Dog Cat exam 3
1/737
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
738 Terms
heart failure
progressive fatal syndrome where heart
reduces CO
increases venous pressure
deteriorates heart function
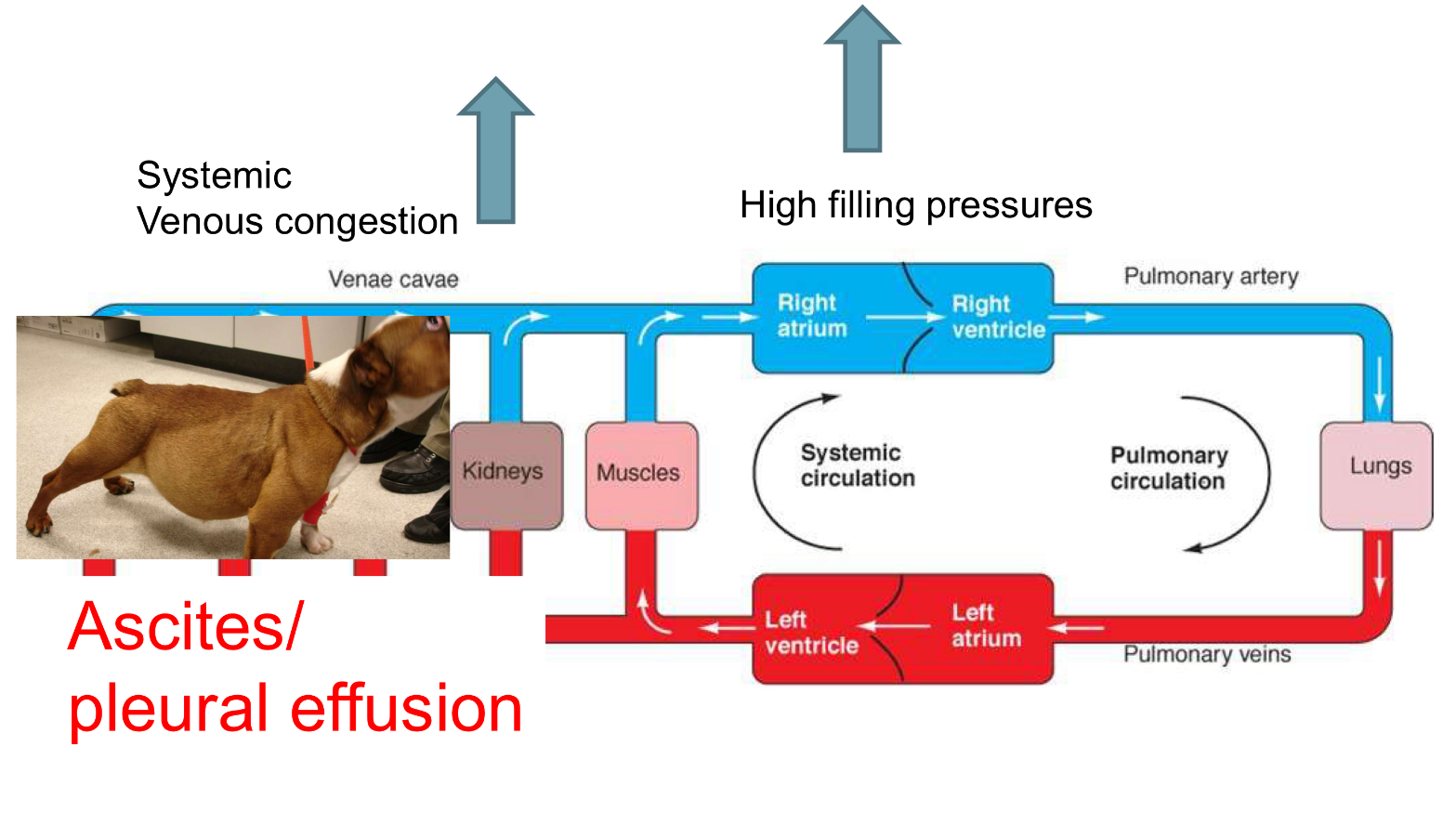
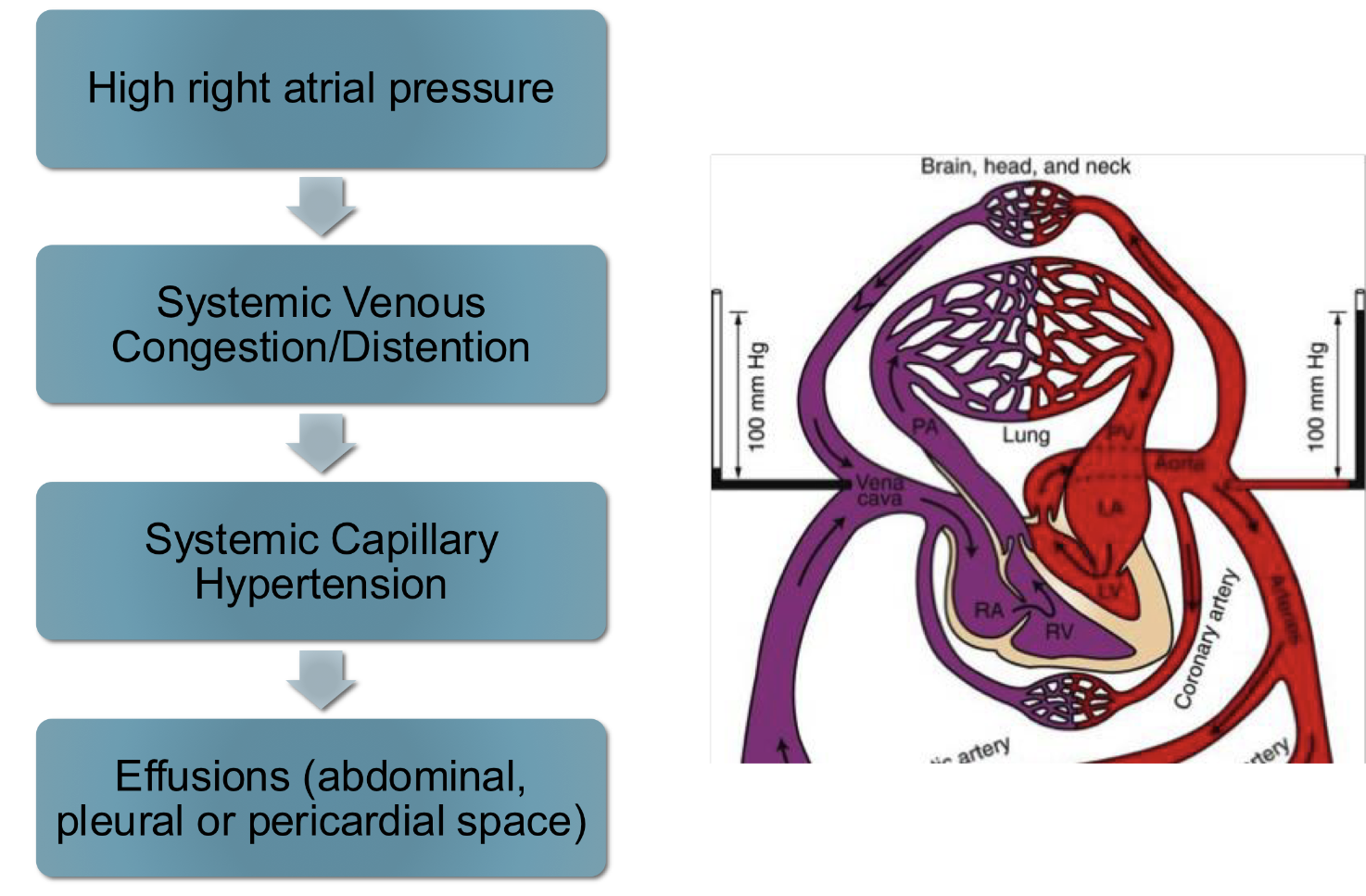
right sided backward (congestive) heart failure signs:
jugular distention
pleural effusion
hepatomegaly
ascites
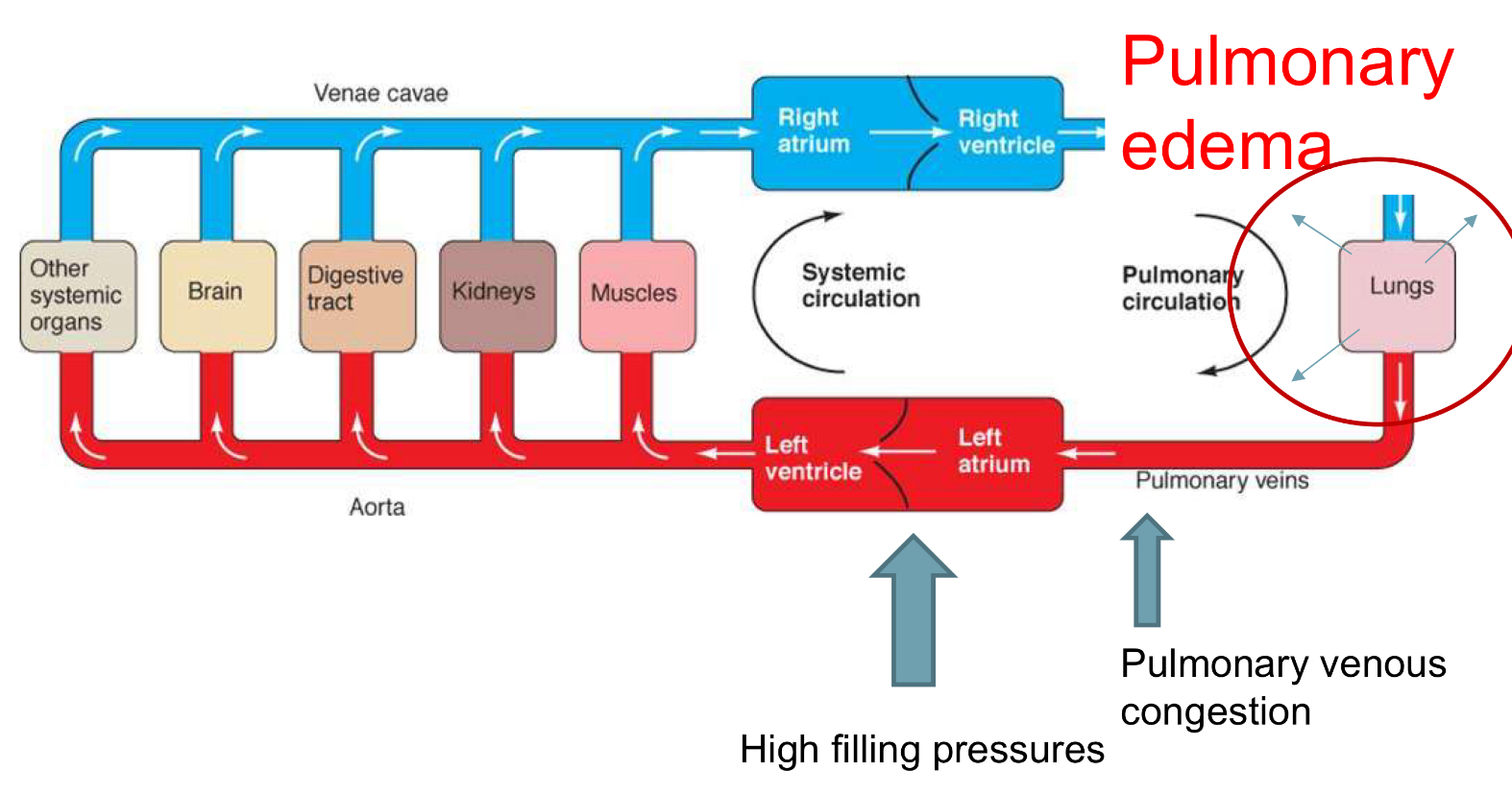
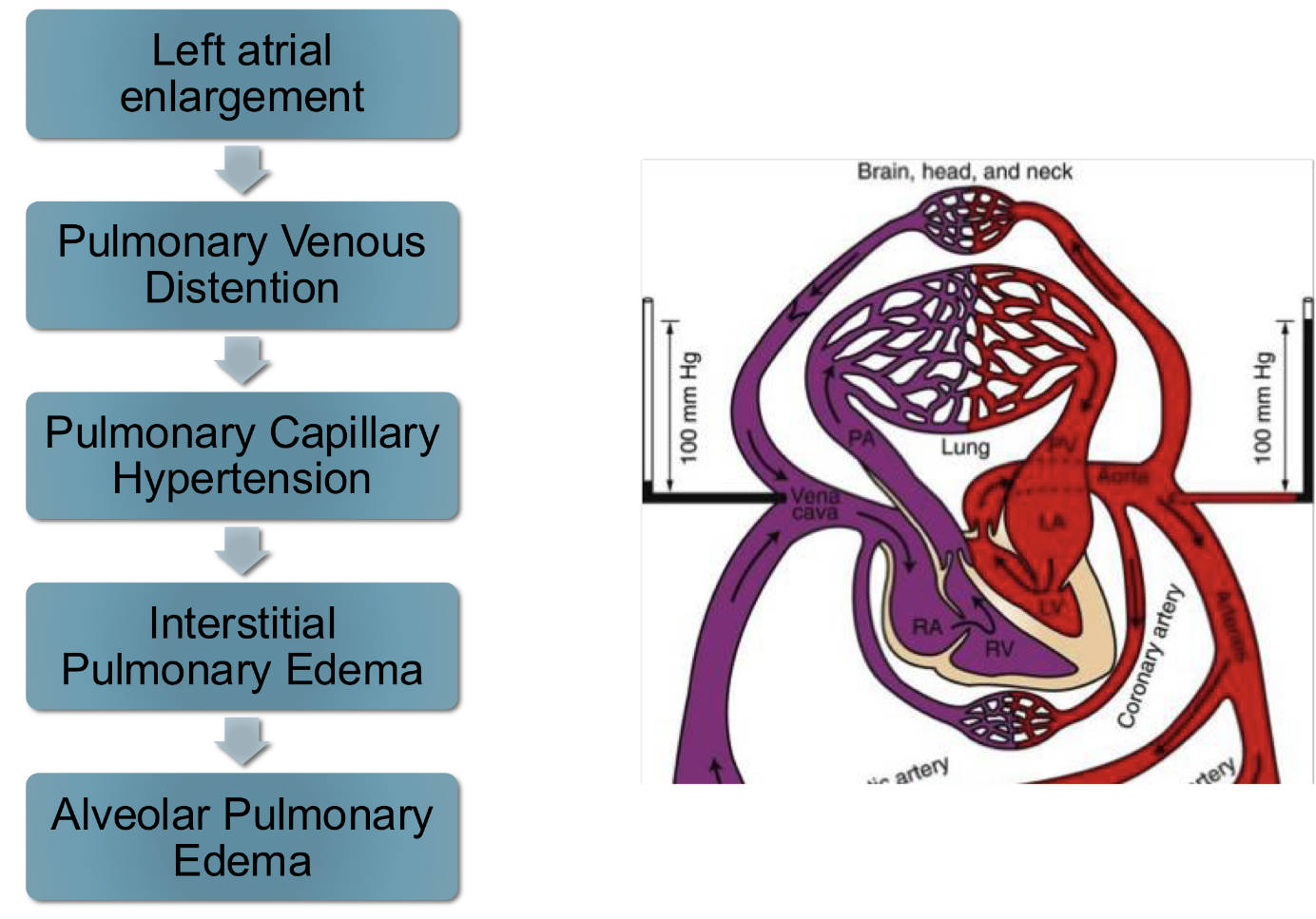
left sided backward (congestive) heart failure signs:
pulmonary edema
pulmonary venous distention
forward heart failure signs:
poor CO
lethargy
weakness
hypotension
exercise intolerance
cold extremities
syncope
azotemia
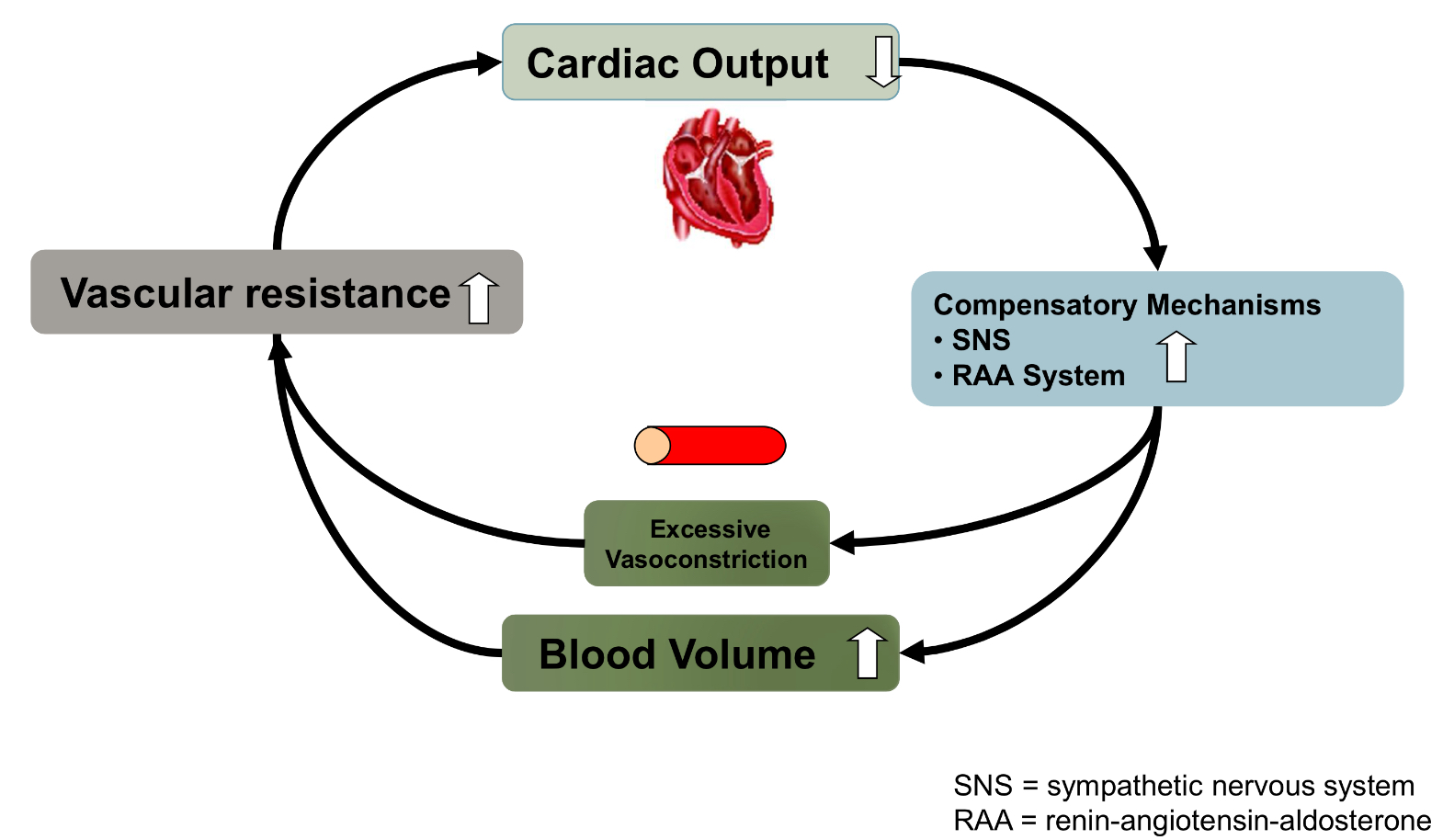
neurohromonal response to heart failure
in the short term these mechanisms increase CO but over time they exacerbate heart failure and reduce CO
sympathetic beta 1 stimulation leads to…
increased HR
increased contractility
improved relaxation
sympathetic alpha stimulation leads to…
vasoconstriction (increased afterload)
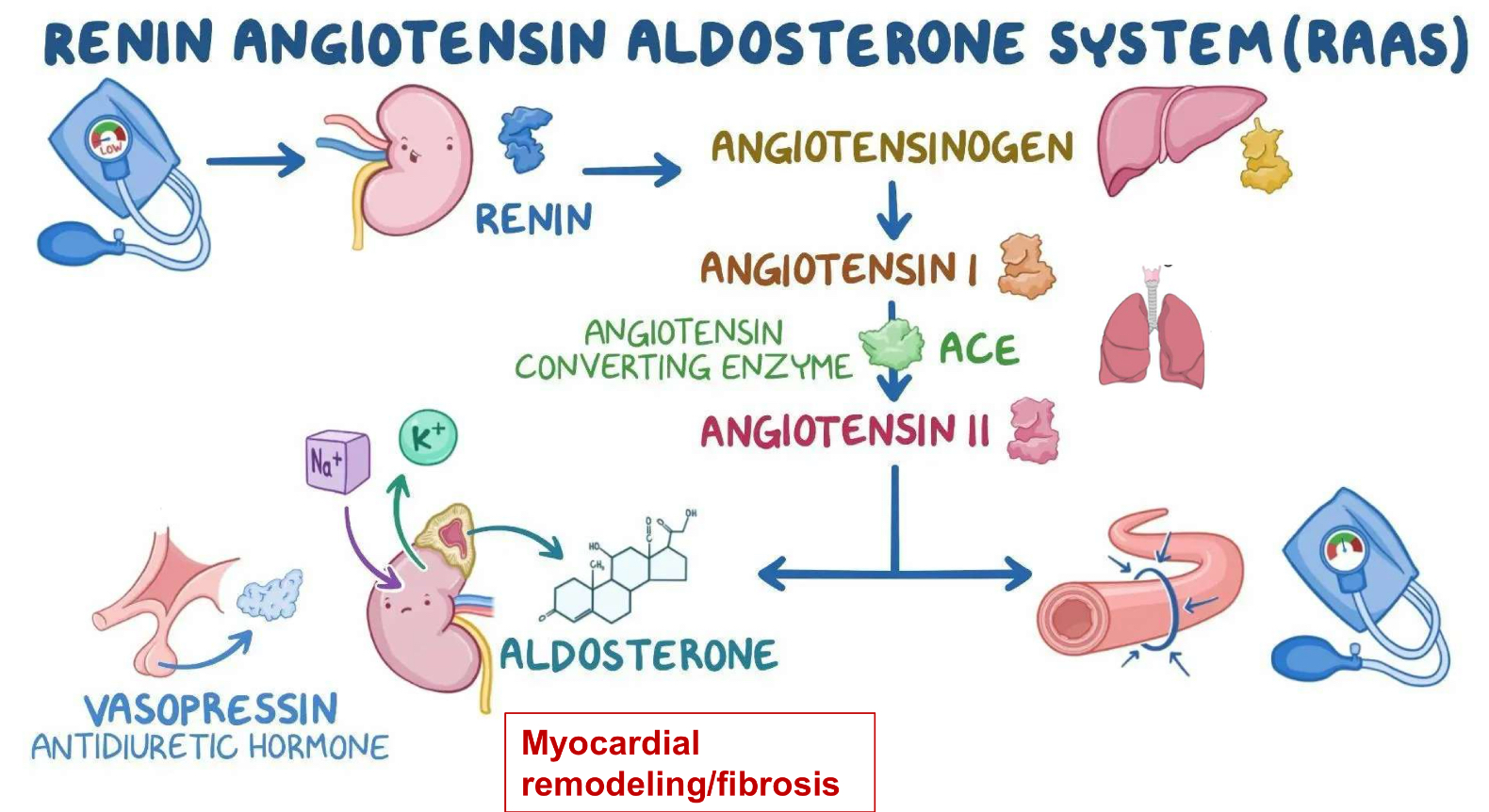
RAAS system
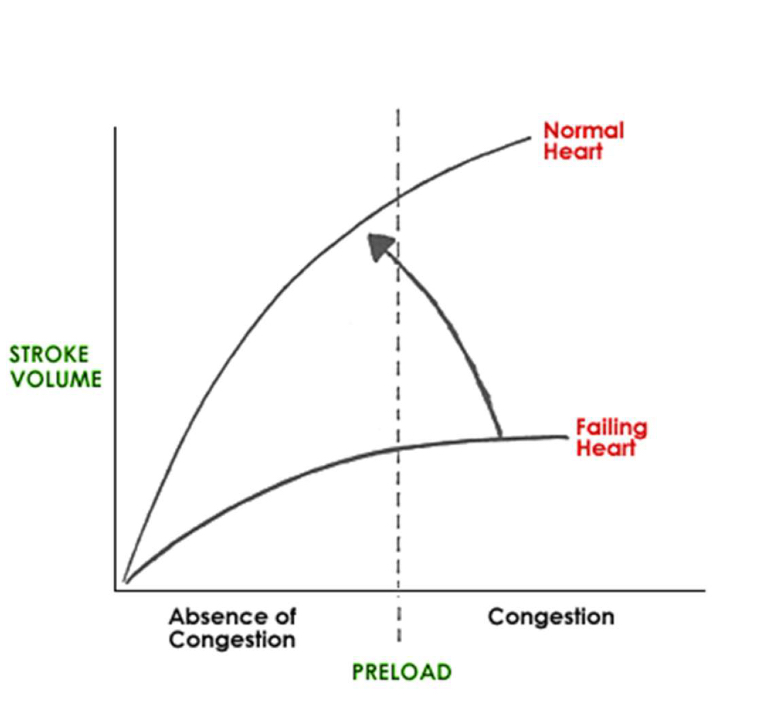
preload
blood volume ventricles are filled with before they contract (measured as end diastolic volume or pressure)
preload is mainly influenced by blood ________
volume
stroke volume
volume of blood ejected with each heartbeat
how does preload affect SV?
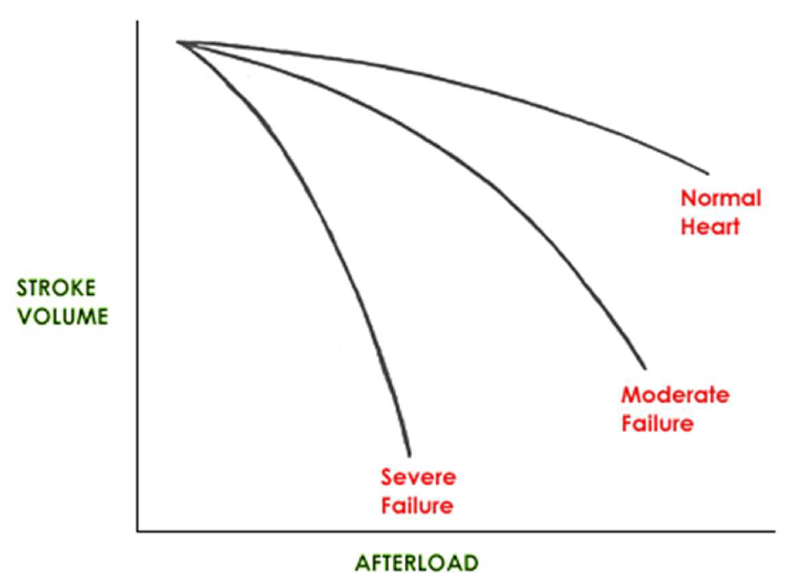
afterload
resistance heart encounters to ejecting blood (increases with increased ventricle volume and arterial resistance)
how does afterload affect SV?
contractility
strength of heart contraction (estimated by echo)
SV increases/decreases with contractility
increases
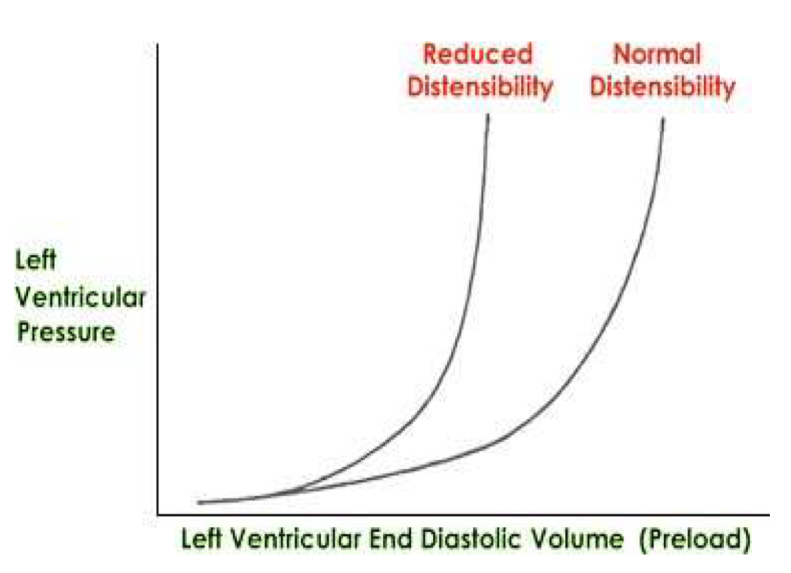
distensibilty
ease of ventricular filling during diastole (ability to stretch)
With decreased distensibility, there is increased/decreased ventricular pressure for the same ventricular volume
increased
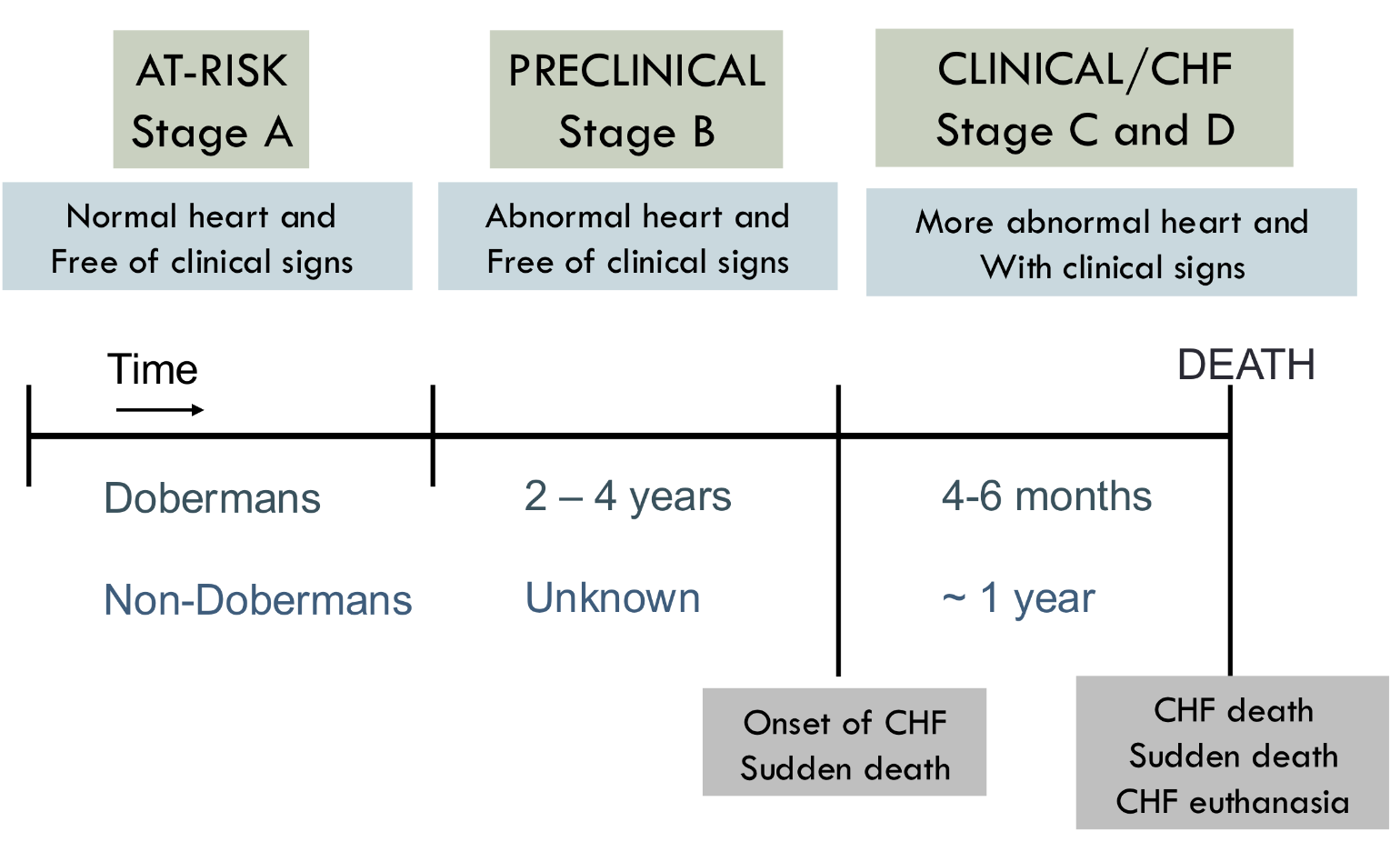
heart failure classification:
A: risk of heart disease
B heart disease with no signs
B1: no chamber enlargement
B2: enlargement left atrium and ventricle
C: past or current signs of heart failure
D: end stage disease
Reduced CO effects:
sympathetic beta stimulation
vasoconstriction
RAAS activation (Na and water retention)
Congestive heart failure resp rate is >_____/min
40
right side CHF signs:
ascites
jugular vein pulsation
murmur grade 1
very quiet that is hard to locate
murmur grade 2
quiet murmur
murmur grade 3
murmur as loud as heart sounds
murmur grade 4
murmur louder than heart sounds
murmur grade 5
very loud murmur with precordial thrill
murmur grade 6
very loud with precordial thrill detected with stethoscope lifeted from chest wall
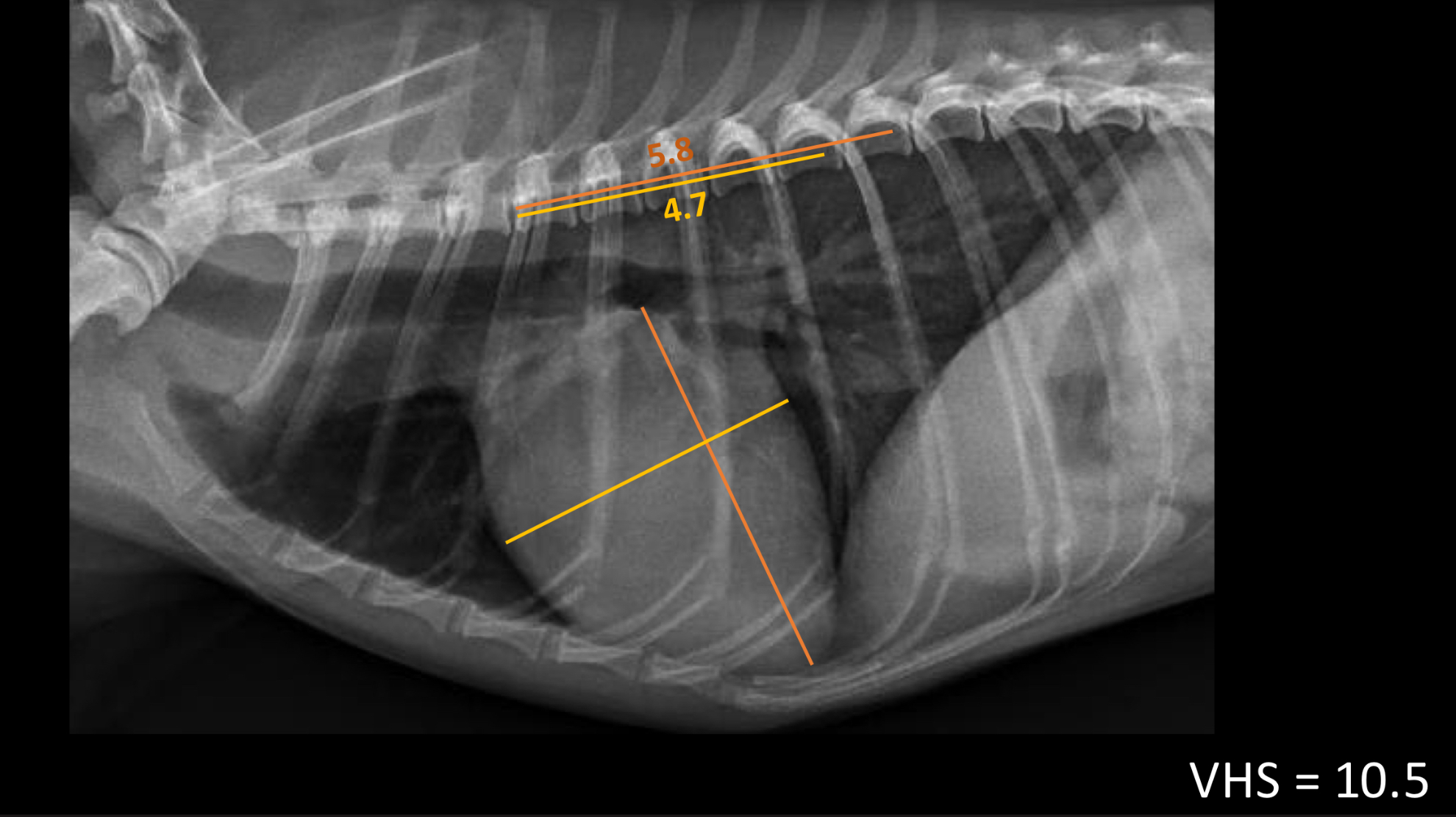
vertebra heart sum in dogs should be <_____ vertebrae
10.5 (measure width and height and add them together)
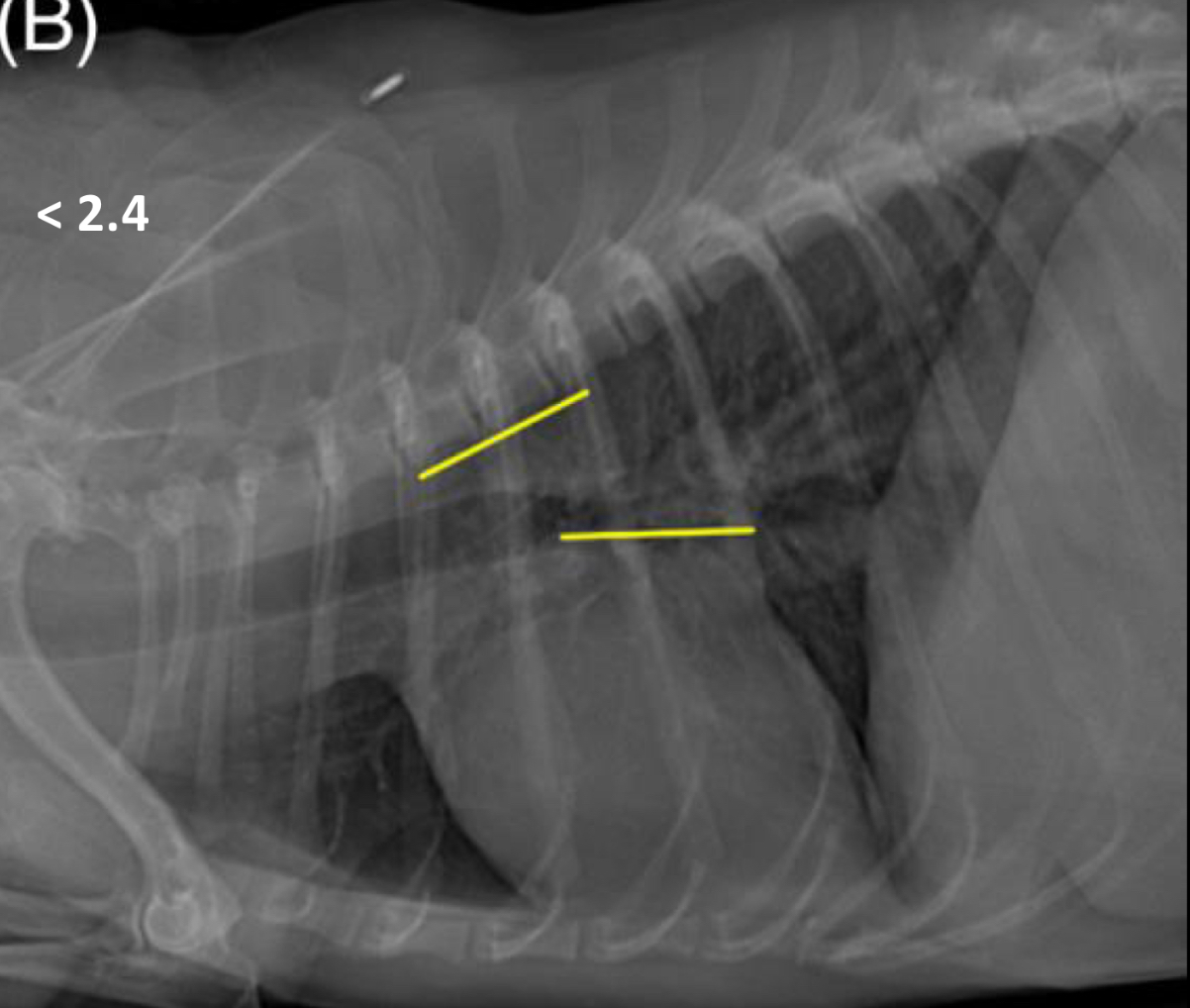
vertebral left atrial size should be < ______ vertebrae
2.4
pulmonary veins should be the same size as the ___ rib
9th
RAAS system activation lab abnormalities:
hypokalemia
pre-renal azotemia
NT-proBNP
marker for congestive heart failure (myocardial stretch)
cardiac troponin I
marker of cardiomyocyte damage (keep in mind a lot of things can damage the heart)
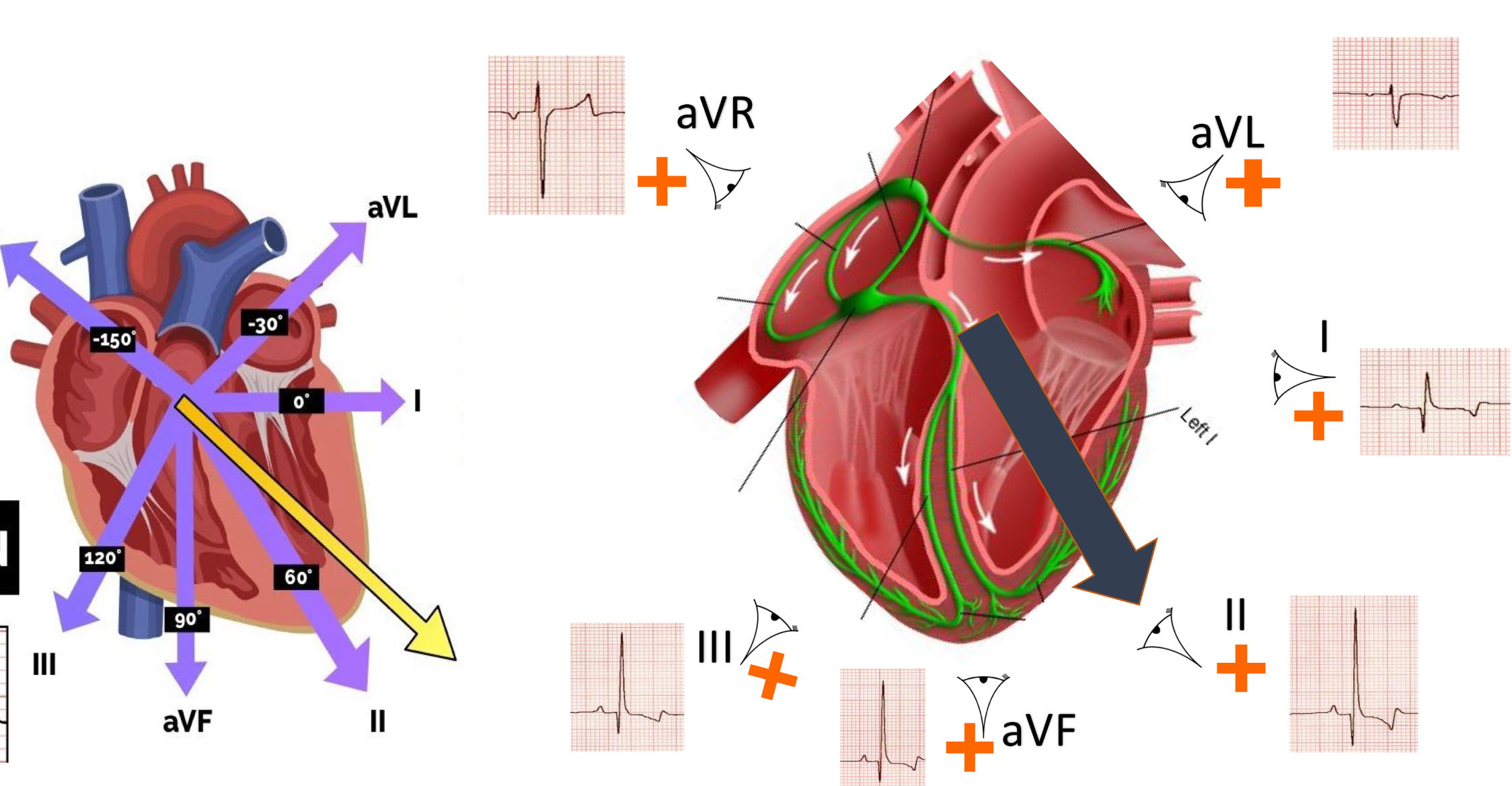
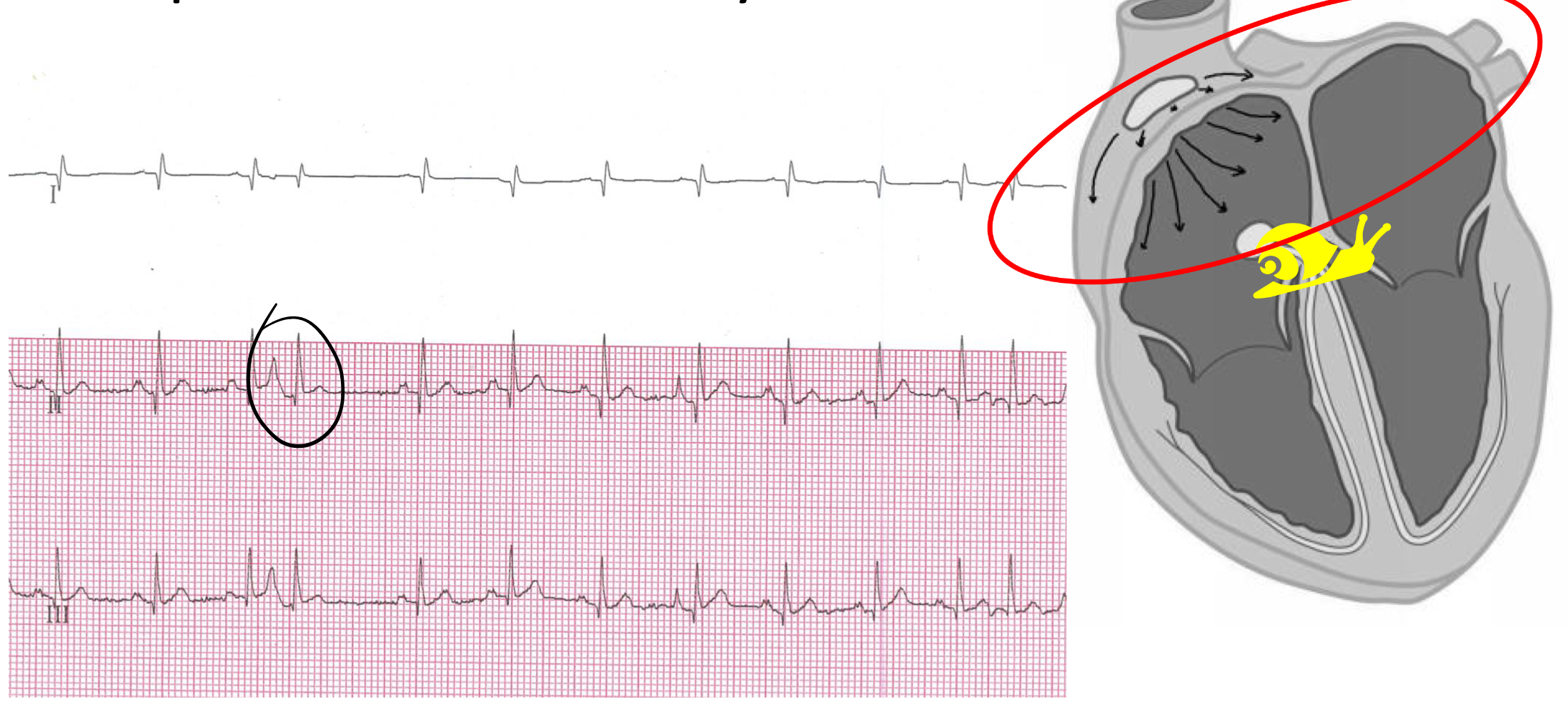
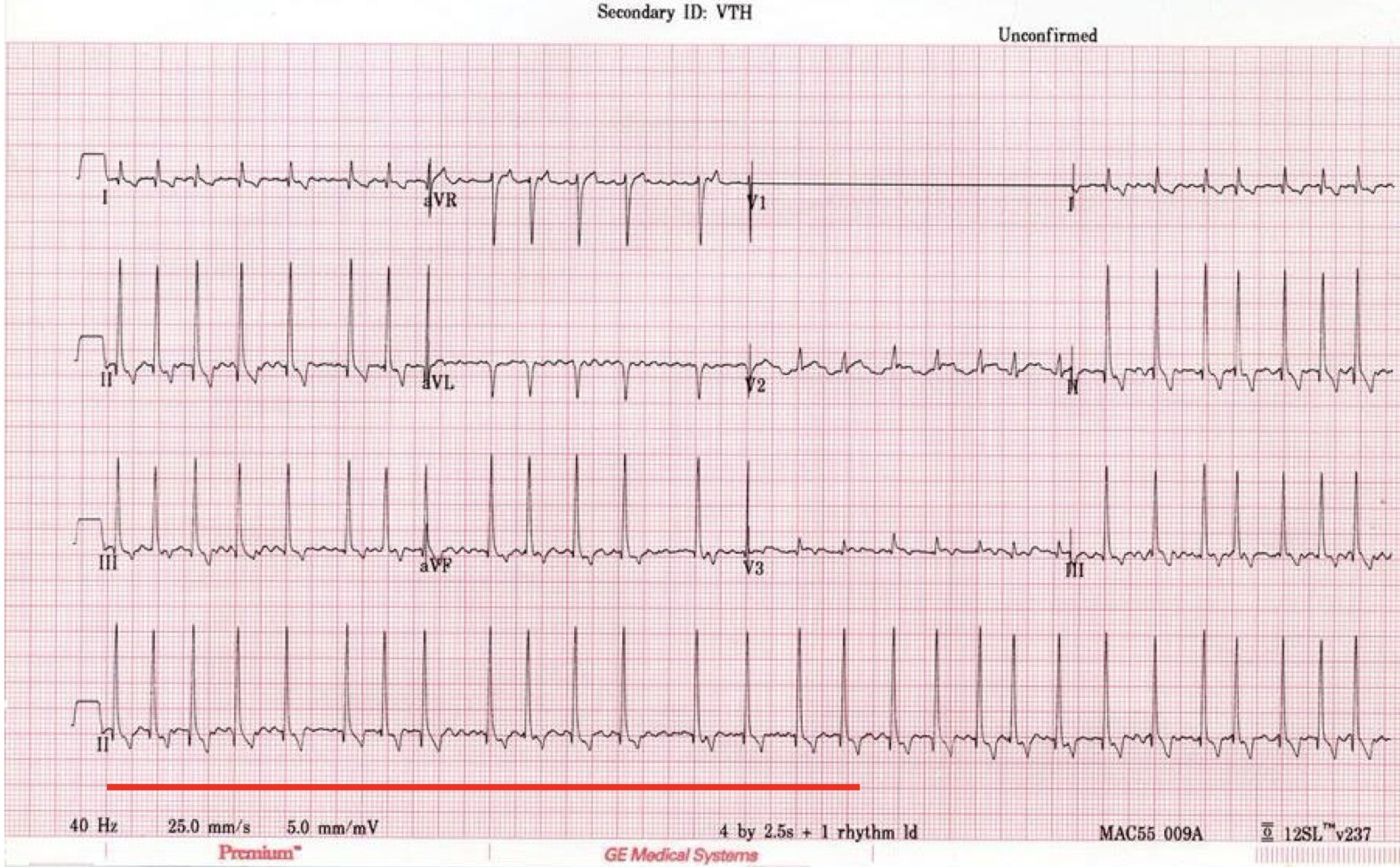
ECG leads
50 mm/s speed
5 cm = 1 sec
complexes x 20 = HR/min
25 mm/s
5 cm = 2 sec
complexes x 10 = HR/min
tachycardia
>160 BPM
ventricular arrhythmia
what kinds of ventricular arrhythmia are treated?
ventricular couplets, triplets, runs
vtach
ventricular arrhythmia treatment:
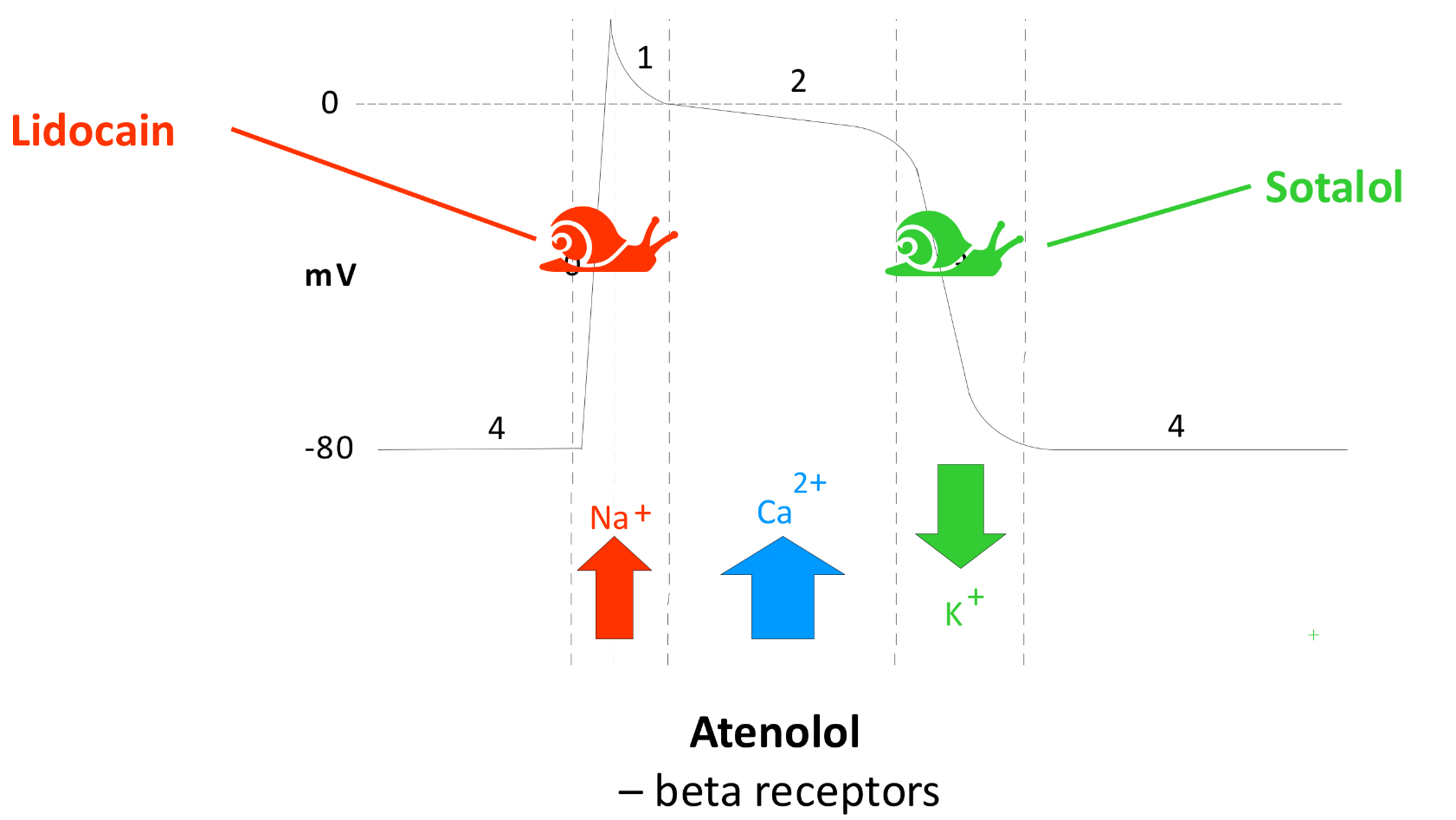
lidocaine IV
sotalol PO
atenolol PO (not in heart failure)
lidocaine, solatol, and atenolol effects:
supraventricular arrhythmia
what kinds of supraventricular arrhythmias are treated?
supraventricular tachycardia
atrial fibrillation
supraventricular arrhythmias treatment:
diltiazem PO or IV (Ca blocker)
sotalol PO
atenolol PO (not for heart disease)
conduction blocks
increase length of time between atrial and ventricular depolarization
mitral valve disease treatment:
furosemide for pulmonary edema
pimobendan to increase contractility
ACE-inhibitor to inhibit RAAS
spirinolactone for anti aldosterone
what should not be done for mitral valve disease?
fluids
drugs that vasoconstrict (dexmedetomidine)
degenerative valvular disease pathogenesis:
mitral regurgitation→increased left atrial volume, pressure→pulmonary edema→ remodeling, myocardial failure
what heart failure categories receive treatment?
B2, C, and D
treatment for valvular disease with B2 heart failure:
pimobendan
treatment for valvular disease with C or D heart failure:
pimobendan
furosemide
ACE inhibitor
spirinolactone
what is the next step for a dog with a 3/6 heart murmur?
thoracic radiographs for vertebral heart sum
what is the next step for a dog with a VHS <10.5?
no treatment, repeat rads in 3-6 months
what is the next step for a dog with a VHS >10.5?
echocardiography
what is the next step for a dog with a B2 heart failure, VHS >11.5, or VLAS >3?
pimobendan
what factors contribute to HCM development in cats?
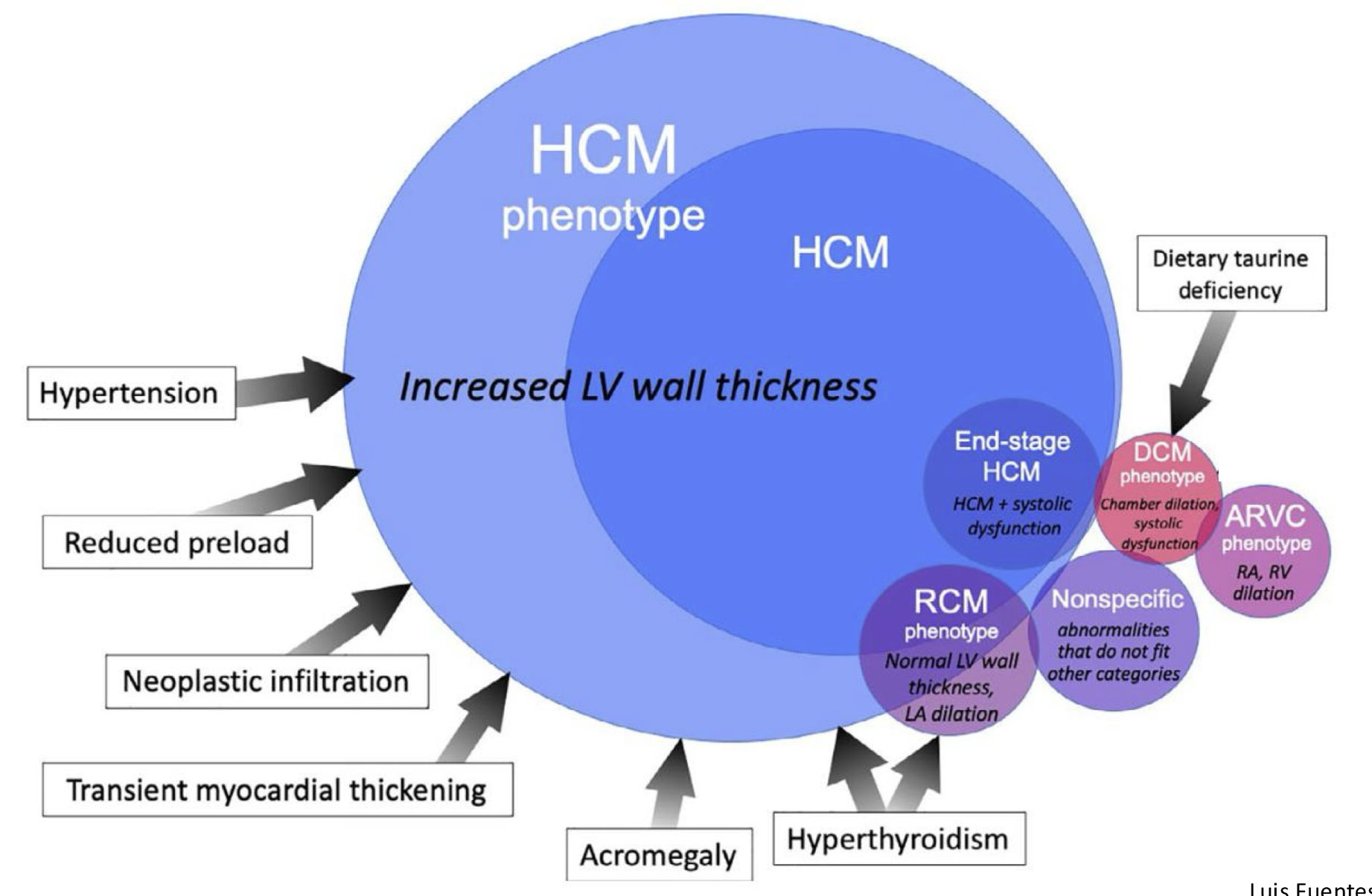
hypertrophic cardiomyopathy types:
localized
generalized
papillary muscle
hypertrophic cardiomyopathy pathogenesis:
left ventricular hypertrophy
impaired left ventricular relaxation
left atrium enlargement
increased pressure in left atrium leading to pulmonary edema
endothelial disruption and slow flow
thrombus formation
section of thrombus dislodges, aortic thromboembolism
obstruction of blood flow
HCM signs:
asymptomatic
heart murmur, gallop
arrhythmia
CHF
sudden paresis/paralysis
tachycardia or bradycardia
tachypnea/dyspnea
pulmonary edema, pleural effusion
weak pulse
where do aortic thromboembolisms occur?
at start of aorta close to heart
saddle thrombus where caudal aorta bifurcates
HCM radiograph findings:
VHS >9.3
pulmonary edema
pleural effusion
HCM echo findings:
hypertrophic left ventricle walls
NT-proBNP
heart product that can predict likelihood of heart disease
what is the treatment for left ventricle outflow tract obstruction with no heart failure?
atenolol
atenolol effects:
reduces HR and prolongs filling
can cause arrhythmias
Rapamycin
drug that regulates mTOR which is involved in cellular growth and stress responses and can potentially be used to slow the progression of HCM
thrombus treatment:
clopidogrel
rivaroxaban
aspirin
low molecular weight heparin (deltaparin, enoxaparin)
CHF treatment:
drain any effusion
furosemide
O2
reduce stress
pimobendan
ACE inhibitor
spirinolactone
cardiomyopathy phenotypes
pulmonary edema pathogenesis:
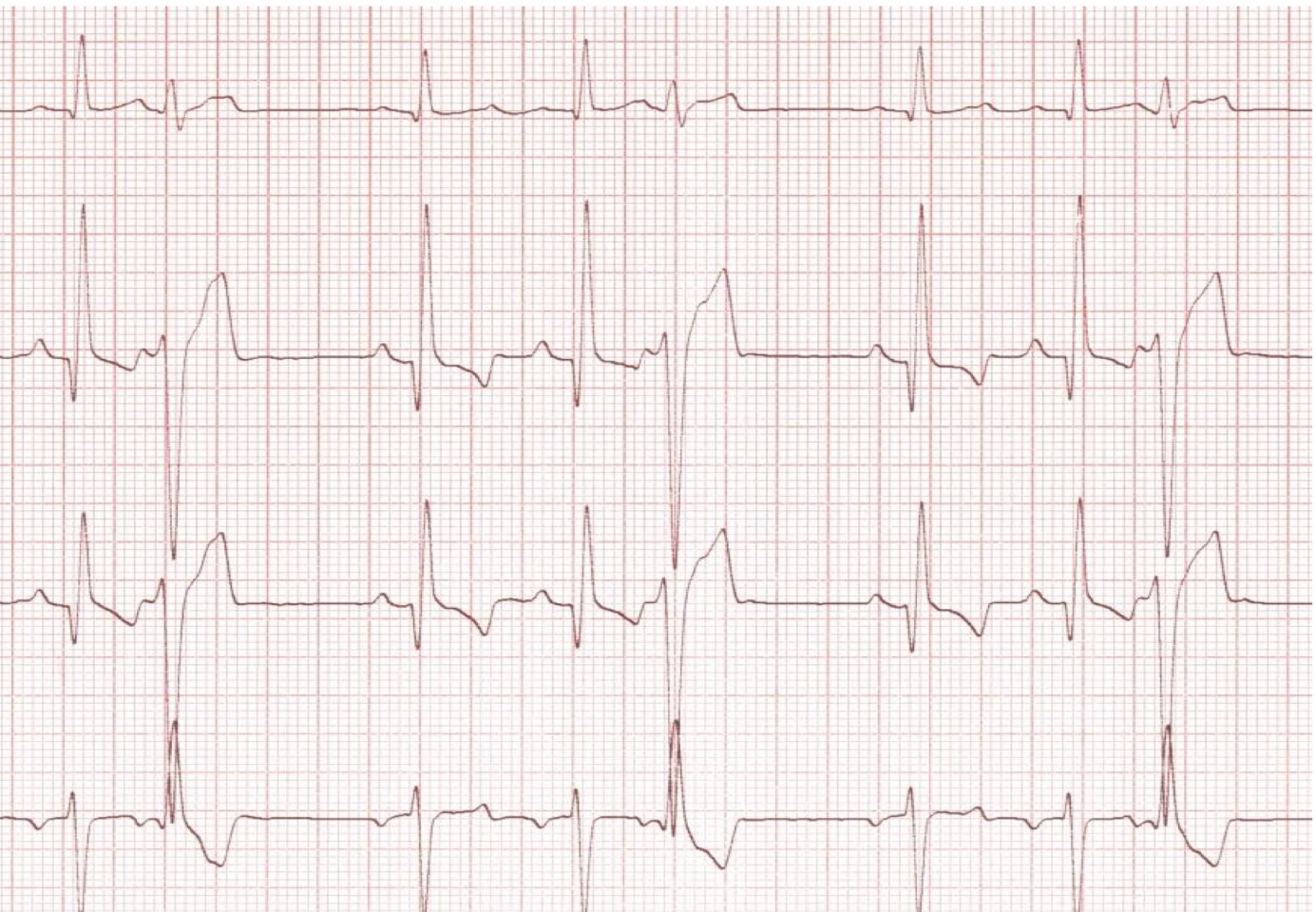
atrial fibrillation
absence of P waves
irregular rhythm
tachycardia
± f waves
narrow QRS complexes
what is the most common clinically relevant arrhythmia diagnosed in dogs?
A-fib (can be secondary to DCM, MVD)
A-fib consequences:
no atrial contribution to filling
tachycardia
reduced CO
increased filling pressures
increased myocardial O2 demand
worsening of CHF
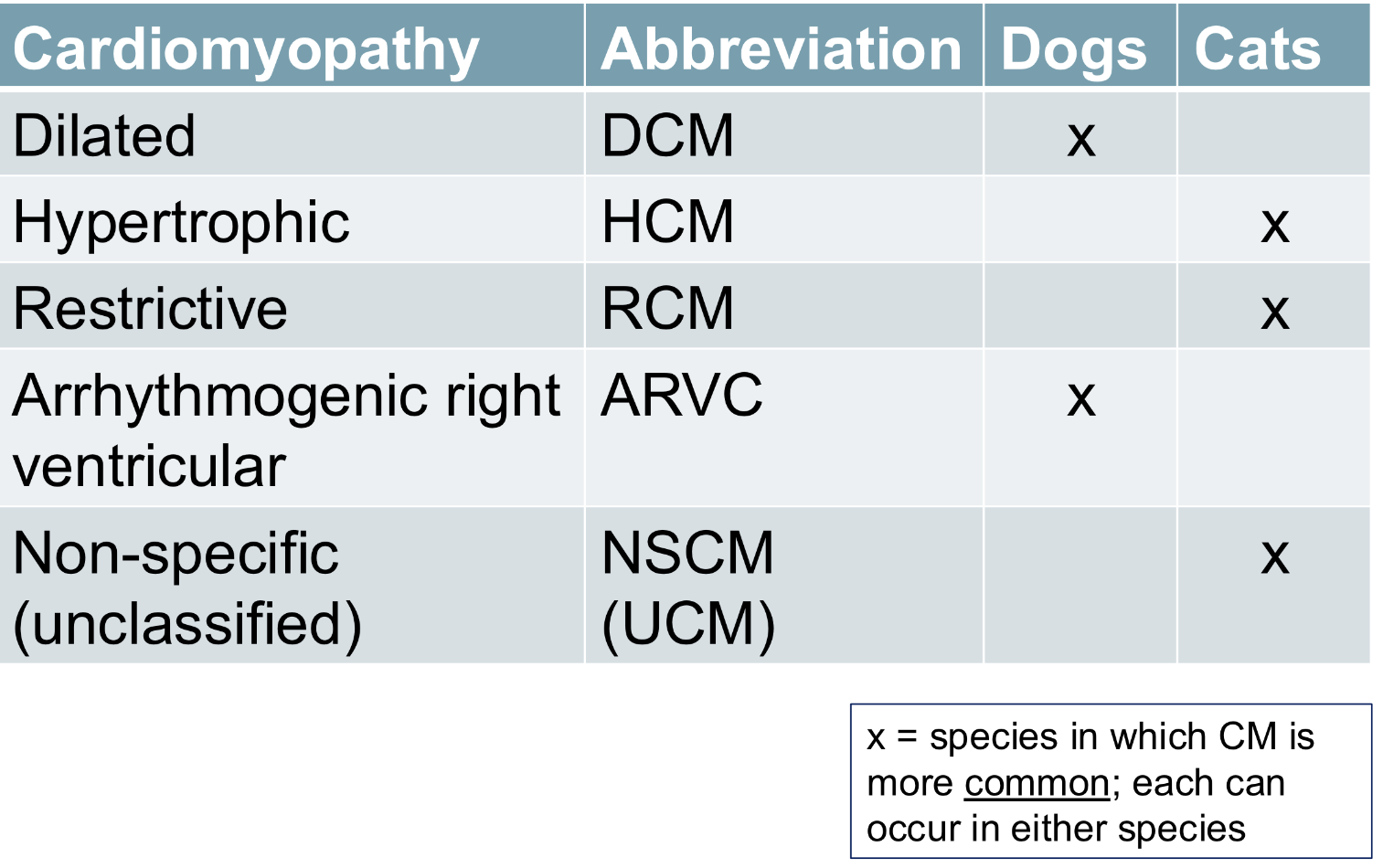
dilated cardiomyopathy phenotype:
dilation of left ± right ventricle
decreased contractility
second most common canine acquired cardiac disease
more common in large dogs
may or may not have heart murmur
DVD/MVD cardiomyopathy phenotype:
small dogs
most common cardiac disease
murmur before heart failure
can cause left atrium or left ventricle dilation secondary to volume overload
causes of primary DCM:
genetic
idiopathic
causes of secondary DCM:
nutritional
tachycardia-induced
toxicity (doxorubicin)
infectious (trypanosoma cruzi/chagas disease)
nutritional DCM is due to…
taurine deficiency
progression of canine DCM
what drugs reduce preload?
furosemide
ACEi
what drugs reduce afterload?
ACEi
pimobendan
what drugs increase contractility?
pimobendan
what drugs increase distensibility?
ACEi
spirinolactone
when should tachycardia be treated in DCM?
pathologic tachyarrhythmia
how to treat stage B DCM:
pimobendan
benazepril
arrhythmogenic right ventricular cardiomyopathy (ARVC)
progressive fibrofatty replacement of right, and to some degree left ventricular myocardium (seen in boxers) that manifests as right ventricle arrhythmias
arrhythmogenic right ventricular cardiomyopathy (ARVC) signs:
asymptomatic
exercise intolerance or syncope associated with ventricular arrhythmia
systolic dysfunction and CHF
arrhythmogenic right ventricular cardiomyopathy (ARVC) diagnosis:
ECG
holter
± echo
myocardial biopsy (best but rarely done)
arrhythmogenic right ventricular cardiomyopathy (ARVC) treatment:
only if clinical signs are present or if arrhythmia is severe
sotalol
mexiletine
combination
ascites pathogenesis:
causes of right sided CHF:
pericardial effusion/cardiac tamponade
pulmonic stenosis
pulmonary hypertension
pericardial effusion/cardiac tamponade pathogenesis:
excessive fluid in pericardial sac→reduced filling of cardiac chambers→reduced cardiac output
causes of pericardial effusion/cardiac tamponade in dogs:
cardiac neoplasia
idiopathic
less common: right CHF, LA tear secondary to valve disease, trauma, migrating foreign body, coagulopathy
causes of pericardial effusion/cardiac tamponade in cats:
CHF
iatrogenic fluid overload
FIP
tumors
pericardial effusion/cardiac tamponade treatment:
pericardiocentesis
right CHF with no pericardial effusion treatment:
ascites: furosemide, pimobendan, abdominocentesis
pulmonary hypertension: sidenafil
continuous left sided heart base murmurs are caused by…
PDA
systolic left sided heart base murmurs are caused by…
aortic stenosis
pulmonic stenosis