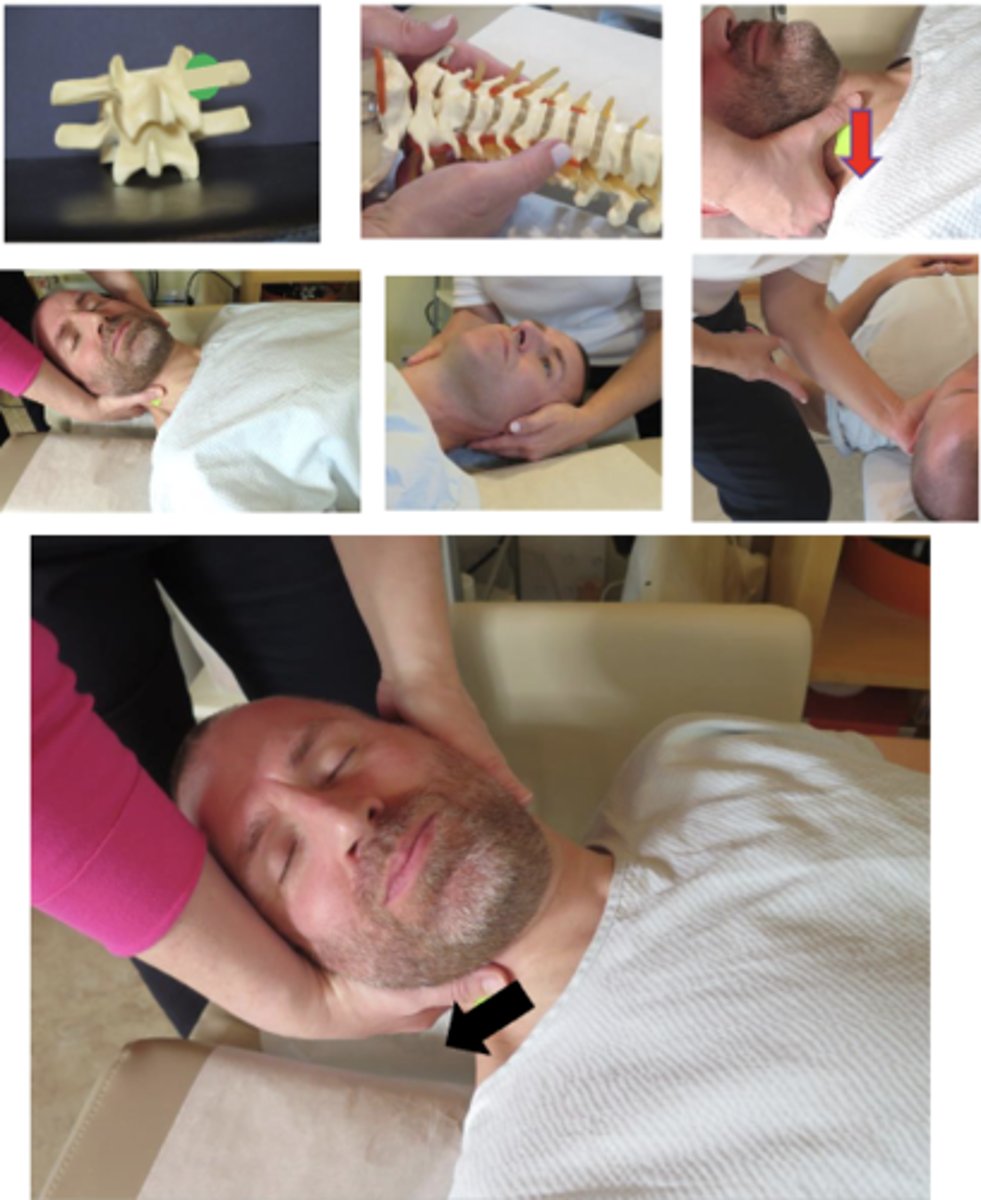
Listing:
• C5 articular pillar (AP) palpates posterior on the left
• C5 has a right rotation restriction
• C5 spinous is deviated to the right
Technique:Supine Thumb/Pillar Pull
• PP: Supine, ask permission to open gown/contact patient, verbalize finding the segment
• DP: Towards head of table, OPPOSITE side of contact, 45° to patient, tissue slack M-L
• CH: Palmar surface of thumb of the hand corresponding to the side of segmental contact, on anterolateral articular pillar of superior vertebrae, palm turned up, fingers supporting the occiput
• IH: Fingers cupping ear, supports contralateral occiput and upper cervical spine
• VEC: A-P and slight I-S inducing clockwise rotation (or counterclockwise rotation depending on the direction)
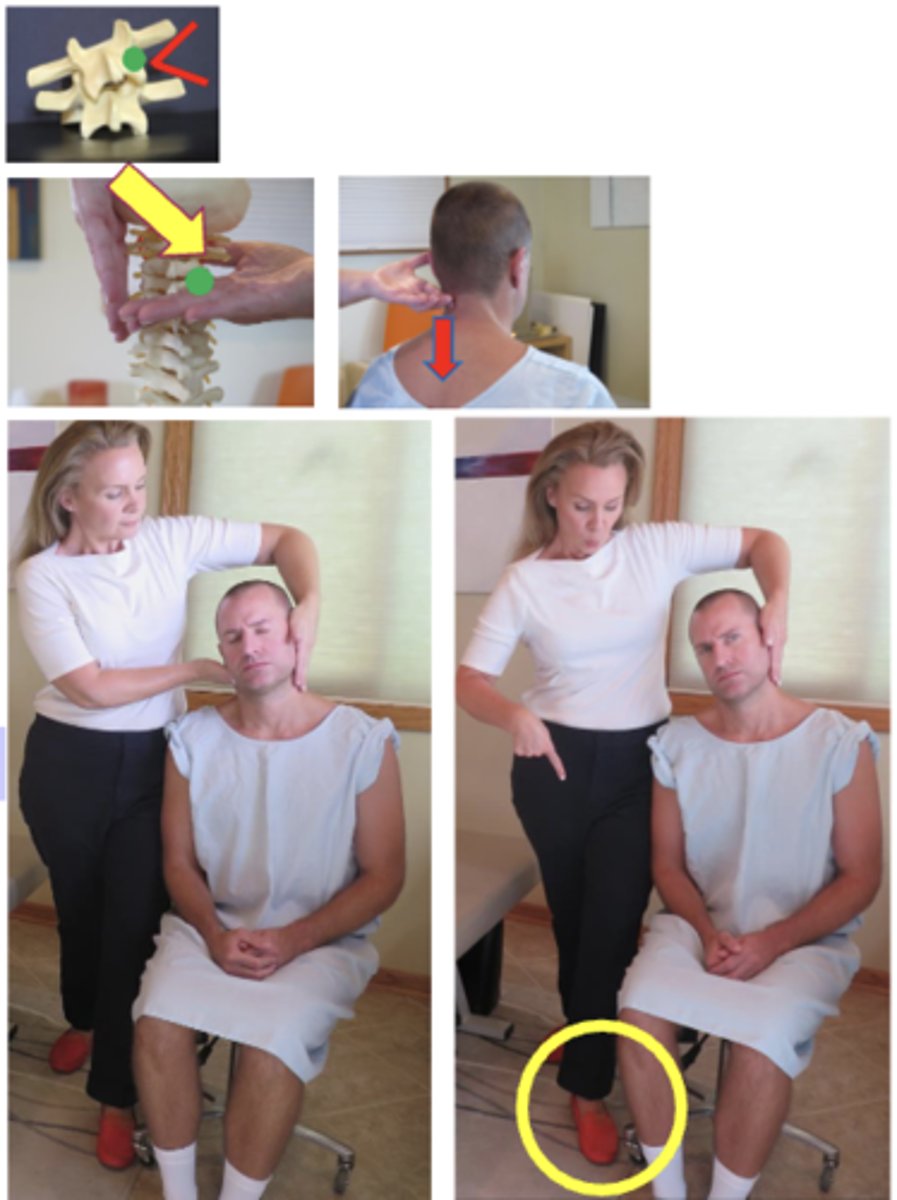
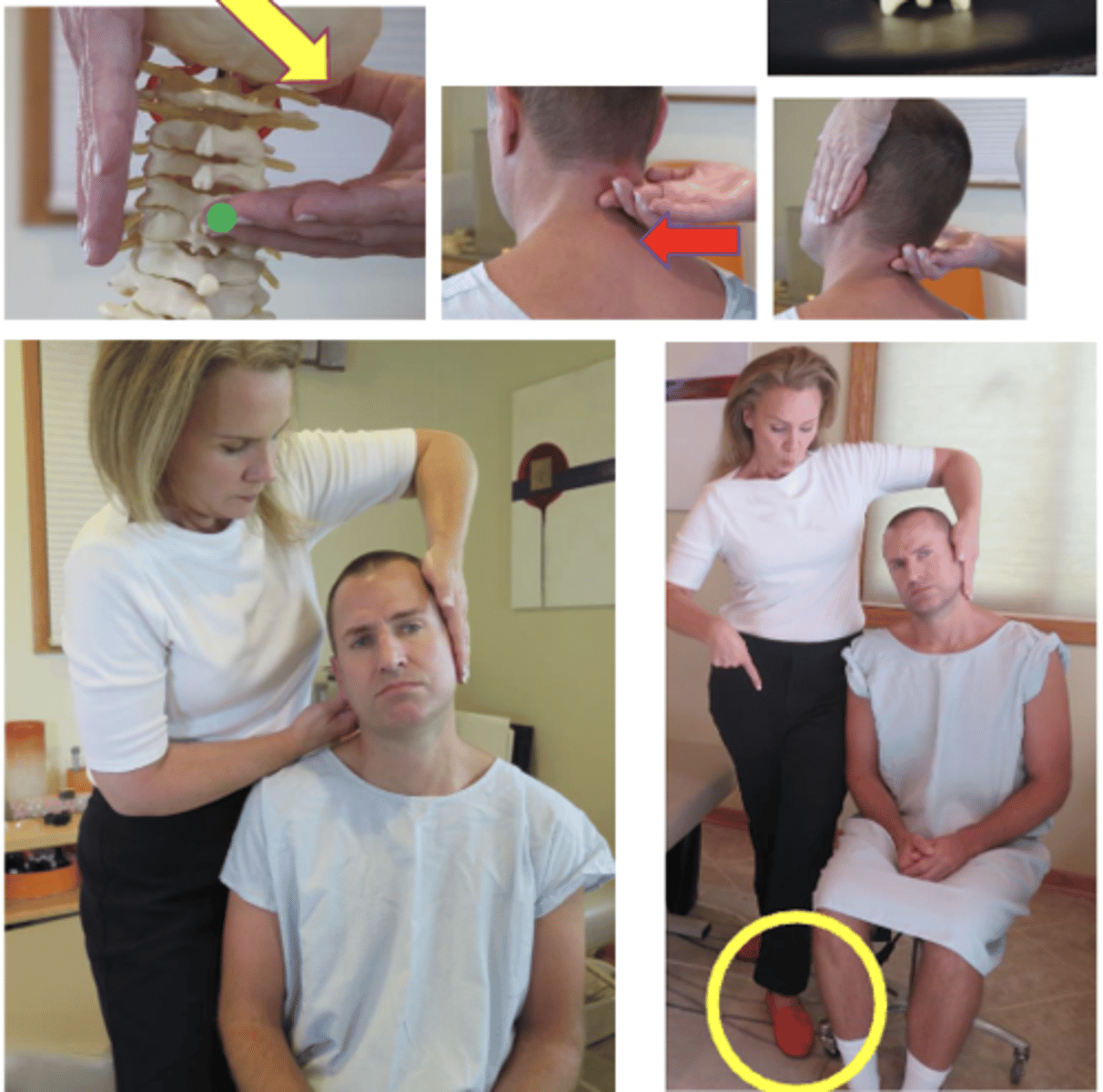
Listing:
On a APLC x-ray endplate lines converge on the left for C5 and C6
C5 has a right lateral flexion restriction
C5-C6 has an open wedge on the right side
Technique:Seated Index/Pillar Push
• PP: Seated in a chair with back, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Stands behind patient, same side as contact, doctor has leg OPPOSITE of contact hand forward, tissue slack S-I
• CH: 2nd digit on articular pillar of superior segment of contact, palm up, THUMB resting on patient's cheek
• IH: Indifferent hand #1, Elbow up and forearm pointing down, fingers pointing down, stabilize opposite occiput & cheek
• VEC: L-M for lateral flexion malposition (close the wedge)
**P-A w/ clockwise or counterclockwise torque for rotationmalposition
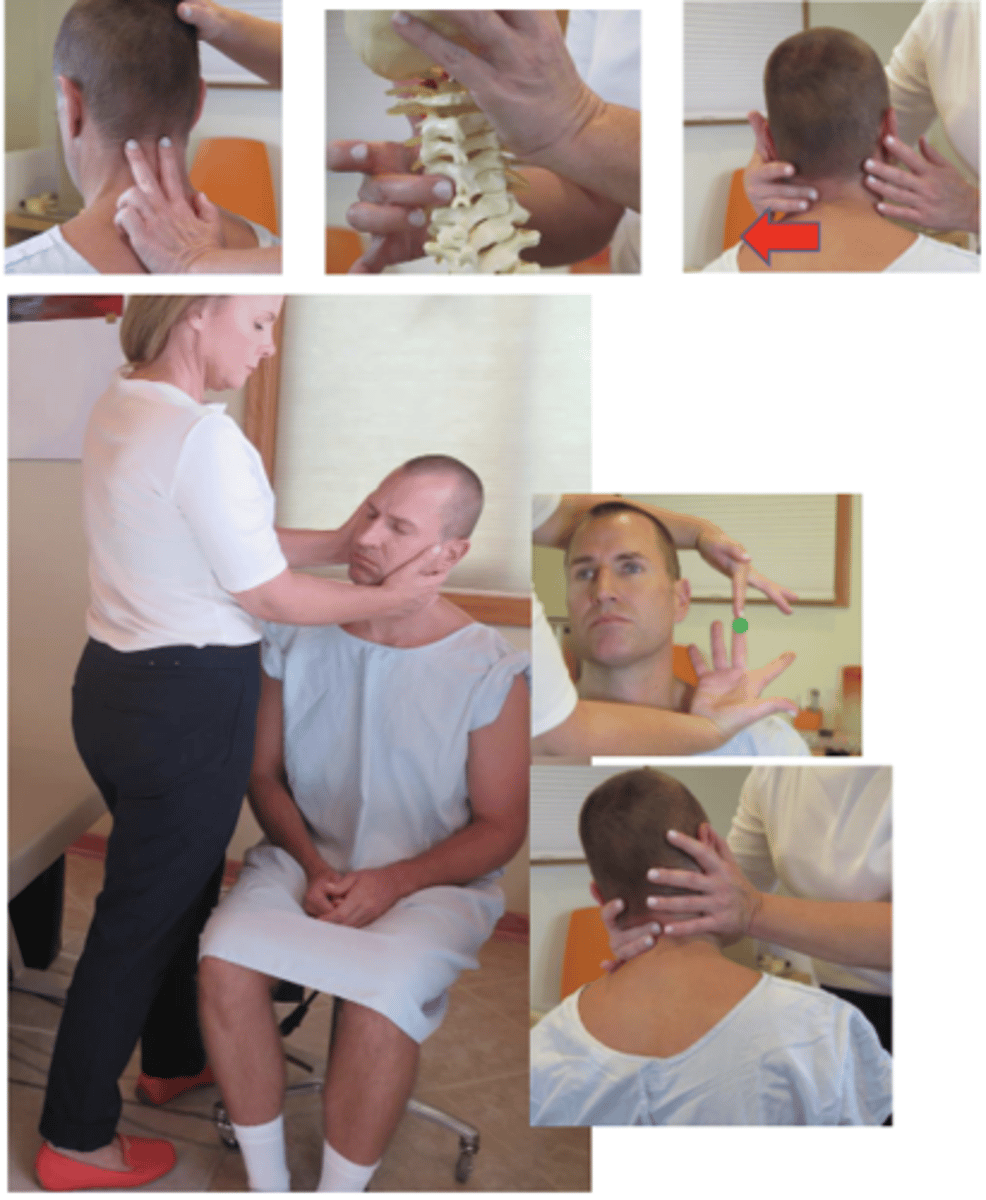
Listing:
• C3 articular pillar (AP) palpates posterior on the left
• C3 has a right rotation restriction
• C3 spinous is deviated to the right
Technique: Seated Digit/Pillar Pull
• PP: Seated in a chair with back, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Stand facing patient, opposite side of contact, reaching across to contact superior segment of posterior articular pillar, tissue slack M-L
• CH: Middle digit on the posterior AP, with palm resting on patient's cheek, remaining fingers supporting head.
• IH: Stabilize head/occ, supporting temporal region, on opposite side contact
• Vec: P-A slight I-S w/clockwise or counterclockwise rotation
Listing:
• C5 articular pillar (AP) palpates posterior on the left
• C5 has a right rotation restriction
• C5 spinous is deviated to the right
Technique:Seated Digit/Spinous Push
• PP: Seated in a chair with back, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Stand behind patient, side of contact,TISSUE SLACK AP to SP (L-M), laterally flex over contact, doctor has leg OPPOSITE of contact hand forward
• CH: 2nd digit on lateral spinous process of contact, palm up, THUMB resting on patient's cheek/behind ear (rat hole)
• IH: Indifferent hand #1, elbow up and forearm pointing down, fingers pointing down, stabilize opposite occiput and cheek
• Vec: P-A and L-M (in line with the patient's eyes)
Listing:
• C3 articular pillar (AP) palpates posterior on the right
• C3 has a left rotation restriction
• C3 spinous is deviated to the left
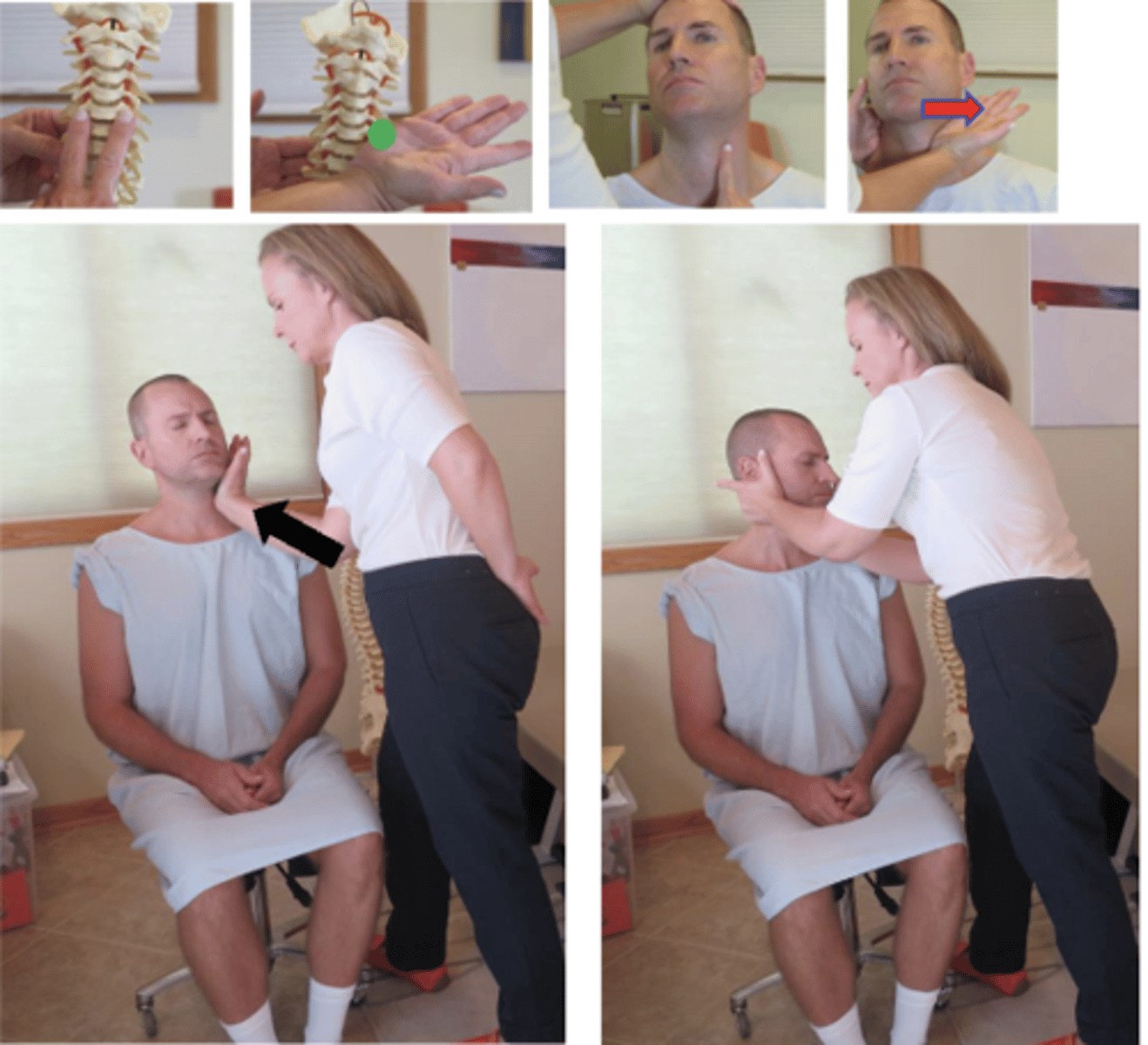
Technique:Seated Hypothenar/Pillar Push
• PP: Seated in a chair with back, asks permission to open gown/contact patient, verbalize finding the segment
• DP: Doctor stands in front of patient, same side as contact, fencer stance, tissue slack M-L, laterally flex away and rotate over contact
• CH: anterolateral aspect of AP, pisiform hypothenar, with finger of hand obliquely vertical to provide support to head
• IH: Reaches around cups occiput
• LOD: A-P and slight I-S
Listing:
• C3 articular pillar (AP) palpates posterior on the left
• C3 has a right rotation restriction
• C3 spinous is deviated to the right
Technique:Prone Index/Pillar Push
• PP: Prone, asks permission to open gown/contact patient, verbalize finding the segment
• DP: fencer stance, facing cephalad EITHER side of contact, tissue slack M-L
• CH: Index on posterolateral aspect of superior articular pillar, on the side of rotation, fingers pointing down and thumb on posterior neck
• IH: #3, thumb under occiput, fingers along face/head opposite side of contact (distract and rotate head to side of contact)
• Vec: P-A and I-S
**P-A and S-I for lateral flexion malposition (closing thewedge)

Listing:
• C1 transverse process (TP) palpates posterior on the left in relationship to the C2 posterior articular pillar (AP)
• C1 has a right rotation restriction
Technique:Supine Index/Atlas Push
• PP: Supine, permission to contact the neck, identify how you found the segment
• DP: Towards head of table, on side of contact, angled 45°-90° to the patient, tissue slack M-L
• CH: Proximal ventral surface of index of the hand corresponding to the side of segmental contact, on posterior aspect of ATLAS TP, thumb rests on cheek
• IH: #1-cradles patients head, supports contralateral occiput and upper cervical spine
• VEC: P-A with clockwise (or counterclockwise depending on the listing)

Listing:
• C1 transverse process (TP) palpates medial on the right
• C1 transverse process (TP) end feel has loss of spring lateral to medial on the left
• C1 has a left lateral flexion restriction
Technique:Supine Index/Atlas Push
• PP: Supine, permission to contact the neck, identify how you found the segment
• DP: Towards head of table, on side of contact, angled 45°-90° to the patient, laterally flexing head over contact, minimizing rotation, tissue slack S-I
• CH: Proximal ventral surface of index of the hand corresponding to the side of segmental contact, on lateral aspect of ATLAS TP, thumb rests on cheek
• IH: #1-cradles patients head, supports contralateral occiput and upper cervical spine
• VEC: L-M•
**"TRANSLATION" of C1 due to 5° of lateral flexion

• C1 transverse process (TP) palpates posterior on the left in relationship to the C2 posterior articular pillar (AP)
• C1 has a right rotation restriction
Technique:Seated Digit/Atlas Pull
• PP: Seated in a chair with a back, permission to contact the neck, identify how you found the segment
• DP: Stand facing patient, opposite side of contact, reaching across to contact atlas transverse, tissue slack M-L
• CH: Middle digit on the ATLAS TP, palm resting on patient's cheek, remaining fingers supporting head.
• IH: Stabilize head/occ, supporting temporal region, on opposite side contact
• Vec: P-A w/clockwise rotation (or counterclockwise depending on the listing)

Listing:
• C1 transverse process (TP) palpates posterior on the left in relationship to the C2 posterior articular pillar (AP)
• C1 has a right rotation restriction
Technique:Seated Index/Atlas Push
• PP: Seated in a chair with a back, permission to contact the neck, identify how you found the segment
• DP: Stand behind patient, side of contact, doctor has leg OPPOSITE of contact hand forward, tissue slack M-L
• CH: Proximal ventral surface of index of the hand corresponding to the side of segmental contact, on posterior aspect of ATLAS TP, palm up, wrist straight, remaining fingers cup lower occiput
• IH: Indifferent hand #1, elbow up and forearm pointing down, fingers pointing down, stabilize opposite occiput and cheek
• Vec: P-A w/clockwise rotation (or counterclockwise depending on the listing)
Listing:
• C1 TP palpates medial on the left
• C1 TP end feel has loss of spring lateral to medial on the right
• C1 has a right lateral flexion restriction
Technique:Seated Index/Atlas Push
• PP: Seated in a chair with a back, permission to contact the neck, identify how you found the segment
• DP: Stand behind patient, side of contact, doctor has leg OPPOSITE of contact hand forward, tissue slack S-I
• CH: Proximal ventral surface of index of the hand corresponding to the side of segmental contact, on posterior aspect of ATLAS TP, palm up, wrist straight, remaining fingers cup lower occiput
• IH: Indifferent hand #1, elbow up and forearm pointing down, fingers pointing down, stabilize opposite occiput and cheek
• Vec: L-M• **"TRANSLATION" of C1 due to 5° of lateral flexion
Listing:
• A bilateral opening palpates between the ramus of the jaw and the bilateral transverse processes of C1
• The occiput has a flexion restriction
Technique:Seated Calcaneal/Zygomatic Pull
• PP: Seated in chair with a back, permission to contact the face, identify how you found the segment, roll towel behind cervical spine to maintain curve
• DP: Stand behind patient, compressing patients head against your body, tissue slack S-I
• CH: Calcaneal contact of both hands, superior aspect of zygoma bilaterally, fingers pointing cephalad arching over patient eyes
• IH: same as contact hand
• Vec: S-I , with enough A-P to stay on contact
*long access distraction through the legs as a preadjustive tension
**alternate contact- reinforced pisiform/glabella

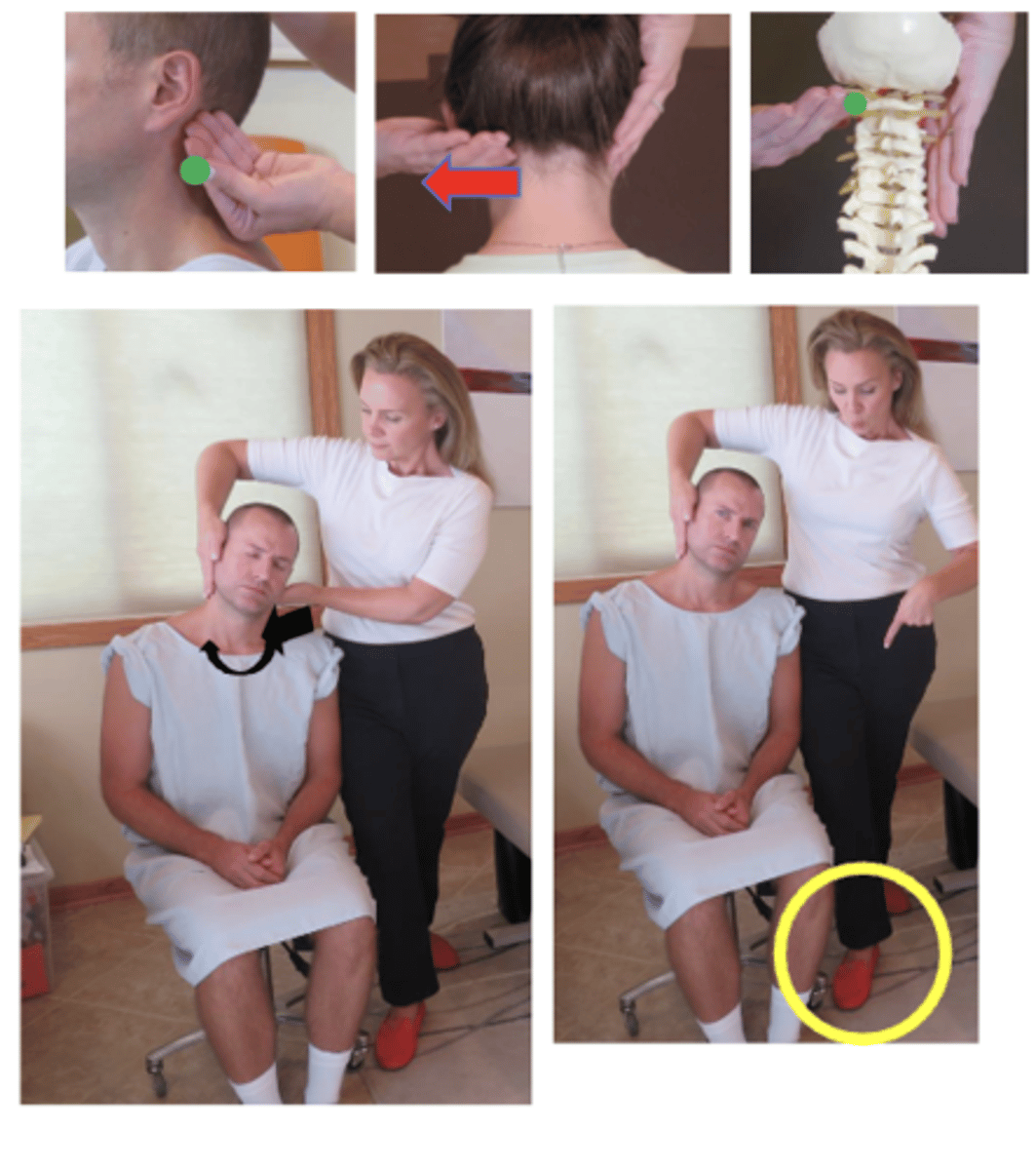
Listing:
• An open space palpates between the inferior right mastoid and superior right TP of C1
• A closed space palpates between the inferior left mastoid and superior left TP of C1
• Occiput has a right lateral flexion restriction
Technique:Seated Index/Occiput Lift
• PP: Seated in chair with a back, head turned away from side of contact, permission to contact the neck, identify how you found the segment
• DP: Stand behind patient, tissue slack M-L, resting patient's head against doctor's sternum
• CH: Proximal palmar surface of middle finger of hand corresponding to side of head rotation (reach around patients face to contact), contact on inferior border of occiput and lateral border of mastoid process on side of dysfunction
• IH: reinforce contact hand stabilizing patients head against doctor's sternum
• Vec: I-S and L-M (closing the wedge)
**develop pre-adjusted joint tension by distracting verticallywith arms and legs

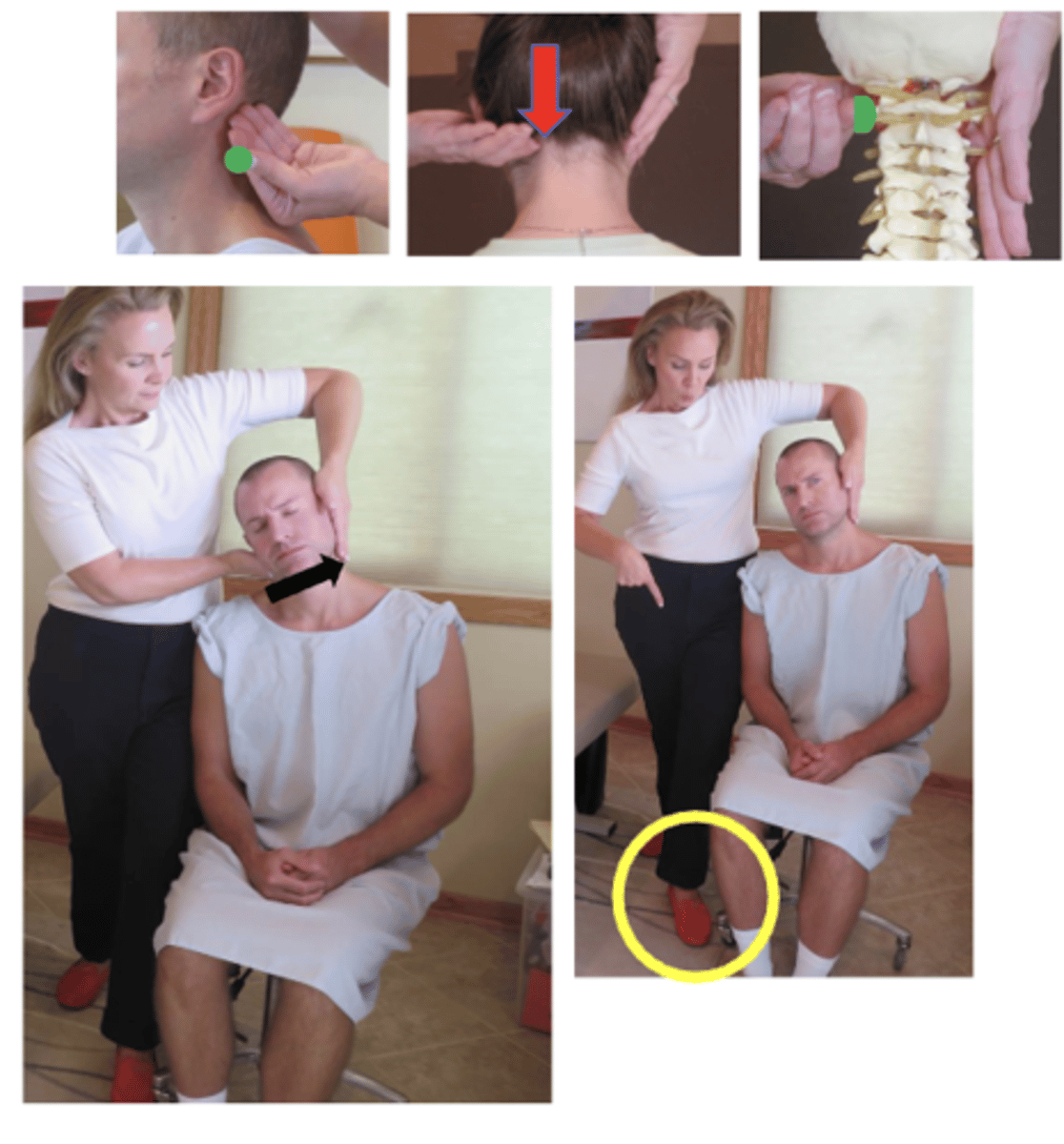
Listing:
• A closed space palpates between the ramus of the right jaw and the right C1 TP
• The occiput has a left rotation restriction
Technique:Seated Index/Occiput Push
• PP: Seated in chair with a back, permission to contact the neck, identify how you found the segment
• DP: Stand behind patient, towards side of contact, tissue slack S-I
• CH: Ventral lateral surface of index finger of the corresponding hand to the side of contact, palm turned up, wrist straight, forearm approximately 45° to patient , remaining fingers cupping lower occiput, superior mastoid groove on the side of contact
• IH: modified indifferent hand 1 # cups the patient's head and supports the contralateral occiput
• VEC: P-A with counterclockwise rotation (orclockwise depending on the listing)
Listing:
• An open space palpates between the inferior right mastoid and superior right TP of C1
• A closed space palpates between the inferior left mastoid and superior left TP of C1
• Occiput has a right lateral flexion restriction
Technique:Seated Index/Occiput Push
• PP: Seated in chair with a back, permission to contact the neck, identify how you found the segment
• DP: Stand behind patient, towards side of contact, tissue slack S-I
• CH: Ventral lateral surface of index finger of the corresponding hand to the side of contact, palm turned up, wrist straight, forearm approximately 45° to patient , remaining fingers cupping lower occiput, superior mastoid groove on the side of contact
• IH: modified in different hand 1# cups patient's head and supports the contralateral occiput
• VEC: L-M, S-I and P-A
*P-A because occiput is a posterior contact

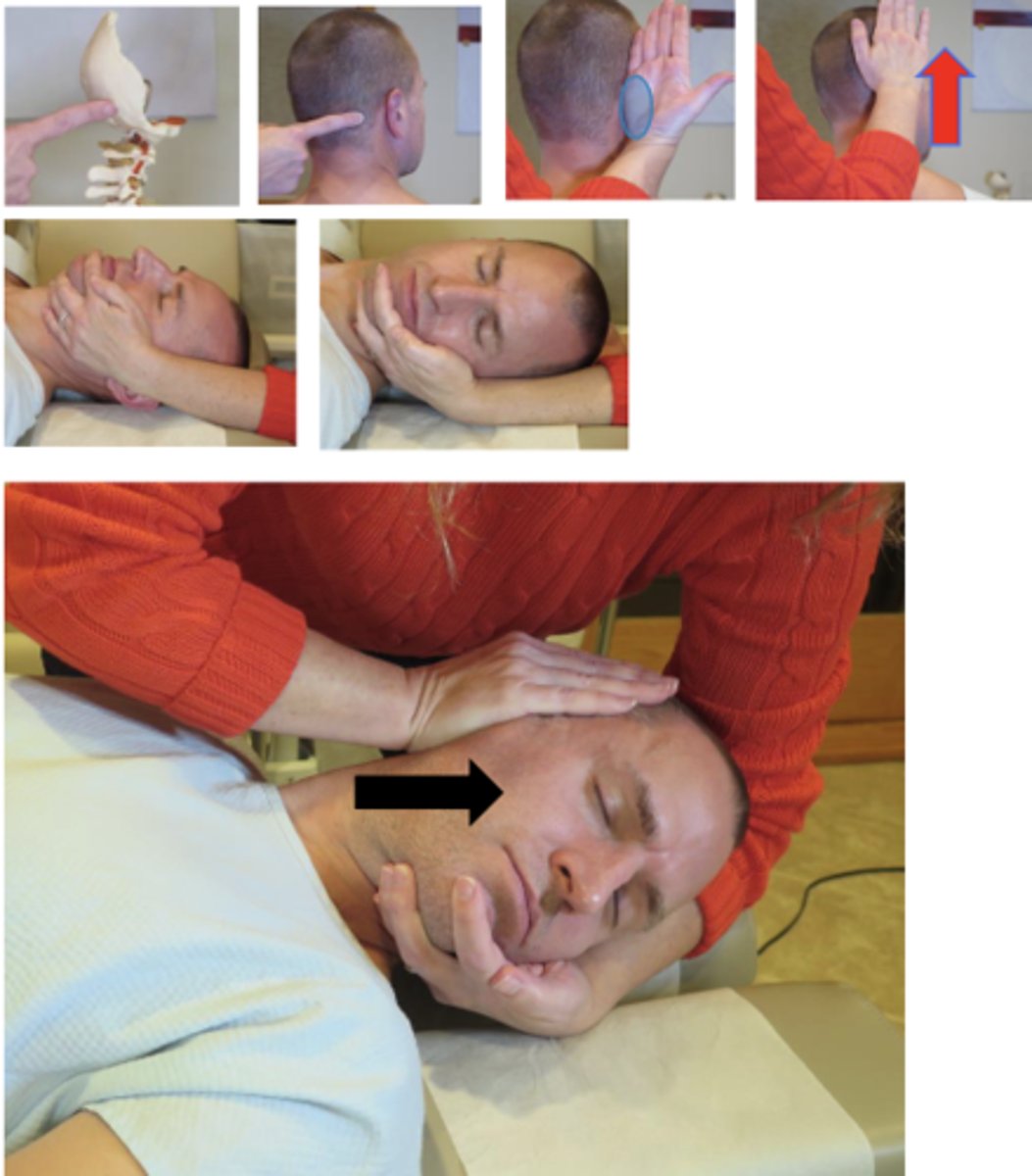
Listing:
• The bilateral mastoids palpate inferior with a closed space between the bilateral TP's of C1
• Occiput has a loss of long axis distraction
Technique:Supine Hypothenar/Occiput Lift
• PP: Supine, doctor supporting the patients head off the end of the table, patients had turned away from the side of contact, in neutral position, permission to contact the neck, identify how you found the segment
• DP: Standing at the head of the table, facing cephalad, on the side of adjustive contact, in a lower fencer stance, weight shifted toward the superior leg, apply pre-adjustive long axis distraction by leaning bodyweight headward, tissue slack I-S
• CH: Hypothenar of caudal hand, contacting inferior edge of occiput medial to the mastoid, fingers pointing vertically and resting on the skull
• IH: Fingers wrap around the patient's chin while forearm supports the patient's head
• VEC: I-S (think inducing long-axis distraction)
*minimize rotational tension on the upper cervical spine
Listing:
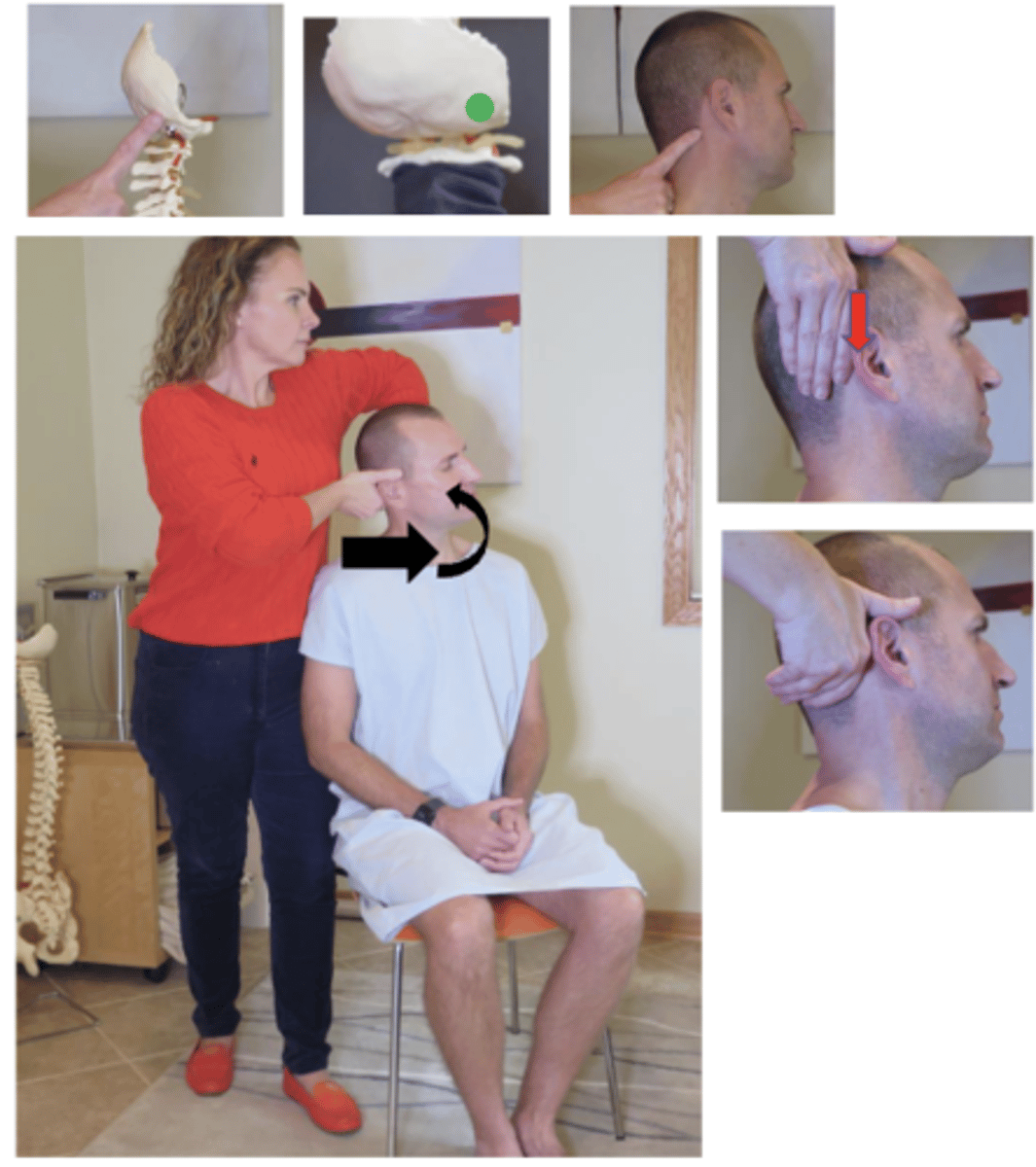
• A closed space palpates between the ramus of the right jaw and the right C1 TP
• The occiput has a left rotation restriction
Technique:Supine Thumb/Occiput Push
• PP: Supine, permission to contact the neck, identify how you found the segment, doctor supporting the patients head off the end of the table, patients had turned away from the side of dysfunction,
• DP: Towards head of table, on side of contact, angled 45°-90° to the patient, distract with legs, tissue slack M-L
• CH: Thumb of the hand corresponding to the side of segmental contact, posterior aspect of the mastoid, contact hand is arched to cup over the patient's ear, fingers resting on the angle of the jaw, forearm down the sternum
• IH: #1• VEC: P-A and I-S (Induce LAD with corkscrew-like motion)
Avoid inducing excessive upper cervical rotation
**alternate contact hand- index, thenar or hypothenar

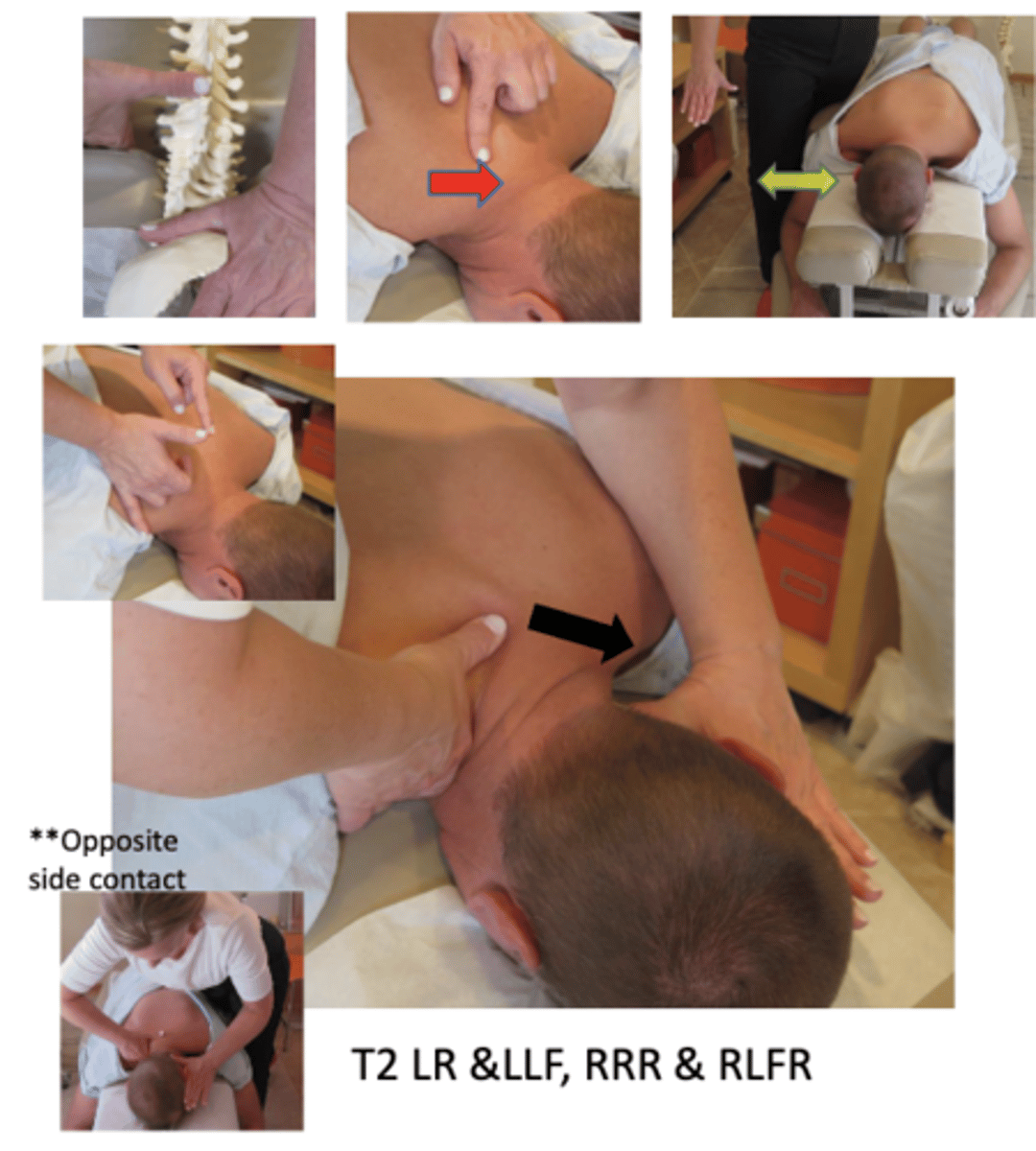
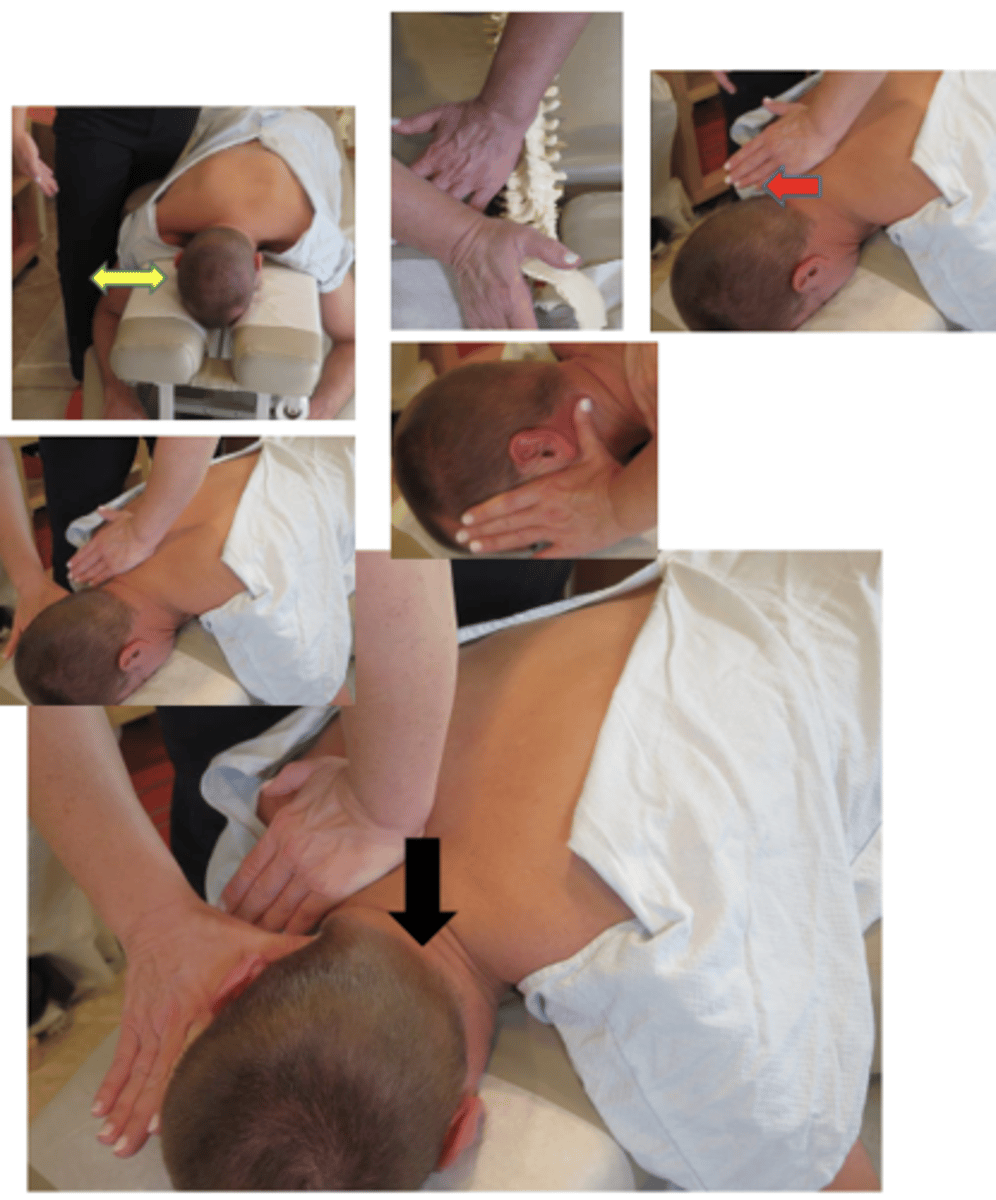
Listing:
• T2 transverse process (TP) palpates posterior on the left
• T2 TP palpates inferior in relationship to the T3 TP on the left
• T2 has a right rotation and right lateral flexion restriction
• T2 spinous is deviated to the right and superior
Technique:Prone Thumb/Spinous Push
• PP: Prone, headpiece below horizontal to produces light flexion in the thoracocervical spine, permission to open gown/contact, identify segment
• DP: Standing in low fencer stance on side of contact, facing cephalad, forward leg level at patient's head, body weight centered over midline of the patient
• CH: Distal palmer surface of cephalad thumb partially abducted and locked, fingers resting on trapezius, contacting lateral surface of spinous process
• IH: #3 thumb behind the occiput with fingers alongside the face opposite side of contact, inducing slight lateral flexion toward contact with distraction
• Vector: L-M, slight P-A
Additional contact - hypothenar OR OPPOSITE SIDEC6-T3
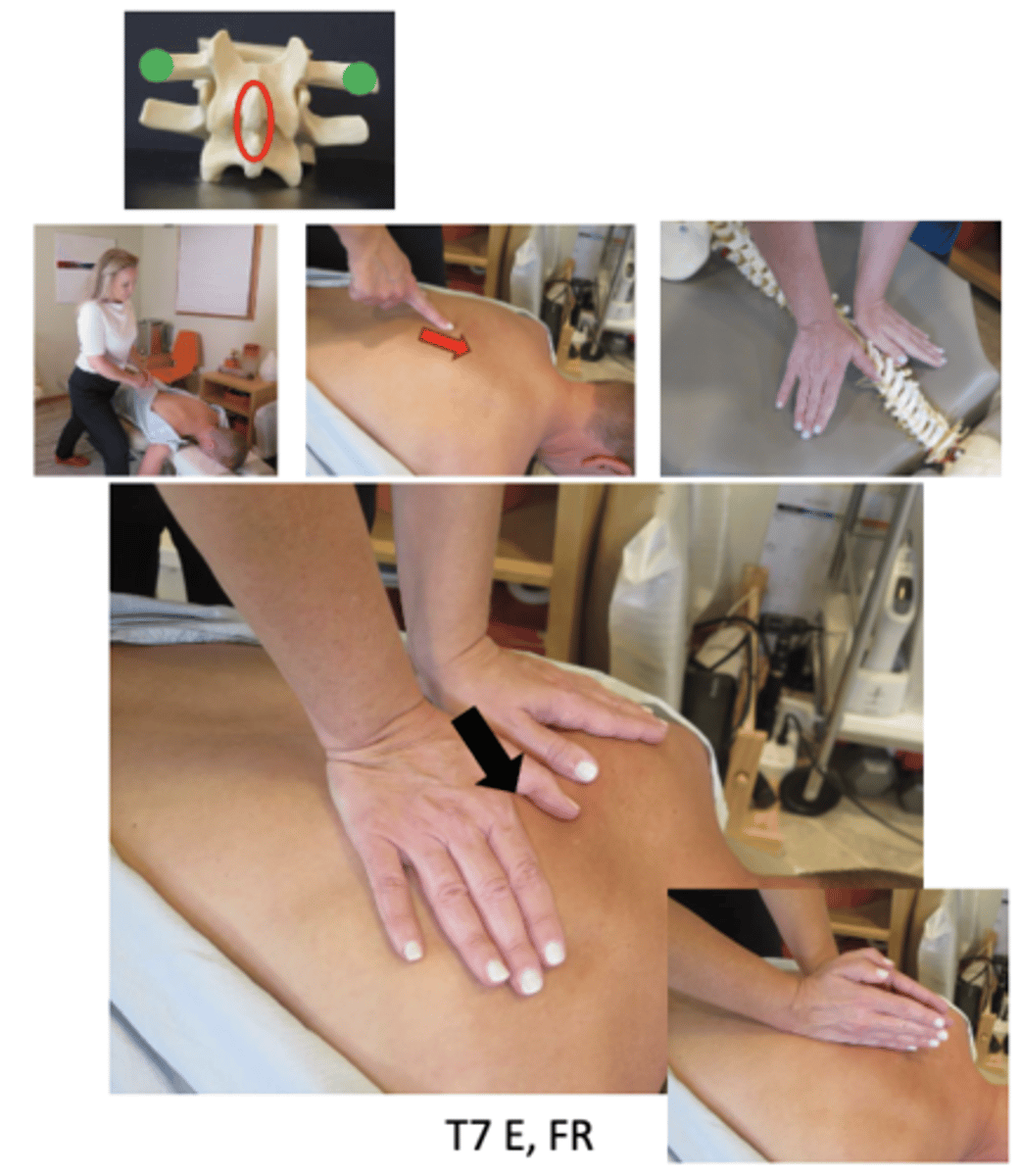
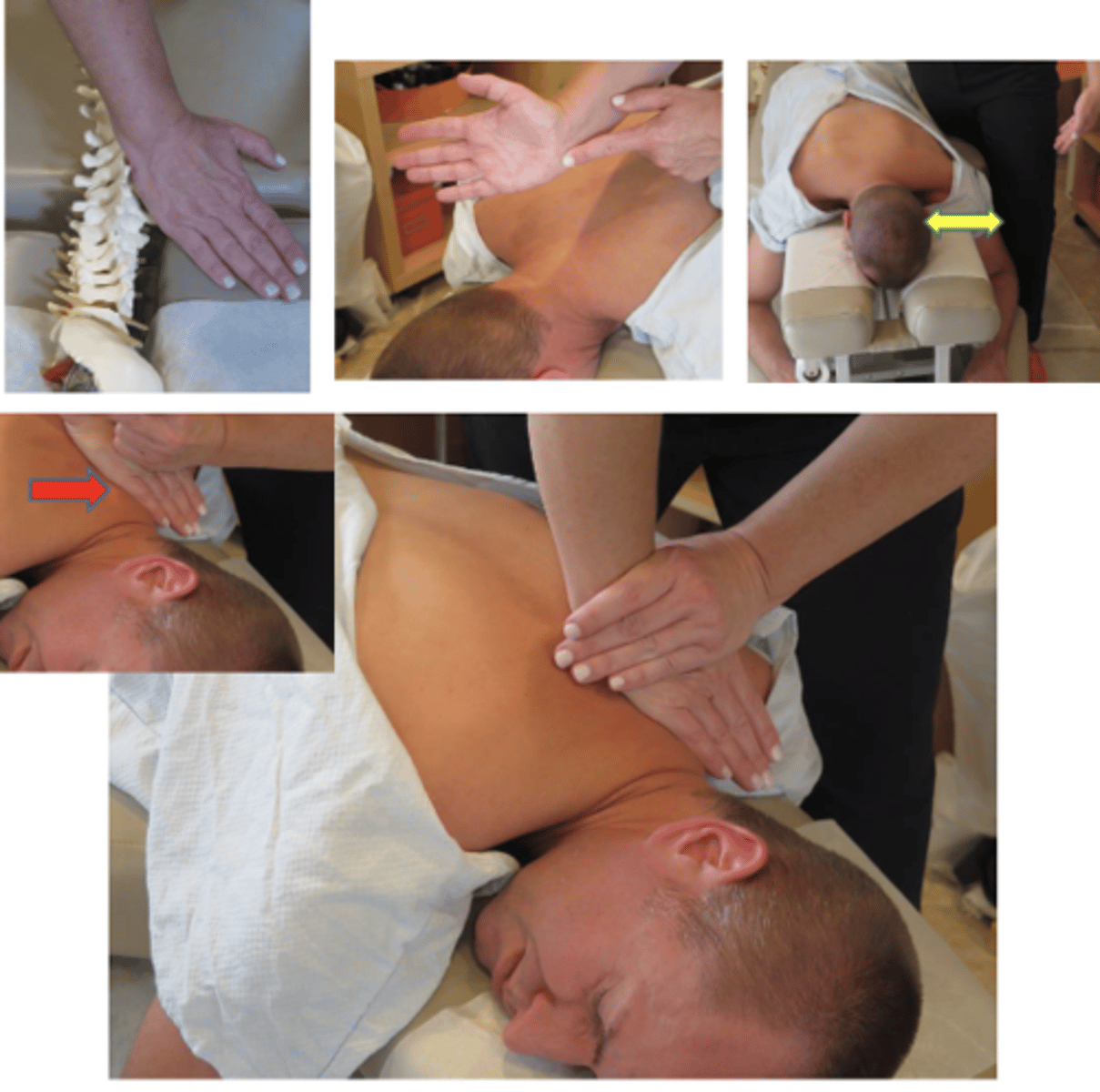
Listing:
• T3 transverse process (TP) palpates posterior on the right
• T3 has a left rotation restriction
• T3 spinous is deviated to the left
Technique:Prone Hypothenar/Transverse Push
• PP: Prone, headpiece below horizontal to produce slight flexion in the thoracocervical spine, permission to open gown/contact, identify segment
• DP: Standing in fencer stance on side of contact, facing cephalad, forward leg level at patient's head, body weight centered over midline of the patient
• CH: Hypothenar (pisiform) of caudal hand, contacting transverse process
• IH: #3 thumb behind the occiput with fingers alongside the face on side of contact, inducing slight lateral flexion away from contact, with distraction
• Vector: P-A
*C7-T4
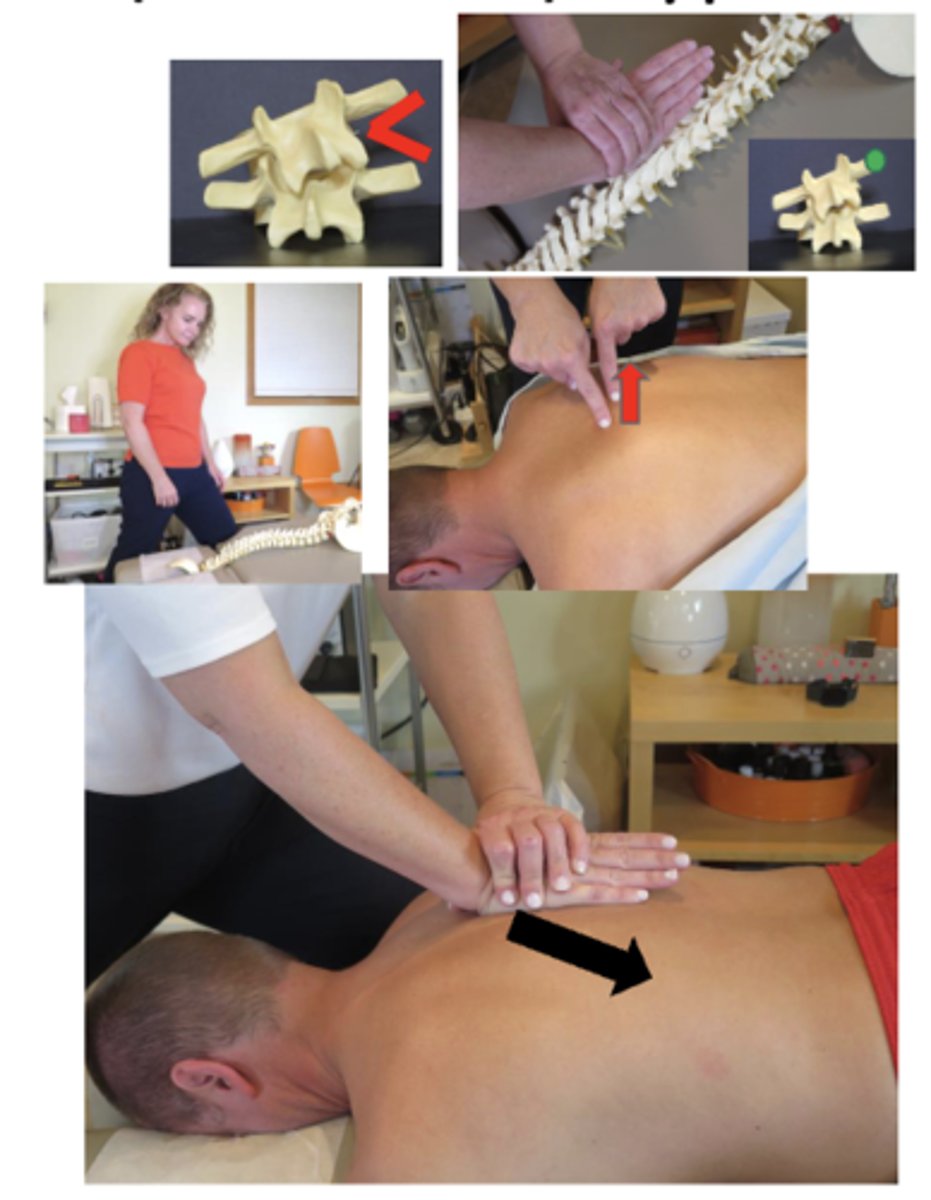
Listing:
• T2 transverse process (TP) palpates posterior on the left
• T2 has a right rotation restriction
• T2 spinous is deviated to the right
Technique:Prone Unilateral Hypothenar/Transverse Push
• PP: Prone, headpiece below horizontal to produce slight flexion in the thoracocervical spine, permission to open gown/contact, identify segment, patient is instructed to turn head AWAY from contact
• DP: Standing in fencer stance on side of contact, facing cephalad, forward leg level at patient's head, body weight centered over midline of the patient
• CH: Hypothenar (pisiform) of caudal hand, contacting transverse process
• IH: Reinforce over hypothenar contact
• Vector: P-A*C7-T4
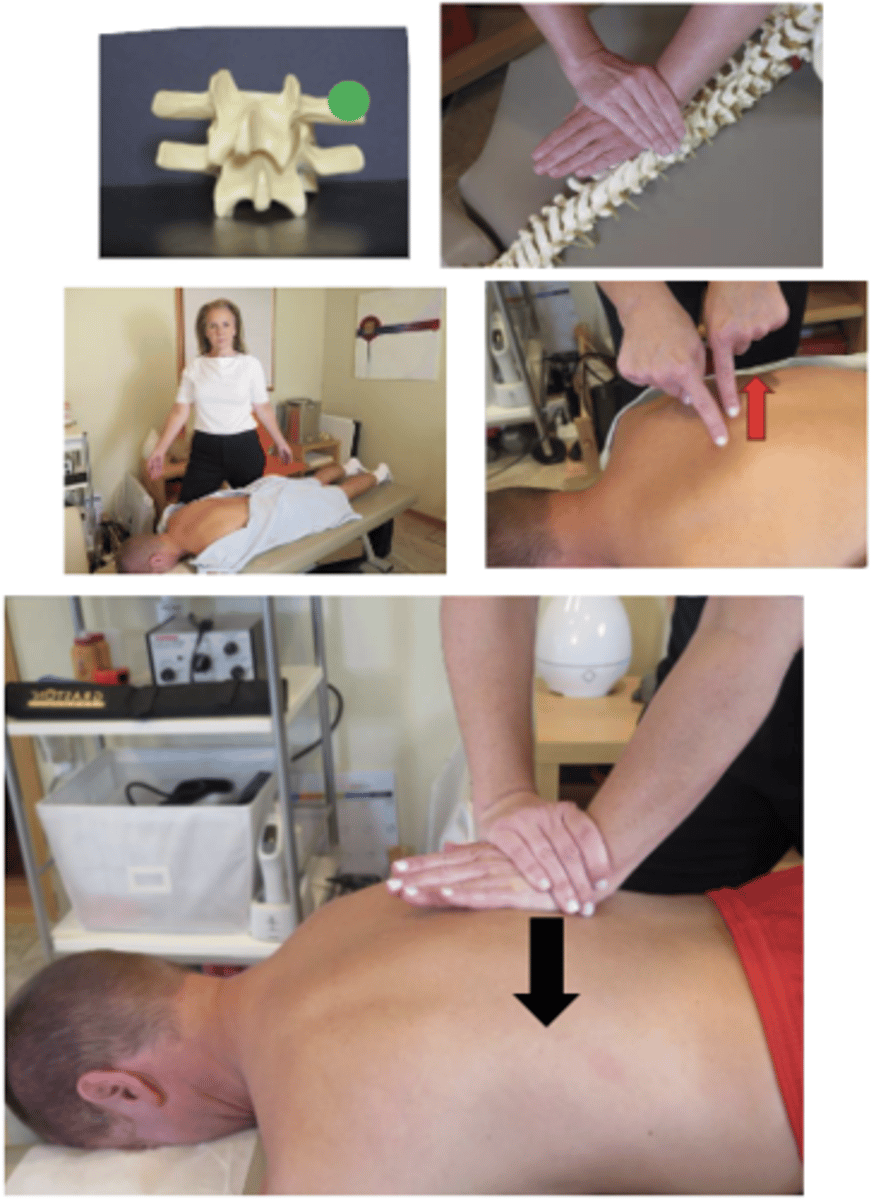
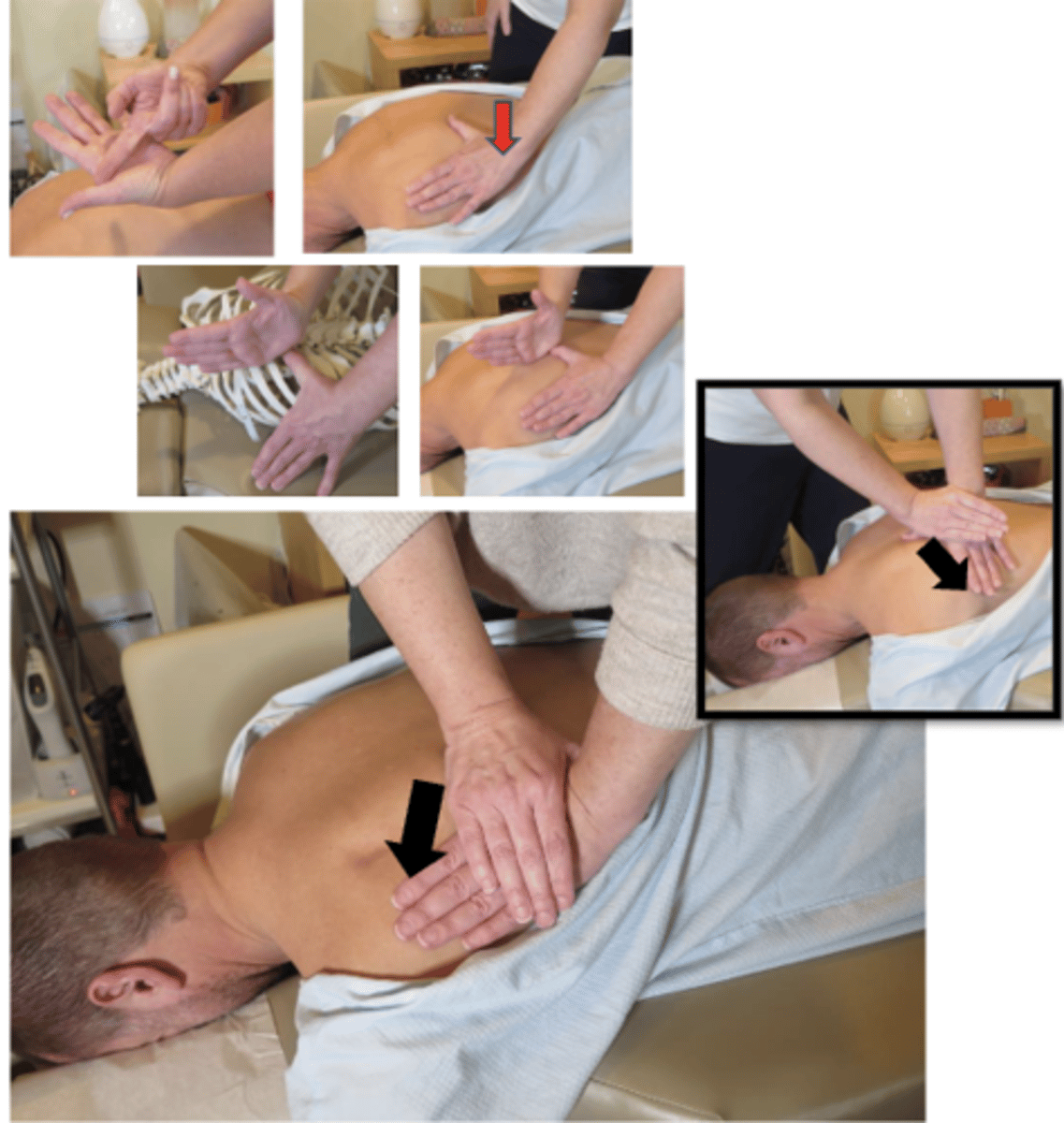
Listing:
• An open space palpates between the T2-T3 interspinous space
• T2 has an extension restriction
• The T2 spinous is deviated superior
Technique:Prone Bilateral Thenar/Transverse Push
• PP: Prone, headpiece in NEUTRAL to induce extension in the thoracocervical spine, permission to open gown/contact, identify segment
• DP: Standing at the head end of the table facing caudal, transferring additional body weight into contact
• CH: Bilateral thenar contacts running parallel to the spine , contacting bilateral transverse process of superior vertebrae
• IH: Same as above
• Vector: P-A and S-I
*Alternative contact: Hypothenar (pisiform)
*T1-T4

Listing:
• Left 5th rib angle palpates posterior and inferior on the left
• There is a loss of caliper motion at left rib 5
• Rib 5 is fixed P-A and I-S on the left
Technique:Prone Covered Thumb/Costal Push
• PP: Prone, permission to open gown/contact, identify finding segment
• DP: Stand on opposite side of contact, facing cephalad for I-S or caudal for S-I vector, tissue drawn from spine out to rib (M-L)
• CH: Caudal thumb-thenar contact follows the rib angle lateral to the transverse process
• IH: Cephalad pisiform-hypothenar contact reinforces over thumbnail with fingers wrapped around the wrist
• LOD: P-A and I-S
*OR P-A and S-I, depending on intended vector
*R3-R12
Listing:
• Right 9th rib angle palpates posterior on the right
• There is a loss of caliper motion at right rib 9
• Rib 9 is fixed P-A on the right
Technique:Prone Ilial Hypothenar/Costal Push
• PP: Prone, a small roll may be placed under the patient's upper abdomen to induce flexion, permission to open gown/contact, identify finding segment
• DP: Square stance or modified fencer stance, on opposite side of contact, transferring weight anterior and superior against contact, tissue drawn from spine out to rib (M-L)
• CH: Cephalad hypothenar contact follows the rib angle lateral to the transverse process
• IH: Caudal fingers grasp the anterior ilium (ASIS) on the side of contact, pelvis should not rotate off the table more than 1-2 inches off the table (this is NOT a thrust) preadjustive tension
• LOD: P-A , I-S
* R7-R12

Listing:
• Left 4th rib angle palpates posterior on the left
• There is a loss of caliper motion at left rib 4
• Rib 4 is fixed P-A on the left
Technique:Supine Opposite-Side Thenar/Costal Drop
• PP: Supine, permission to open gown/contact, identify finding segment, arms crossed hands grasping shoulders
• DP: Modify fencer stance, opposite side of contact, roll patient toward you, tissue drawn from spine out to rib (M-L)
• CH: Thenar eminence , contacting medial to the rib angle, reaching across patient
• IH: Patients crossed arms at elbows
• LOD: A-P
**For lower rib fixations the patient may be started in a seated position, a deep modified fencer stance on either side of the patient, maintaining thoracolumbar flexion keep contact hand more vertical to establish tension in the lower thoracic spine , indifferent hand cradling patient's neck
* R2-R12

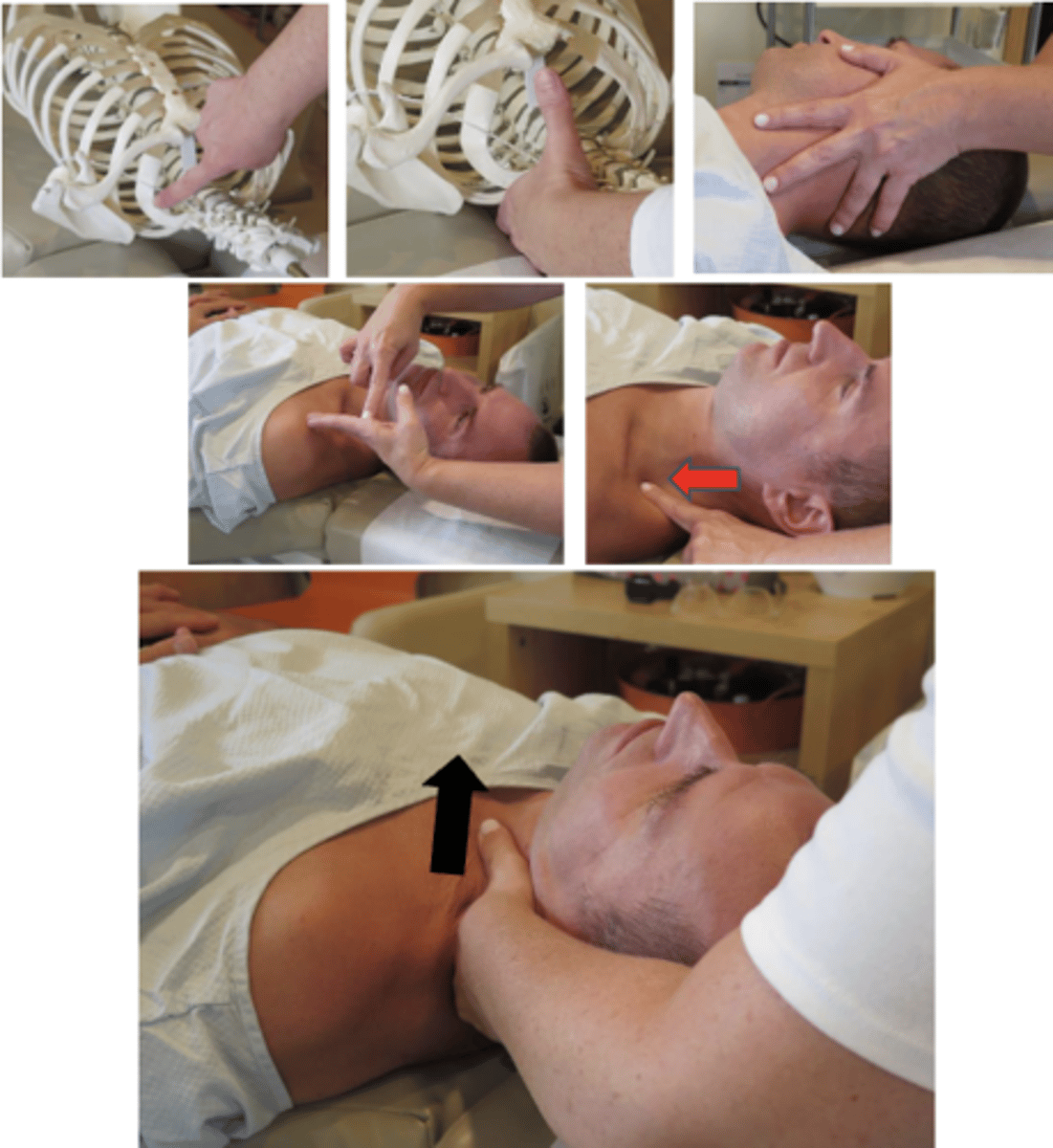
Listing:
• Left 1st rib angle palpates superior
• There is a loss of superior to inferior motion (caliper) at left rib 1
• Rib 1 is fixed S-I on the left
Technique:Supine Index/Costal Push
• PP: Supine, permission to open gown/contact, identify finding segment
• DP: Standing at head end of the table , facing caudal, standing off to the side of contact at 45° angle, tissue slack can be drawn down onto contact (S-I) or from behind contact (P-A)
• CH: Index from same side as contact, on angle of first rib
• IH: #1, laterally flexing patients had over contact, rotating head away from contact 20%, with lateral flexion over contact
• LOD: S-I and L-M* R1
Listing:
• Right rib 2 palpates anterior at the costosternal junction
• There is a loss of caliper motion at right rib 2
• Rib 2 is fixed A-P on the right
Technique:Supine Hypothenar/Costosternal Push
• PP: Supine, special consideration given to female patients due to contact areas involved, female patients should use a tissue barrier, permission to open gown/contact, identify finding segment
• DP: Standing side opposite of contact, tissue drawn from sternum out to rib (M-L)
• CH: Hypothenar/knife edge contact of cephalad hand on anterior rib lateral to costosternal junction
• IH: Caudal hand grasps posterior lateral thoracic cage distal to contact, pulling rib cage anterior
• LOD: A-P and M-L
**This is a shallow impulse focusing on the lateral vector to avoid compressing the rib cage
* R2-R6

Listing:
• A decreased intercostal space palpates between right ribs 8-9
• There is a loss of bucket handle motion at right rib 8
• Rib 8 is fixed I-S on the right
Technique:Side Lying Web/Costal Push
• PP: Side lying, dysfunctional side up , arm abducted overhead, permission to open gown/contact, identify finding segment, roll may be used under thorax to induce lateral flexion
• DP: Stand behind patient in a fencer stance, inferior to contact, preparing to develop pre-adjustive tension by leaning headword, tissue drawn from below contact up to rib (I-S)
• CH: Web contact of cephalad (outside) hand slides onto inferior margin of superior rib of dysfunction
• IH: Supports the contact hand, on dorsal surface, with fingers wrapped around the wrist
• LOD: I-S and L-M (Taking care to avoid excessive medial pressure to the rib cage)
* R3-R12
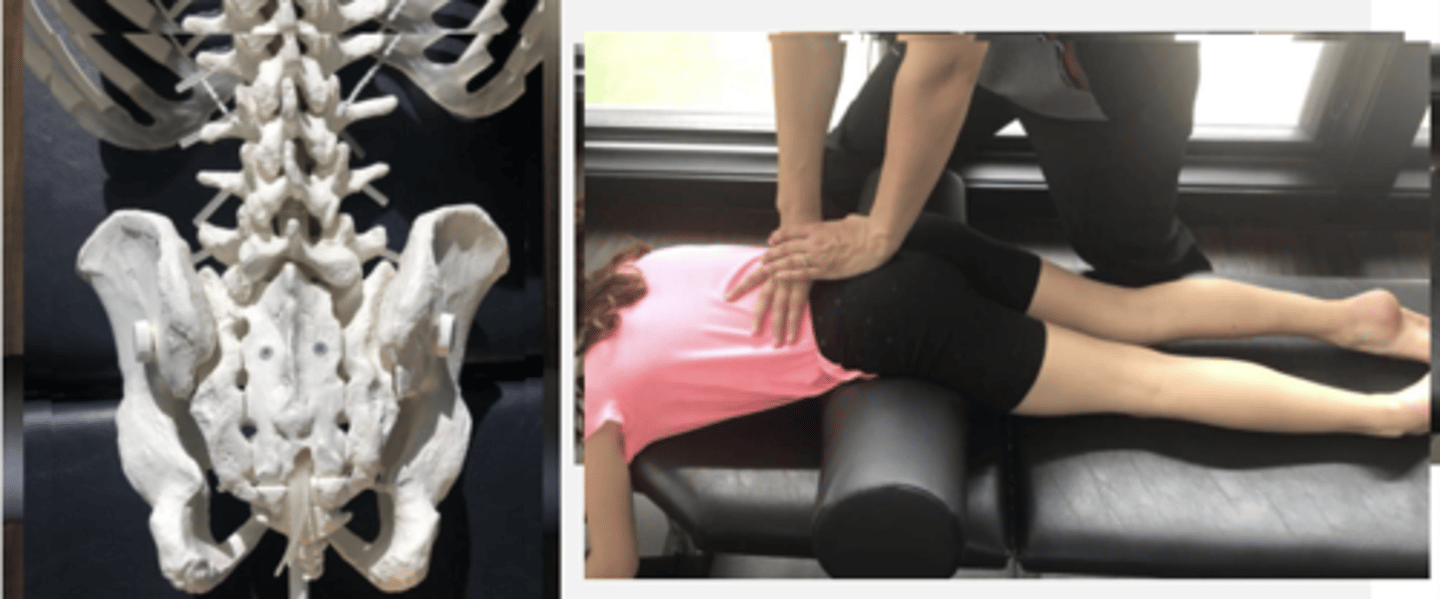
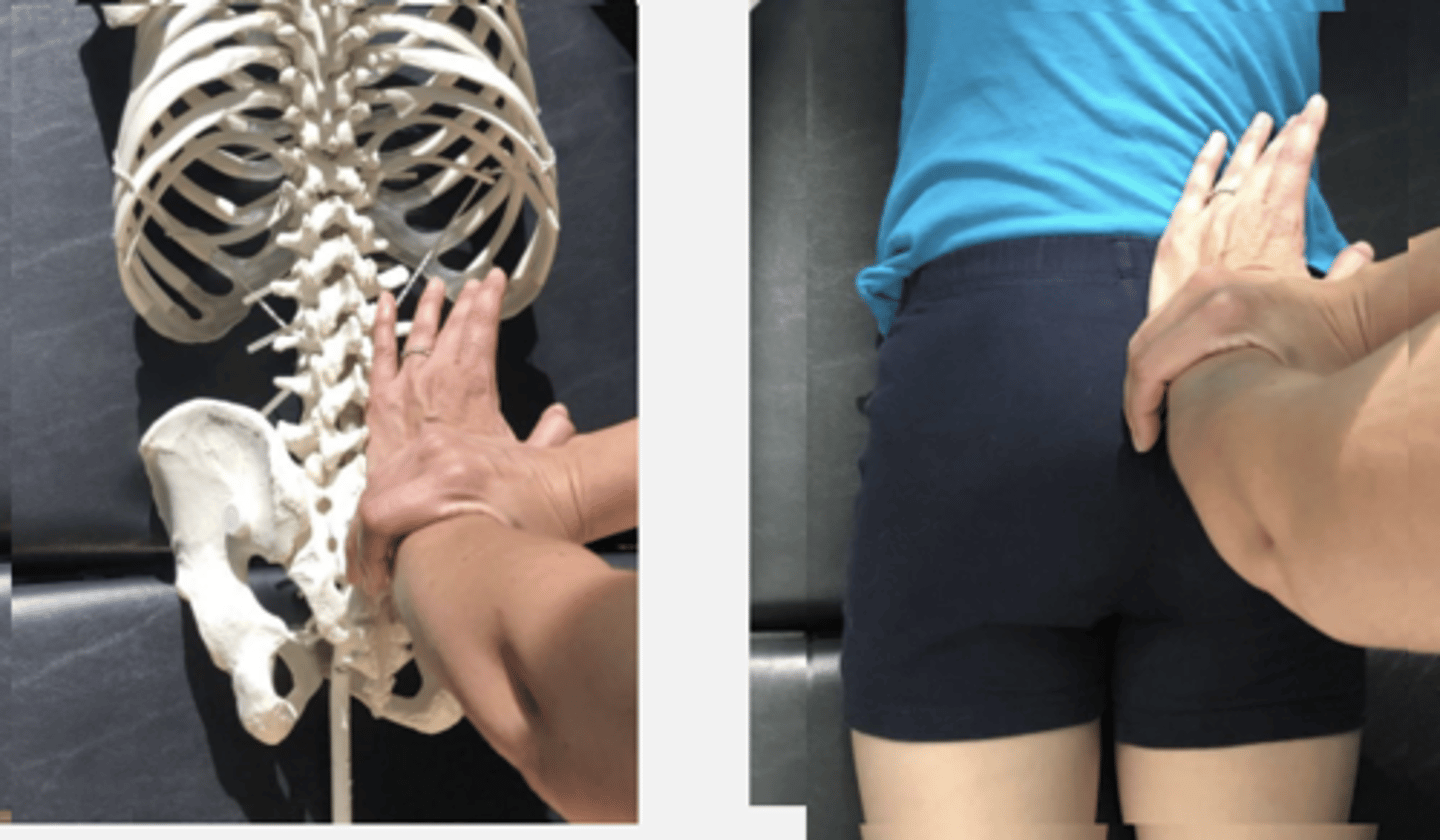
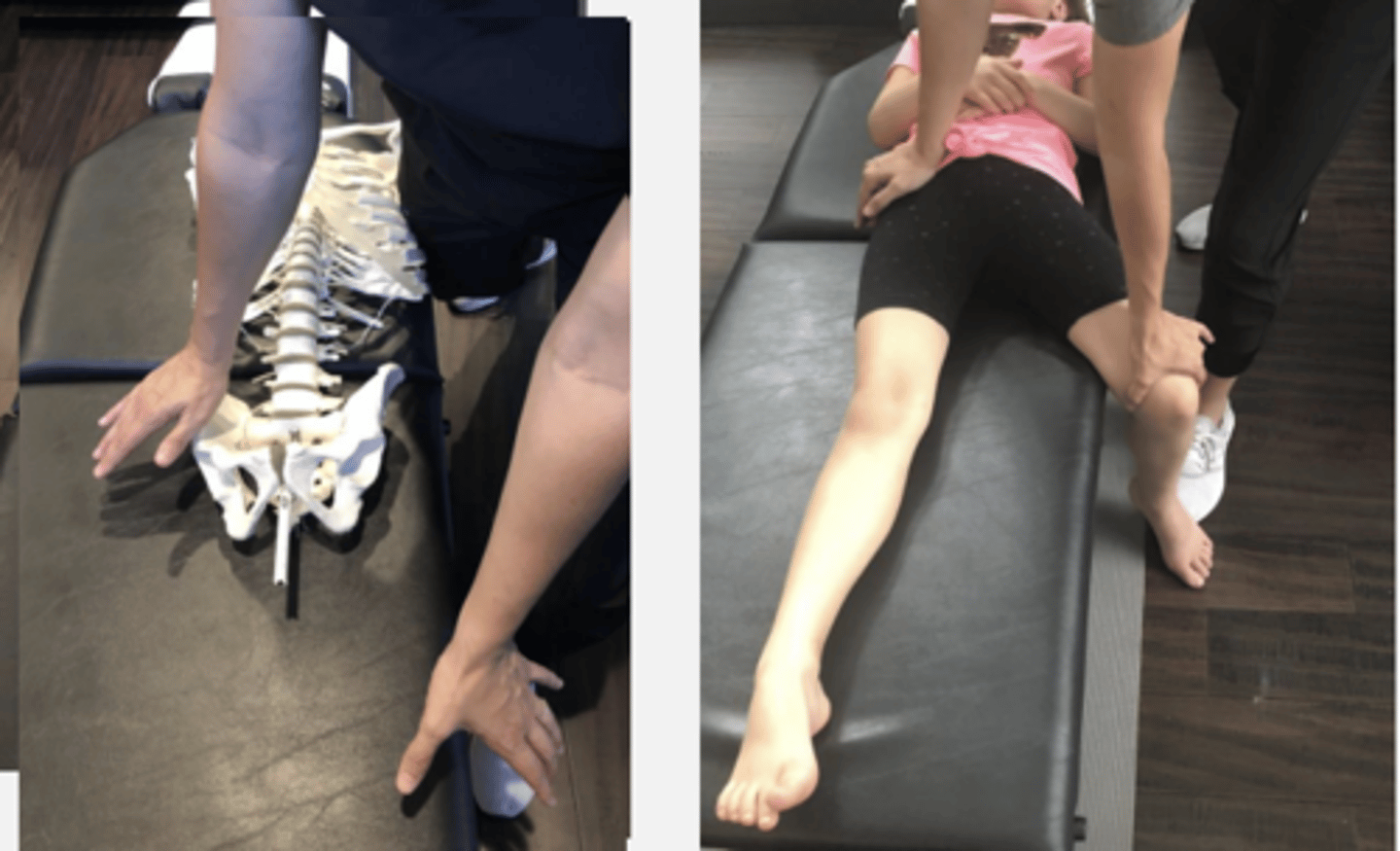
Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on R
-Loss of extension
-Sacral base - nutated, CN restriction
Technique:
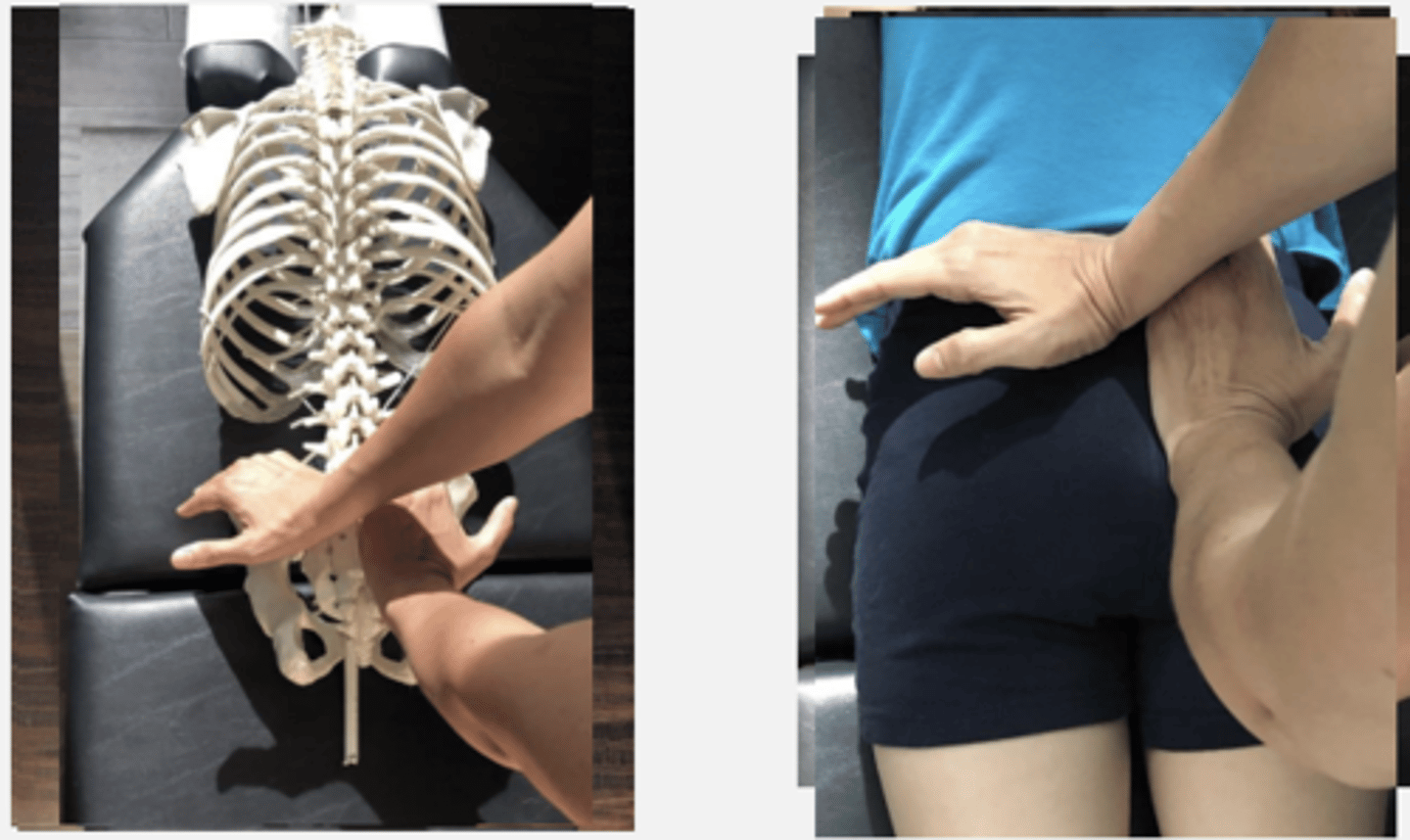
-Prone Bilateral Hypothenar Ilium Sacral Apex Push
PP: Prone-verbalize how you found the segment
DP: Square or Modified fencer stance on side opposite the dysfunction
CH: Cephalad (R) hand, hypothenar (pisiform) on L PSIS
IH: Caudal (L) hand knife-edge on side of sacral apex closest to you
LOD: CH: P-A, M-L, slight I-S
IH: P-A, slight S-I
Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on L
-Loss of extension
Technique:
-Prone Unilateral Reinforced Pisiform Ilium Push
PP: Prone- verbalize how you found the segment
DP: Square or Modified fencer stance on side opposite the dysfunction
CH: Cephalad ( R) hand, hypothenar (pisiform) on L PSIS
IH: Reinforcing CH
LOD: P-A, M-L

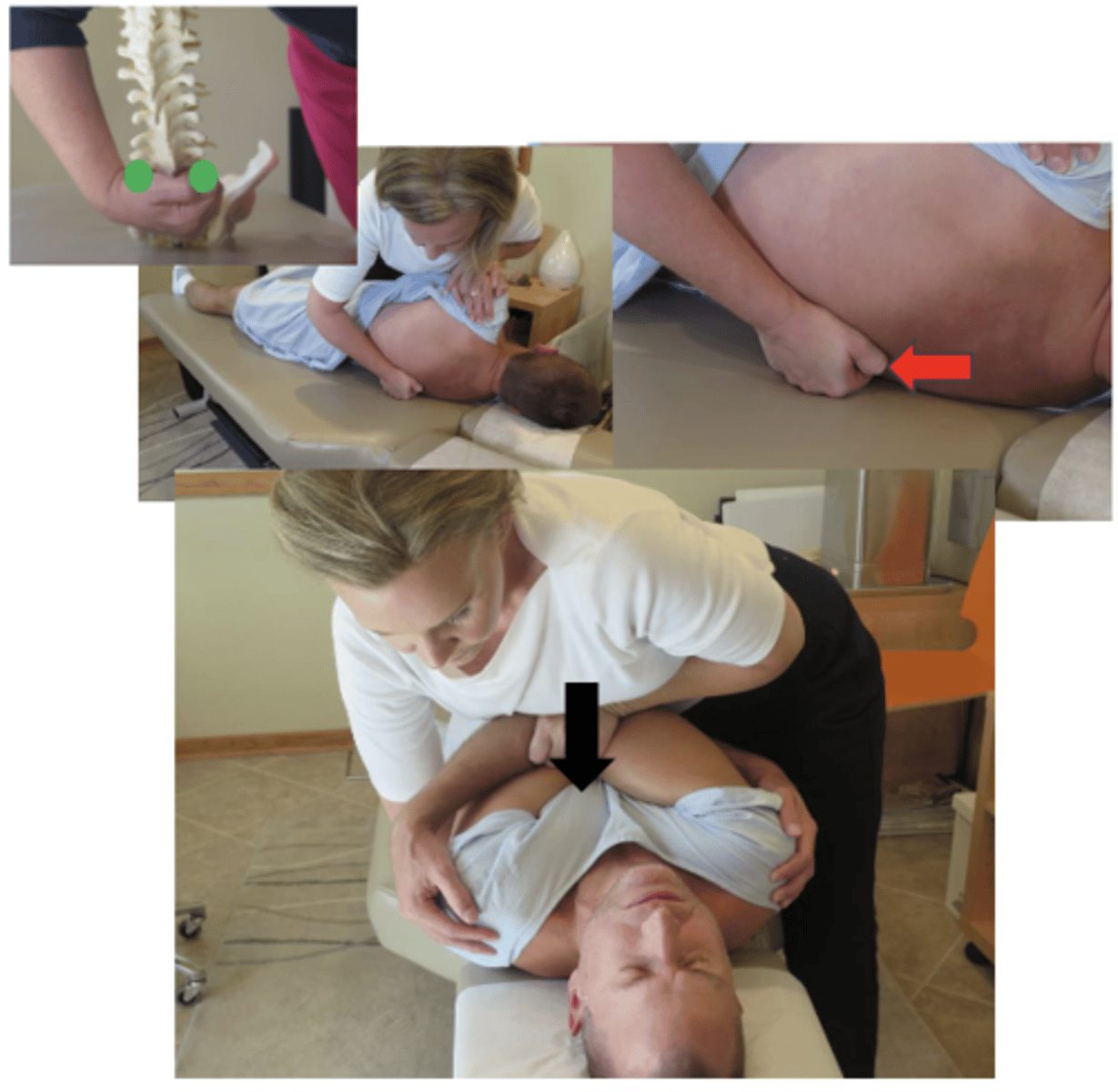
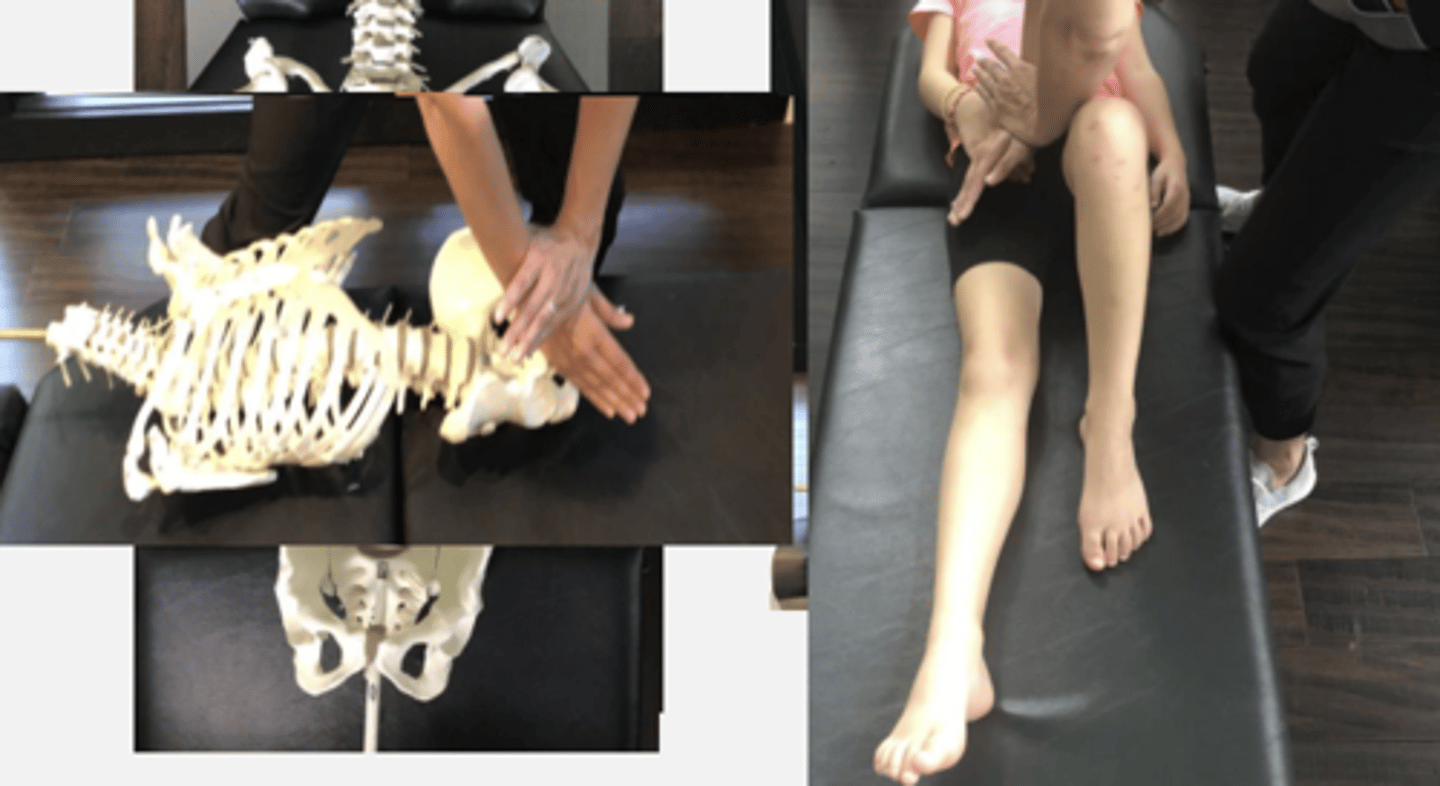
Static & Motion Findings:
-PSIS palpates anterior, superior, and lateral on R
-Loss of flexion
-R sacral base - CN, NR
Technique:
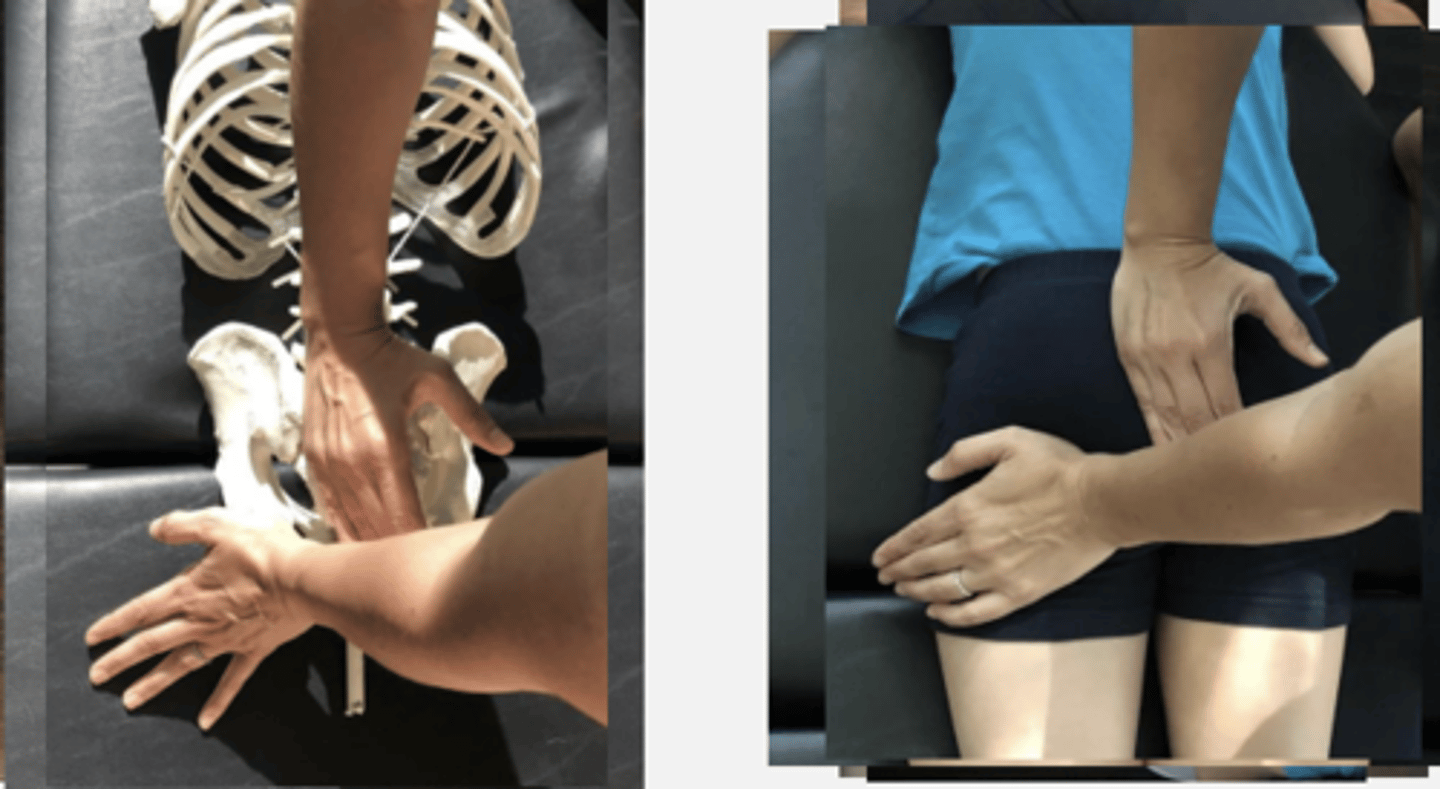
-Prone Bilateral Hypothenar Ischium Sacral Base Push
PP: Prone- verbalize how you found the segment
DP: Square or Modified fencer stance on side opposite the dysfunction
CH: Caudal (L) hand, hypothenar (calcaneal) contact on (L) ischial tuberosity
IH: Cephalad ( R) hand, hypothenar(pisiform) on L sacral base(just medial to the L PSIS)
LOD: CH: P - A, S -I
IH: P -A, I - S
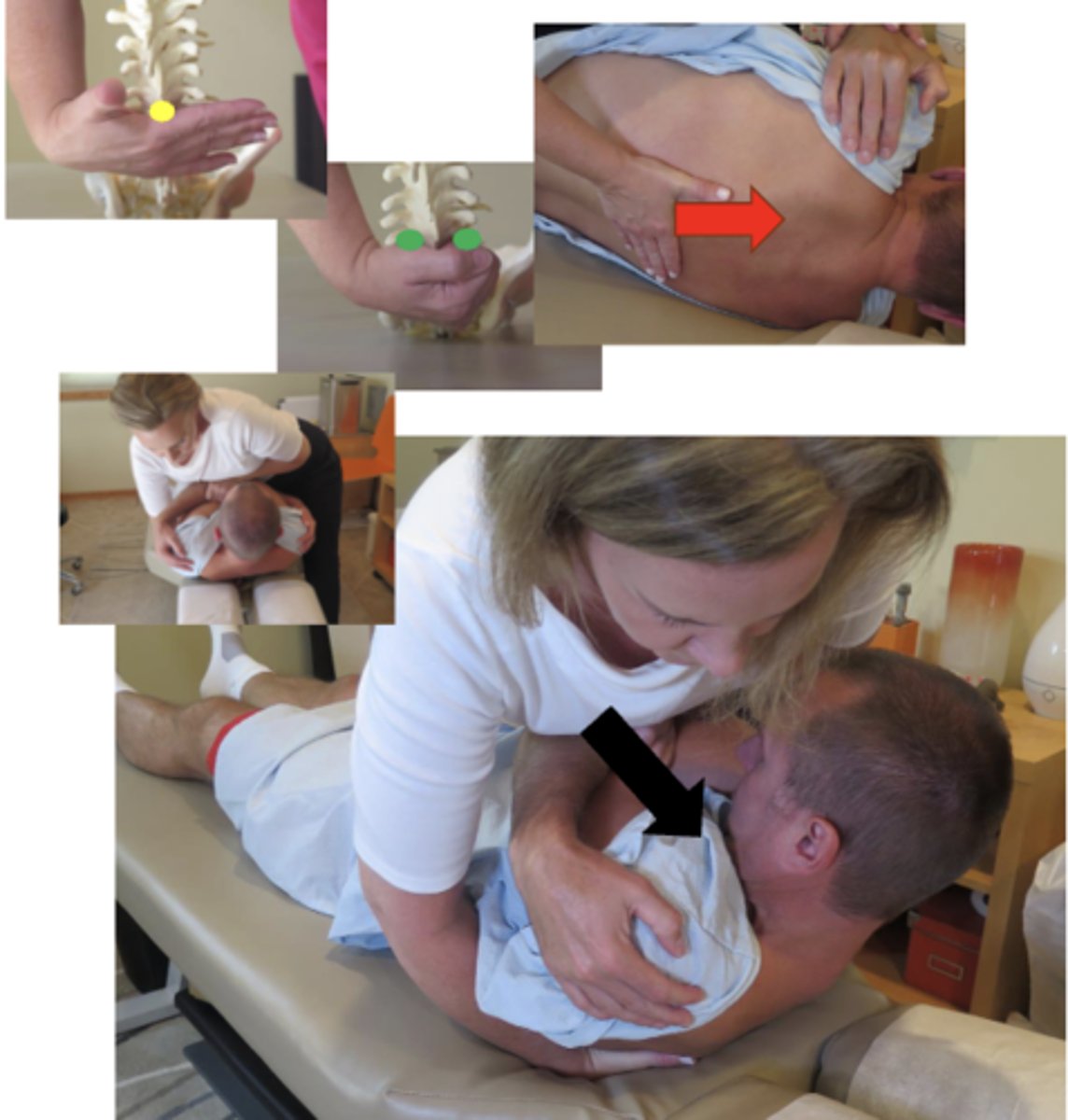
Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on R
-Loss of extension
-Sacral base - nutated, CN restriction
Technique:
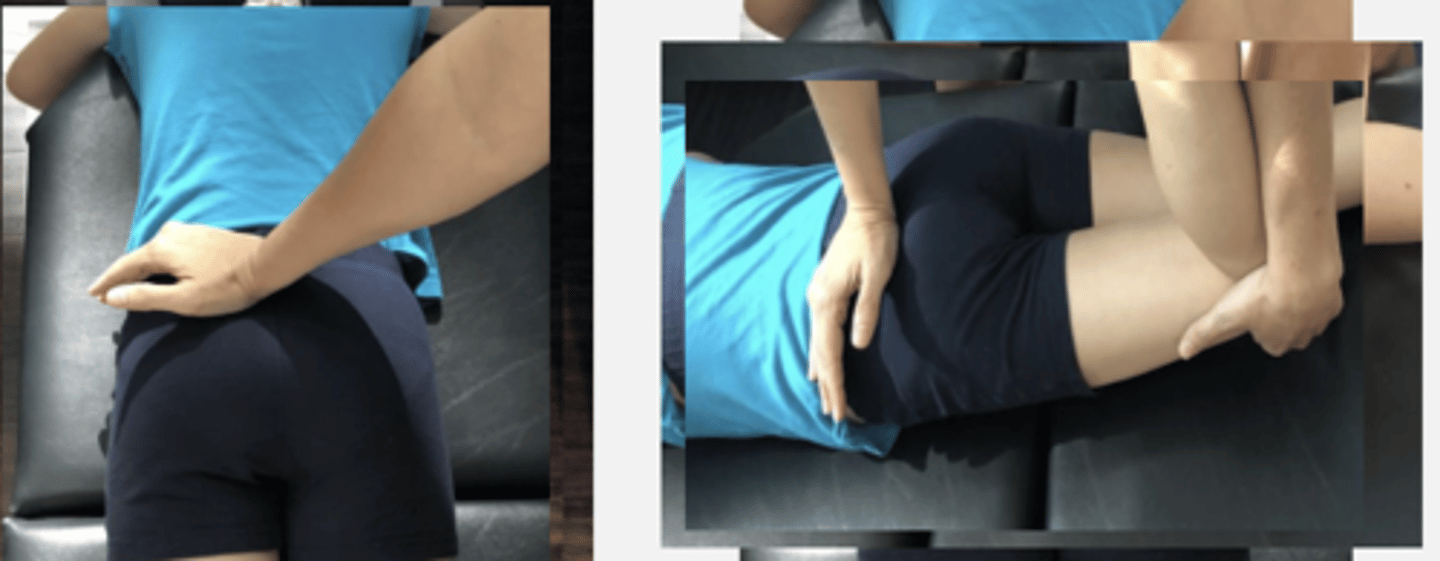
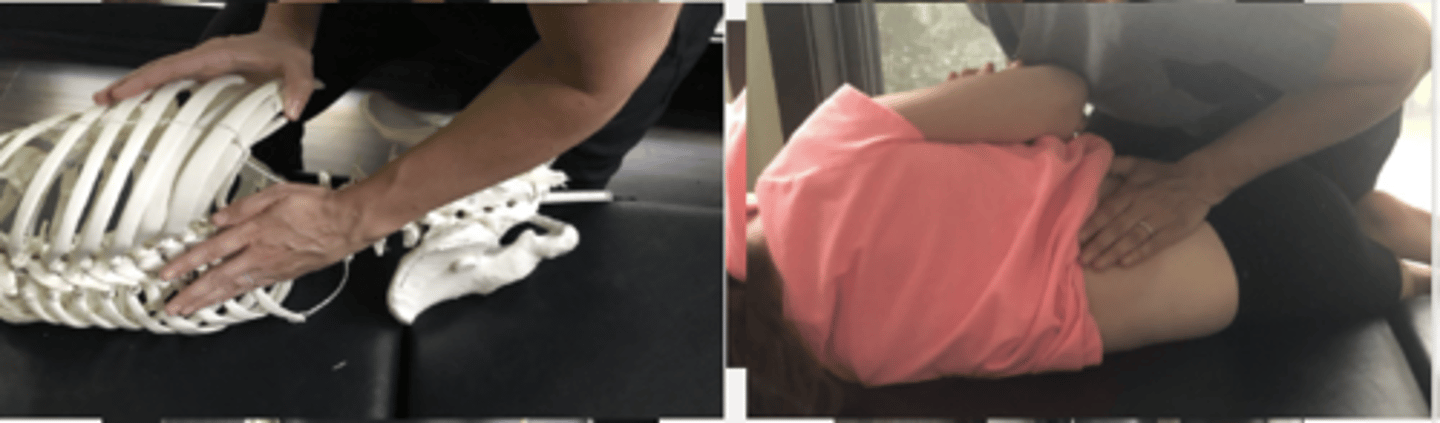
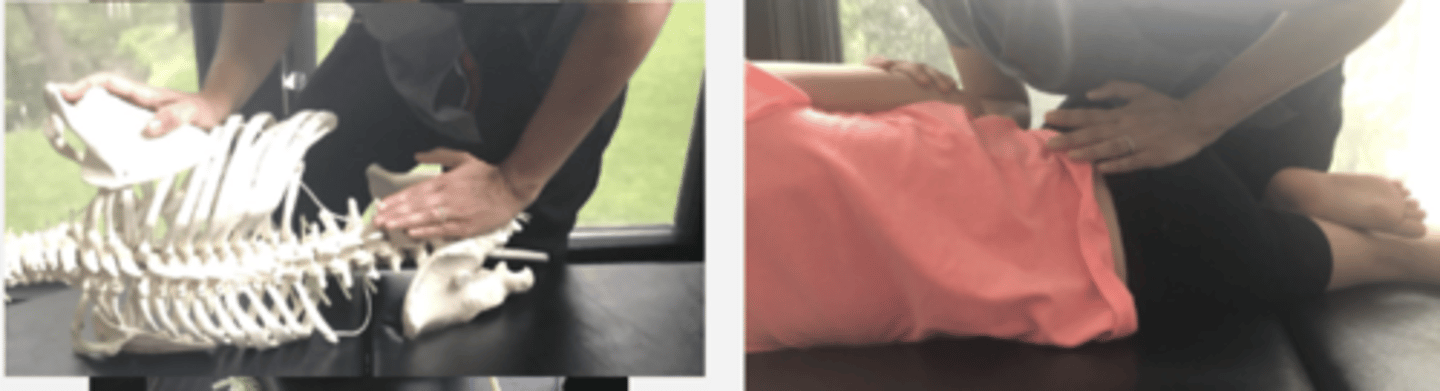
-Prone Hypothenar Ilium Push with Hip Extension
PP: Prone- verbalize how you found the segment
DP: Square or Modified fencer stance on side opposite the dysfunction
CH: Cephalad ( R) hand, hypothenar (pisiform) on L PSIS
IH: Caudal (L) hand grasps pt's distal thigh on same side as the adjustive contact (L distal thigh)
LOD: CH: P - A, M - L
IH: Reinforcing with shallow lift of the thigh contact
Static & Motion Findings:
-L sacral base palpates posterior & superior
-Loss of nutation
Technique:
-Prone Unilateral Reinforced Pisiform Sacral Base Push
PP: Prone- verbalize how you found the segment
DP: Modified fencer stance on same side of dysfunction
CH: Caudal (L) hand, hypothenar (pisiform) on superior margin of sacral base just medial to PSIS
IH: Reinforcing CH
LOD: P-A, I-S
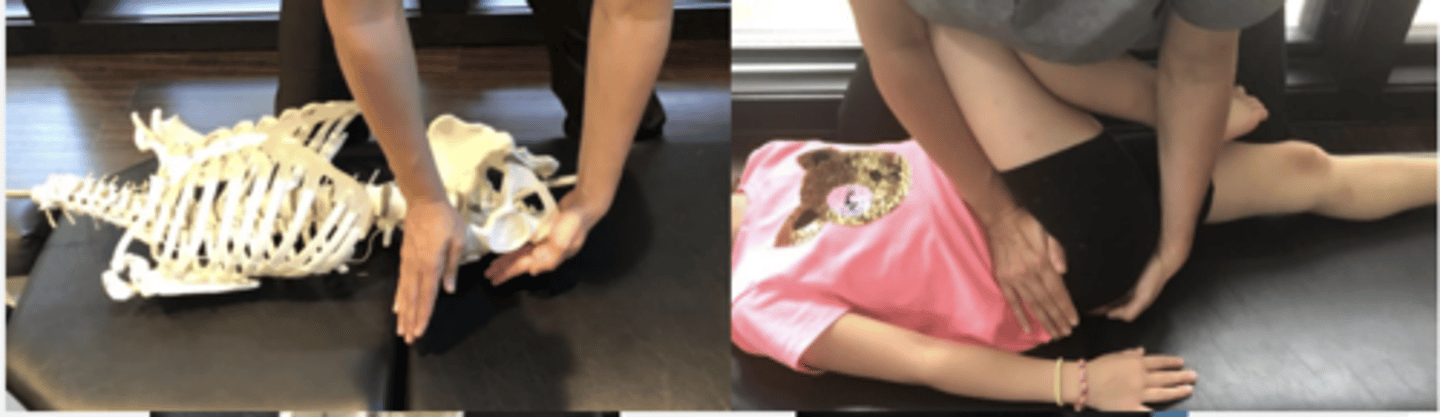
Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on L
-Loss of extension
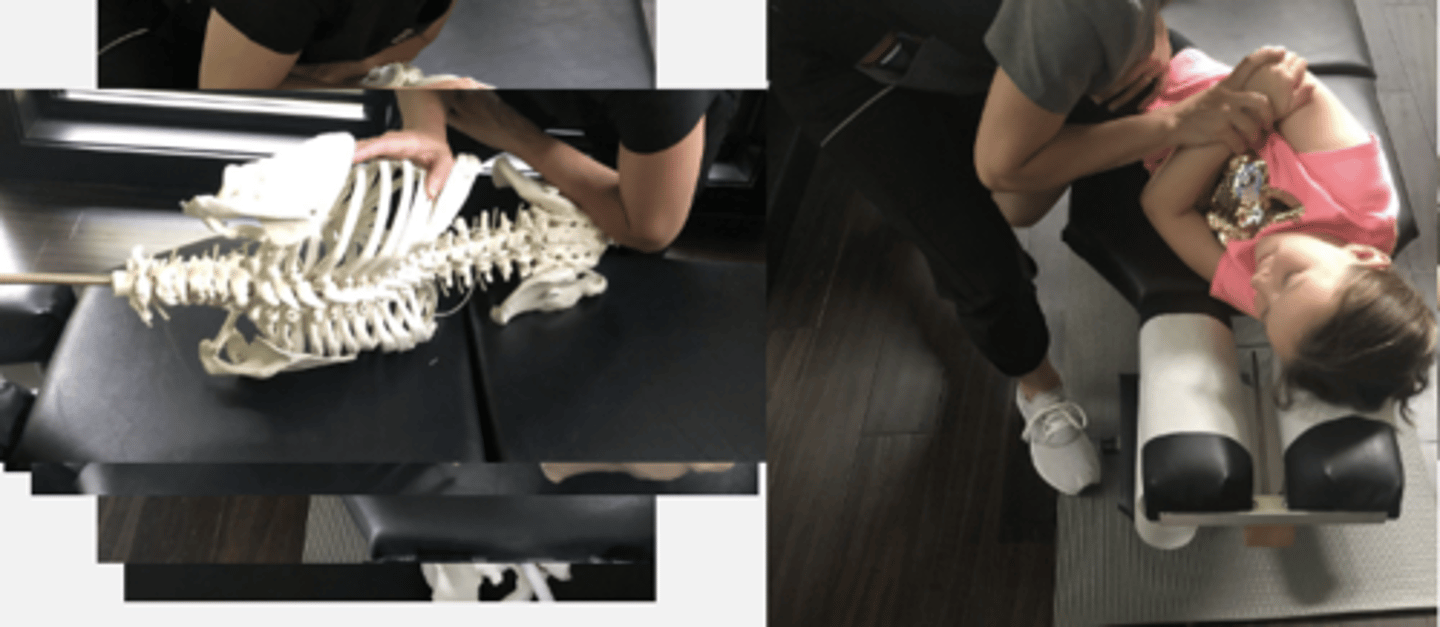
Technique:
-Side Posture Hypothenar Ilium Push
PP: Basic side posture position with the dysfunctional side up - verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction
CH: Caudal (L) hand,hypothenar (pisiform) on RPSIS
IH: Cephalic ( R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: CH: P-A, M-L, I-S

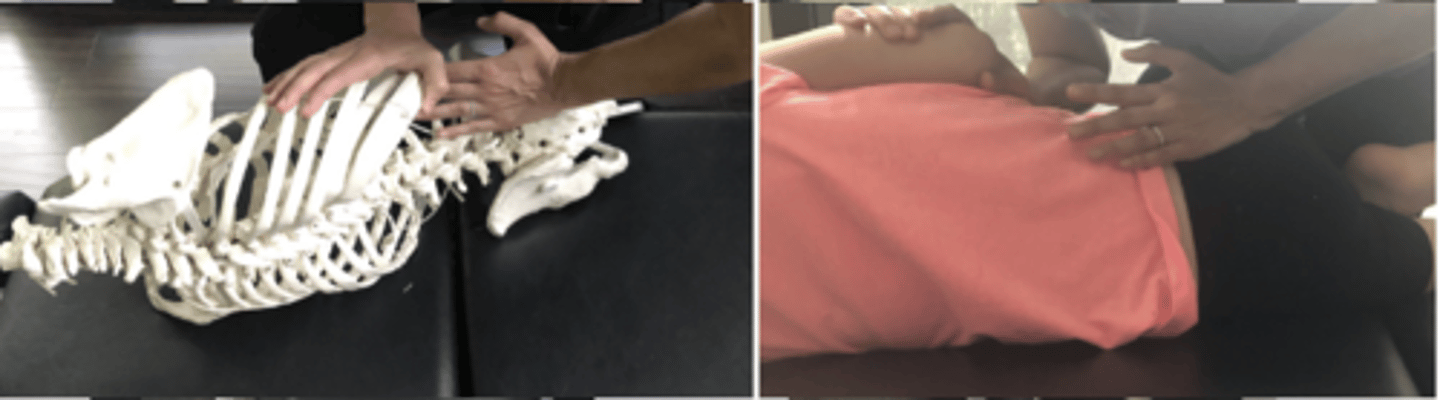
Static & Motion Findings:
-PSIS palpates anterior, superior, and lateral on R
-Loss of flexion
Technique:
-Side Posture Hypothenar Ischium Push
PP: Basic side posture position with the dysfunctional side up - verbalize how you found the segment
DP: Modified fencer stance onside of dysfunction
CH: Caudal (L) hand, soft broad hypothenar contact R ischium
IH: Cephalic ( R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: CH: P-A, along shaft offemur to induce SIJ flexion

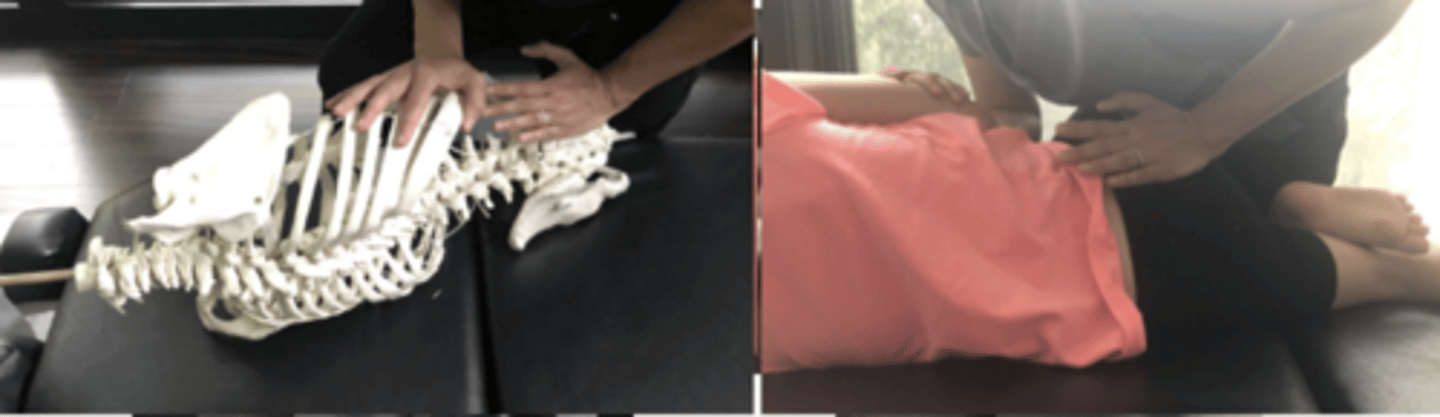
Static & Motion Findings:
-PSIS palpates anterior, superior, and lateral on R
-Loss of flexion
Technique:
-Side Posture Forearm Ischium Push
PP: Basic side posture position with the dysfunctional side up - verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction -naturally becomes more of a chest drop
CH: Caudal (L) forearm, soft broad contact pull inferior and lateral over the medial, inferior margin of
IH: Cephalic ( R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: CH: Thrust P-A, along shaft of femur to induce SIJ flexion
Static & Motion Findings:
-PSIS palpates anterior, superior and lateral on R
-Loss of flexion
-Sacral base palpates posterior & superior on R
-Nutation Restriction
Technique:
-Side Posture Hypothenar (Pisiform) Sacral Base Push, Dysfunctional Side Up
PP: Basic side posture position with the dysfunctional side up-verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction
CH: Caudal (L) hand, hypothenar (pisiform) on R sacral base (just medial to R PSIS)
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, slight I-S
Static & Motion Findings:
-PSIS palpates anterior, superior and lateral R
-Loss of flexion
-Right sacral base palpates posterior & superior
-Nutation restriction
Technique:
-Side Posture Hypothenar (Pisiform) Sacral Base Push, Dysfunctional Side Down
PP: Basic side posture position with the dysfunctional side down-verbalize how you found the segment
DP: Modified fencer stance on side opposite dysfunction
CH: Caudal (L) hand, hypothenar (pisiform) on L sacral base down side (just medial to L PSIS)
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A

Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on L
-Loss of extension & counternutation
Technique:
-Side Posture Hypothenar (Pisiform) Sacral Apex Push, Dysfunctional Side Down
PP: Basic side posture position with the dysfunctional side down-verbalize how you found the segment
DP: Modified fencer stance on side opposite dysfunction
CH: Caudal (L) hand, hypothenar (pisiform) on up-side of the sacral apex (R lateral side of sacral apex)
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A
Static & Motion Findings:
-PSIS palpates posterior, medial, and inferior on R
-Loss of extension & counternutation
Technique:
-Side Posture Forearm Sacral Apex Push, Dysfunctional Side Down
PP: Basic side posture position with the dysfunctional side down-verbalize how you found the segment
DP: Modified fencer stance on side opposite dysfunction
CH: Caudal (L) hand, forearm on up-side of the sacral apex (R lateral side of sacral apex)
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A

Static & Motion Findings:
-L4 SP palpates posterior & inferior on the L
-Loss of left rotation & right lateral flexion
Technique:
Prone Hypothenar Mammillary Push
PP: Prone-verbalize how you found the segment
DP: Square stance on side of contact
CH: Cephalad (R) hand, hypothenar (pisiform) on L4 MP with fingers running parallel to the spine
IH: Reinforces in anatomical snuffbox
LOD: For rot with LF: P-A, S-I
just rotation: P-A
Static & Motion Findings:
-L3 MP palpated posterior & inferior on the L
-Loss of right rotation & right lateral flexion
Technique:
Prone Hypothenar Spinous Push
PP: Prone-verbalize how you found the segment
DP: Square stance on side of contact
CH: Cephalad (R) hand, hypthenar (pisiform) on L3 SP with fingers crossing the spine
IH: Reinforces in anatomical snuffbox
LOD: P-A, L-M, S-I
Static & Motion Findings:
-L3 MP palpates posterior on the R
-Loss of left rotation
Technique:
Side Posture Hypothenar Mammillary Push
PP: Basic side posture position with the dysfunctional side up-verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction
CH: Caudal (L) hand, hypothenar contacts dys segment MP (L3 MP) with fingers parallel to spine
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, slight I-S

Static & Motion Findings:
-L3 MP palpates inferior on the R
-Loss of left lateral flexion
Technique:
Side Posture Hypothenar Mammillary Push, closed-wedge side
PP: Basic side posture position with the dysfunctional side up-verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction
CH: Caudal (L) hand hypothenar on L3 MP with fingers runing parallel to spine
IH: Cephalic (R) hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, I-S
(Place roll under patient to assist the LF motion)

Static & Motion Findings:
-L3 MP palpates inferior on L3
-Loss of right lateral flexion
Technique:
Side Posture Hypothenar Mammillary Push, open-wedge side
PP: Basic side posture position with open wedge side up-verbalize how you found the segment
DP: Modified fencer stance on side of dysfunction
CH: Caudal (L) hand hypothenar on L3 MP with fingers runing parallel to spine
IH: Cephalic (R) hand slight downward traction holding the pt's up-side shoulder to assist in production of LF
LOD: P-A, L-M, S-I
(Lower the thoracolumbar section or place pt's down arm cephalad to induce LF)

Static & Motion Findings:
-L3/L4 interspinous space is decreased
-Loss of flexion
Technique:
Side Posture Hypothenar Spinous Push
PP: Basic side posture position with either side up-verbalize how you found the segment
DP: Modified fencer stance
CH: Caudal hand hypo/calcaneous slides onto superior segment (L3) spinous with fingers angled across the spine
IH: Cephalic hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, I-S
(Opening interspinous space)

Static & Motion Findings:
-L3/L4 interspinous space is increased
-Loss of extension
Technique:
Side Posture Hypothenar Spinous Push
PP: Basic side posture position with either side up-verbalize how you found the segment
DP: Modified fencer stance
CH: Caudal hand hypo/calcaneous slides onto inferior segment (L4) spinous with fingers angled across the spine
IH: Cephalic hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, I-S
(Closing the interspinous space)
Static & Motion Findings:
-L5/S1 interspinous space is decreased
-Loss of flexion
Technique:
Side Posture Hypothenar Sacral Apex Push
PP: Basic side posture position with either side up-verbalize how you found the segment
DP: Modified fencer stance
CH: Caudal hand hypo/calcaneous slides inferiorly to contact sacral apex
IH: Cephalic hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: P-A, S-I
Static & Motion Findings:
-L3 MP palpates posterior on L
-Loss of right rotation
(Can be used with lateral flexion too)
Technique:
Side Posture Hypothenar Spinous Push
PP: Basic side posture with the dysfunctional side down (since spinous has deviated to R) - verbalize how you found the segment
DP: Modified fencer stance on side opposite dysfunction
CH: Caudal (L) hand hypothenar on L3 SP with fingers crossing the spine
IH: Cephalic (R) hand slight upward (downward for lateral flexion) traction holding the pt's up-side shoulder or overlapping hand
LOD: CH: P-A, L-M

Static & Motion Findings:
-L3 MP palpates posterior on R
-Loss of left rotation
Technique:
Side Posture Digital Spinous Kick Pull
PP: Basic side posture position with the dysfunctional side up (since spinous has deviated to L) - verbalize how you found the segment
DP: Square stance on side of dysfunction & contact their knee with you knee/distal tibia
CH: Fingertips (digital contacts) of 2nd, 3rd, 4th digits of caudal (L) hand hooks the down side of the L3 SP
IH: Cephalic hand slight upward traction holding the pt's up-side shoulder or overlapping hand
LOD: L-M pulling movement to induce axial rotation with quick extension (kick) of contact leg

Static & Motion Findings:
-L3 MP palpates posterior on L
-L4 MP palpates posterior on R
-Loss of right rotation
-Loss of left rotation
Technique:
Side Posture Bilateral Digital Spinous Push, Pull
PP: Basic side posture position with the superior dysfunctional side down (since spinous has deviated to R) - verbalize how you found the segment
DP: Square stance on side of dysfunction & contact their knee with your knee/distal tibia
CH: Fingertips (digital contacts) of 3rd & 4th digits of cephalic (R) hand reach under the pt's up-side arm to contact lateral surface of L3
IH: Fingertips of caudal (L) hand hook the downside of the L4 SP
LOD: Cephalic hand-pushes L-M
Caudal - pulls L-M with quick extension of contact leg

Static & Motion Findings:
-L pubis palpates more superior than R
-L pubis loss of inferior glide
Technique:
Hypothenar/Thigh
PP: Supine off center of table to side of involvement & corresponding leg hangs off table
DP: Modified fencer stance on involved side facing caudal
CH: Palmar contact of caudal (L) hand to distal femur of leg on involved side
IH: Cephalad (R) hand palmar contact over the opposite ASIS to stabilize the pelvis
LOD: CH applies A-P stress on pt's thigh. Ask pt to raise thigh against resistance & after 4-5 seconds deliver a slight & shallow impulse thrust S-I down the thigh
Static & Motion Findings:
-R pubis palpates more anterior than L
-R pubis loss of posterior glide
Technique:
Hypothenar/Pubis
PP: Supine-uninvolved knee & hip flexed with foot flat on table
DP: Modified fencer/square stance on uninvolved side facing caudal
CH: Hypothenar contact of cephalad (R) hand on anterior aspect of the involved pubis (barrier over pubis)
IH: Caudal (L) hand reinforces CH or establishes a palmar contact over the involved distal thigh
LOD: A-P
Static & Motion Findings:
-R pubis palpates more inferior than L
-R pubis loss of superior glide
Technique:
Hypothenar/Ilium, Palmar/Ischium
PP: Supine-involved knee & hip flexed with foot flat on table
DP: Square stance on uninvolved side leaning over pt with your upper body contacting the anterior aspect of pt's tibia
CH: Caudal (L) hand palmar contact of ischium
IH: Cephalic (R) hand reaches over and to place hypothenar on ASIS of the involved side
LOD: CH: P-A, I-S
IH: A-P
Static & Motion Findings:
-Diffuse pain with palpation
-Diffuse pain with provocation
Technique:
Pubic Distraction
PP: Supine-flex both knees & hips with feet flat on table pt's shoulder width apart
DP: Standing at foot of table facing the patient
CH: Palmar contacts of both hands to medial aspects of knees
IH: Palmar contacts of both hands to medial aspects of knees
LOD: Instruct pt to squeeze knees together until adductor mm fatigue occurs. Then deliver a shallow M-L impulse thurst to both knees
Static & Motion Findings:
-Coccyx palpates anteriorly
-Loss of posterior glide
Technique:
Thumb/External Coccyx Push
PP: Prone-with Dutchman roll placed under ASIS. Verbalize how you found the segment
DP: Modified fencer stance facing cephalad
CH: Cephalad thumb contact to base of coccyx
IH: Caudal pisiform/hypothenar contact reinforced over contact thumbnail
LOD: I-S, slight P-A