Menarche
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Adrenarche
The awakening of the adrenal gland
Begins around age 8
Increase in adrenal androgen production (male sex hormones)
DHEAS/androstenedione
Increased body odor, oiliness in the skin, appearance of pubic and axillary hair
Gonadarche
Gonads begin to mature and produce sex hormones
Begins around age 8
Hypothalamus produces GnRH → signals pituitary gland to release LH and FSH → LH and FSH stimulate gonads to grow and produce sex hormones
Thelarche
Development of breast buds
Pubarche
Onset of growth of pubic hair
Axillary hair
Growth Spurt
Acceleration in growth rate due to GnRH and insulin-like growth factor 1 (somatomedin C)
Menarche General
First menstrual period
Occurs between ages 9 and 15: usually 2 years after thelarche
Average age is 12-12.5
Average height is 4’11” - 5’2”
Average weight is 99-110 lbs
Critical body weight is important
Body’s fat content must account for 17% of the body’s weight before menarche can occur
At age 18, the fat content must be at least 22% for the maintenance of regular menstrual cycles
Chronological Order of Female Pubertal Events
Adrenarche (8 y/o)
Gonadarche (8 y/o)
Thelarche-Breast bud (9-10 y/o)
Pubarche-onset pubic hair (11-12 y/o)
Maximal growth spurt (11-12 y/o)
Menarche (11.5-12.8 y/o)
Adult pubic hair-13.7 y/o
Adult breast-14.6 y/o
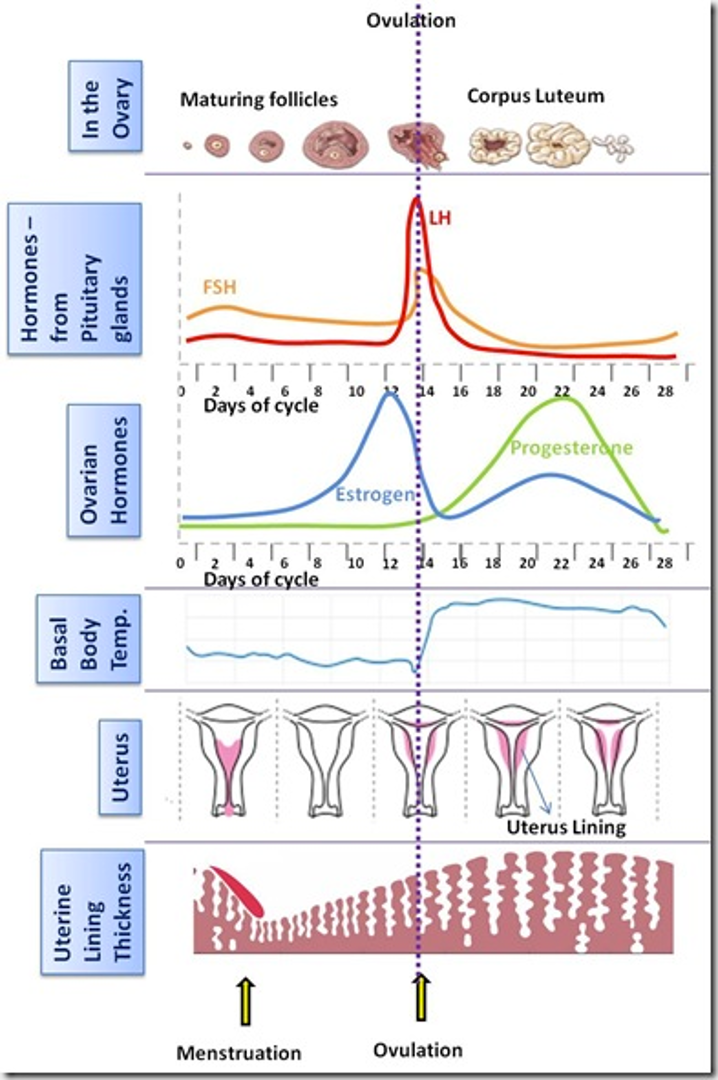
Hormones
Estrogen, progesterone, LH, FSH
See a marked increase in menarche
Other factors
Fat:lean ratio
Nutrition
Underlying disease
Higher fat levels associated with increased estrogen production (fat cells contain aromatase, an enzyme that converts androgens into estrogens)
Increase fat → increases aromatization androgens → estrogen → (+) feedback to hypothalamus/pituitary → LH surge (needed for ovulation)
Clinical Effects of Hormones on Menarche (6)
Increased vaginal secretions
Reduced vaginal pH
Vaginal mucosa thickens and becomes rugated, cornification
Labia protrudes, thickens, rugated
Uterus increases in size and length
Mean weight of ovaries increases
Menstrual Cycle General
Onset 9-14 y/o
Typically occurs at Tanner stage IV breast development
Rare before Tanner III development
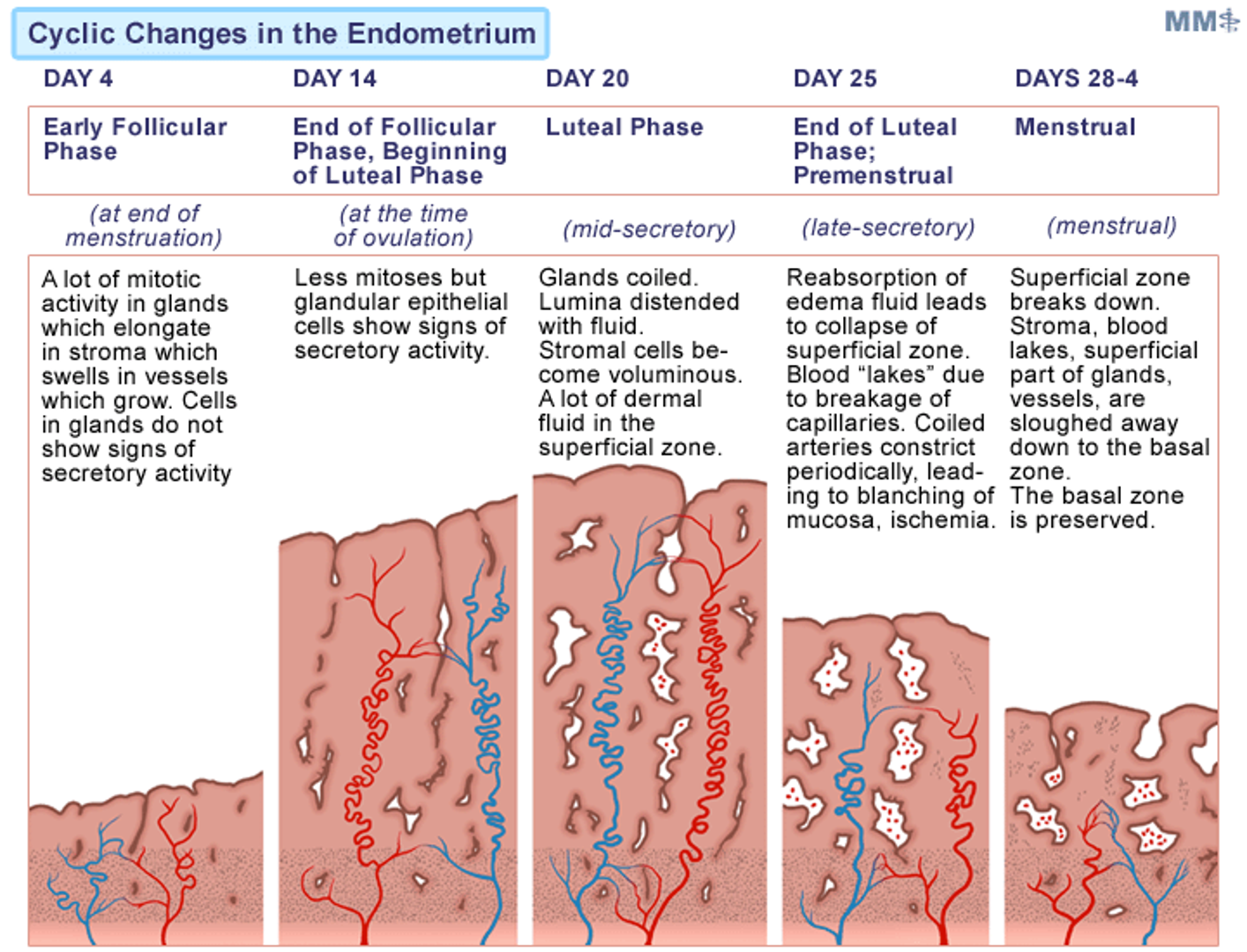
Normal Menstruation
Duration: 3-5 days
Menstrual blood mostly arterial (spiral arteries) (25% venous)
Contains tissue debris, prostaglandins, large amounts of fibrinolysin from endometrial tissue
Fibrinolysin lyses clots in menstrual blood to dissolve clots and maintain normal blood flow
Average blood loss: 30 mL
Early Cycles and Transition to Regular Ovulation
Tend to be irregular at onset and perimenopause
At least 50% of menstrual cycles anovulatory in the first year but in fairly regular intervals
Having irregular cycles → most likely anovulatory
During first 2 years after menarche → cycles somewhat irregular but 90% will have cycles within range of 21-42 days with 2-8 days of flow
By the 7th year of menarche → 90% cycles ovulatory
Once ovulatory, may experience dysmenorrhea
Oligomenorrhea Definition
Infrequent menstruation: > 35 days
Polymenorrhea Definition
Frequent menstruation: < 21 days
Dysmenorrhea Definition
Painful menstruation
Menorrhalgia Definition
Dysmenorrhea, painful menses
Menorrhagia Definition
Excess/prolonged uterine bleed but at regular intervals
Metorrhagia Definition
Irregular bleeding
Uterine bleeding at times other than expected menses
Menometorrhagia Definition
Excessive uterine bleeding both during menses and at irregular intervals
Uterine and Ovarian Cycle
Shed off menses → start building lining back up
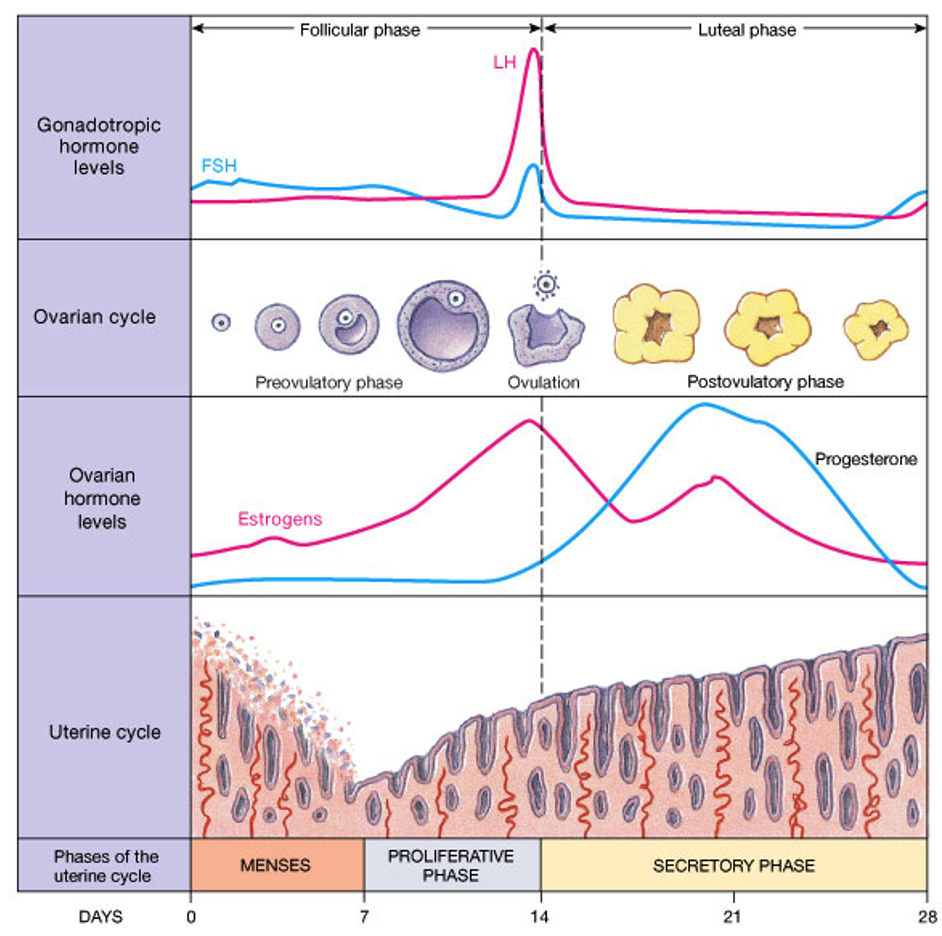
Follicular (Proliferative) Phase
First day of menses until ovulation
Variable in length
Characteristics
Low basal body temperature
Development of ovarian follicles
Vascular growth of endometrium
Secretion of estrogen from ovary
Uterine cramps from prostaglandins
Luteal (Secretory) Phase
Ovulation until onset of menses
Under influence of progesterone: want progesterone to be the highest in the middle of the luteal phase to ensure that it is aiding in the development of pregnancy
Constant in duration (12-16 days: mean 14 days)
Characteristics
Elevated basal body temperature
Corpus luteum forms
Endometrial changes
Decreased sexual desire and sexual enjoyment
GnRH
Hypothalamic hormone that controls gonadotropins
Stimulates synthesis and release FSH and LH
Continuous exposure of GnRH inhibits FSH and LH
Secreted in pulsatile manner: amplitude/frequency variable
Regulated by estrogen/progesterone feedback
Estrogen Production
Ovarian follicle has 2 key cell types: both of these regulate estrogen production and follicular development
Granulosa cell receptors
Theca cell receptors
LH acts on theca cells to promote biosynthesis of androgens → androgens diffuse to neighboring granulosa cells where aromatase enzyme complex converts them to estrogen under the influence of FSH
Granulosa Cell Receptors
FSH receptors
Functions
Promotes follicular growth
Converts androgens into estrogen
In late stage follicles: LH receptors which help prepare the follicle for ovulation and triggers progesterone production
Theca Cell Receptors
LH receptors
Stimulates androstenedione production
Provides androgens to granulosa cells for estrogen synthesis
Progesterone
Depends on LH/FSH
Functions
Implantation of oocyte into endometrium
Sustain pregnancy early in 1st trimester
Produce 24 hours prior to ovulation and lasts for 11 days
Without fertilization: decrease progesterone and decrease FSH/LH
Cycles Diagram
Like to wait for patients to come in at the end of their cycle if they have heavy bleeding → should have a thin lining
A thick lining would mean something abnormal
Oogenesis
Many oocytes (around 12) but usually only one matures before ovulation → others become atretic
The oocytes mature until the follicle containing one of them reaches an average of 18-25 mm diameter and then breaks open → releases oocyte into abdomen (ovulation) and the rest become atretic
Pain from this ovulation → Mittelschmerz
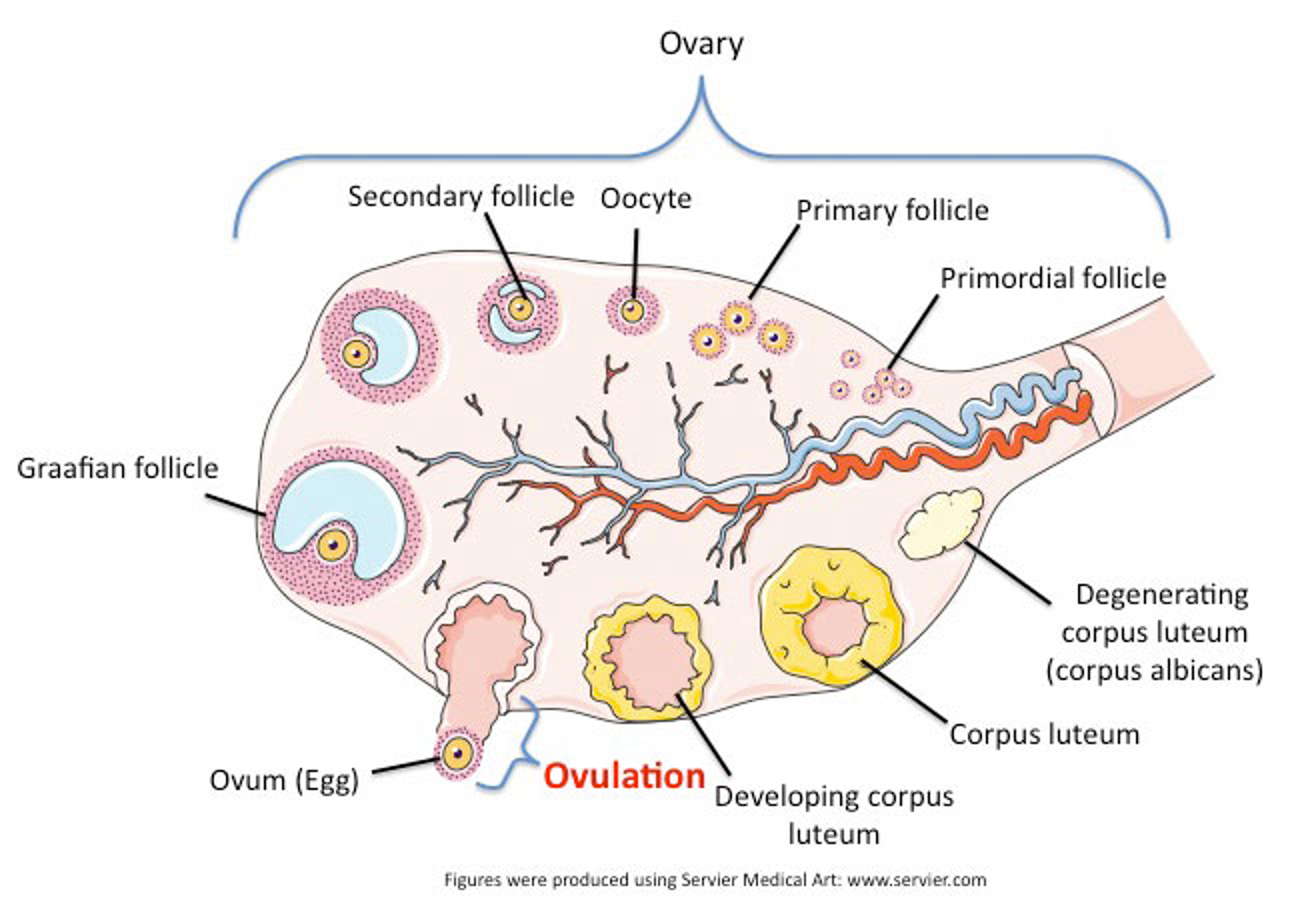
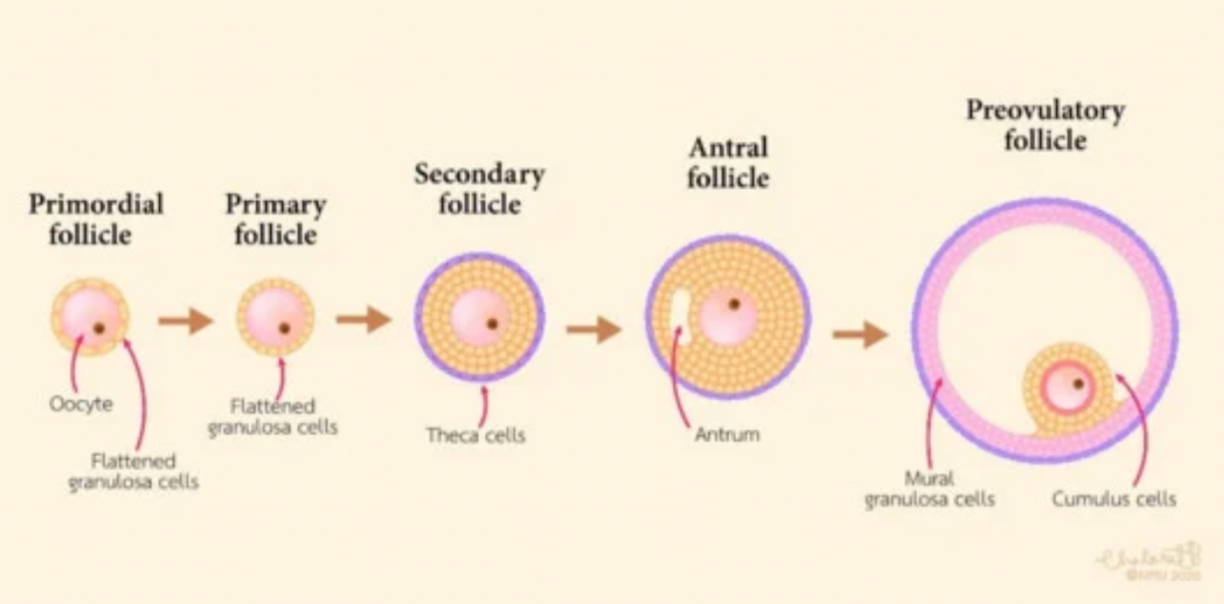
Progression of Follicles
Primordial follicle → seen with anovulation
Pre-antral follicle → most become atretic (do not become mature)
Antral follicle → dominant cell secretes estrogen → decrease FSH → atresia
Pre-ovulatory follicle
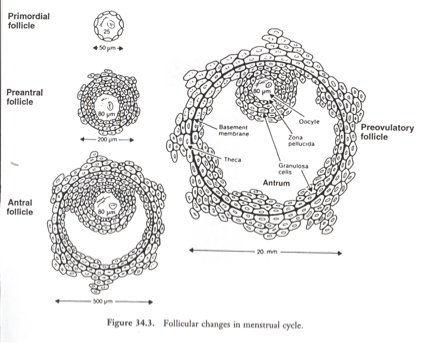
Follicular Changes in Menstrual Cycle Picture
Ovulation
Ovulation 28-36 hours after LH begins to rise and then 8-20 hours after LH peak
Occasional spotting at ovulation caused by changes in estrogen levels
LH surge most reliable indicator of ovulation
LH surge
Completes division of oocyte
Luteinization of granulosa cells
Synthesis of progesterone and prostaglandins (rupture of follicle wall)
Multiple Ovulation
Double ovulation → releasing 2 eggs within 24 hour window
Fraternal twins
Superfetation → ovulation at different times
Extremely rare, but a second ovulation can occur days or weeks later in the same cycle
Can lead to a second pregnancy at a different developmental stage
Sperm can survive 5-7 days, so if ovulation occurs at slightly different times, fertilization can happen days apart
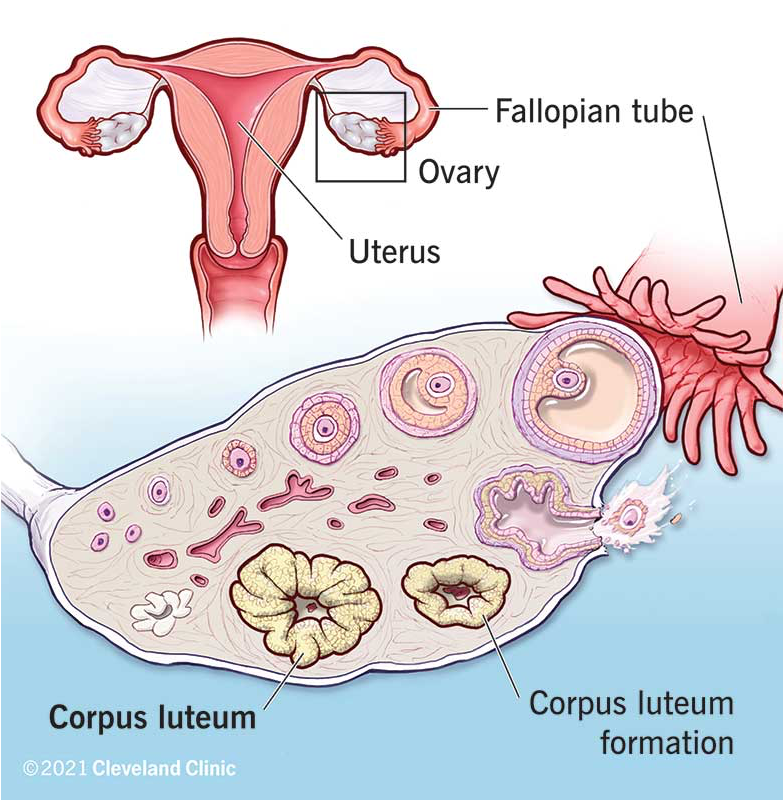
Corpus Luteum
Forms from cells that surrounded oocyte
Maintained 13-14 days unless pregnant
Progesterone peaks 8-9 days post ovulation
When pregnant, corpus luteum produces progesterone for several weeks until placenta can take over
Maintained by hCG early in pregnancy
Defective luteal phase → infertility/spontaneous abortion
Do not have enough progesterone to maintain endometrial lining for successful implantation
Reason for giving someone progesterone the second half of their cycle to help get pregnant
Menstruation
Without pregnancy → decrease steroids → constriction of spiral arteries → ischemia and breakdown of endometrium → bleeding
Corpus luteum becomes corpus albicans
Endometrial lining regenerates and cycle begins all over again
Cycle Changes in the Endometrium