Body Systems topic 3
1/126
Earn XP
Description and Tags
Respiratory System
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
127 Terms
basic functions of the respiratory system overall (7)
Olfactory epithelium (olfactory receptors) for sense of smell
Produces sounds
Protects respiratory surfaces from dehydration, temperature changes,
and pathogens
surface area for gas exchange between air and
circulating blood
Moves air to and from exchange surfaces of lungs
Acid-base balance
Regulates pH
define respiration
Respiration is the exchange of gases between the atmosphere, blood, and cells.
what are the three basic steps of respiration?
Ventilation (breathing)
External (pulmonary) respiration
Internal (tissue) respiration
what is contained within the upper and lower respiratory tract
Upper respiratory tract is:
above vocal cords:
nose, nasal cavity
paranasal sinuses
pharynx
Lower respiratory tract is
below vocal cords:
larynx
trachea
bronchi
bronchioles
alveoli
what componants are in the respiratory portion and which are in the conducting system of the respiratory system as a whole
The conducting system consists of:
a series of cavities and tubes
nose
pharynx
larynx
trachea
bronchi
bronchiole
terminal bronchioles
The respiratory portion consists of:
the area where gas exchange occurs
respiratory bronchioles
alveolar ducts
alveolar sacs
alveoli.
define what anatomic dead space is?
It is the air in the conducting portion of the airways which does not take part in the process of gas exchange.
explain the role of the nose in the respiratory system (what are nasal hairs, pathway of air, functions)
Nasal hairs:
in epithelium of vestibule - trap large particles in air (filters)
Skin, nasal bones and cartilage lined with mucous membrane
internal portion communicates with the paranasal sinuses and nasopharynx
through the internal nares
Functions:
warming, moistening, and filtering incoming air
receiving olfactory stimuli
serving as large, hollow resonating chambers to modify speech sounds
what are the paranasal siinuses
Open into nasal cavity
They lighten the skull and resonate voice
There are ethmoid, sphenoid, frontal and maxillary sinuses
What are the tonsils (where and roles)
Where:
at entrance of the respiratory tract
Roles:
Are lymphatic tissues protect against infection.
Lymph nodes monitor lymph drainage from lungs and provide specific defenses when infection occurs.
decribe the pathway of air through the nose
nose vestibule to choanae (internal openings of nasal cavity to pharynx)
through superior, middle, and inferior nasal meatuses
trap particles
warm and humidify
bring olfactory stimuli to receptors
Describe the structure of the nasal cavity
divided into right and left by nasal septum (bones + cartilage)
roof of ethmoid bone
floor is hard plate
superior, middle, and inferior nasal conchae on lateral walls
Describe the two palates in the nasal/oral cavity
Hard palate
forms floor of nasal cavity separates nasal and oral cavities
Soft palate
extends posterior to hard palate divides superior part of the pharynx (nasopharynx) from rest of pharynx
structure/location of pharynx + role
STRUCTURE
skeletal muscular tube
lined with mucous membrane
comprised of three regions:
nasopharynx - respiration
oropharynx - digestion and respiration
laryngopharynx - digestion and respiration
LOCATION
extends from internal nares to cricoid cartilage
ROLES
resonating chamber for speech production
Tonsils in the walls protect entry in body
What is the nasopharynx?
From choanae to soft palate
openings of Eustachian (auditory) tubes from middle ear cavity
adenoids or pharyngeal tonsil in roof
passage for airway only
What is the oropharynx
between the soft plate and epiglottis
common passageway for food and air
what is the laryngopharynx
Extends from epiglottis to cricoid cartilage, and ends as esophagus inferiorly
Common passageway for food and air
What is the larynx
Connects the pharynx with the trachea
contains the:
thyroid cartilage
epiglottis
cricoid cartilage
produces sound
Opening and closing of the vocal folds occurs during breathing and speech
Explain what the thyroid cartilage is
adams apple
what is the epiglottis
a leaf-shaped piece of elastic cartilage which prevents food from entering the larynx.
During swallowing, larynx moves upward, epiglottis bends to cover glottis
what is the cricoid cartilage
a ring of cartilage connects larynx and trachea
explain the process of voice production in the larynx
Speech is a modified sound made by the larynx → requires pharynx, mouth, nasal cavity and sinuses to resonate sound
Vocal folds (true vocal cords) - produce sound
Taut vocal folds produce high pitches
Relaxed vocal folds produce low pitches
Vestibular folds (false vocal cords) found above vocal folds
explain how whispering occurs?
Whispering is forcing air through almost closed rima glottidis - oral cavity alone forms speech.
Tongue and lips movements form words
What is the true vocal cord?
contains skeletal muscles
contains elastic ligaments
when muscles contract of the larynx contract → the cartilage moves and vocal chords are stretched tight.
when air is pushed past tight ligament = sound.
what is laryngitis
Is an inflammation of the larynx - usually caused by respiratory infection or irritants.
explain what the trachea is?
From larynx → T5 anterior → oesophagus → splits into primary bronchii
composed of smooth muscle and c shaped rings of cartilage (keep airway open)
lined by pseudostratified epithelium
cilia remove debris from lungs → throat to be swallowed.
what is a tracheostomy? and intubation
TRACHEOSTOMY
is incision in trachea below cricoid cartilage if larynx is obstructed
Reestablished airflow past an airway obstruction
INSTUBATION:
is passing a tube from mouth or nose through larynx and trachea
Explain the location of the lungs inside the thoracic cavity
Enclosed and protected by the pleural membrane:
Parietal pleura: outer layer attached to wall of thoracic cavity
Visceral pleura: inner layer covering lungs
Pleural cavity is potential space between the pleurae, contains a lubricating fluid secreted by the membranes
Lungs extend from the diaphragm to just slightly superior to the clavicles
lie against the ribs anteriorly and posteriorly
Lungs almost totally fill the thorax
What is visible from the costal surface of the lungs?
apex
base
costal surface of right and left lung
right lung = 3 lobes separated oblique and horizontal fissures.
left lung = 2 lobes separated by oblique fissure and a cardiac notch (depression)
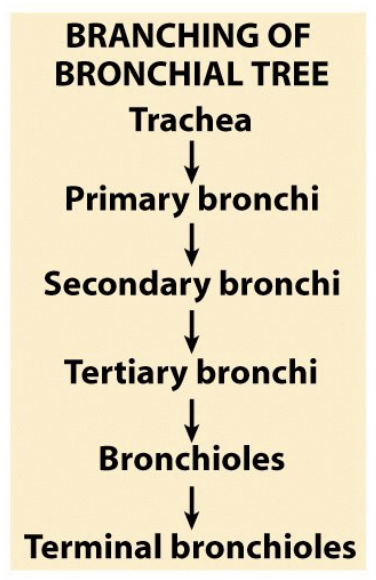
order of branching of the bronchial tree
trachea, primary bronchi, secondary bronchi, tertiary bronchi, bronchioles, terminal bronchioles.
bronchioles → alveoli order
Branchings of single arteriole, venule and bronchiole are wrapped by elastic connective tissue - respiratory bronchioles are also wrapped by smooth muscles that can change diameter of these airways.
respiratory bronchiole → alveolar ducts → alveolar sacs → alveoli → alveolar pores
change in cartilage structure as bronchi branch
When passing deeper into the lungs
Incomplete rings of cartilage replaced by rings of smooth muscle (bronchioles)
then replaced by connective tissue
Histology summary of respiratory system
CONDUCTION COMPONANT -
Transports, cleans, warms, and humidifies air.
Nose, pharynx, larynx, trachea, bronchi, terminal bronchioles
ciliated pseudostratified columnar epithelium
RESPIRATORY PORTION
Gas exchange (O2/CO2 diffusion)
Respiratory bronchioles, alveolar ducts, alveolar sacs, alveoli
progresses from ciliated cuboidal epithelium to squamous epithelium.
histological composition of the respiratory system cells and functions
Epithelial cells - lined with basal cells that are attached to the basement membrane
Squamous epithelial cells - make up the beginning (nasal) and ends (alveoli) of the respiratory tract.
Ciliated and non-ciliated columnar epithelia - Upper tract and large bronchi
cuboidal epithelia - Small bronchi and bronchioles
Surface liquid - overlays the epithelial cells, is mucus, airway liquids, neutralising immunoglobulins, and antimicrobials
Resident leukocytes - line the mucosa, alveolar macrophages are found in lower airways and alveoli
Bronchiole smooth muscle cells - underlying the respiratory tract from the basal end provide structural support and elasticity to the airways.
4 layers of the trachea
mucosa - pseudostratified columnar epithelium with cilia and goblet cells
submucosa - loose connective tissue and seromucous glands
Hyaline cartilage - incomplete rings C-shaped structure closed by trachealis muscle
Adventitia - binds it to other organs
what is required for effective mucociliary drainage
normal cilia
optimum thickness and viscosity of mucous.
what causes increased and decreased mucocilary drainage
INCREASED:
intense exercise
postural drainage
percussion
nebulisation
DECREASED
old age
sleep
disease
dry cold air
explain what cystic fibrosis is?
The airways fill with thick sticky mucus, making it difficult to breathe.
the thick mucus is an ideal breeding ground for bacteria
affects mostly the lungs and digestive system
explain what asthma is?
Asthma is characterised by spasms of smooth muscle in bronchial tubes that result in partial or complete closure of air passageways
Can lead to:
inflammation
inflated alveoli
excess mucus production.
Symptoms
cough
wheeze
shortness of breath
chest tightness
Can treat with nebulisation therapy
what is nebulisation therapy
Nebulisation therapy = inhale mist with chemicals that relax muscle and reduce thickness of mucus.
What are the types of alveolar cells?
Type 1 cells:
simple squamous cells - gas exchange
Type 2 cells (septal cells):
free surface has microvilli
secrete alveolar fluid containing surfactant
Alveolar Macrophages:
remove debris
Alveolar-capillary membrane
Respiratory membrane = 1/2 micron thick
Vast surface area for gas exchange from alveoli to blood
This air-blood barrier is composed of:
alveolar and capillary walls
their fused basal laminas
Define respiration and the tree basic steps
Respiration: exchange of gases between atmosphere, blood, and cells.
Occurs in 3 basic steps:
Pulmonary ventilation (breathing)
External (pulmonary) respiration: all processes involved in exchange of O2 and CO2 with the external environment
Internal (tissue) respiration: uptake of O2 and release of CO2 by cells
Compare hypoxia to anoxia
Hypoxia
Low tissue oxygen levels.
Anoxia
Complete lack of oxygen in tissues.
Explain what pulmonary ventilation is
A mechanical process that depends on volume changes in the thoracic cavity.
Volume changes lead to pressure changes, which lead to the flow of gases to equalise pressure.
Inspiration = Air in lungs < atmospheric pressure
Expiration = Air out Lung > Atmospheric pressure
What is Boyle’s Law?
Boyle’s law: the volume (V) of a gas varies inversely with pressure (P), assuming that temperature is constant.
P = pressure of gas in mm Hg
V = volume of a gas in cubic millimeters
PInitialVInitial = PFinalVFinal
P = 1/V
Explain the role of a change in thoracic cavity size in respiration
when breathing in the thoracic cavity increases
contraction of the diaphragm, flattens, increases chest vertical dimenstions
contraction of the intercostal muscles, increases anterior-posterior dimension of the chest
When breathing out the thoracic cavity shrinks
muscles in expanding thoracic cavity inhalation
sterocleidomastoid
scalenes
external intercostals
diaphragm
muscles in relaxing/shrinking thoracic cavity exhalation
internal intercostals
external oblique muscles
internal oblique muscles
transverse abdominis
rectus abdominis
compare intrapulmonary pressure and intrapleural pressure
Intrapulmonary pressure (Ppul) = pressure within the alveoli
always eventually equalises with atmospheric pressure
Intrapleural pressure (Pip) = pressure within the pleural cavity
intrapleural pressure is always less than intrapulmonary pressure and atmospheric pressure.
both fluctuate with breathing phases
when does lung collapse occur?
is caused by equalisation of the intrapleural pressure with the intrapulmonary pressure
2 forces pull the lungs away from the thoracic wall, promoting lung collapse
Elasticity of lungs causes them to assume smallest possible size
Surface tension of alveolar fluid draws alveoli to their smallest possible size
what is Transpulmonary pressure?
keeps airways open
Transpulmonary pressure = difference between the intrapulmonary and intrapleural pressures (Ppul – Pip)
define inspiration? how?
the movement of air into the lungs.
occurs when
alveolar pressure < atmospheric pressure.
intrapulmonary pressure < atmospheric pressure
HOW?
diaphragm and external muscles increase the size of the thorax, intrapulmonary volume increases and pressure decreases below atmospheric prssure
Air flows into the lungs, down its pressure gradient, until intrapulmonary pressure = atmospheric pressure.
forced vs quiet inspiration?
QUIET INSPIRATION
Diaphragm contacts 1 cm and ribs lifted by external intercostal muscles.
intrathoracic pressure falls and air is inhaled
FORCED INSPIRATION
Accessory muscles of inspiration (sternocleidomastoids, scalenes, and pectoralis minor) lift chest upwards as you gasp for air.
sequence of event for inspiration
inspiratory muscles contract
thoracic cavity volume increases
intrapulmonary volume increases
intrapulmonary pressure drops
air flows into lungs down conc. gradient until = atmospheric pressure
expiration summary
the movement of air out of the lungs.
when alveolar pressure > atmospheric pressure
also an inward pull of surface tension due to the film of alveolar fluid
quiet vs forced EXPIRATION
QUIET:
Passive process with no muscle action
Elastic recoil and surface tension in alveoli pulls inward.
Alveolar pressure increases and air is pushed out
FORCED:
Abdominal mm force diaphragm up
Internal intercostals depress ribs
sequence of events for EXPIRATION
inspiratory muscles relax
thoracic cavity volume decreases
elastic lungs recoil passively
intrapulmonary volume decreases
intrapulmonary pressure rises
air flows out of lungs
relationship between flow F pressure P and resistance R in airways
F = P/R
air resistance and sympathetic nervous system
Sympathetic nervous system stimulates the adrenal gland to release epinephrine (adrenaline) that relaxes smooth muscle and dilates airways
thus, reducing air resistance
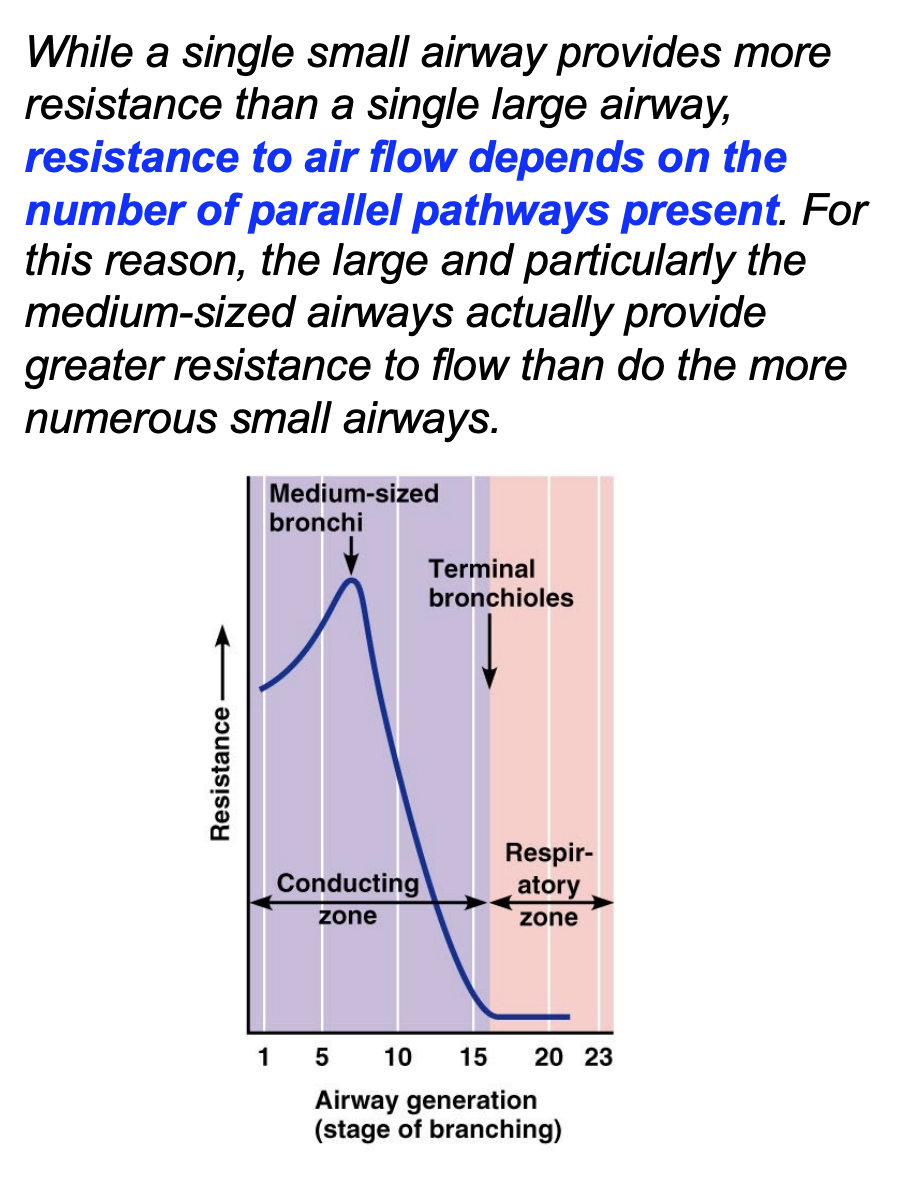
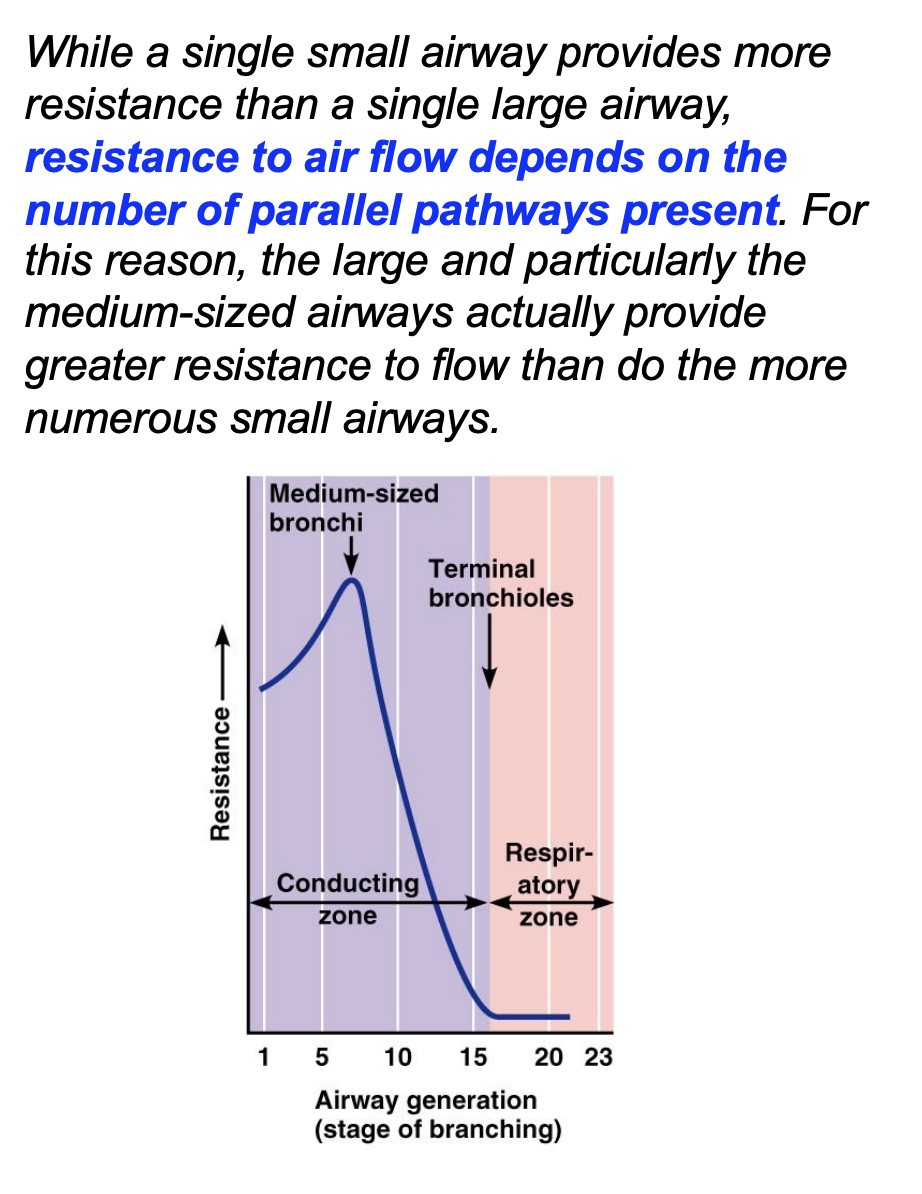
resistance in respiratory passageways
depends on airway size
define surface tension and apply explain what alveolar surface tension is
Surface tension: the attraction of liquid molecules to one another at a liquid-gas interface
The liquid lining the alveoli creates surface tension that acts to minimise surface area, tending to shrink or collapse the alveoli
role of surfactant in reducing alveolar surface tension (what happens in premature babies)
Surfactant = a detergent-like substance, produced by Type II alveolar cells
Surfactant is a substance produced in the lungs that keeps the tiny air sacs (alveoli) open and stable
premature babies
Respiratory Distress Syndrome - Insufficient surfactant in premature babies causes alveoli to collapse at the end of each exhalation
work harder to breathe
define lung compliance
refers to the ability of the lungs to stretch and expand.
A measure of the change in lung volume.
High compliance → easier to expand lungs.
Low compliance à→harder to expand lungs.
what are the two main factors which affect lung compliance?
Distensibility of the lung tissue and surrounding thoracic cage
high volumes = compliance is low
elastic tissue stretched - more effort required to stretch it further
Surface tension of the alveoli
low volumes = compliance low
surfactant decreases surface tension, increases compliance.
which factors can diminish lung compliance?
scar tissue
blocked respiratory passages (fluid/mucus)
reduced surfactant production
low flexibility of thoracic cage
what are factors which affect the work of breathing?
the metabolic needs of the body
the force exerted by the lungs to overcome the resistance of air flow
rate at which respiratory muscles need to generate force (respiratory rate)
what is a pulmonary function test?
spirometer and spirogram
spirometer vs spirogram?
spirometer - measures Air volumes exchanged during breathing and rate of ventilation
Spirogram - the record produced.
what is respiratory minute volume?
Total volume of air taken in one minute
Respiratory minute volume (VE) = respiratory rate × tidal volume
measures pulmonary ventilation
what is alveolar ventilation?
Alveolar ventilation (VA) = respiratory rate × (tidal volume - anatomic dead space)
amount of air reaching alveoli per min
Alveoli contain less O2 than atmospheric air because inhaled air mixes with “used” air
how to increase alveolar ventilation rate?
increase tidal volume
increase respiratory rate
what are the different lung volumes?
tidal volume
amount air moved during quiet breathing
Reserve volumes
amount you can breathe either in or out above that amount of tidal volume
inspiratory and expiratory reserve volumes IRV and ERV
Residual volume
amount of air in lungs after maximal exhalation which is permanently trapped in the system
minimal volume
air trapped in a collapsed lung
what are the types of lung capacity?
Inspiratory capacity
tidal volume + inspiratory reserve volume
Functional residual capacity
expiratory reserve volume + residual volume
Vital Capacity
expiratory reserve volume + tidal volume + inspiratory reserve volume
Total lung capacity
vital capacity + residual volume
what are obstructive vs restrictive pulmonary diseases
Obstructive pulmonary diseases
make it more difficult to get gas out of the lungs = affect expiratory airflow.
Restrictive pulmonary diseases
make it more difficult to get gas into the lungs = affect inspiratory airflow
explain FEV and FVC in the pulmonary function test
FEV - forced expiratory volume in 1 second:
volume of air exhaled in the 1st second during forced exhalation after maximal inspiration
measured using spirometry
FVC - forced vital capacity
maximum amount of air you can forcibly exhale from lungs after fully inhaling.
used to differentiate between obstructive/restrictive lung disease
compare the FVC and FEV of obstructive and restrictive diseases
Obstructive
FVC - normal
FEV - decreased
Restrictive
FVC - decreased
FEV - normal
explain the flow-volume loops pulmonary function test process
Procedure: performed with the patient breathing into a pneumotachograph.
Maximal breath in
Forced aggressive expiration
Maximal fast breath in
what is a peak expiratory flow rate?
The maximum speed of expiration, as measured with a peak flow meter
Peak flow readings are higher when healthy, lower when airways are constricted.
what is a pleural cavity injury
the sealed cavities are opened to the outside
pneumothorax - fill with air
hemothorax - fill with blood
explain daltons law
Each gas in a mixture of gases exerts its own pressure as if all the other gases were not present
Each gas contributes to total pressure in proportion to its relative abundance
Partial pressure (p) = pressure contributed by a single gas in a mixture
Total pressure (P) = the sum of all partial pressures
define air composition
The amounts of O2 and CO2 vary in inspired (atmospheric), alveolar, and expired air.
Alveolar air has less O2 since absorbed by blood
explain what henry’s law is (gas laws)
about diffusion between liquids and gasses
When gas under pressure contacts a liquid, pressure forces gas molecules into the solution.
Henry’s law = the amount of a gas that will dissolve in a liquid is proportional to the partial pressure of the gas and its solubility coefficient (its physical or chemical attraction for water), when the temperature remains constant.
Equilibrium:
gas molecules diffuse out of liquid as quickly as they enter it.
number of gas molecules in solution is constant.
what are some phenomena explained by henry’s law?
narcosis
motion sickness
why you can breathe compressed air while scuba diving despite 79% nitrogen.
decompression sickness (in divivers)
clinical application of henry’s law?
hyperbaric oxygenation
involves breathing pure O2 in a pressurised environment
treat decompression sickness, heart disorders, carbon monoxide poisoning etc.
what is the V/Q ratio?
V = ventilation = the amount of air you breathe in
Q = Perfusion = blood blow
V/Q ratio = the amount of air that reaches lungs divided by the amount of blood flow in the capillaries in lungs.
increased perfusion in the lungs - decreases V/Q
decreased perfusion in the lungs - increases V/Q
VQ ratio on healthy individual
3.3 at the apex, 1at the middle lung, 0.63 at the base
From high to lower air ventilation (more at top apex of lung then bottom base)
what is a V/Q mismatch
an abnormal V/Q ratio, part of the lung receives oxygen without blood flow or blood flow without oxygen
can cause:
hypoxemia (low O2 in blood)
respiratory failure
what is the respiratory rate?
number of breaths per minute
what is tidal volume?
amount of air moved per breath (ml)
how to calculate respiratory volume?
Respiratory minute volume (VE) = respiratory rate × tidal volume
Total volume of air taken in one minute
Measures pulmonary ventilation
what is repiratory minute volume (Ve) set to match
the needs of:
must match metabolic requirements (O2 delivered CO2 removed)
exercise - Ve increases → hyperpnoea (abnormally deep respiration)
hyperventilation (rapid and deep) - ventilation excessive - pCO2 decreases
what is the unit for blood gas levels?
1 Torr = 1mmHg
Torr is a non-SI unit of pressure
internal vs external respiration?
Internal:
occurring inside the cells
External:
between alveolus and capillary
how does the rate of diffusion of gasses change with altitude - why?
pO2 - rate of diffusion decreases as altitude increases.
what affects diffusion rate in lungs
alveolar surface area
diffusion distance (cells between)
O2 and Co2 which diffuse faster
O2 diffuses faster through membrane
co2 more easily dissolved in fluids though
how to restore V/Q ratio if perfusion to an area of the lung falls?
To restore V/Q matching we need to decrease ventilation
via bronchocontriction
Decreased blood flow results in decreased ventilation.
how to restore V/Q ratio if ventillation to an area of the lung falls?
To restore V/Q matching we need to decrease perfusion
via vasoconstriction
Decreased ventilation results in decreased perfusion.
Decreased ventilation results in decreased perfusion.
Causes of hypoxemia - (Abnormal arterial blood gases (bad))
Causes of hypoxemia (hypoxaemia = low O2 levels in blood)
insufficient O2 in the alveoli
low o2
insufficient ventillation
insufficient diffusion from alveoli into blood
imbalance between ventilation of alveoli and blood flow to alveoli
V/Q mismatch
what causes Hypocarbia or hypocapnia
Is a decrease in alveolar and blood pCO2 below 35 mmHg
caused by:
excessive removal of CO2 from the body
Ventilation removes CO2 so hypocapnia is due to hyperventilation