Toddler and Preschooler Nutrition
1/125
Earn XP
Description and Tags
Information from Judith E. Brown - Nutrition Through the Life Cycle-Cengage (2018)
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
126 Terms
Age Range For Toddlers
1 to 3 years
Age Range For Preschool Age
3 to 5 years
What % of toddlers and preschoolers live in poor and near poor families?
44%
What % of toddlers and preschoolers under the age of 6 in a family with a female householder were in poverty>
49.1%
Healthy People 2020 Objective: Increase Fruit
Baseline: 0.5 cup equivalents of fruits per 1000 calories
Target: 0.9 cup equivalents of fruits per 1000 calories
Healthy People 2020 Objective: Increase Veggies
Baseline: 0.8 cup equivalents of total vegetables per 1000 calories
Target: 1.1 cup equivalents per 1000 calories
Healthy People 2020 Objective: Increase Dark Green Veggies
Baseline: 0.1 cup equivalents of dark green or orange vegetables or legumes per 1000 calories
Target: 0.3 cup equivalents per 1000 calories
Healthy People 2020 Objective: Increase Whole Grain
Baseline: 0.3 oz equivalents of whole grains per 1000 calories
Target: 0.6 oz equivalents per 1000 calories
Healthy People 2020 Objective: Reduce Solid Fats
Baseline: 18.9% of total daily calorie intake
Target: 16.7%
Healthy People 2020 Objective: Reduce Added Sugars
Baseline: 15.7% of total daily calorie intake
Target: 10.8%
Healthy People 2020 Objective: Reduce Solid Fats and Added Sugars
Baseline: 34.6% of total daily calorie intake
Target: 29.8%
Healthy People 2020 Objective: Reduce Saturated Fat
Baseline: 11.3% of total daily calorie intake
Target: 9.5%
Healthy People 2020 Objective: Reduce Sodium
Baseline: 3641 mg
Target: 2300 mg
Healthy People 2020 Objective: Increase Calcium
Baseline: 1118 mg
Target: 1300 mg
Average gain in Toddler per month
8 oz (6 lb a year) and grow 0.4 inches (4.8 inches a year)
Average gain in preschoolers per month
4.4 lb a year and grow 2.75 inches per year
Measuring Growth
The length of toddlers <2 years of age is measured in the recumbent position

Body mass index (BMI) for age (kg/m2)
• <5th percentile indicated underweight
• Between 85th-95th percentile indicated overweight
• ≥95th percentile indicated obesity
severe obesity = BMI ≧120% of the 95th percentile for age and sex
Expanding physical and developmental skills of toddlers
15 months: crawls upstairs
18 months: runs stiffly
24 months: walks up stairs one foot at a time and jumps in place
30 months: alternates feet going up stairs
36 months: rides a tricycle
Development of feeding skills of toddlers
Nine to ten months: bottle weaning
12 to 14 months: completely weaned
12 months: refined pincer grasp
Pincer grasp wherein the pointer finger and the thumb squeeze to grasp an object.[
18-24 months: able to use tongue to clean lips and has well-developed rotary chewing
Adult supervision vital to prevent choking
Toddler-sized portions average
one tablespoon per year of age
Feeding Behaviors of Toddlers
Rituals in feeding are common
May have strong preferences and dislikes
Food jags common
A food jag is defined as "when children prefer to eat the same food prepared the same way every day or at every meal."
Serve new foods with familiar foods
Toddlers imitate the eating behavior of others
Cognitive development of preschoolers
Magical thinking and egocentrism
Egocentrism - the inability to differentiate between self and other
Learning to set limits for himself
Beginning of cooperative and organized play
Expansion of vocabulary to over 2000 words
Begins using complete sentences
Development of feeding skills of preschoolers
Can use a fork, spoon, and cup
Eating becomes less messy
Spills occur less frequently
Foods should be cut into bite-size pieces
Adult supervision is imperative
Feeding behaviors of preschoolers
Appetite is related to growth; increases prior to the “spurts”
Involve child in meal selection and preparation
Appetite and Food Intake of Preschoolers
May prefer familiar foods - comfort or control?
Serve child-sized portions
Make foods attractive
Strong-flavored or spicy foods may not be accepted
Control amount eaten between meals
Young children often do not like their foods to touch or to be mixed together
Temperament Differences
“Easy”—adapts to regular schedules & accepts new foods
“Difficult”—slow to adapt and may be negative to new foods
“Slow-to-warm-up”—slow adaptability, negative to new foods but can learn to accept new foods
“Intermediate low” to “intermediate high” – a mixture of behaviors
How many exposure to new food until it is accepted?
8 to 10 exposures
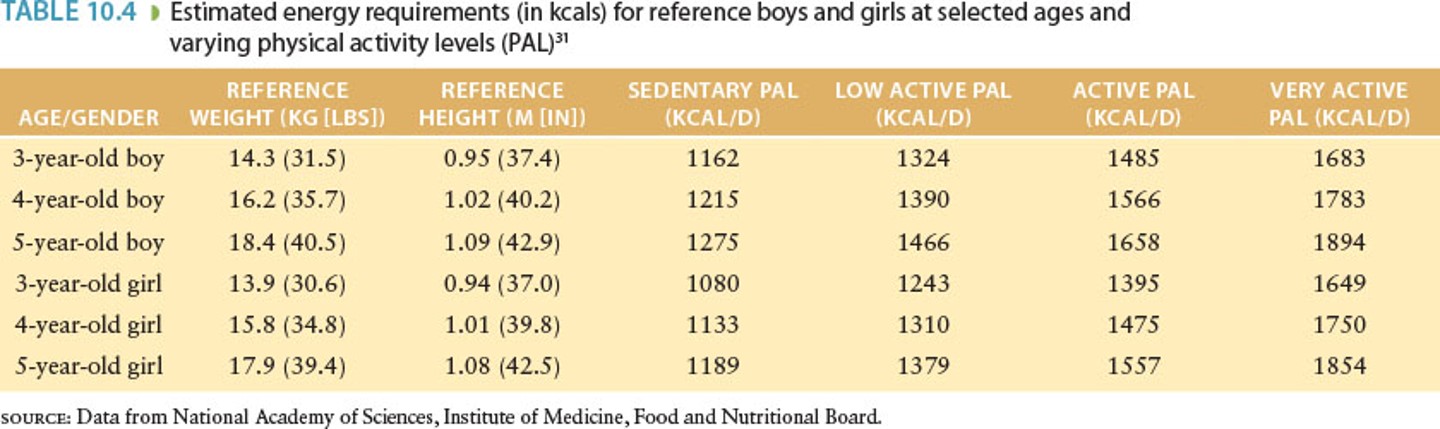
EERs in kcal
DRI for Protein

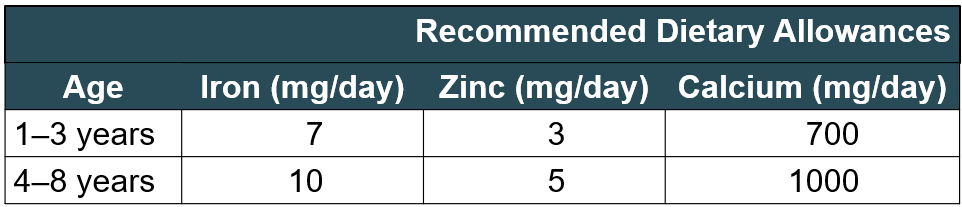
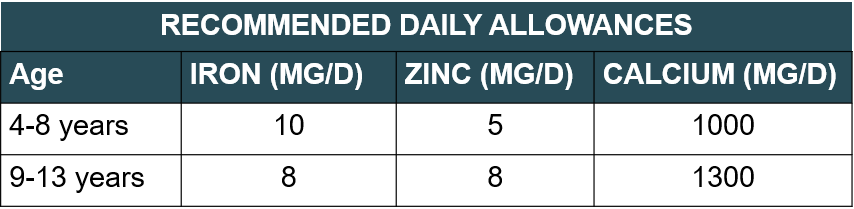
DRI for Iron, Zinc, and Calcium
Common Nutrient Problems
Iron-deficiency anemia
Dental caries
Constipation
Elevated blood lead levels
Food security
Food safety
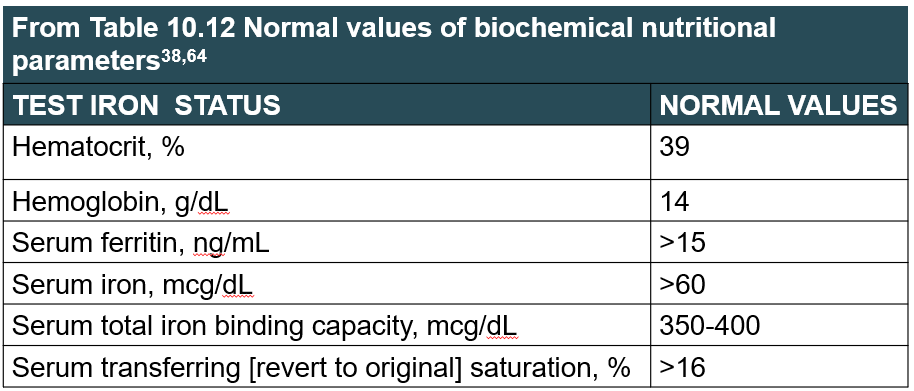
Normal values of biochemical nutritional parameters
How to prevent Iron deficiency
Limit milk consumption to 24 ounces a day
Low-iron and may displace high-iron foods in the diet
Infants at risk should be tested at nine to 12 months, six months later, and annually from ages two to five
Nutrition intervention
Iron supplements
Counseling with parents on proper dietary iron intake
Lean meat/fish/poultry with Vitamin C-containing foods
Repeat screening
Pica
Eating disorder characterized by persistent consumption of non-nutritive substances (e.g. dirt, hair, paper).
Dental Carries
Prevalence: one in three children ages three to five
Causes: bedtime bottle with juice or milk, Streptococcus mutans, and sticky carbohydrate foods
Prevention
Fluoride
Supplemental amounts vary by age and fluoride content of water supply
Excessive fluoride supplementation or water content can cause fluorosis
Streptococcus mutans
Bacterium responsible for dental cavities and tooth decay. Uses carbohydrates for food
Constipation
Definition: hard and dry stools associated with painful bowel movements
Causes: “stool holding” and diet
Prevention: adequate fiber and fluid
Table 10.10 on pg 276: 1-3 years 19g/day; 4-8 years 25g/day
Sources: whole grain bread/cereals, legumes, fruits, and vegetables (age appropriate)
Excess fiber can lead to diarrhea, displace other energy-dense foods, and decrease bioavailability of iron & calcium

Food Security
Access at all times to sufficient supply of safe, nutritious foods
Fight-BAC food safety practices
Clean: wash hands and surfaces often
Separate: don’t cross-contaminate
Cook: cook to proper temperatures
Chill: refrigerate promptly
Key foodborne pathogens
Campylobacter (raw poultry, raw milk), salmonella (raw or undercooked eggs such as in raw cookie dough), E coli (undercooked beef, unpasteurized apple cider and juice, unpasteurized milk)
Adiposity (BMI) rebound
normal increase in BMI that occurs after BMI declines
Prevention of overweight and obesity (pg. 269-270)
Limit sugar-sweet beverages
Encourage fruits and vegetables
Limit television and screen time (max 2 hrs/day)
Eat a daily breakfast
Limit restaurants and fast foods
Limit portions
Diet that is high fiber, calcium-rich, and follows DRI for macronutrients
Moderate to vigorous physical activity for at least 60 min/day
Limit energy dense Foods
Treatment of overweight and obesity expert committee: Recommendations
Stage one: prevention plus
focuses on the behaviors identified in the prevention section
Stage two: structured weight management (SWM)
Daily eating plan, further reduction of screen time, supervised physical activity/play for 60 min/day, meet with RD
more structured and requires more frequent follow-up
Stage three: comprehensive multidisciplinary intervention
Food monitoring, negative energy balance, physical activity goals, evaluations at specific intervals
the intensity of behavior change is increased and a multidisciplinary team, including an RD, exercise specialist, behavioral counselor, and PCP is needed; weekly visits are recommended
Stage four: tertiary care intervention
offered to severely obese adolescents who have failed other interventions; NOT appropriate for the obese toddler or preschool-age child
Nutrition and prevention of cardiovascular disease in toddlers and preschoolers
Limit dietary saturated fats, trans fat, and cholesterol
Avoid smoking, encourage daily physical activity, and reduce sedentary time, sugar-sweetened beverages, and salt
Diet including fruits, vegetables, whole grains, non or lowfat dairy, and fish two times per week
Acceptable macronutrient distribution ranges for fat
Two to three years: 30 to 35%
Four to 18 years: 25 to 35%
Recommendations for intake of iron
Important to prevent iron deficiency
meats, fortified cereal, dried beans, and peas
less than 24oz milk daily
Recommendations for intake of fiber
Important for prevention of constipation
fruits, vegetables, and whole grains (see slide 45)
Recommendations for intake of fat
Follow Dietary Guidelines and MyPlate
needed for fat-soluble vitamins and essential fatty acids
Recommendations for intake of calcium
Important for achieving peak bone mass
dairy, canned fish with soft bones, green leafy vegetables, calcium-fortified beverages, and tofu made with calcium
1-3yrs = 700mg/day
4-8yrs = 1000mg/day
Calcium is low in general population and for children with special needs
Recommendations for intake of fluids
Consumed through beverages, foods, and sips of water
Requirements increase with fever, vomiting, diarrhea, and hot/dry/humid environments
AAP recommends limiting juice to 4-6 oz. per day.
Children on Vegetarian Diets
Children with vegan and macrobiotic diets tend to have lower growth rates but remain within normal ranges.
Amounts required to meet nutrient needs may be more than children can physically eat
Vitamin B12 and/or calcium supplements likely needed
Vegetarian diet guidelines (on pg 278)
Provide three meals and two to three snacks per day
Avoid excessive bulky foods (e.g., bran)
Include energy dense foods (e.g., cheese)
Provide an omega-3 fatty acid source (e.g., tofu)
Ensure an adequate intake of calcium, zinc, iron, and vitamins B12 and D
What % of children with disabilities have a nutrition problem?
90%
Eligibility for early intervention services
< 3 years
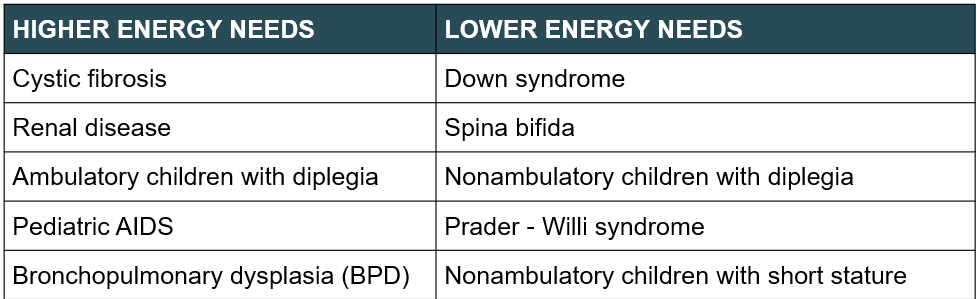
Chronic conditions generally associated with high and low energy needs
Diplegia
A type of paralysis that affects symmetrical body parts, such as both legs or both arms. It is typically caused by damage to the brain or spinal cord, resulting in muscle weakness or loss of control in the affected areas.
Prader-Willi Syndrome (PWS)
Genetic disorder causing insatiable appetite, obesity, intellectual disabilities, and low muscle tone. Also presents with short stature, hypogonadism, and behavioral issues.
Lower calories needed by children with slow growth or decreased muscles. Opposite for ADHD or ASD
Rett syndrome
Rett syndrome: A rare genetic disorder that affects brain development, primarily in girls. It leads to severe cognitive and physical impairments, including loss of purposeful hand skills, impaired speech, and repetitive hand movements. Symptoms usually appear between 6 and 18 months of age.
Feeding Problems
Low interest in eating
Long mealtimes (>30 minutes)
Preferring liquids over solids
Food refusals
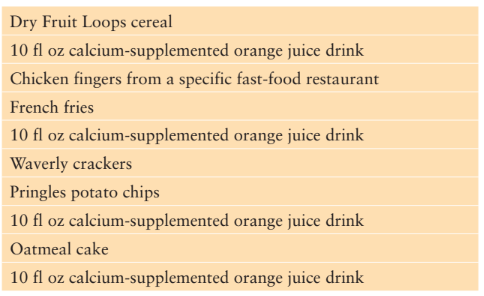
Example of food choices for child with suspected developmental delay
Feeding problems w/ autism
Limited Food Selection/Strong Food Dislikes. Someone with autism may be sensitive to the taste, smell, color and/or texture foods. They may limit or totally avoid some foods and even whole groups of foods. Common dislikes include fruits, vegetables and slippery, soft foods.
Not Eating Enough Food. Kids with autism may have difficulty focusing on one task for an extended period of time. It may be hard for a child to sit down and eat a meal from start to finish. The gluten free/casein free diet has not been found to be effective. However, some people report relief in symptoms after following a GFCF diet.
Feeding problems w/ adhd
ADHD is a problem with inattentiveness, over-activity, impulsivity, or a combination. For these problems to be diagnosed as ADHD, they must be out of the normal range for a child's age and development. ADHD is a brain disorder caused by faulty connections between nerve cells that regulate attention. Diet alone probably isn't the driving force behind the multiple behavioral and cognitive symptoms that plague children with attention deficit hyperactivity disorder (ADHD). But several studies have renewed interest in whether certain foods and additives might affect particular symptoms in a subset of children with ADHD.
Diets for autism
No specific diet is recommended for prevention or treatment
Gluten-free and casein-free diets have been used by parents but not endorsed by professional societies
Excessive fluid intake
child would rather drink than eat
AAP recommendation for juice
4-6 fl oz/day for ages 1-6 years applies to ALL children
Pediatric Malnutrition - Formerly Failure to thrive (FTT)
Child’s weight for age falls below 5th percentile on multiple occasions or declines to cross two or more growth percentiles lines on growth chart
Toddler Diarrhea
Typically caused by sucrose and sorbitol content of fruit juices
Limiting juice may be recommended
Celiac Disease
An autoimmune disorder affecting the small intestine due to gluten intolerance. It causes damage to the lining of the intestine, leading to malabsorption of nutrients. Symptoms include abdominal pain, diarrhea, weight loss, and fatigue. Treatment involves a strict gluten-free diet to manage symptoms and prevent complications.
Cerebral Palsy
Condition affecting movement and muscle control. Results from damage to the brain before or during birth, or in early childhood. Can cause difficulties with coordination, balance, and muscle strength. May also impact speech and fine motor skills. Treatment focuses on therapy, medication, and assistive devices to improve function and quality of life.
Spastic quadriplegia
severe cerebral palsy
compared to quadriplegia, spastic quadriplegia is defined by spasticity of the limbs as opposed to strict paralysis. It is distinguishable from other forms of cerebral palsy in that those afflicted with the condition display stiff, jerky movements stemming from hypertonia of the muscles. Spastic quadriplegia is generally caused by brain damage or disruptions in normal brain development preceding birth.
No two individuals with cerebral palsy are alike; some individuals may be hypometabolic as a result of hypotonia, while others may be hypermetabolic related to increased muscle tone.
brochopulmonary dysplasia (BPD)
A chronic lung disease that affects premature infants. It occurs due to damage to the lungs from mechanical ventilation and oxygen therapy. Symptoms include difficulty breathing, wheezing, nd increased risk of respiratory infections. Treatment involves oxygen therapy, medications, and supportive care.
Increase nutrient needs, lower interest in eating, and can slow growth
Preterm infants at high risk of breathing difficulties
Recommend small, frequent meals with concentrated energy that are easy to eat
Food Allergy
An adverse immune response to a specific food, causing symptoms like hives, swelling, difficulty breathing, or anaphylaxis.
Food Intolerance
an adverse reaction involving digestion or metabolism but not the immune system
Middle Childhood Age Range
5 to 10 years
Preadolescence Age Range
Girls: 9 to 10 years
Boys: 10 to 12 years
How is the growth rate during preadolescence?
Physical growth rate is steady but there is tremendous cognitive, emotional, and social development.
Nutrition Problems During Preadolescence
Iron deficiency anemia
Undernutrition
Dental caries
Weight issues at both ends of spectrum
Healthy People 2020 Objectives related to school-age children
Healthy People 2020 Objective | Baseline | Target | |
NWS-2.1: | Increase the proportion of schools that do not sell or offer calorically sweetened beverages to students. | 9.3% | 21.3% |
NWS-2.2: | Increase the proportion of school districts that require schools to make fruits or vegetables available whenever other food is offered or sold. | 6.6% | 18.6% |
NWS-10.2: | Reduce the proportion of children (aged 6–11 years) who are considered obese. | 17.4% | 15.7% |
NWS-11.2: | Prevent inappropriate weight gain in children aged 6–11 years (developmental). | ||
PA-4: | Increase the proportion of the nation’s public and private schools that require daily physical education for all students. Elementary schools Middle and junior high schools | 3.8% 7.9% | 4.2% 8.6% |
Healthy People 2020 Objectives related to school-age children
Healthy People 2020 Objective | Baseline | Target | |
PA-6.2: | Increase the proportion of school districts that require regularly scheduled elementary school recess. | 57.1% | 62.8% |
PA-8.2.2: | Increase the proportion of children and adolescents aged 6–14 years who view television, videos, or play video games for no more than 2 hours a day. | 78.9% | 86.8% |
PA-8.3.2: | Increase the proportion of children and adolescents aged 6–14 years who use a computer or play computer games outside of school (for nonschool work) for no more than 2 hours a day. | 93.3% | 100% |
PA-13.2: | Increase the proportion of trips to school of 1 mile or less made by walking by children and adolescents aged 5–15 years (developmental). | ||
PA-14.2: | Increase the proportion of trips to school of 2 miles or less made by bicycling children and adolescents aged 5–15 years (developmental). |
Height and weight gain during school age
•Average 7lbs (3-3.5kg) weight and 2.5in (6cm) height
When to use CDC and WHO growth charts
CDC: 2 to 20
WHO: >20
Physiological development for school age children
Muscular strength, motor coordination, and stamina increase
More complex pattern movements (dance/sports/gymnastics, etc.)
Body fat reaches a minimum then increases in preparation for adolescent growth spurt (BMI rebound occurs on average at 6 years or age)
Cognitive development of school age children: Self efficacy
Knowledge of what to do and ability to do it
Changes from magical thinking and egocentrism to concrete operations
Develops sense of self
More independent and learning roles in family/school/community
Peer relationships become important
DRI for Normal Growth
Age | Estimated Energy Requirements (kcal) |
0-3 months | (89 x wt [kg] – 100) + 175 |
4-6 months | (89 x wt [kg] – 100 ) + 56 |
7-12 months | (89 x wt [kg] – 100) + 22 |
13-36 months | (89 x wt [kg] – 100) + 20 |
Boys 3-8 years | 88.5 – (61.0 x age [y]) + PA x (26.7 x wt [kg] + 903 x ht [m]) + 20 |
Girls 3-8 years | 135.3 – (30.8 x age [y]) + PA x (10 x wt [kg] + 934 x ht [m]) + 20 |
Boys 9-19 years | 88.5 – (61.9 x age [y]) + PA x (26.7 x wt [kg] + 903 x ht [m]) + 25 |
Girls 9-19 years | 135.3 – (30.8 x age [y]) + PA x (10 x wt [kg] + 934 x ht [m]) + 25 |
Physical activity coefficients
Physical activity coefficient (Boys)
PA = 1 (sedentary)
PA = 1.13 (low active)
PA = 1.26 (active)
PA = 1.42 (very active)
Physical activity coefficient (Girls)
PA = 1 (sedentary)
PA = 1.16 (low active)
PA = 1.31 (active)
PA = 1.56 (very active)
Low active – 30 to 60 minutes of moderate activity daily
Active – 60 minutes of moderate activity daily
Very active – 120 minutes moderate activity daily OR 60 minutes moderate + 60 minutes vigorous activity daily
Protein for school age
Recommended is 0.95 gram of protein per kg body weight per day for boys & girls ages 4-13yrs
Dietary Reference Intakes for key nutrients for school-age children
Iron deficiency
•Less common in middle childhood than toddler age
•Treatment is oral iron trial for four weeks
•Dietary recommendations: eat iron-rich foods
•Meat, fish, poultry, and fortified cereals
Vitamin C rich foods to help absorption
Dental carries
Seen in half of children aged six to nine
Influenced by time teeth are exposed to carbohydrate
Complex carbohydrates such as fruits, vegetables, and grains are better choices than simple sugars
Regular meal and snack times are beneficial
Continued need for fluoride supplementation
Brush after eating!
% of school age children that are overweight between 2015 and 2016
32.8% of children ages 6 through 8 years and 35.6% age 9 to 11 years are overweight or obese (prevalence has increased over 30 years). See Table 12.3 on pg. 307 for categories of overweight/obesity.
Obesity prevalence differs by race/ethnicity
38.2% Hispanic
35.0% African American
19.1% White
12.1% Asian American
Characteristics of overweight school age children
Taller
Advanced bone ages (bone maturation)
Earlier sexual maturity
Look older
Higher risk for health consequences of obesity
30.5% increase in type 2 diabetes from 2001-2009
Effects of early onset obesity on adult morbidly and mortality is unclear
Predictors of childhood obesity
Age at onset of BMI rebound
Normal increase in BMI after decline
Early BMI rebound results in higher BMIs in children
Home environment - maternal and/or parental obesity is a predictor of childhood obesity
BMI Rebound
BMI rebound is the normal increase in BMI that occurs after BMI declines and reaches its lowest point, at about 4-6 years of age. The age at which BMI rebound occurs may have a significant effect on the amount of body fat that the child will have during adolescence and into adulthood. Early BMI rebound is defined as beginning before 5.5 years of age, while the average age of BMI rebound is 6 – 6.3 years of age. BMI rebound after age 7 is considered to be late. Studies have shown that adolescents and adults who had an early BMI rebound as children have higher BMI than those subjects who had an average or late BMI rebound.
The connection between parental obesity and obesity in children is likely due to genetic as well as environmental factors.
AAP Recommendation for Screen Time
AAP recommendations
No screen devices in bedrooms
Development of Family Media plan
No more than two hours each day of screen time
Strong relationship between TV viewing and obesity (reduced energy expenditure, increased dietary intake, disruption of sleep patterns)
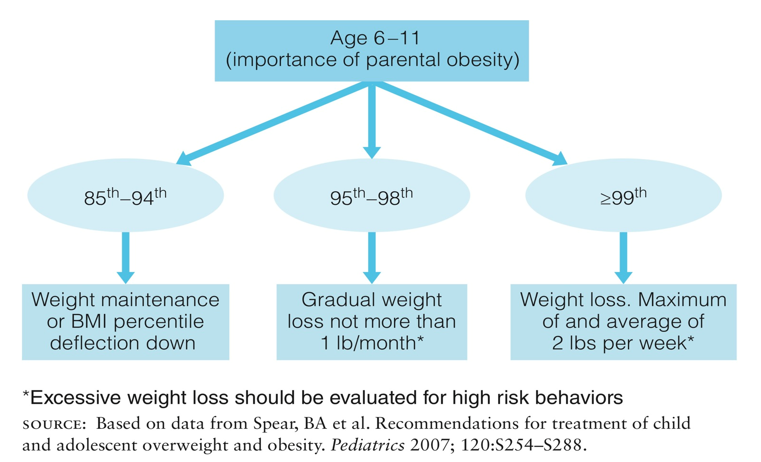
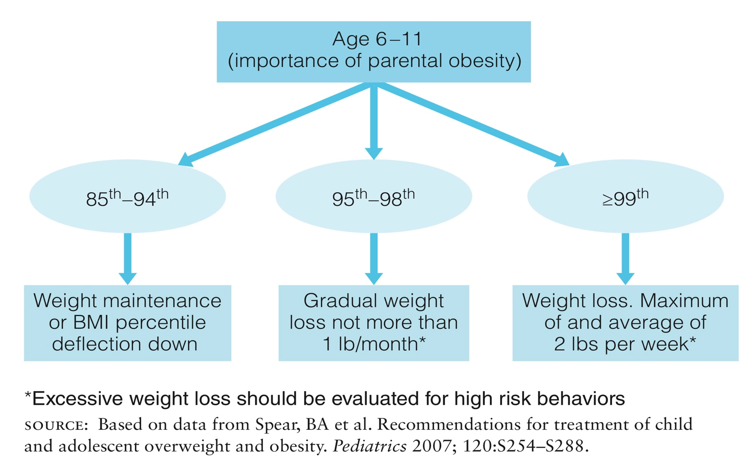
Treatment of overweight and obesity
Four stages
Stage 1: Prevention Plus
Stage 2: Structured Weight Management (SWM)
Stage 3: Comprehensive Multidisciplinary Intervention (CMI)
Stage 4: Tertiary Care Intervention (reserved for severely obese adolescents)
Obesity Percentiles
. With his weight-for-age at the 95th percentile and his height-for-age at between the 75th and 90th percentiles, Timothy is large for his age as compared to other boys the same age. The most significant finding is a BMI-for-age greater than the 95th percentile. This places him in the “obese” category.
2. Timothy’s parents should limit the amount of money they give him for extra food items school. They should provide healthier choices of foods, such as fruit and vegetables, in the home for after-school snacks. It would be good for the whole family to adopt healthier eating behaviors, especially since his mother is obese.
3. (a) Timothy’s parents could talk to his PE teacher at school and make sure that he is being encouraged to be active during PE class. (b) His parents could look into the possibility of having Timothy participate in an after-school program where physical activity and active play would be encouraged. They could investigate available community programs and resources that would facilitate physical activity. (c) Eating in front of the TV should be discouraged. (d) The whole family could be engaged in a more active lifestyle.
4. Having an obese parent does increase the likelihood that a child will have a weight problem. Having two obese parents further increases the risk of overweight. Researchers are realizing that pediatric overweight is a multifaceted problem, involving genetic as well as environmental factors. Lifestyle issues such as overeating and inactivity are also contributing factors.
Acceptable fat range
25 to 35% of energy for 4-18 years of age
Calcium and vitamin D
Adequate intake at this time needed for peak bone mass
4-8yrs = 1000mg/day 9-13yrs = 13oomg/day
Dairy products and calcium-fortified foods
Adequate vitamin D needed for calcium absorption
4-18yrs = 600IU/day
Vitamin D from exposure to sunlight and fortified foods
If needed, supplements for these nutrients can be given under the guidance of a physician or RD.
Types of Lactose intolerance
Primary – lactase enzyme production decreases over time (falls sharply in adulthood)
Secondary – decreased lactase enzyme production after an illness or injury
Congenital – lack of lactase enzyme from birth