CM3 M5L1: Peri-Operative Surgical Management
1/85
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
86 Terms
When is a Urine pregnancy test (UPT) included within Pre-op workup?
any female of childbearing age (even if they had tubal ligation!)
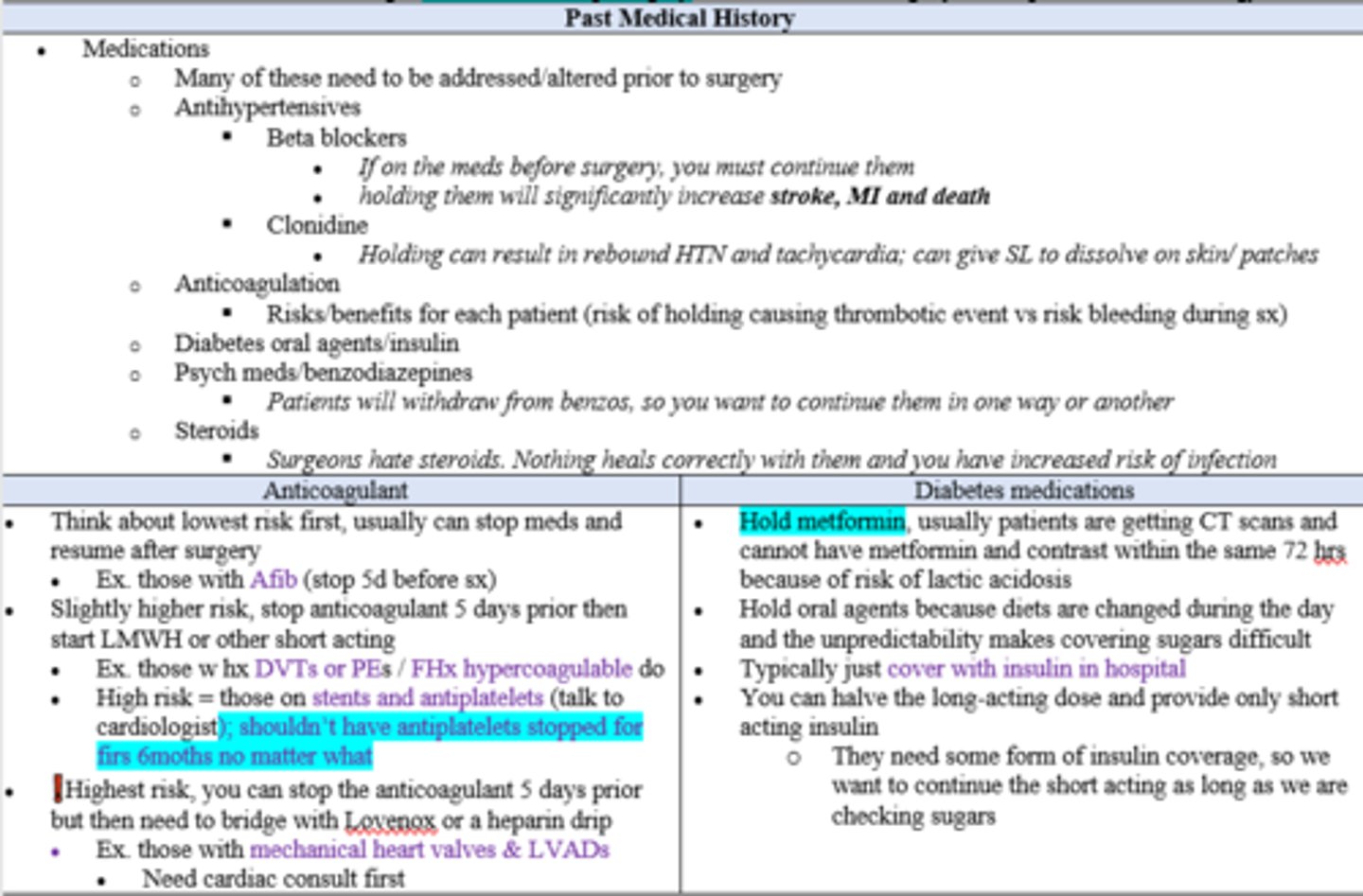
In a pre-op evaluation, what are some medications which should be evaluated prior to surgery?
Antihypertensives (But DO NOT HOLD Beta Blockers or clonidine)
Anticoagulants (Consider risk/benefits)
Diabetic oral agents (typically cover with insulin in hospital)
Psych Meds (FYI Holding benzos may cause w/d)
Steroids (keep them on if already taking, can delay healing and increase risk for infection)
(True/False) Preoperative Antianginal medications, including beta- blockers, calcium channel blockers, and nitrates, should be continued throughout the perioperative period.
True
(however, don't START a Beta Blocker on day of surgery, because it has a risk of causing bradycardia and hypotension if not gradually titrated up prior to surgery)
All patients undergoing vascular surgery or have been deemed high risk for cardiac complications, regardless of lipid levels, should be considered for prophylactic ______________.
HMG-CoA reductase inhibitors (aka "-Statins")
(True/False) Preoperative Coronary revascularization (i.e. CABG or PCI) should be performed only on patients who have guideline-concordant indications independent of the planned non-cardiac operation.
True
Surgical patients who have undergone recent coronary stenting are at high risk for stent thrombosis, especially if antiplatelet therapy is stopped prematurely.
Therefore, elective surgery should be deferred for at least ______ after placement of a bare-metal stent and ideally for ______ after placement of a drug-eluting stent.
30 days /1 month;
6 months (or 3 months if life-saving cancer surgery)
Patients with Acute Coronary Syndromes require immediate management of their cardiac disease prior to any preoperative evaluation. Postoperative MI typically occur within 3 days of surgery and are associated with a 30-day mortality rate of 11.6%. What signs and symptoms can you expect in a pt having a post-op MI?
- NO chest pain
- unexplained Hypotension (low BP)
- Hypoxemia (low serum O2)
- Delirium (confused, agitated)
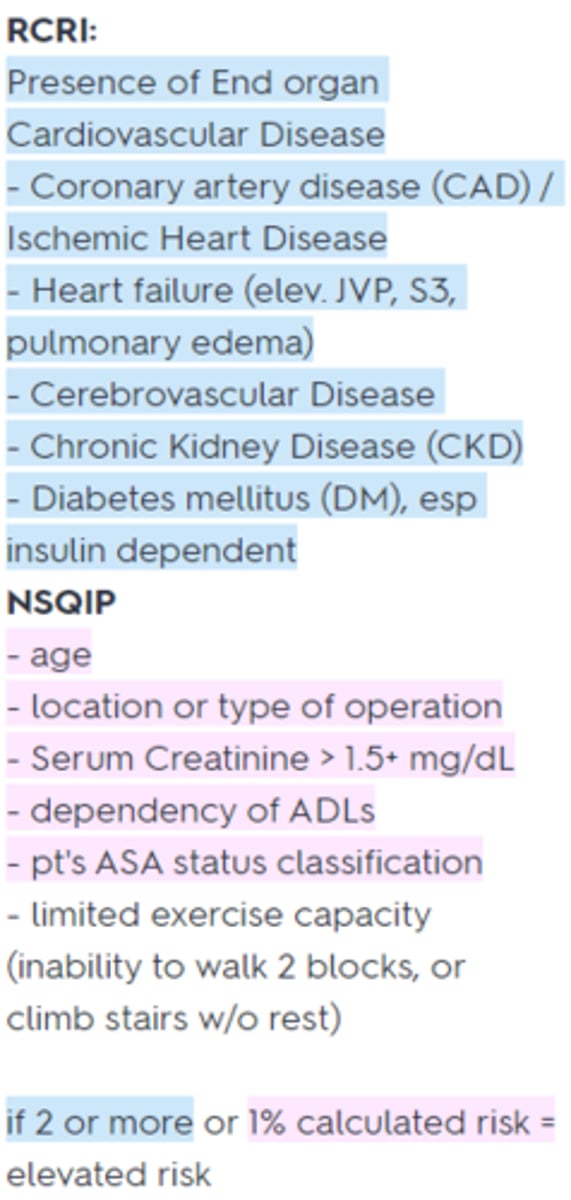
What past medical hx specific risk factors (according to the Revised Cardiac Risk Index (RCRI) and National Surgical Quality Improvement Program (NSQIP) prediction tools) increase the risk of postoperative cardiac complications (i.e. MI, or cardiac arrest) and therefore need non-invasive ischemia testing (ECG, Stress test)?
RCRI:
Presence of End organ Cardiovascular Disease (CAD, HF, CVD, CKD, DM)
NSQIP
Age, type of operation, SrCr >1.5+ mg/dL, ADL dependency, ASA classification, exercise capacity
if 2 or more or 1% calculated risk = elevated risk (see pic)
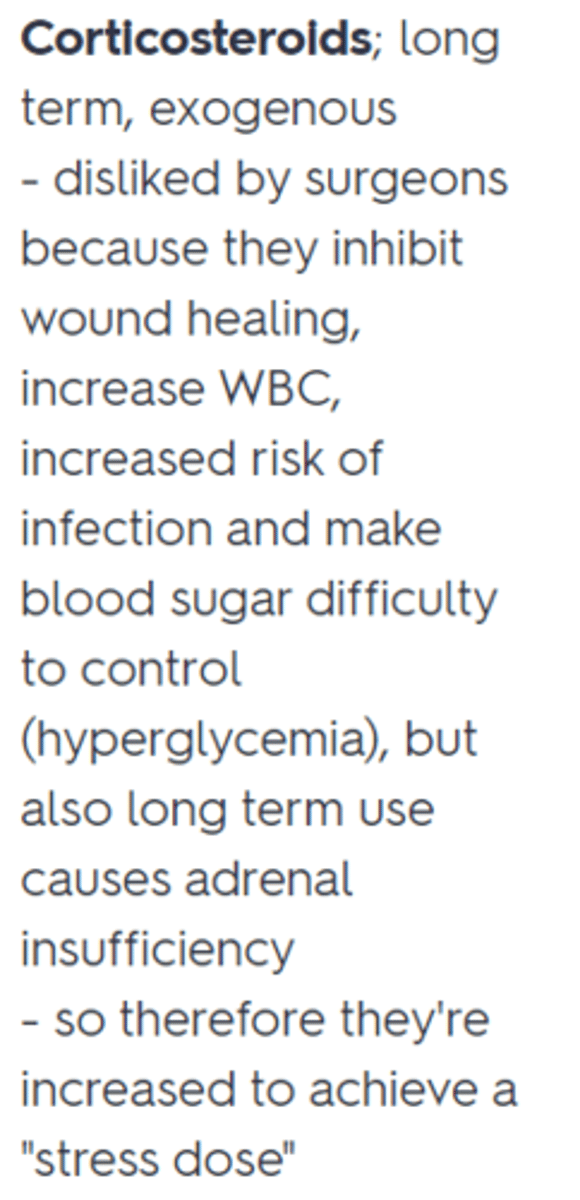
In patients with risk of adrenal insufficiency, which medication class might you INCREASE prior to surgery in order to prevent peri-surgical hypotension by increasing catecholamine production?
Corticosteroids (Stress Dose steroids needed for moderate to major surgery; must keep patients on them if already taking - see pic)
When is a Basic Metabolic Panel (BMP) included within Pre-op workup?
- Renal Dysfunction
- Hepatic Dysfunction
- Diabetes
- Diuretic Therapy (K+ sparing vs. K+ wasting)
When is a Complete Blood Count (CBC) included within Pre-op workup?
- h/o Anemia
- Hepatic Dysfunction
- Cancer diagnosis
- Dialysis pts (usually anemic and thrombocytic)
- Large surgery with significant expected blood loss
What types of surgeries carry a higher risk of postoperative cardiac complications due to their associated major fluid shifts, hemorrhage, and hypoxemia (according to RCRI) and therefore should undergo a more thorough cardiac clearance (aka pre-operative Noninvasive ischemia testing)
Major (Abd/intraperitoneal; intrathoracic, vascular - esp suprainguinal or AAA repair)
(FYI Emergency Procedures are also high risk, but should not be delayed for pre-op cardiac testing regardless - will just monitor very closely perioperatively)
When are Coagulation Studies included within Pre-op workup?
- recent anticoagulation
- h/o bleeding disorder / coagulopathy
- Cirrhosis (decreased II, VII, IX, X - may need FFP)
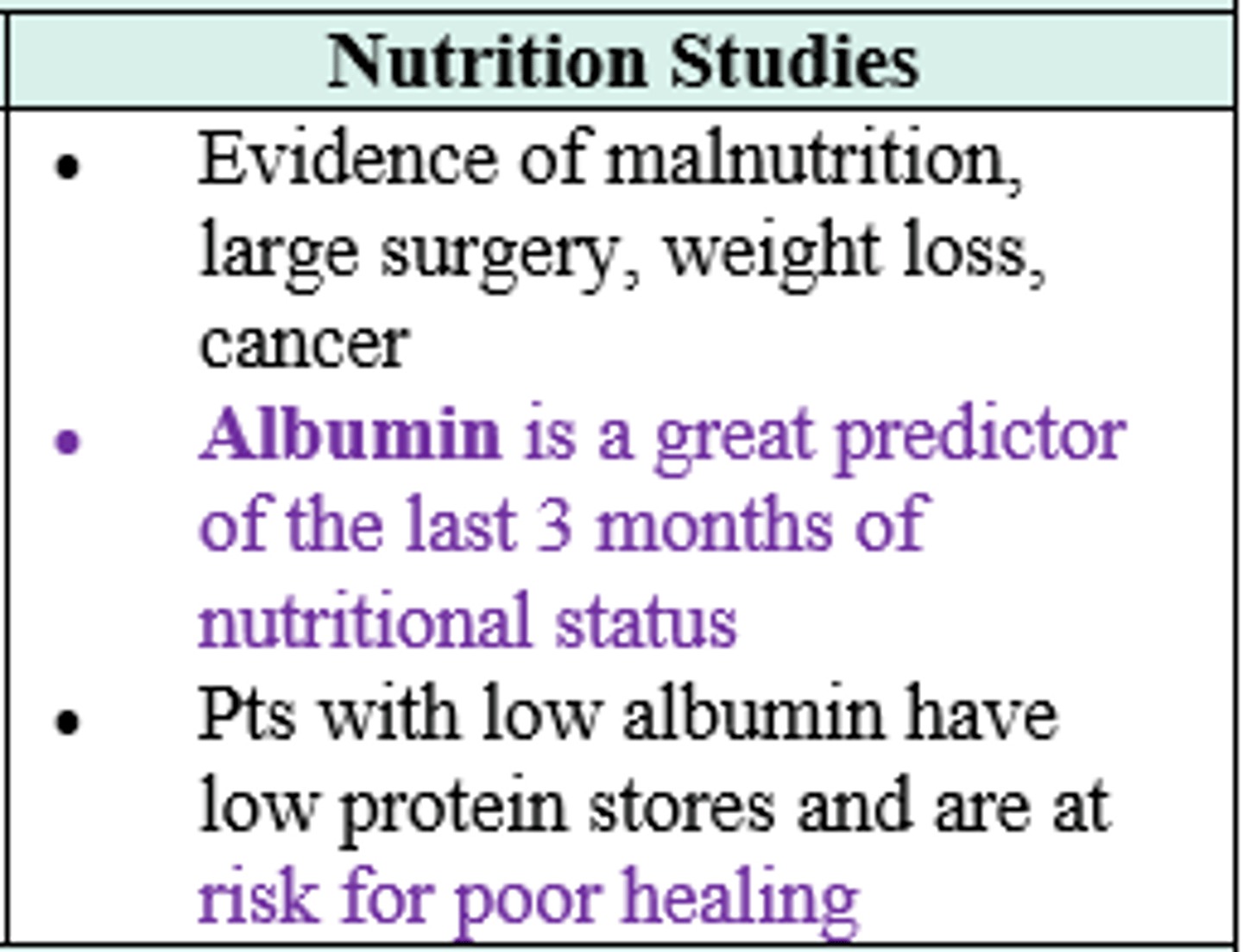
When is a Nutrition Studies included within Pre-op workup?
- evidence of malnutrition
- large surgery
- weight loss
- cancer
When is a CXR included within Pre-op workup?
- intra-thoracic surgery
- Active Lung Disease
- Concern for Metastatic Disease (rhonchi or rales on PE)
When is a EKG included within Pre-op workup?
- any cardiac surgery
- any high risk surgery (i.e. Major vascular surgery)
- h/o cardk,lnh iac risk factors in intermediate risk surgery (i.e. CVA, CHF, Creatine >2, DM requiring Insulin, Ischemic Cardiac Disease)
What types of surgeries don't require preoperative noninvasive ischemia testing (EKG, stress test, etc.), esp. if pt is < 50yo and asymptomatic ?
Low risk Surgery
(Breast surgery
- EGD
- Colonoscopy
- cataract surgery
- or other Ambulatory surgeries/ outpatient)
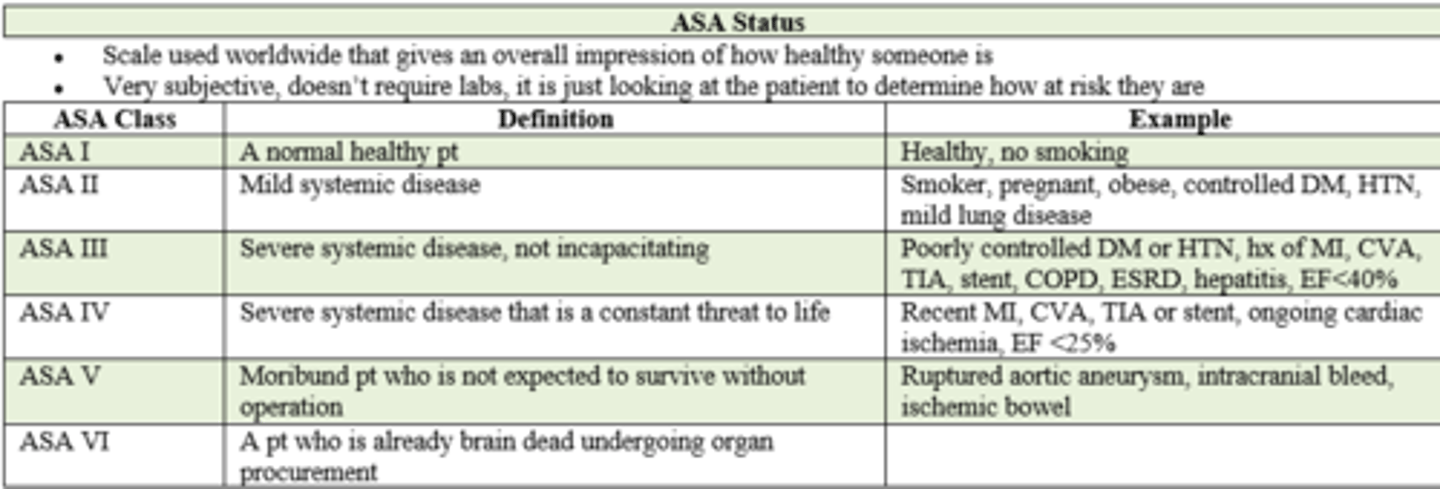
What is a classification system, in addition to either the RCRI or NSQIP risk prediction tools, that's used in pre-op evaluation to assess a pt's surgical risk for peri-op / post op complications ?
American Society of Anesthesiology (ASA) Status
- ranges from Class 1 (normal healthy pt) - 6 (brain dead, undergoing organ procurement for donation)
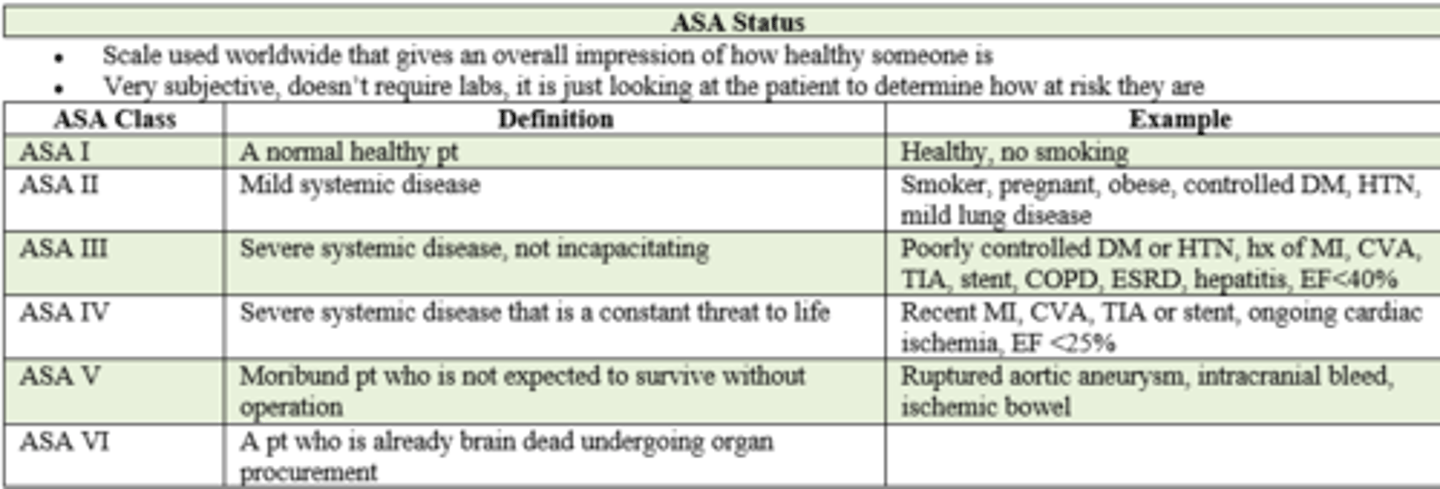
if a pt has poorly controlled DM, HTN, and an extensive pmhx of MI, CVA, TIA, stent placement, COPD, ESRD, hepatitis, and ejection fraction of < 40%, what is their ASA status prior to surgery?
ASA III / 3
- severe systemic disease,
- not incapacitating
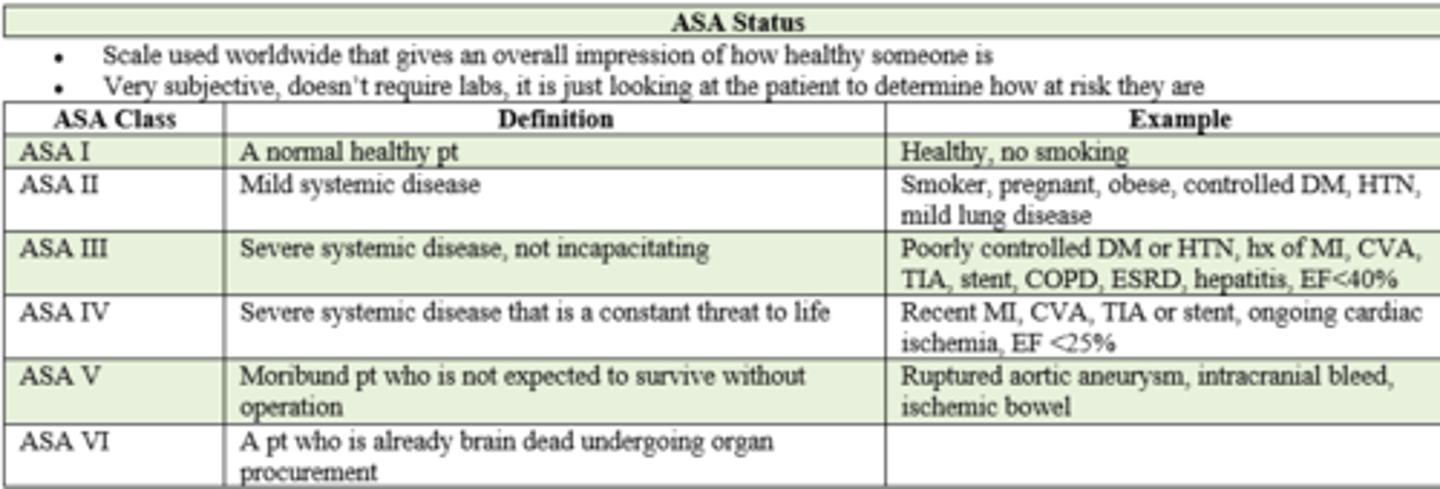
If a pt is a smoker, pregnant, obese, but her DM, HTN, and mild lung disease is under control, what is her ASA status prior to surgery?
ASA II / 2
- mild systemic disease
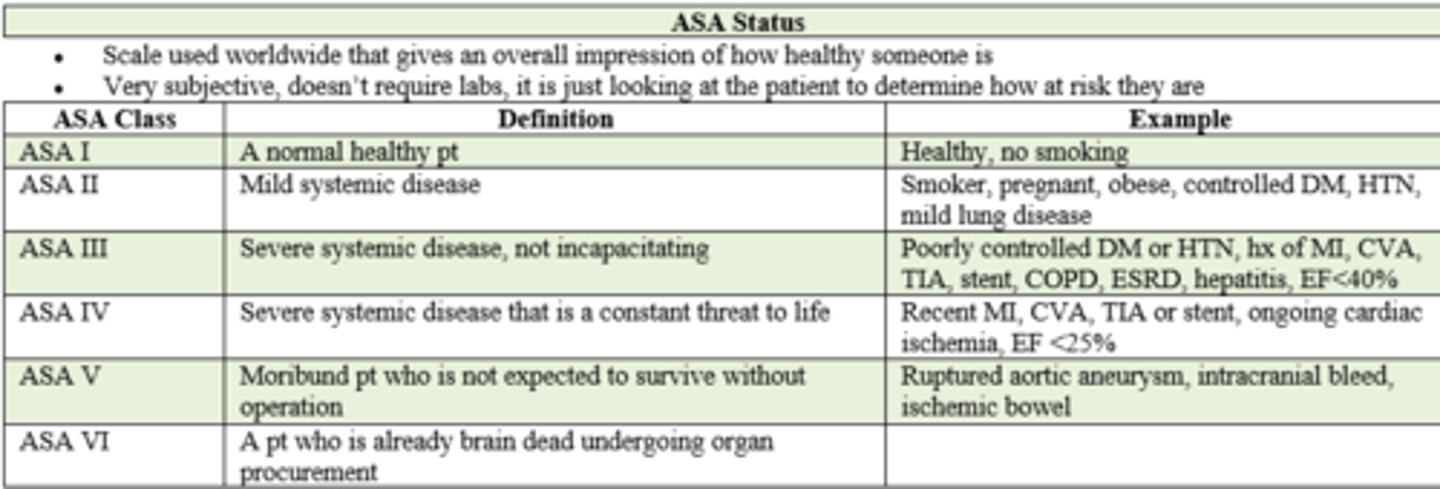
if a pt has had a RECENT MI, CVA, TIA, stent placement and ejection fraction of < 25%, what is their ASA status prior to surgery?
ASA IV / 4
- severe systemic disease
- constant threat to life
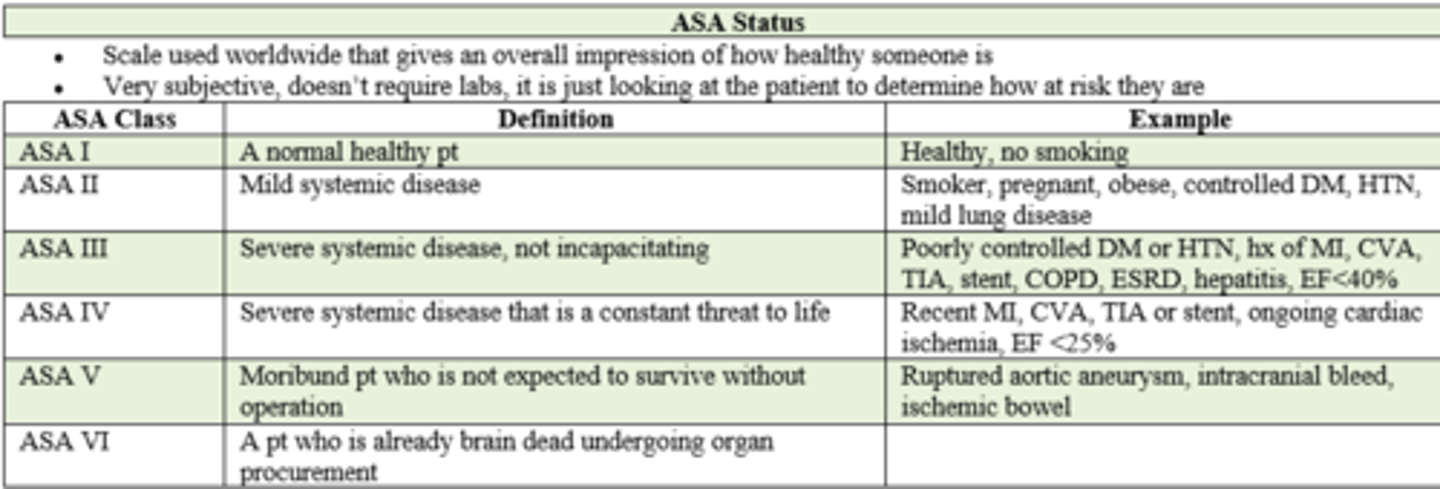
if a pt has a ruptured Aortic Aneurysm, intracranial bleed, or ischemic bowel what is their ASA status prior to surgery?
ASA V / 5
- moribound pt
- will not survive without surgery
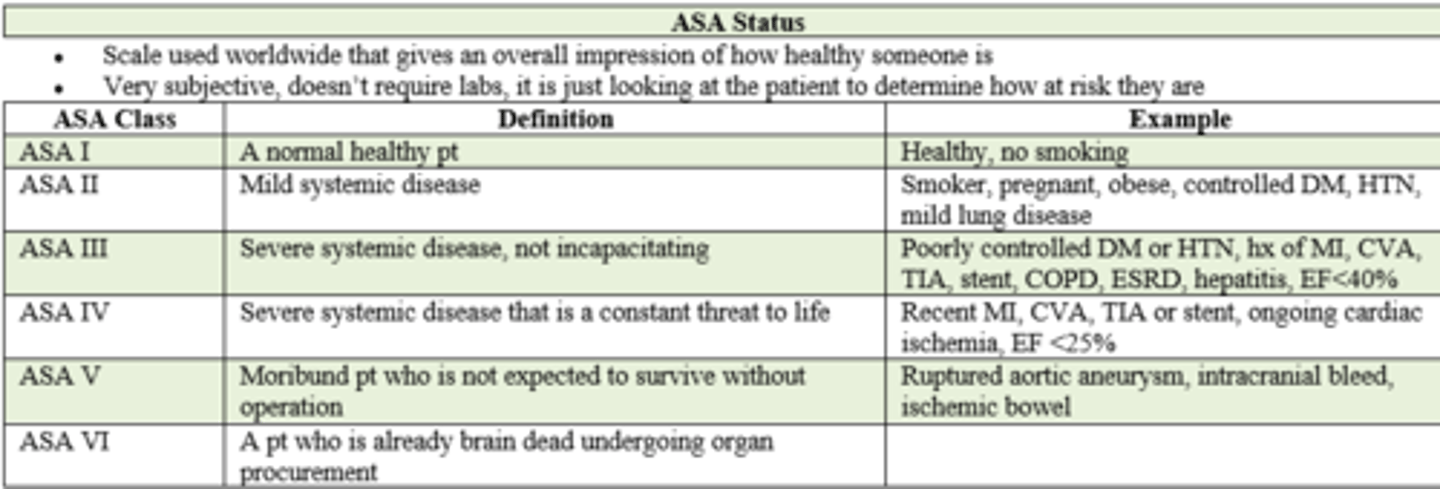
Patient is brain dead and they're about to go undergo operation for organ procurement. What is their ASA class status?
ASA VI / 6
A patient is undergoing NON-emergent / elective surgery and has had a recent MI 5 months ago (10 pts = 7% risk). In order to achieve cardiac "clearance," what pre-op non-invasive ischemia testing is needed?
What do theses tests assess?
- EKG --> rhythm
- Echo --> function
- Stress Test --> perfusion
(FYI Recent MI < 6 months ago = 10 pts = high risk for post-op cardiac complication --> defer/delay surgery until testing complete)
Which type of stress test is the gold standard to assess perfusion of the heart during a cardiac clearance assessment?
Nuclear (radioacho dye + echo during exertion. Ischemic places will not light up - see pic)
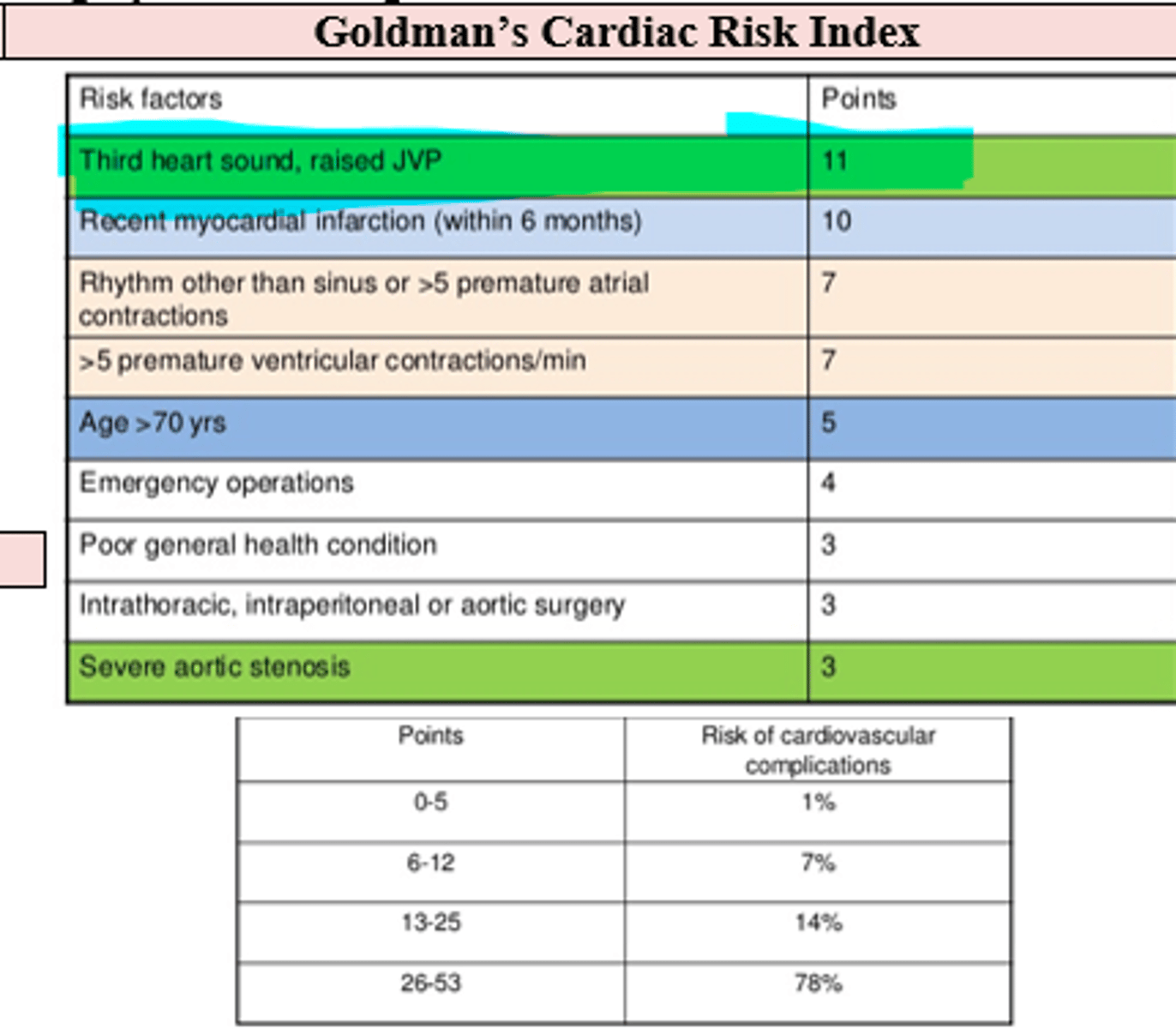
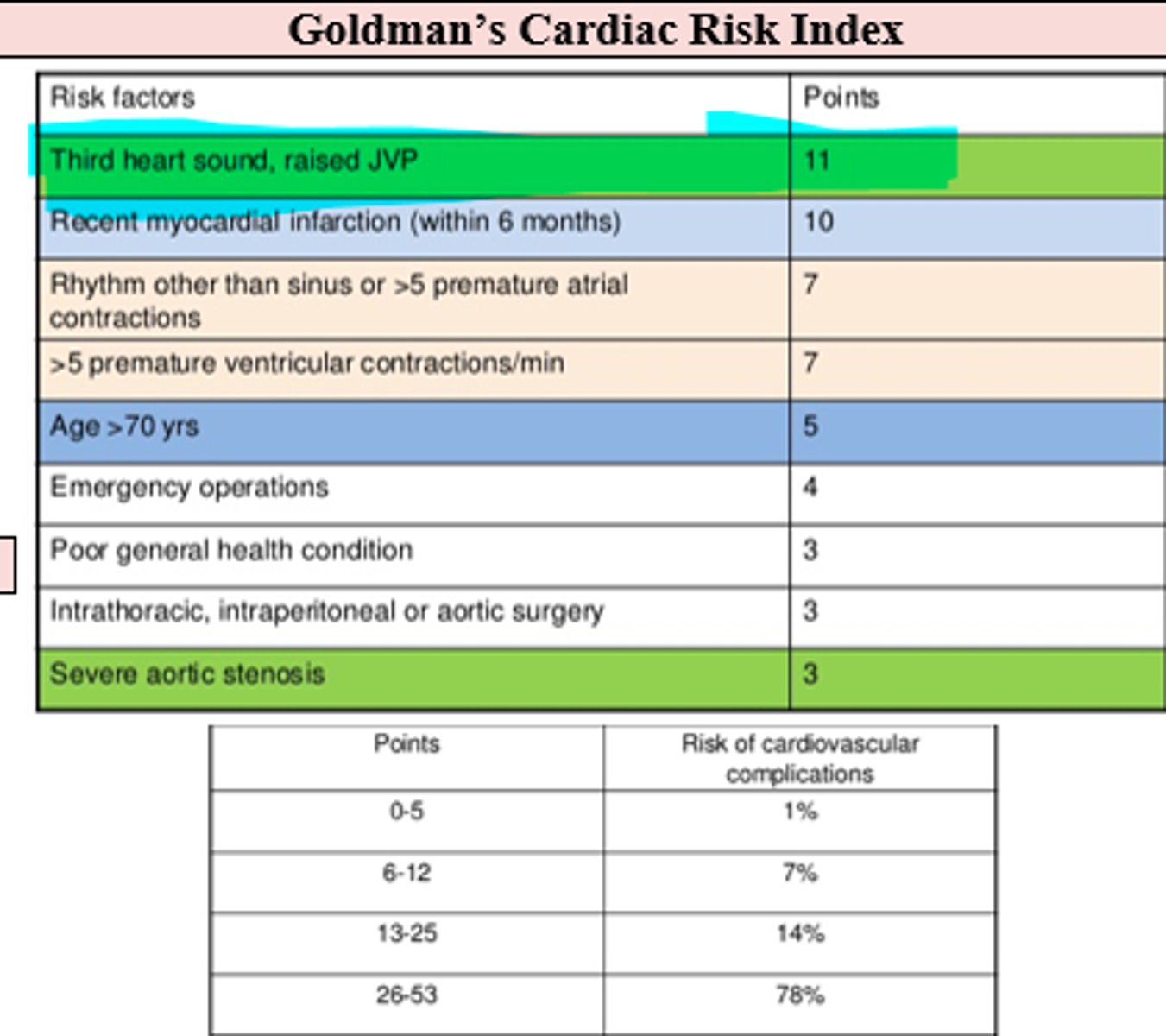
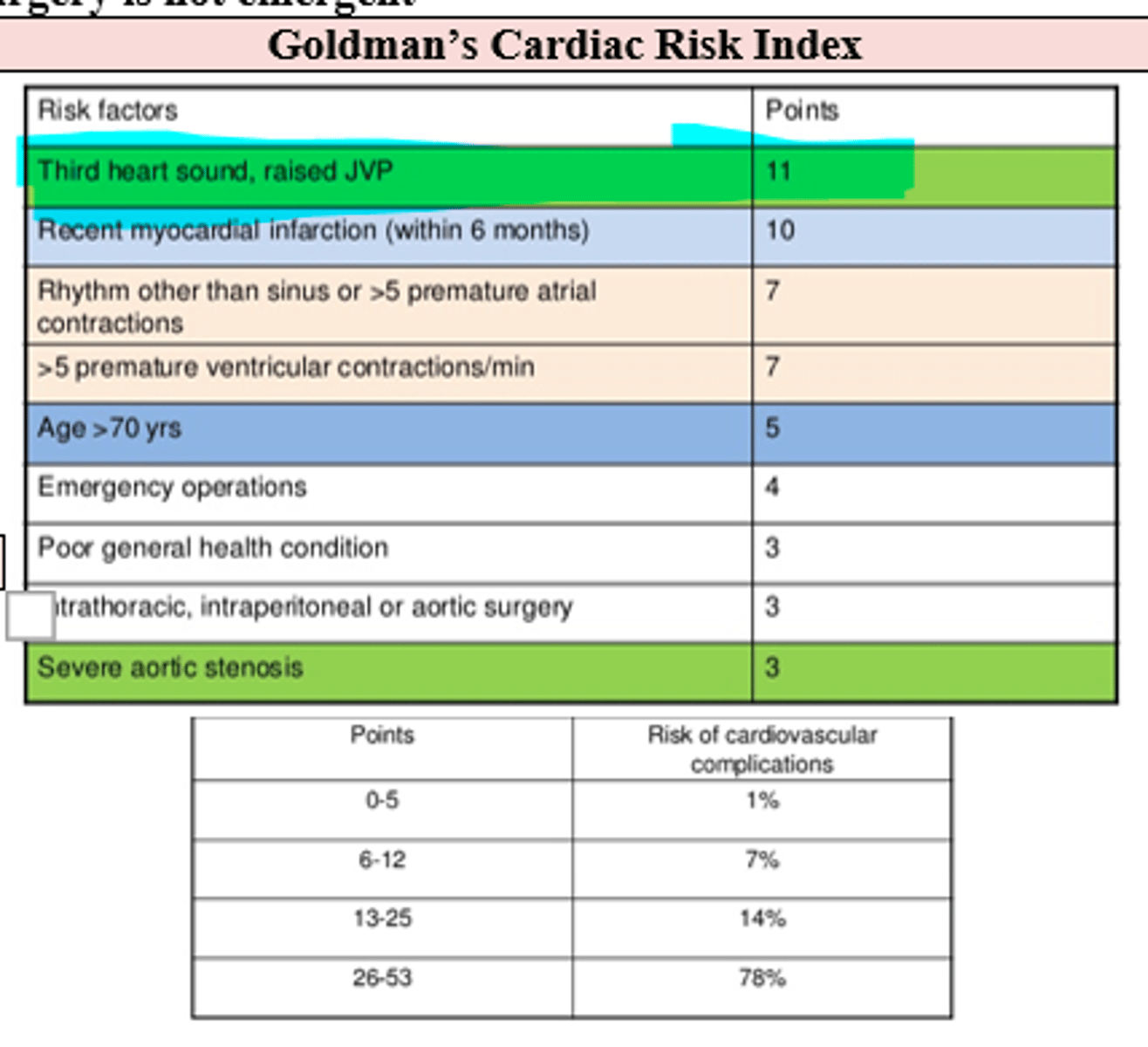
What are the risk factors (Goldman's cardiac risk index) that increase pt's overall surgical CV risk of complication and what are their associated risk points, starting with the highest point risks?
(These help determine if cardiac clearance is necessary, and if surgery can even be done)
- 3rd Heart Sound (sign of HF) = 11 pts
- Raised JVP (sign of HF) = 11 pts
- Recent MI < 6 months ago = 10 pts
- arrhythmia or 5+ PACs = 7 pts
- 5+ PVCs = 7 pts
- 70+ years old = 5 pts
- emergency operations = 4 pts
- poor general health = 3 pts
- intrathoracic, intraperitoneal, or aortic surgery = 3 pts
- severe aortic valve stenosis = 3 pts
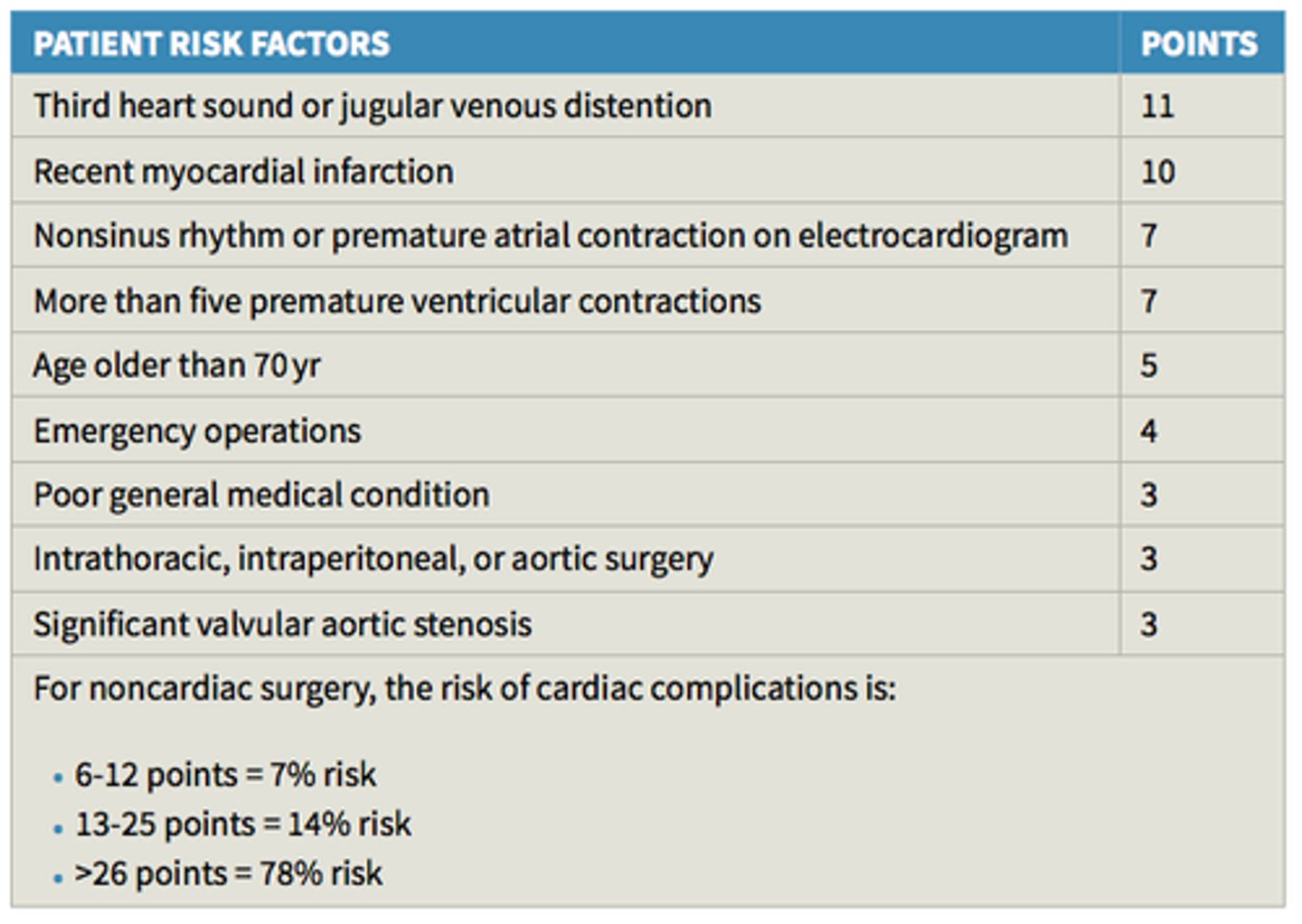
At what Goldman cardiac risk index score should you absolutely NOT perform surgery (unless vital to the pt's survival) given cardiac risks?
26-53 points = 78 % risk
What are some chronic cardiac conditions and procedures in pt's pmhx that requires delay/defer non-emergent / elective surgery until after pre-op cardiac testing (EKG, Echo, Stress test), periop risk assessment, and stabilization of their condition ?
- Stent placement and type (Bare metal vs drug eluting stents)
- Symptomatic arrhythmia
- Pacemaker or Implanted defibrillator (ICD)**
- Artificial/Mechanical heart valves / Valvular Heart Disease
- Heart failure
- Severe HTN (180/110 mmHg)
**let anesthesiologist know, so that intraoperative use of electrocautery doesn't interfere electromagnetically
The most important peri-operative cardiac complications
- Myocardial Infarction (MI)
- Cardiac Death
- Heart failure
- arrhythmias
- unstable angina
The most important post-operative pulmonary complications
- pneumonia
- respiratory failure requiring prolonged mechanical ventilation
- Pulmonary thromboembolism (PE)
What are some surgeries/surgical risk factors that have the greatest post-op risk for pulmonary complications?
- Cardiac surgery
- Intra-Thoracic surgery
- Upper midline Abdominal/peritoneal surgeries (esp if open surgery; laparoscopic is safer)
- Prolonged General anesthesia
(emergency surgery also poses great risk, however will not be delayed either way)
Why is general anesthesia considered one of the surgical risk factors in regards to the pulmonary system ?
- it switches us to (+) pressure ventilation
- Decreases Func. Residual Cap. (FRC) ~11%
- Atelectasis (lung collapse) forms
- Decreases Tidal Volume (TV) post-op
(FYI - Incentive Spirometry needed post-op to help reverse these effects)
What are some patient risk factors / conditions that increase perioperative Pulmonary complication risk, in addition to type and location of surgery, advanced age, physical debility, poor functional capacity, preoperative sepsis, dependency in ADS, and ASA physical status classification?
- smoking
- asthma
- COPD
- HF
- Obesity
- Obstructive Sleep Apnea (OSA)
if pt has a pmhx of smoking, asthma, COPD, Obesity, Obstructive Sleep Apnea (OSA), what should be a part of the pre-op evaluation?
- Auscultate for abnormal breath sounds (rhonchi, rales)
- Exercise tolerance (flight of stairs or walk 2 blocks w/o stopping - functional capacity)
- Pulmonary Function Testing (FEV1 most predictive test)
- ABG on room air to establish baseline (only for those with severe COPD)

What Pulmonary preoperative testing are usually reserved for those with confirmed pulmonary disease and/or showing signs of hypoxemia or hypercapnia, to assess risk of complications prior to major abdominal or cardiothoracic surgery?
- PFTs (FEV1)
- ABG serum testing
What post-operative reduction strategies can be implemented to promote lung expansion /reduce incidence of atelectasis ?
- Incentive Spirometry
- CPAP
- intermittent positive-pressure breathing (IPPB)
- Deep breathing exercises
or "I COUGH" = Incentive spirometry, Coughing and deep breathing, Oral care, Understanding (patient education), Get out of bed (early ambulation), and Head of bed elevation to reduce the rates of pneumonia and unplanned intubation after general and vascular surgery.
Which physical exam findings are consistent with cirrhosis?
- spider angiomata
- caput medusa
- Hepatomegaly
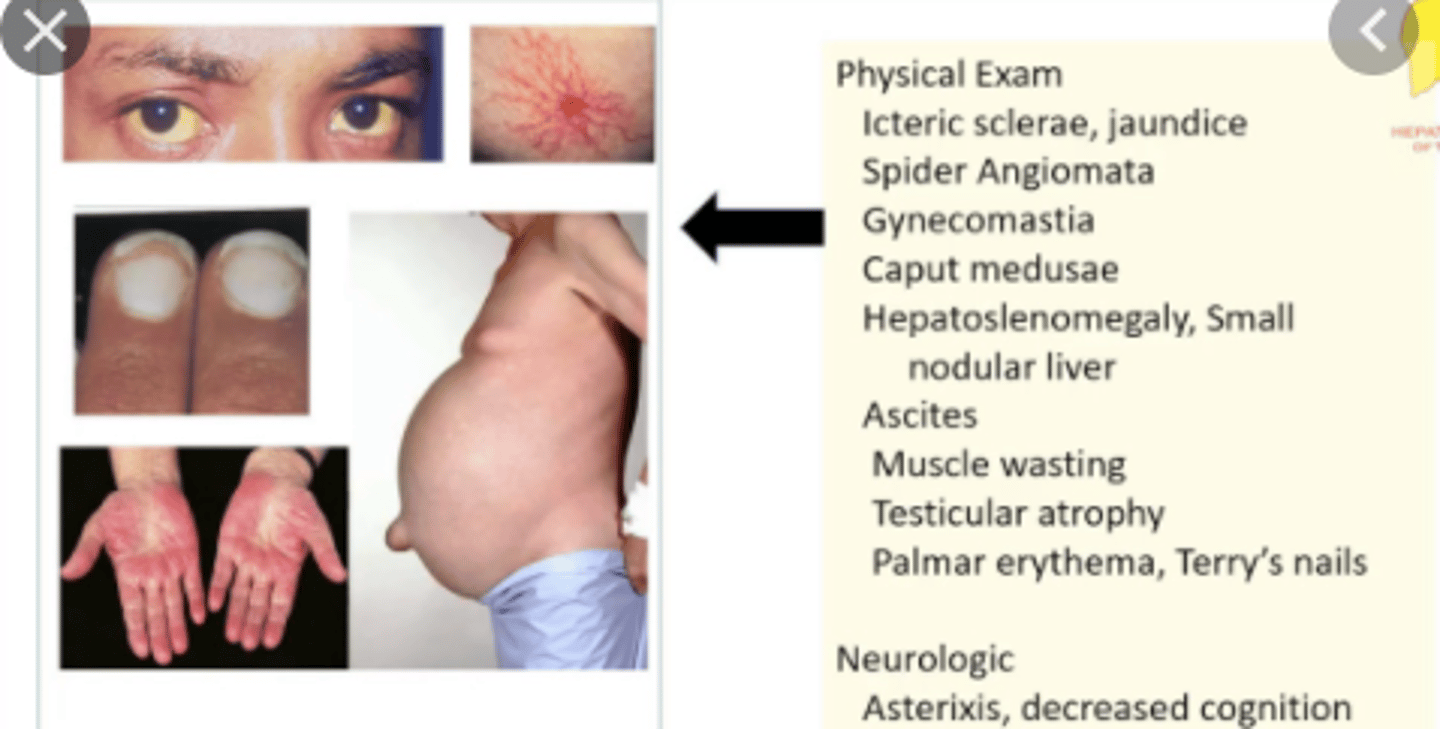
What are some issues / surgical complications in Cirrhotic patients?
- Ascites
- Coagulopathy
- Encephalopathy
- Portal Vein HTN
- Fluid Shifts
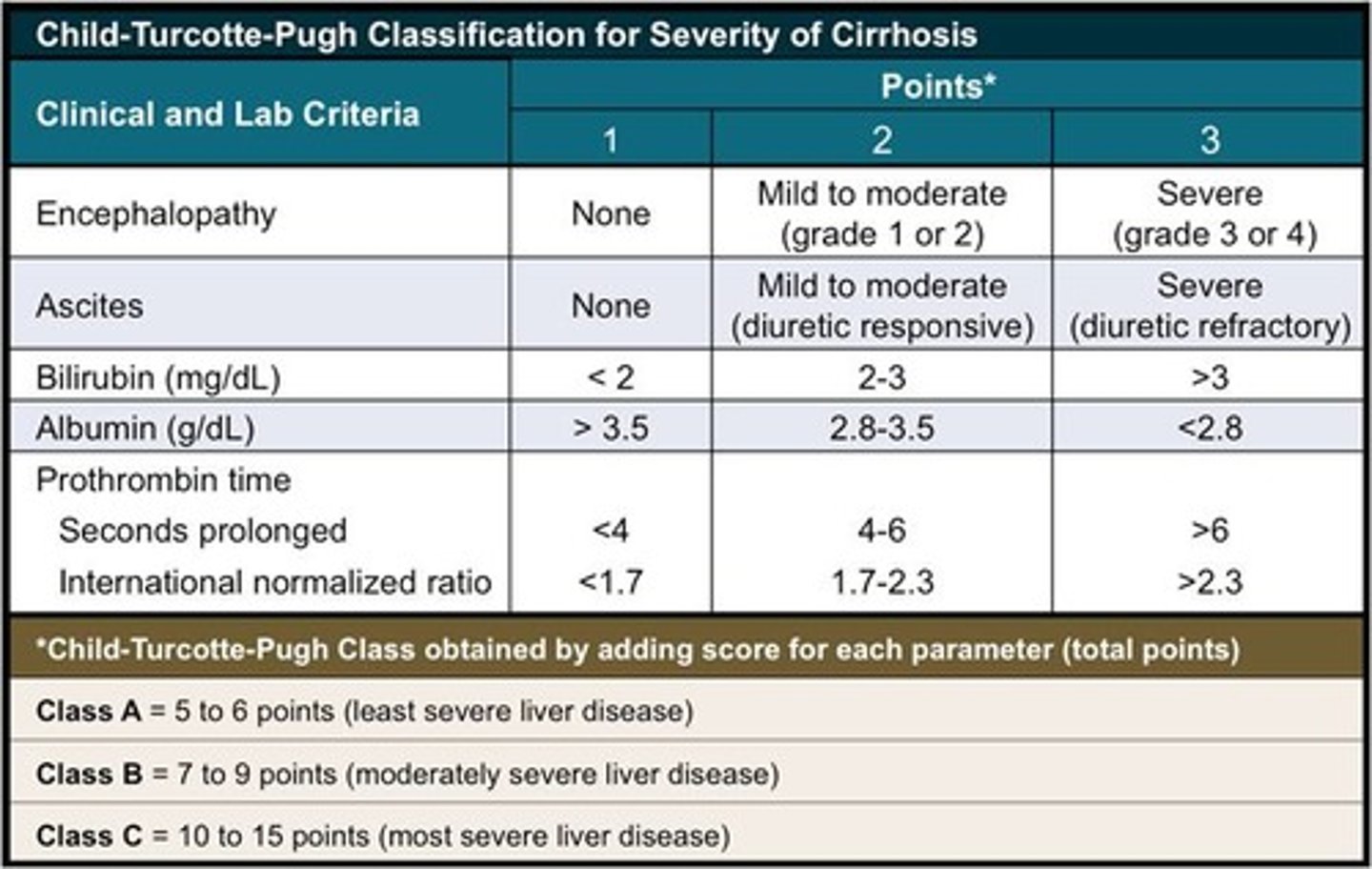
___________ classification system is used to assess severity of Cirrhosis / Liver Disease based on the level or presence of encephalopathy, ascites, bilirubin, albumin, INR.
Child-Turcotte-Pugh
(Class C = 10-15 pts, most severe --> 80% risk and therefore rarely operated on unless life or death)
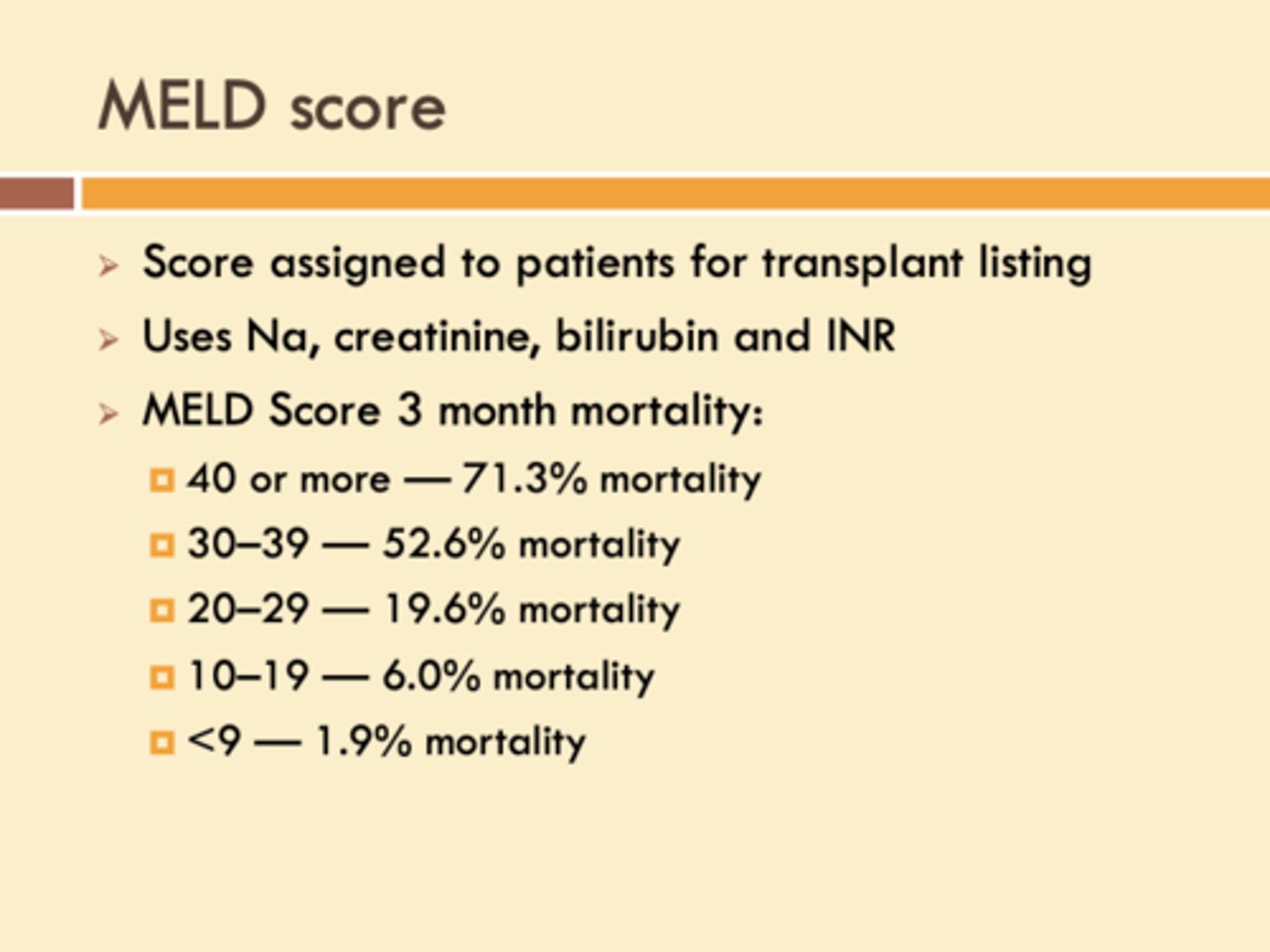
_____________ score looks at creatinine levels, recent dialysis, bilirubin, INR, and Sodium (Na) levels to determine 3 month patient mortality % in a patient with Liver Disease / Cirrhosis.
Model for End stage Liver Disease (MELD)
What are some Kidney / Renal Concerns to consider during pre-op surgical evaluation ?
- electrolyte abnormalities (esp. HyperKalemic, Metabolic Acidosis)
- Fluid balance
- Vascular access (h/o fistulas and dialysis can make it difficult to establish IV access or check BP)
Why should you always implement NPO (neil per os = no food or drink) if suspecting an impending URGENT surgery?
(FYI - not emergent, bc this is done regardless of NPO status)?
- reduce risk of aspiration during surgery
- surgery can occur ASAP
When should you tell your pre-op pt undergoing surgery to stop clear liquids? milk products /light meals? heavy meals?
2 hours prior to procedure
6 hours "
8 hours "
(FYI - This doesn't apply to emergency surgery)
When obtaining consent prior to a non-emergent procedure but your patient is not competent to give it you, what is the order of who you should contact instead?
1. Spouse (even if estranged)
2. Adult Children
3. Parent
4. Sibling
What are the risks you must go over with your patient prior to non-emergent surgery in order to obtain informed consent?
- Bleeding
- Infection
- Injury to other structures
- Surgery specific risks
- Need for additional operations
- Anesthesia (MI/Stroke/PE/Death)
***must document specifics***
What type of anesthesia is good for extremity procedures bc they're selective and with low risk?
Local / Regional
(ex: Spinal/Epidural)
What type of anesthesia is good for day surgeries that are less invasive, such as colonoscopies ?
Moderate Sedation / MAC
(ex: Propofol, Ketamine)
What type of serum test will you order pre-operatively when transfusion of blood products is unlikely ,but possible ?
Type and Screen
(ABO/RH blood Type and Antibody Screen - blood products will not be held for patient)
What type of serum test will you order pre-operatively when there's a high risk of transfusion of blood products in a pt who has had a h/o multiple transfusions / antibodies?
Type and Cross
(ABO/RH blood Type and Antibody Cross
- pt's blood mixed with donated blood
- on hold for pt only)
What are some common post-op complications ?
- Hypotension
- Fever (>101.5 F)
- SOB
- Altered Mental Status (AMS)
What is the difference between the definition clinical fever in medicine and a post op fever?
- in clinical medicine = 100.4 F
- in s/p pt's = 101.5 F
Your post-op patient is currently experiencing Hypotension.
What is on your DDX and what should the work up include?
- Hypovolemia
- Medications
- Hemorrhage
- Septic Shock
- Anesthesia (diagnosis of exclusion)
Work up:
- Vitals
- Labs (CBC for Hgb/Hct, Cardiac enzymes)
- Medication Reconciliation
- EKG
Your post-op day 1 (POD 1) patient is currently experiencing Fever of +101.5F, what is on your DDX of what is causing this ?
- Atelectasis (complete or partial collapsed lung)
- Systemic inflammatory response syndrome (SIRS; will also be tachycardic, tachypneic, and elevated WBC)
Your post-op day 3-5 (POD 3-5) patient is currently experiencing Fever of +101.5F, what is on your DDX of what is causing this ?
iatrogenic causes (UTI, pneumonia/ HAP, Wound infection)
Your post-op day 6-7 (POD 6-7) patient is currently experiencing persistent Fever of +101.5F, what is on your DDX of what is causing this ?
Surgical site infection (get CT to look for abscess or infection)
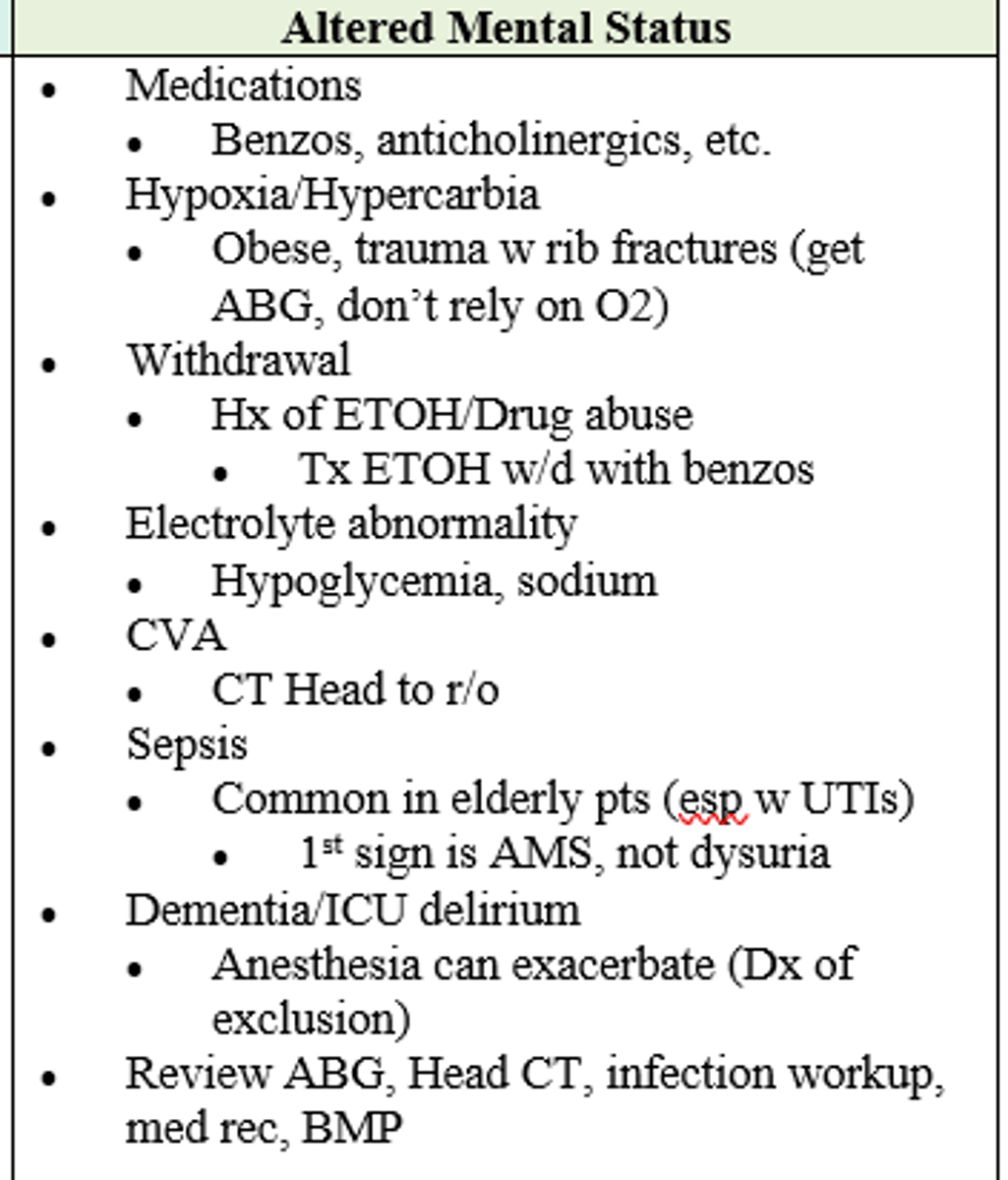
Post-op patient is currently experiencing AMS.
What is on your differential and what should work up include?
Ddx:
- Medications
- Hypoxia/ Hypercarbia
- Withdrawal (i.e. ETOH)
- Electrolyte Abnormality
- CVA
- Sepsis
- Dementia (exacerbated by surgical stress)
- ICU Delirium
Work up:
-Labs (ABG for o2/co2, BMP)
- Infection work-up
- Imaging (Head CT)
- Med reconciliation
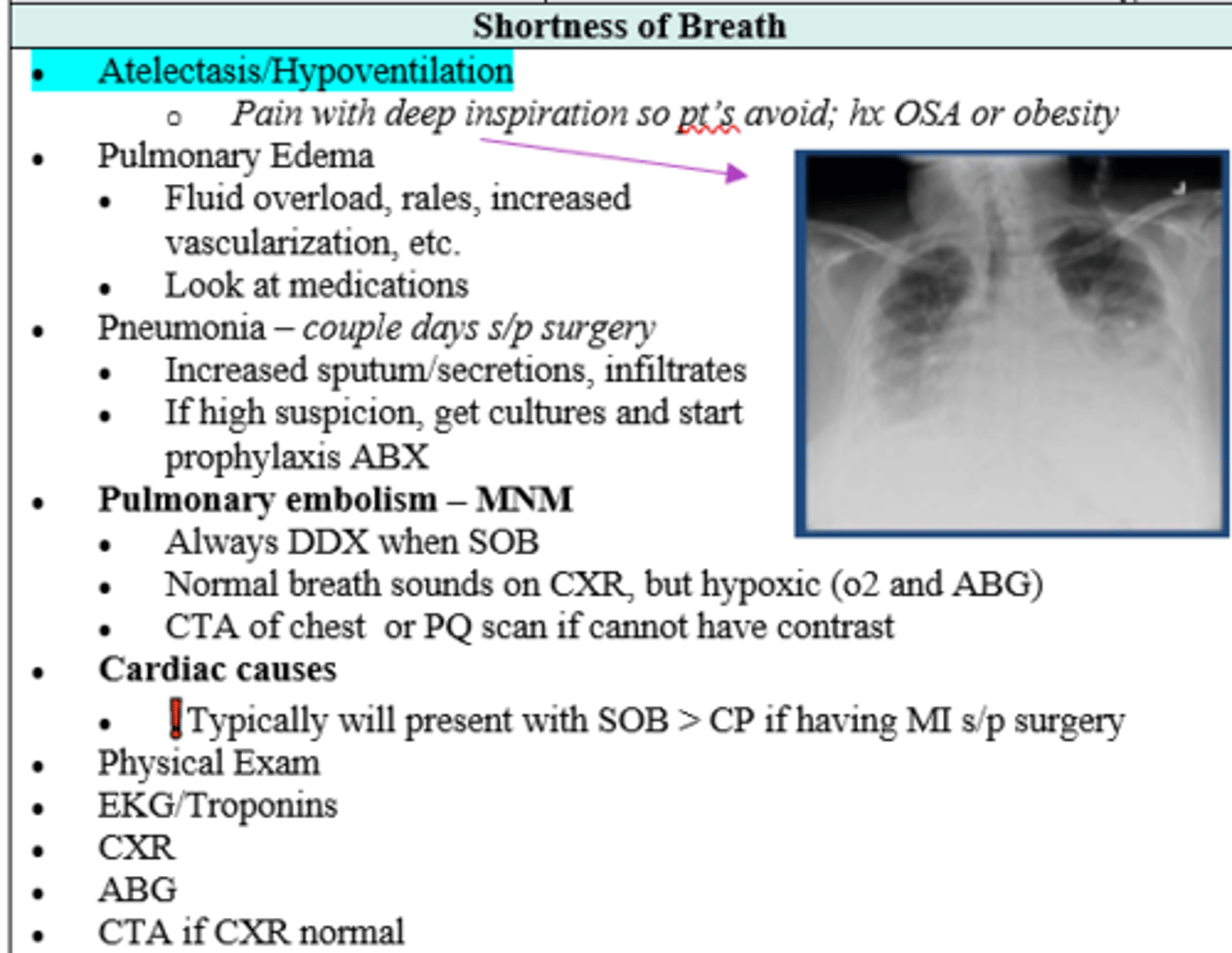
Your post-op patient is currently experiencing SOB.
What is on your differential and what should work up include?
Ddx:
- Atelectasis / Hypoventilation (collapsed lung)
- Pulmonary Edema
- Pneumonia
- Pulmonary Embolism - most concerning)
- Cardiac causes (i..e Afib, MI)
Work up:
PE
Labs (Cardiac enzymes/ troponins, ABG for o2 & co2)
EKG
Imaging (CXR and CTA if CXR normal and high suspicion for PE)
What needs to be included on your Post-op orders?
1. Level of admission (standard/floor vs. step down vs. ICU)
2. Diet (NPO vs clear fluids only vs. normal)
3. IV fluid needs
4. Med orders (which to hold or restart, and RX for pain, nausea, and/or ABX)
5. Monitoring (vitals, UOP, Labs)
6. Wound care
7. Activity (WB vs NWB)
8. DVT prophylaxis needed ?
What should be checked 4-6 hours post-op ?
- pain control
- nausea
- vital signs
- urine output (UOP)
- wound bed drain output
At which point during surgery is the risk for perioperative MI at its highest?
First few minutes of introducing anesthesia (dt massive vasoplegia/ vasodilation which drops both preload and afterload)
Inflammation/Healing puts body in (anabolic/catabolic) state
Catabolic (body puts all its energy into healing; weight loss common in first few months)
What is the implication of holding beta-blockers for surgery in a patient already prescribed them?
Significantly increases risk for stroke, MI, and death
A patient who is rx'd Clonidine must continue to take it via skin patch prior to surgery. What is the reason for this?
Rebound HTN and tachycardia can result if held
Patient with history of Afib needs surgery. He takes anticoagulants due to his Afib, but has no other PMHx. What should be done?
Stop anticoagulants 5 days before surgery (low risk patient)
Which of the following patients require cardiac consult prior to surgery given their extremely high risk of holding anticoagulation?
A. Hx of DVT or PE
B. Hx of Afib
C. Mechanical Heart Valve/ LVAD
D. Stent & Antiplatelet use
C & D (stent & AP use; Mechanical Heart Valve and LVAD pts are HIGHEST risk)
Your patient has DM2 and regularly takes metformin and daily vitamins. She needs CT with contrast. How do you proceed?
Hold metformin (pts w chance of CT scan cannot have metformin & contrast within 72h dt risk lactic acidosis)
You have a patient at risk of poor healing from surgery given evidence of malnutrition. What can be evaluated to give a glimpse of last 3 months of nutritional status?
Albumin
Patient had an MI 7 months ago and is needed to undergo a surgery. What is their risk (%) of having another MI during surgery?
5% (Recent MI within 3 mos = 30% risk with gradual decline that plateaus at 5% after 6 months)
Why would you perform cardiac evaluation tests?
If testing will change mgmt or if surgery is non emergent
Which Goldman's Cardiac Risk Index factors score the highest points?
Third heart sound and raised JVP (11pts; evidence of Congestive Heart Failure)
What pulmonary risks does a pt with OSA have during or after surgery?
Hypoventilation syndrome, hypercarbia respiratory failure
Which FEV1 indicates a significant pulmonary risk in which a patient will be unable to be extubated s/p surgery?
<0.8 (FEV1 is the most predictive PFT)
What is the risk for a compensated cirrhotic patient when undergoing any surgery, even minor?
Transformation into decompensated cirrhosis (encephalopathy -> increased confusion -> cerebral edema -> death)
What is the risk of performing surgery on a pt with ascites?
Fluid leaking from surgical wound can cause dehiscence, risk of hernias and spontaneous peritonitis
Patient with cirrhosis becomes rapidly hypotensive when ascites is drained. What is the mechanism behind their HoTN?
Fluid Shifts
In true emergencies, what consent is surgery performed under?
Presumed Consent (two providers document surgery is required)
Which pts should receive DVT prophylaxis as post-op orders?
ALL patients
After surgery, how often should patient be urinating?
every 6 hours (concern for urinary retention if less than this, mc in men)
1 day after open abdominal surgery, patient develops fever over 101.5. Their HR is 130 and RR 26. Labs reveal WBC of 17,000. Likely dx?
SIRS (Systemic Inflammatory Response Syndrome)
Which MNM diagnoses must be ruled out when pt has hypotension s/p surgery?
MI, Bleeding, Sepsis
6-7 days after surgery patient develops fever of >101.5, but you see no outward signs of infection. How do you proceed?
CT (look for surgical site abscess)
What is the mc symptom of a post-op patient presenting with MI?
SOB
After surgery, patient becomes SOB and hypoxic, both on pulse ox and ABG. Their breath sounds are normal. Top ddx and how do you rule out?
Pulmonary Embolism (CTA of chest or PQ scan if cannot have contrast)
After surgery, Obese pt with PMHx of OSA has pain with deep inspiration and is avoiding breathing. CXR shows diffusely white consolidation and areas of white lines b/l in middle and lower lobes. Dx?
Atelectasis/ Hypoventilation

A few days s/p surgery patient has increased sputum & secretions. CXR shows infiltrates in lungs. Dx and labs?
Pneumonia; get sputum cultures and start prophylaxis abx
Older patient develops altered mental status a few days after surgery. What is a common cause of sepsis in older patients that could be causing AMS?
UTI (1st sign AMS, not dysuria)