L4: Descending inputs
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
Why are inputs from higher centres (descending inputs) needed
For goal-directed movements
move with purpose
the spinal cord on its own produces feedforward→ which only predicts→ and can get this wrong
note: these are not two separate components!→ it forms a heterachy!
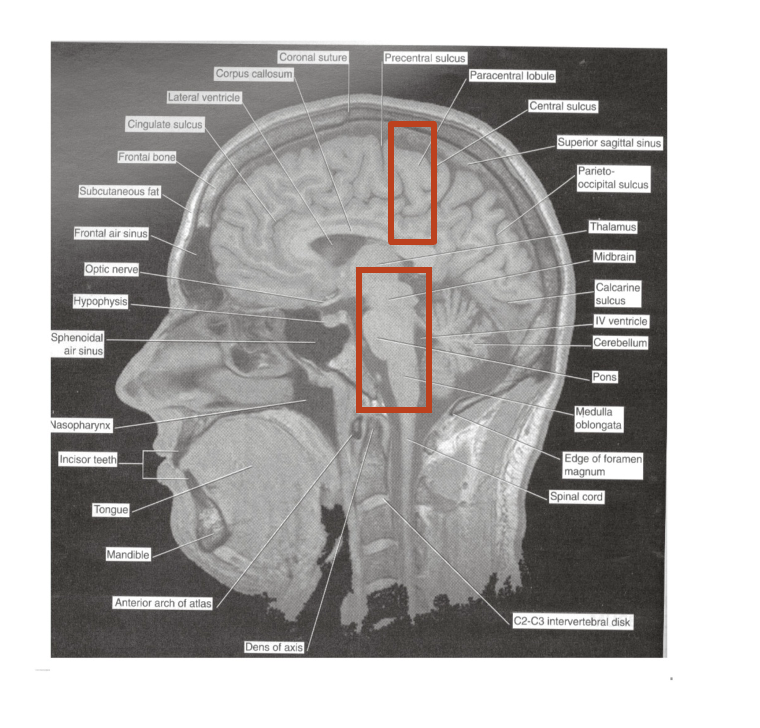
Two places these inputs are from
Cortical motor areas (motor cortex
Brain stem (pre motor area)
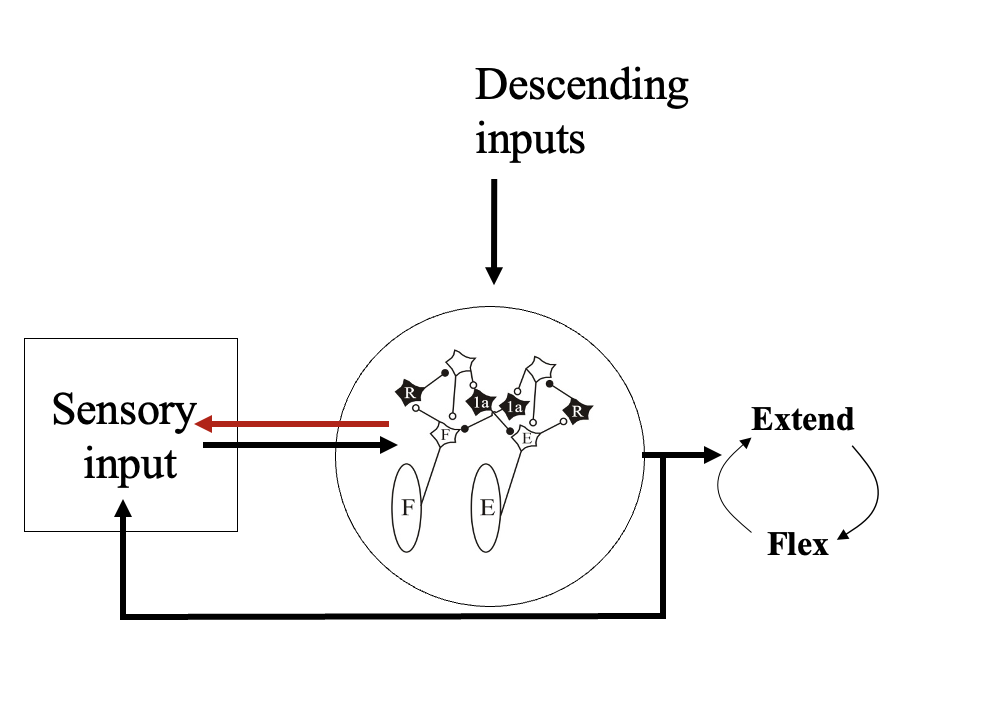
How are these descending commands integrated with spinal circuits
project to the brain stem and spinal cord
connect to spinal interneurons
to motor neurons
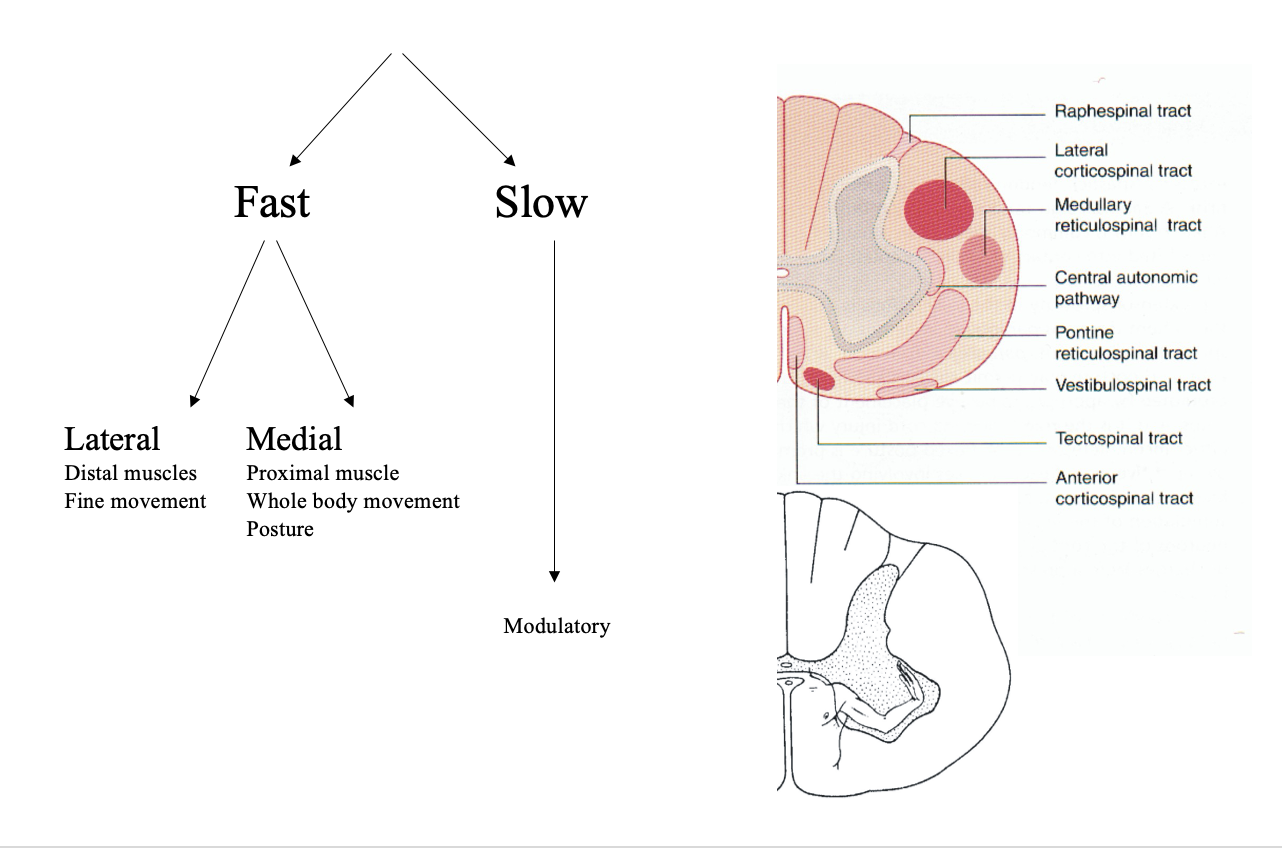
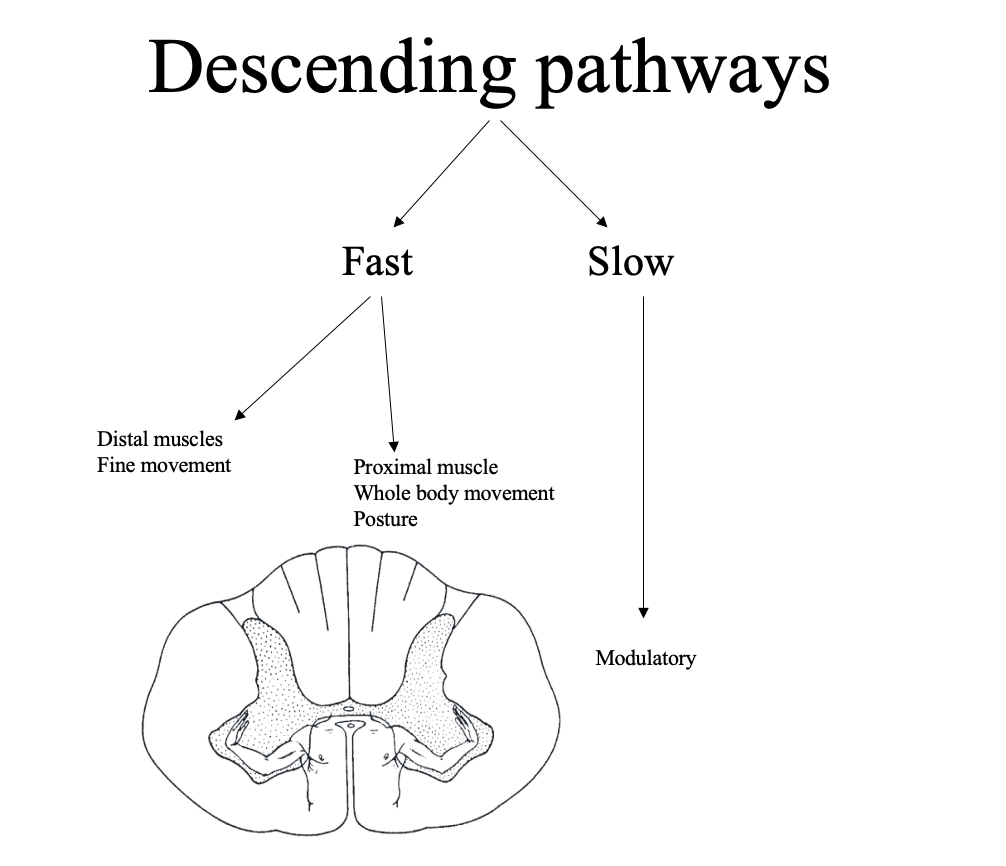
Two types of descending pathways
Fast pathways→
instantaneous activation
control specific aspects of on going movements and motor neurone timing
Slow pathways→
More constant and longer lasting
Uses amines and neuropeptides
to modulate spinal and motor systems
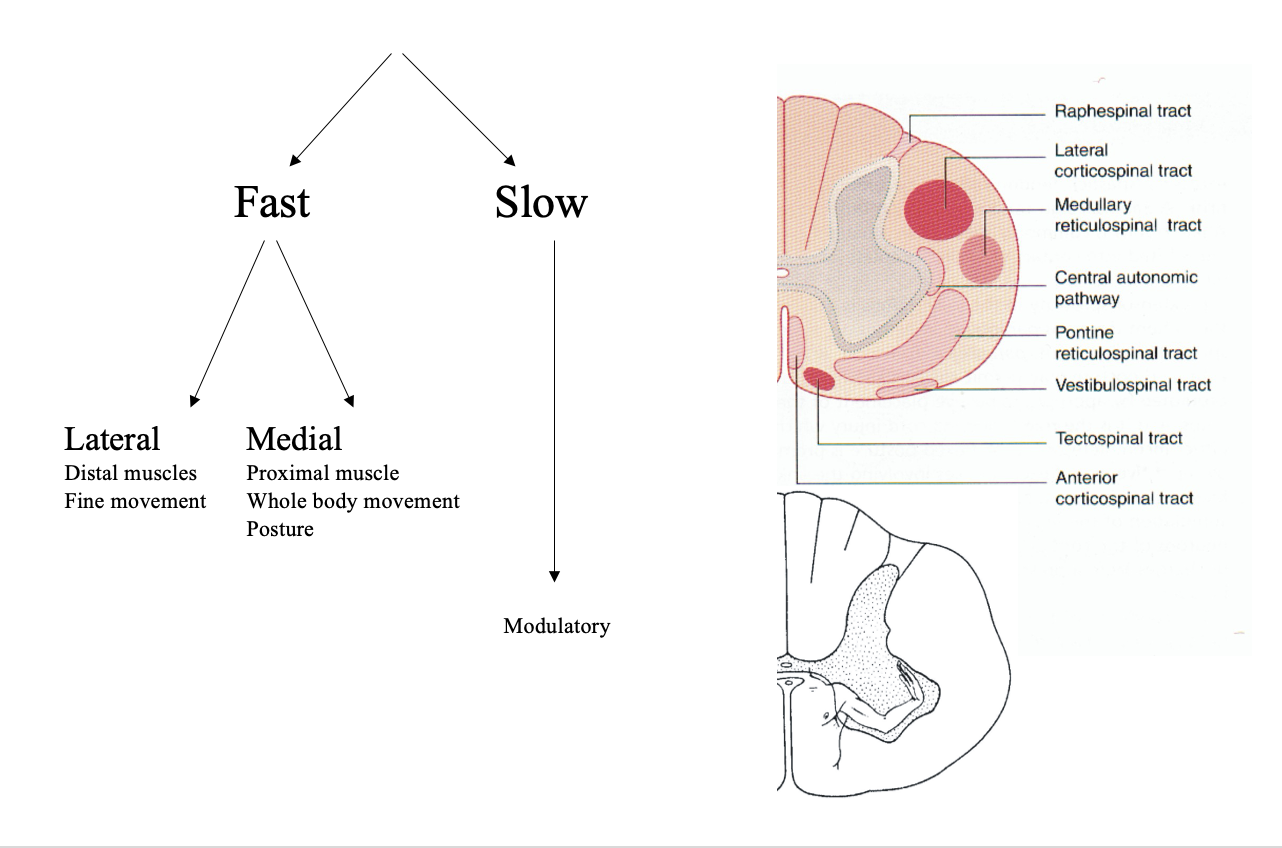
Fast pathways are split via spatial differences
Medial
Proximal muscle
whole body movements
posture
Lateral
Distal muscles
movements of extremities
Fine movements
note: proximal distal rule from L2
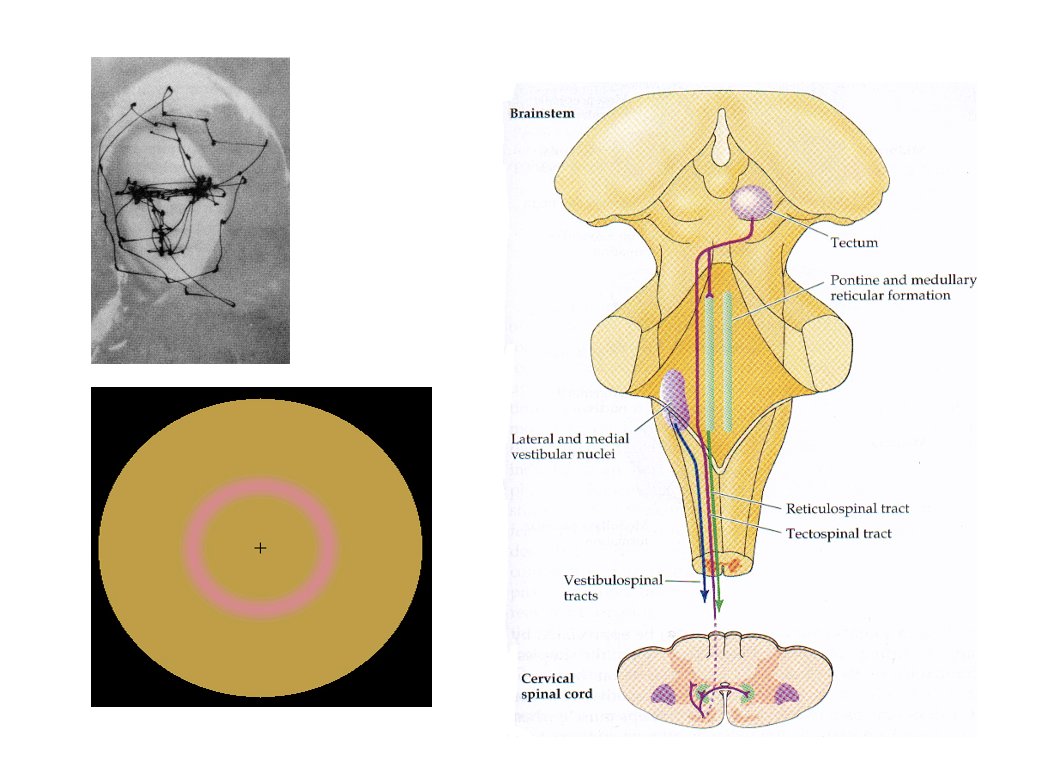
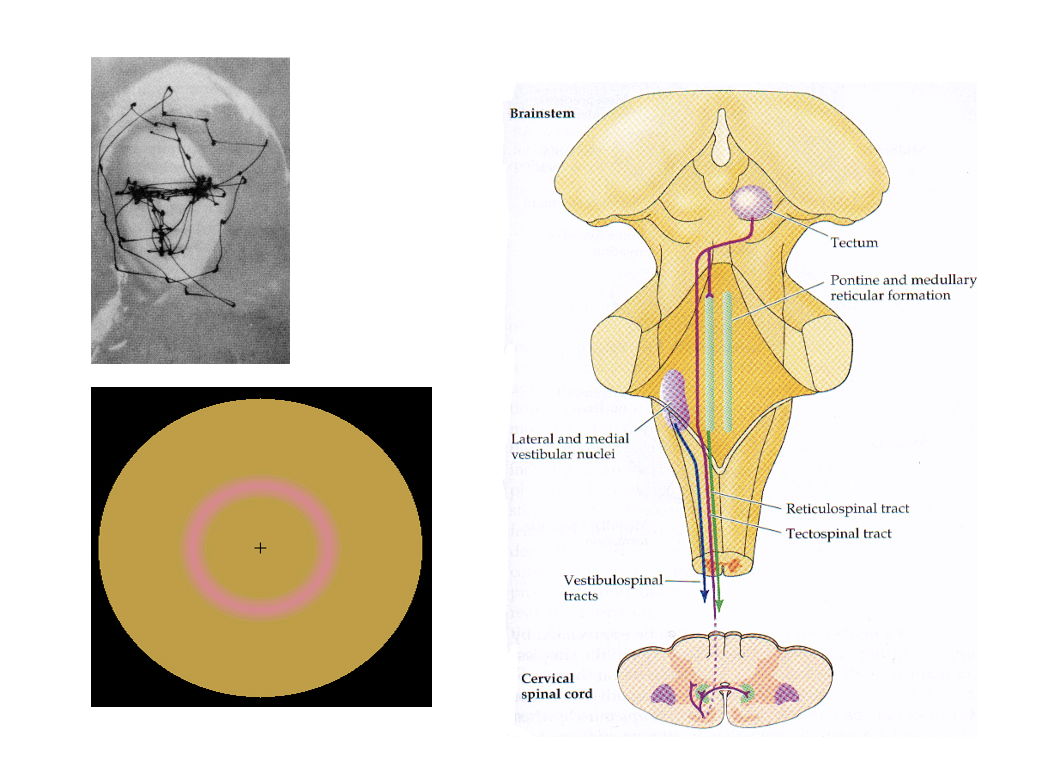
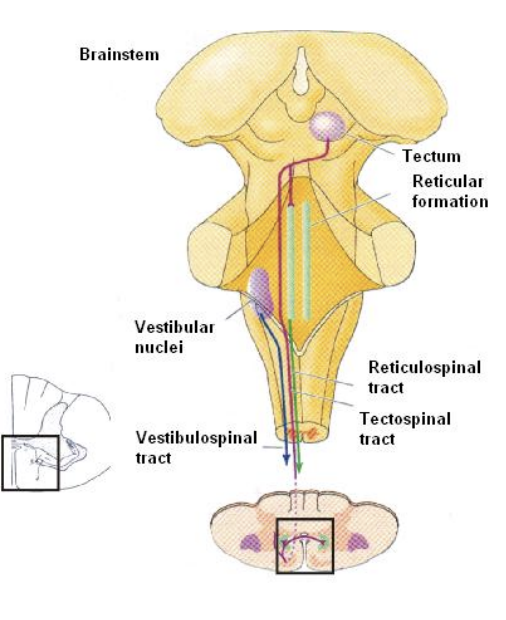
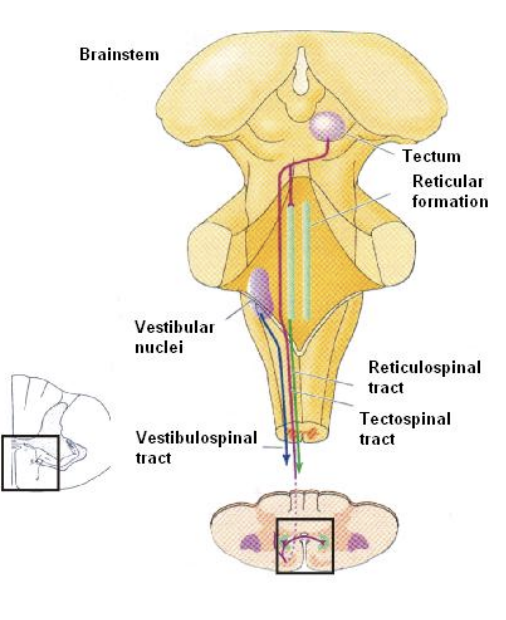
Medical brain stem pathways
Vestibulospinal: postural control, maintaining equilibrium and has projections to limb extensor (antigravity) muscles
2 pathways
Tectospinal: orientation (head and eye movements) to sound and objects
Reticulospinal: orientation and CPG activation
several brainstem tracts
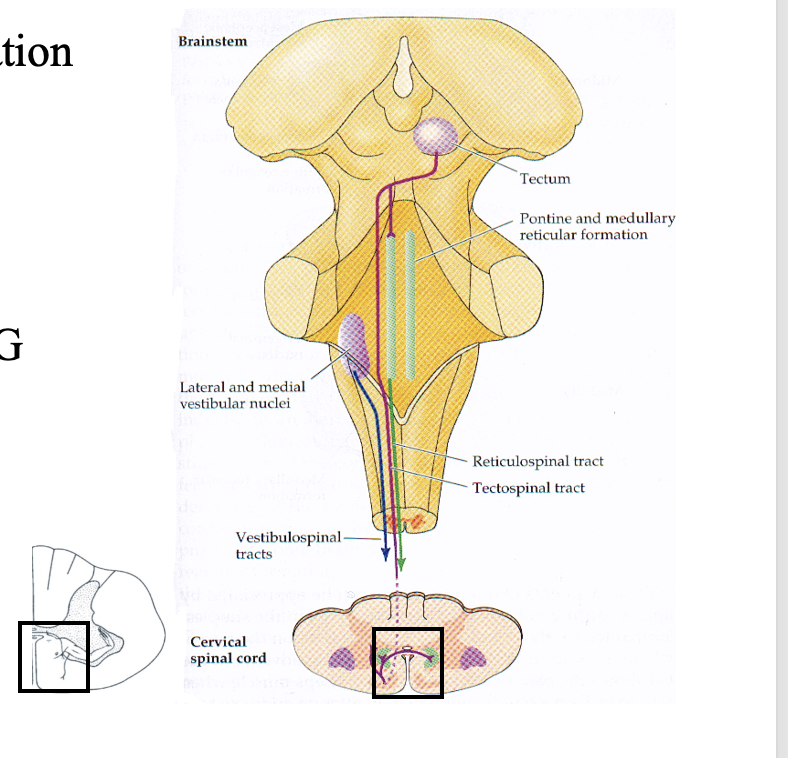
Vestibulospinal system
process information from the vestibular
found in the ear
Cupula in semi-circular canals:
filled with endolymph and modified hair cells in jelly-like substance
posture and balance
has projections to limb extensor (antigravity) muscles
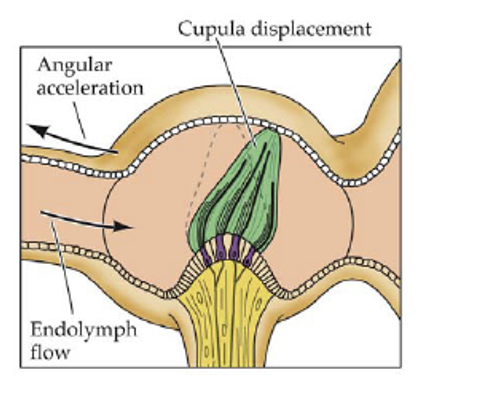
How does this help control posture and balance
Move head (voluntary or involuntary)
deflects a couplet
sends a signal
get information of movement from the head
sent to motor system to matai the posture
e.g increase your base so you don not fall over
Very accurately and quickly dectects a change in signal
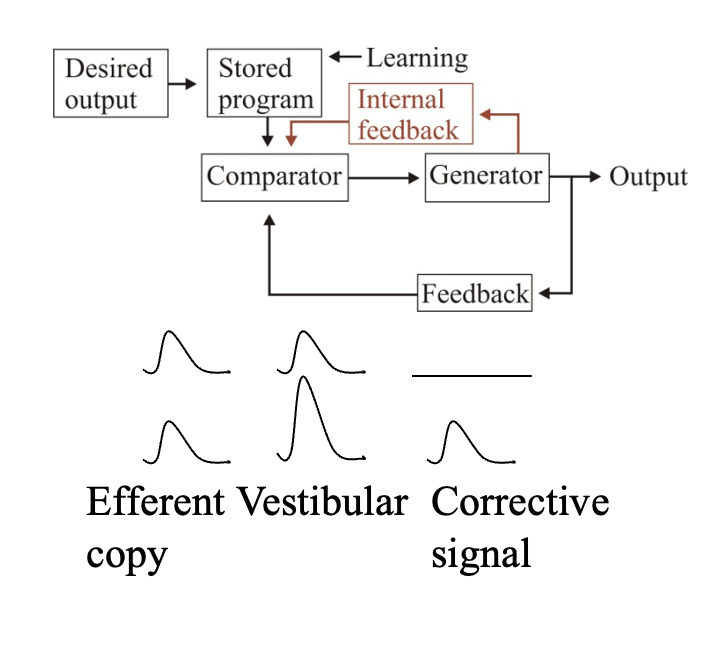
However, if we move the head voluntarily, the signal is still picked up. How is the reflex movement to maintain balance stopped in this case?
Feed-forward command to shut it down?→ but cannot be sure the prediction is correct
Solution: internal feedback (need to check this!)
Send efferent copy of the signal back to the muscle
calculates how much sensory input (re-afferent) is needed
finds the correct signal
adjusts posture as needed
its is not known has it does these calculations
Tectospinal system: strucuture
Coordinates head and eye movements (to sensory stimuli)
Has four bodies:
2 inferior colliculi→ integrate auditory, spatial and sensory data
2 superior colliculi→ direct behavioural responses to sensory stimuli
What does the superior colliculus do
Eye movements→ direct how we e.g scan faces in a particular way
Involuntary saccadic eye movements→ need to move constantly other wise the photoreceptors adapt
Why are these eye movements needed
Allows to orientate head and eye movements to sensory stimuli
Linking the auditory and visual space around you
Example:
when hear or something catches your eye at night
superior colliculus will guide your eye, head or even trunk towards the stimulus (i.e can control the whole motor system to orientate)
so you can get more info as to what it is (can foveate)
and build up the sensory map around you
Reticulospinal pathway: what involved in
general body orientation
simple motor patterns
EVIDENCE: pathway activates spinal CPG circuits (see later with cat)
Where do reticulospinal neurons receive inputs from
motor cortex
cerebellum
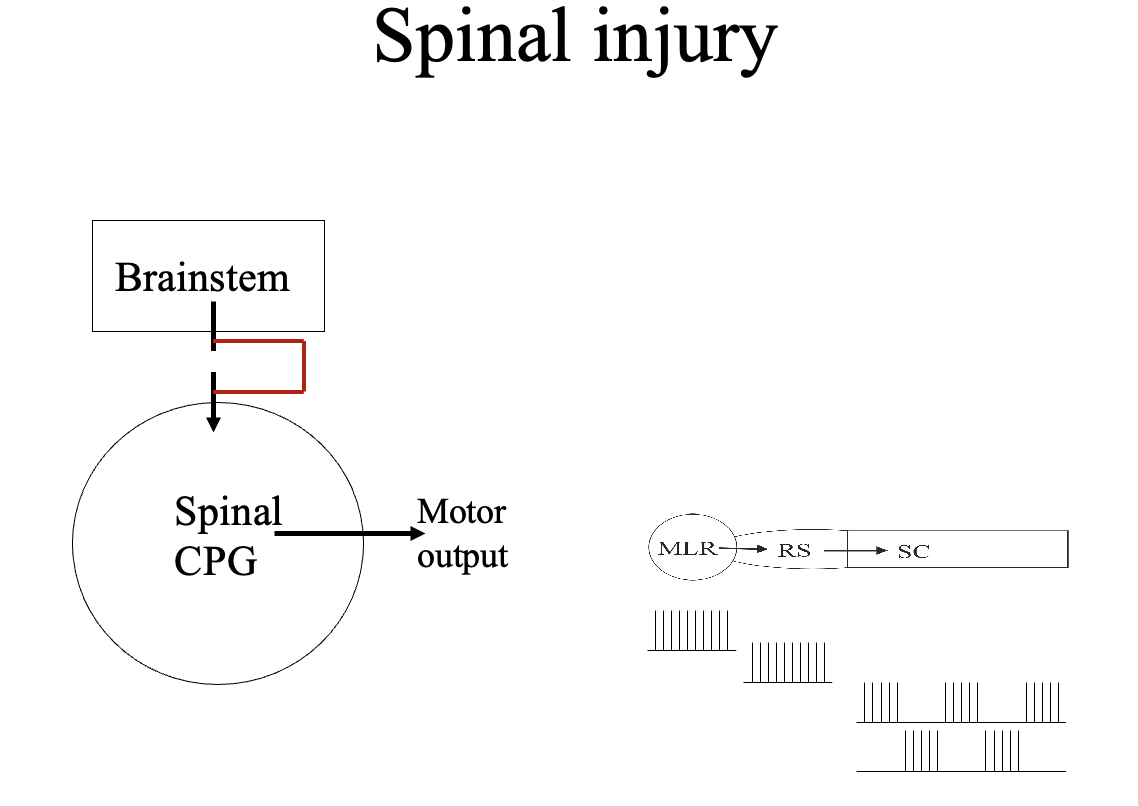
Descending pathways activate spinal motor systems: Shik and Orlovsky experiment with cat
Procedure:
electrical stimulation of midbrain of cat
elicit locomotion
Results
Low stimulation→ walking
Increased→ trotting
Further→ galloping
Conclusion:
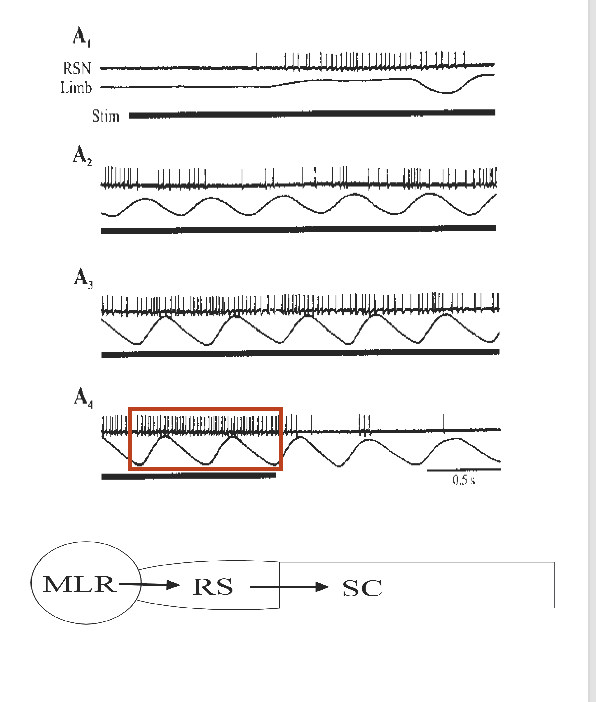
region stimulated→ Mesencephalic locomotor region (MLR)
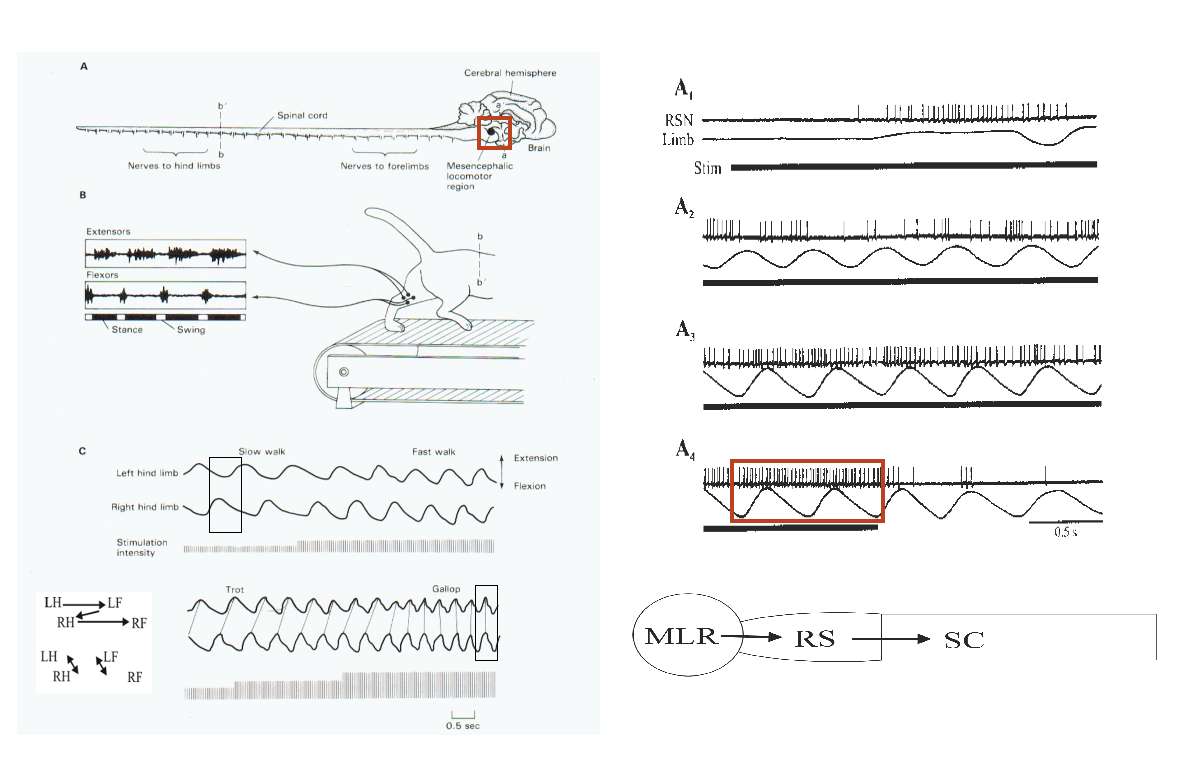
What does the MLR do
activates the reticulospinal system
→ switch on movements
THEREFORE: the descending systems allow the brain to modulate spinal locomotor networks (and their sensory inputs)
so that the output is appropriate for particular tasks
analogous structures have been found in other vertebrate systems
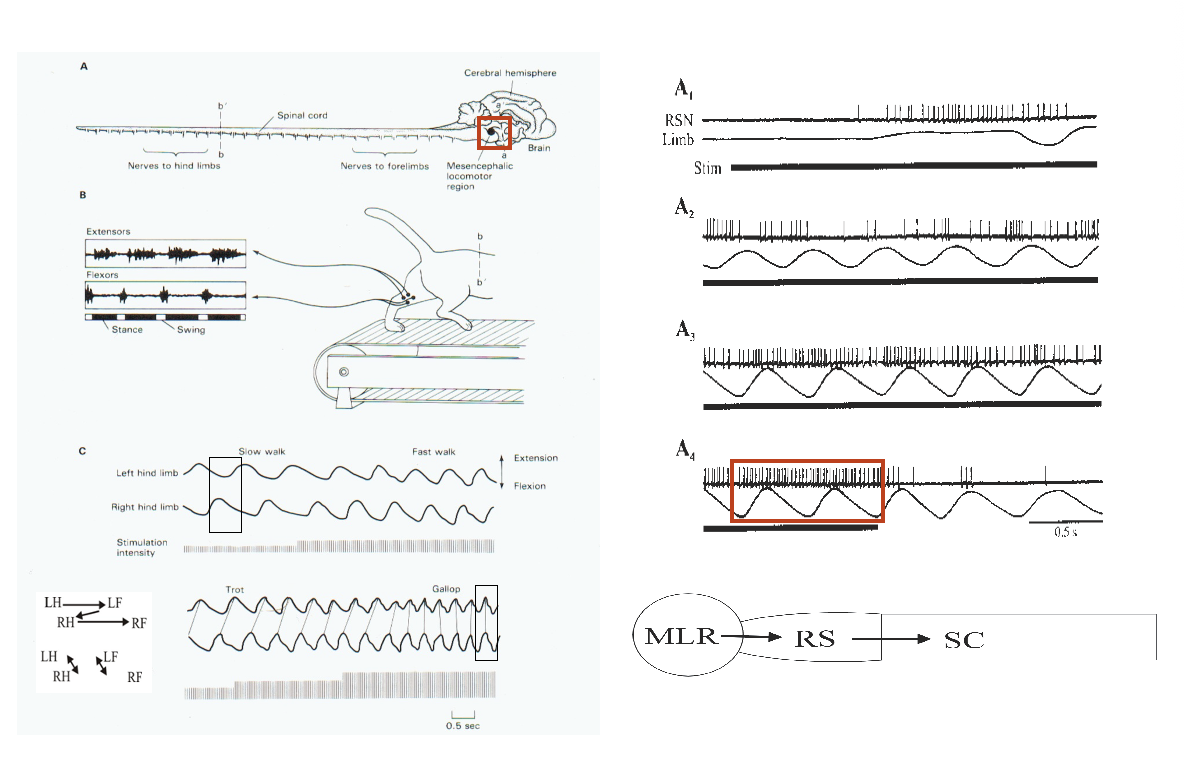
Why is the CPG involved in this response?
The MLR just sends a continuous train of AP at at constant frequency
this cannot coordinate the cycle of flex/extensor movement
This signal is just to switch on CPG
CPG interprets this signal as a command to generate a motor output
e.g the freq of action potentials
(e.g walking or running)
THEREFORE: the coordination of the basic output id done by spinal cord CPG
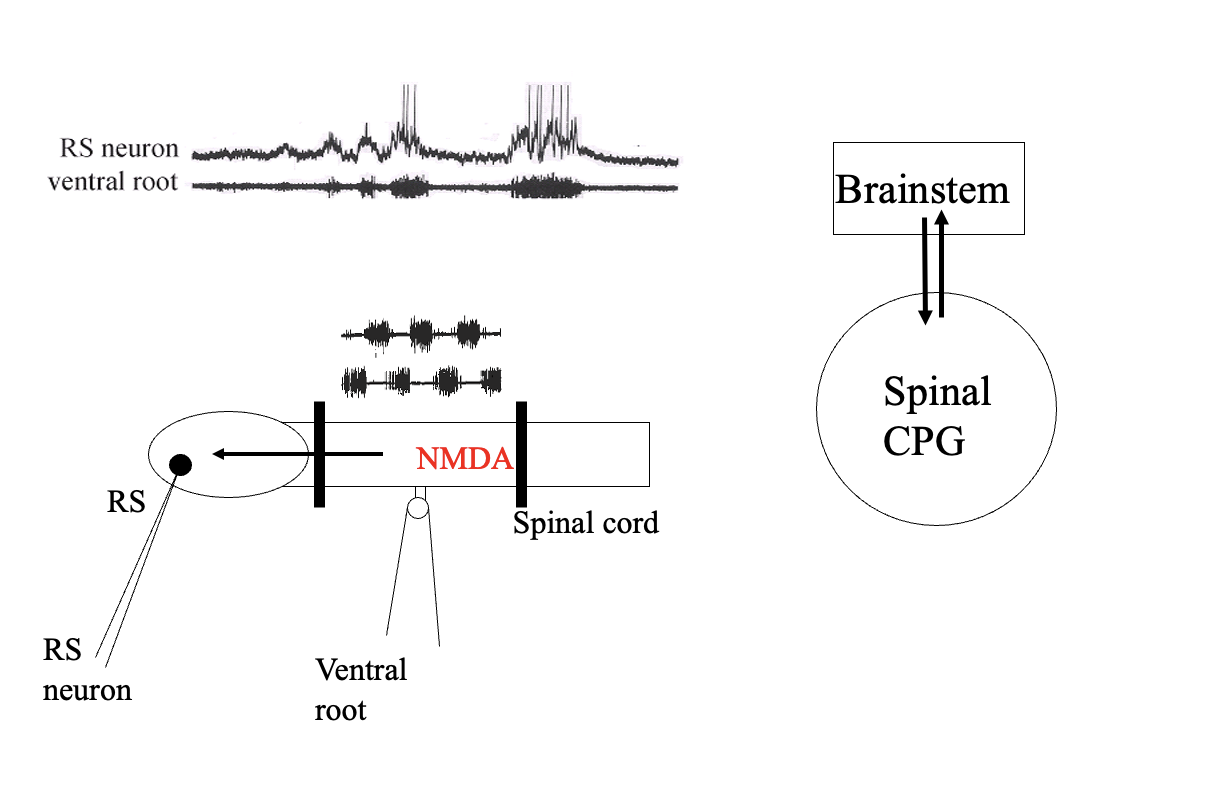
Not only is there signal from brain-stem to spinal cord, but there is input from spinal cord→ brainstem Example of 2 way interaction (HETERARCHY)
→Brainstem motor centres send inputs to but also inputs from the spinal cord
note:
another example of this (already seen in last lecture:
spinal CPG and sensory inputs
e.g golgi tendon organ reflex reversal (input to and from the spinal cord)
How was this (spinal cord→ brain stem) input found out?
Procedure:
evoke fictive locomotion in spinal cord
put barrier to stop connection to the brain
record from the neruon in the reticulospinal system
Result:
Neurons also gets depolarised
Conclusion:
two way interaction
sends a signal BACK to brainstem
THEREFORE: evidence of heterarchy
LATERAL brain stem pathways
Rubrospinal
Corticospinal
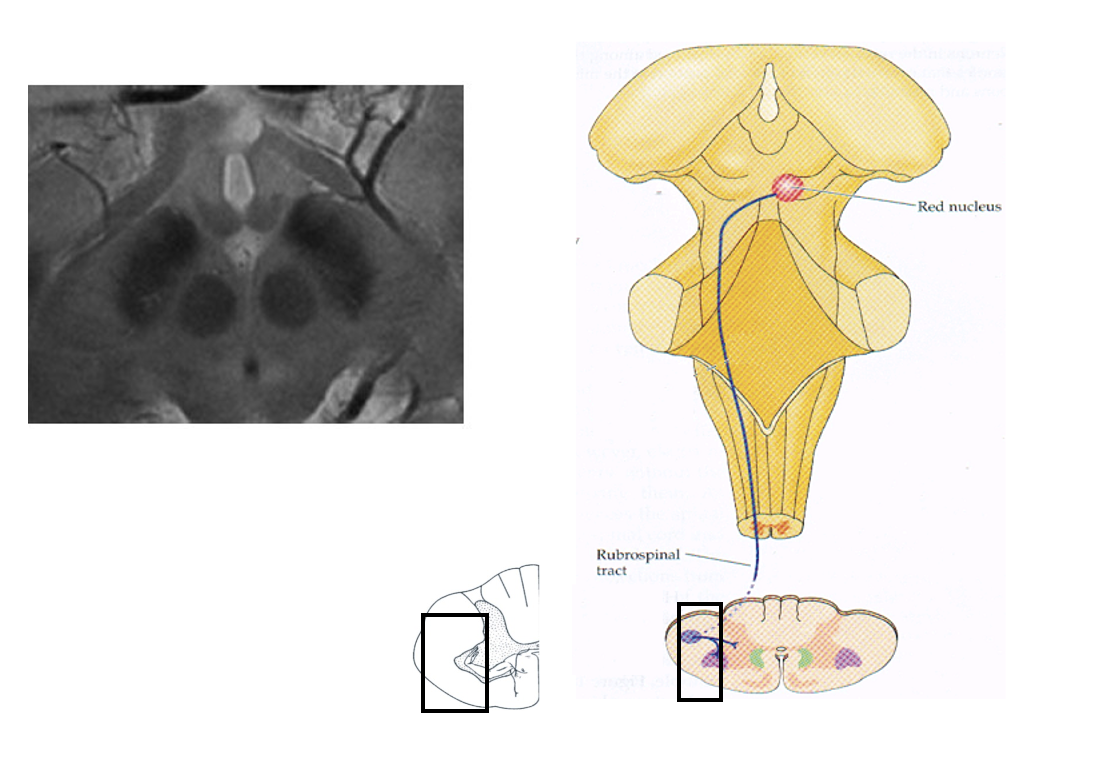
Rubrospinal tract: where does it come from (hint at name)
from the red nucleus
which crosses over and goes to the lateral regions of the oppsite side of the spinal cord
in lower vertebrates
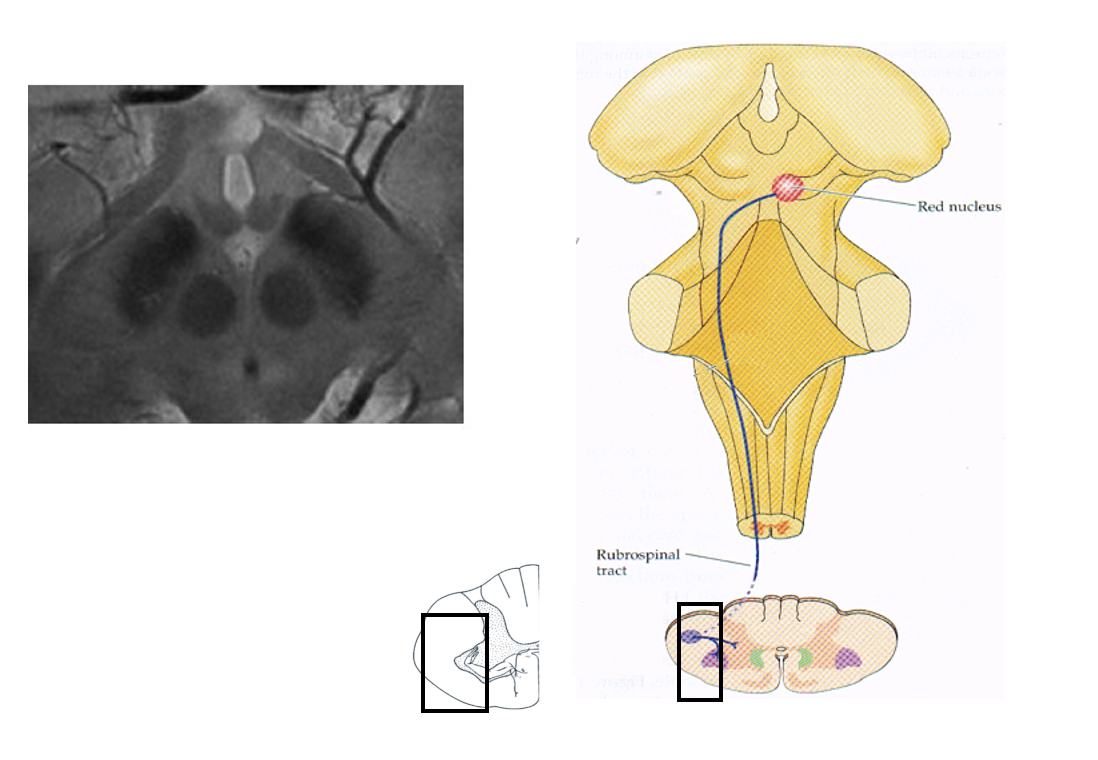
Rubrospinal tract: controls what in mammals
reaching
limb movements
Inputs of the rubrospinal tract
Some direct inputs from motor neurons
esp. in primates
Motor cortex
Cerebellum
Rubrospinal tract in humans?
replaced by the corticospinal tract
Instead: the red nucleus mainly sends inputs to the cerebellum
not the spinal cord
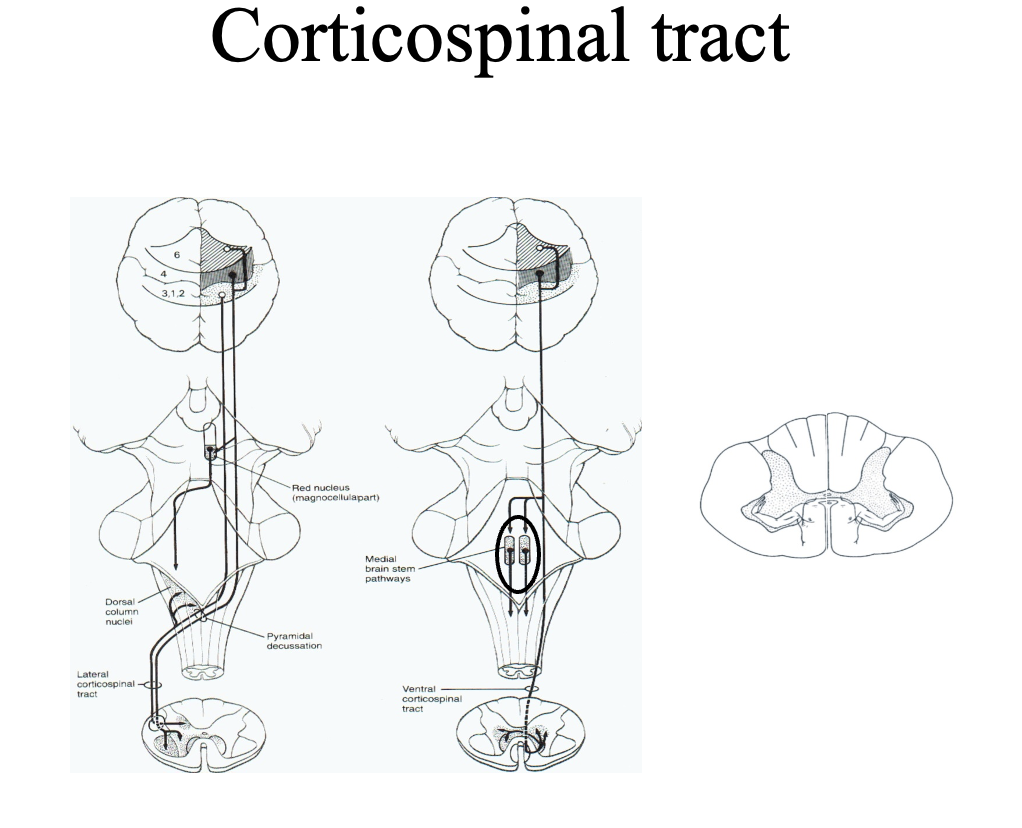
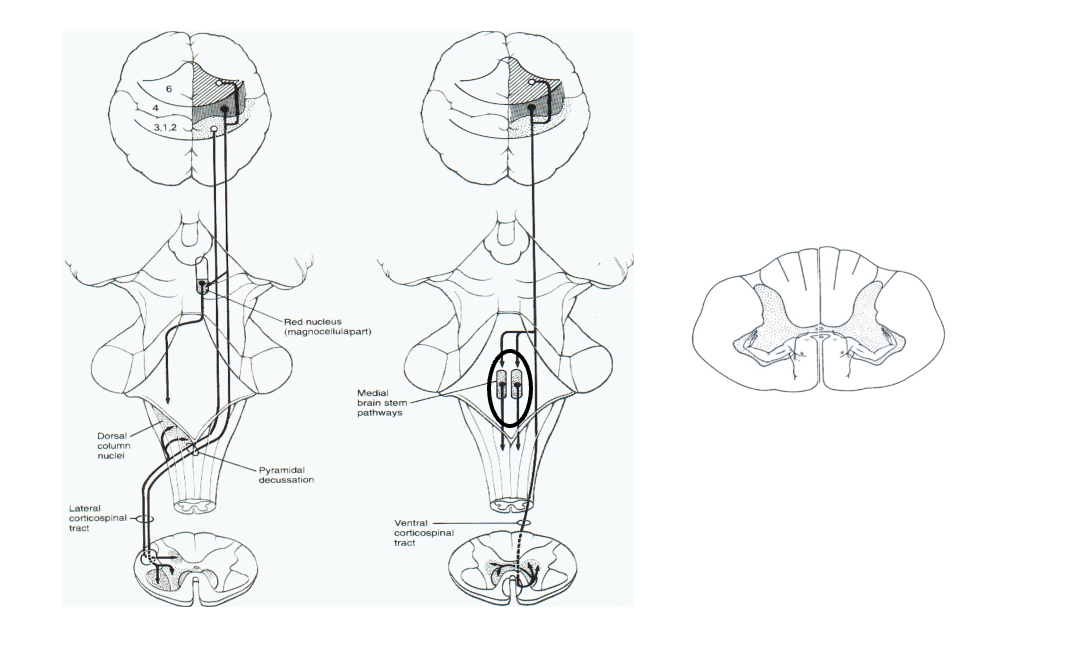
Corticospinal pathway→two pathways
The most important descending pathway in mammals
Large lateral pathway (left) (80% of fibres)
crosses the brain stem
Smaller ventromedial pathway (right) (20% of fibres)
uncrossed
What do corticospinal lesions cause
(e.g from stroke)
Initially→ muscle weakness and loss of reflexes
With time→ subsequent spasticity
why: reflects changes in sensory processing over time due to loss of descending regulation
Comparative anatomy of corticospinal tract
Show how corticospinal tract has changed during evolution
Rodents→ tract terminates in dorsal (sensory) areas
Cat/dogs→ terminate in intermediate zone
monkey→ some direct connections to motor neurons appear
Humans→ inputs to motor neurons are widespread in humans
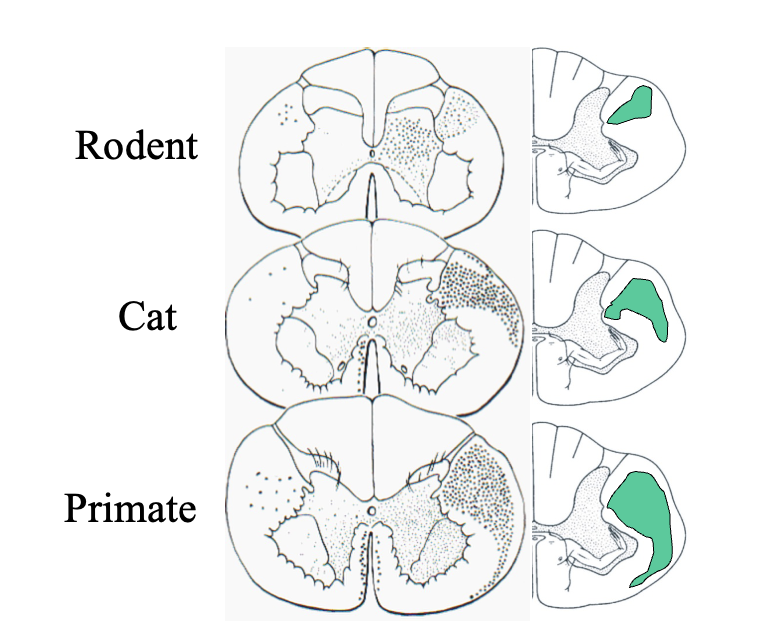
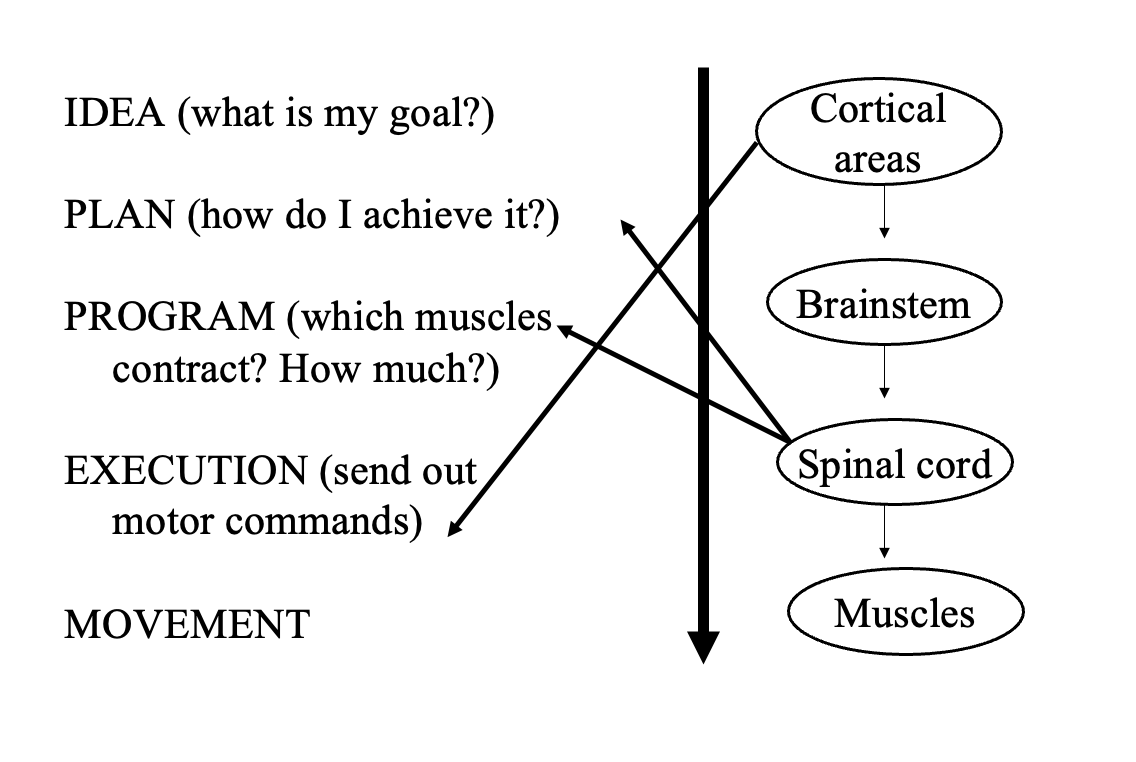
Therefore→ we emphasise the heteracrhy
cortical areas are involved in direct execution of motor system
Descending pathways can also influence (what is this comparable to)
Development of spinal systems
(this is comparable to the effects of vision from L1→ where vision helps the development of the motor system and vise versa)
At what age do the direct projections from motor cortex to motor eurons begin to mature
At 9 months
About the same time that manipulative skills begin to develop
These manipulatve skills between children of 7-8 months can be compared to stroke patients who have lsot corticospinal inputs
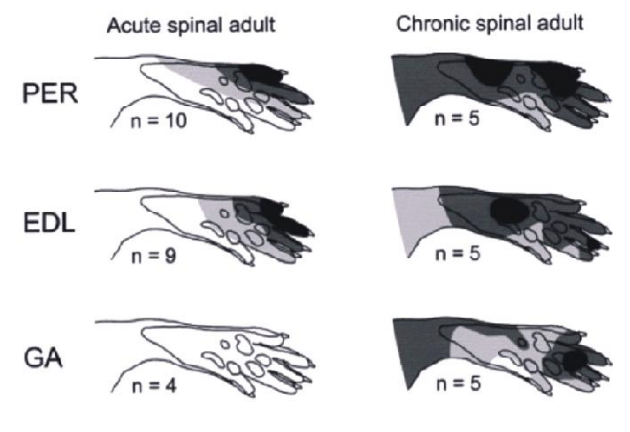
Investigating descending regulation of inputs: receptive fields of nociceptive afferents and conclusion: EVIDENCE that inputs influence development
Procedure:
Rats with spinal cord transected so just goes to dorsal
either in
neonates (right)
(acute) adults (left)
Results:
receptive fields of nocicepetic afferent are increased in neonates compared to (acute( adults
Conclusion:
receptive fields are regulated during development by descending pathways
What was also found in this experiment (neonate vs adult)
Direction of limb movement in response to nociceptive stimuli also differs in normal adult rats vs rates subjected after birth
Adult normal→ direction is away from nociceptive stimulus
Adult transected→ direction inappropriate towards the nociceptive stimulus
Neontatal transection→ prevents normal shaping of flexion withdrawal reflexes by descending inputs

Role of descending inputs in the development of spinal function is also shown in human cerebral palsy
Cerebral palsy→ defects descending systems
which are associated with changes in the regulation of spinal reflexes
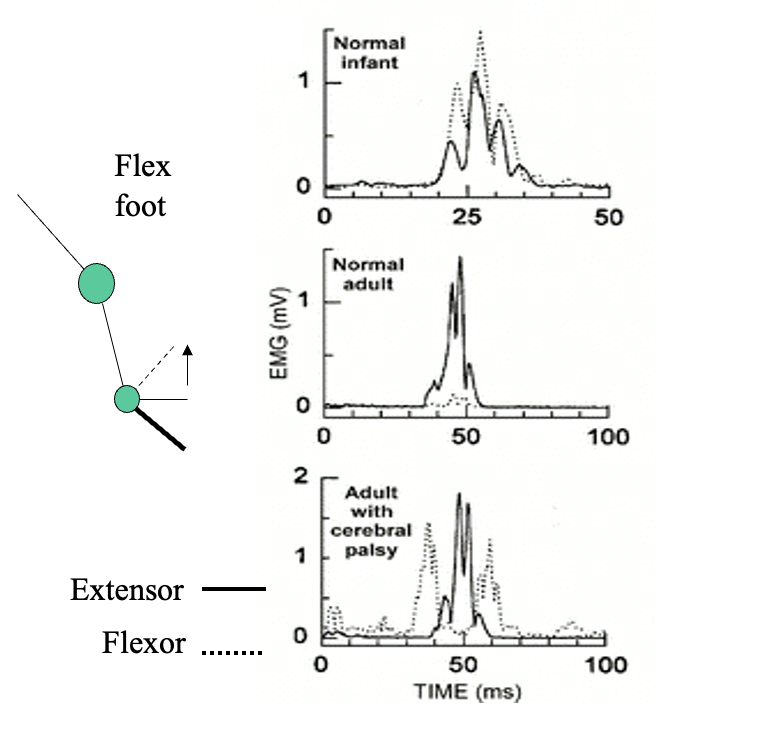
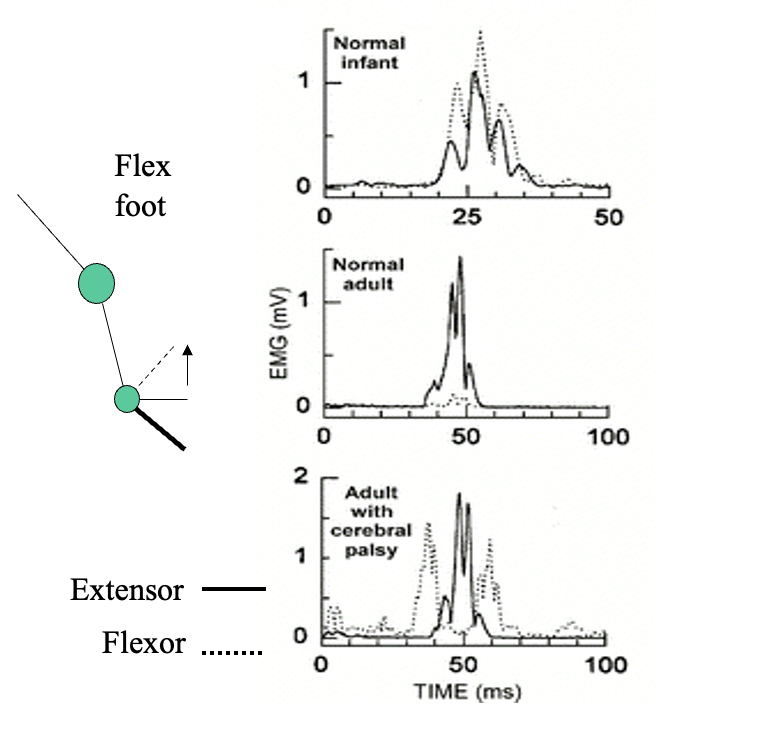
Dorsiflexion differences in normal adult vs infants and adults with cerebral palsy
Dorsiflexion: pushing the foot up
Normal foot→ short-latency muscle response: causes reflex contraction of the tibialis anterior (extensor) muscles→ to oppose the movement
Cerebral palsy→ Activate flexor and extensor muscles
What does this suggest: role for descending inputs in regulating the development of mature spinal function
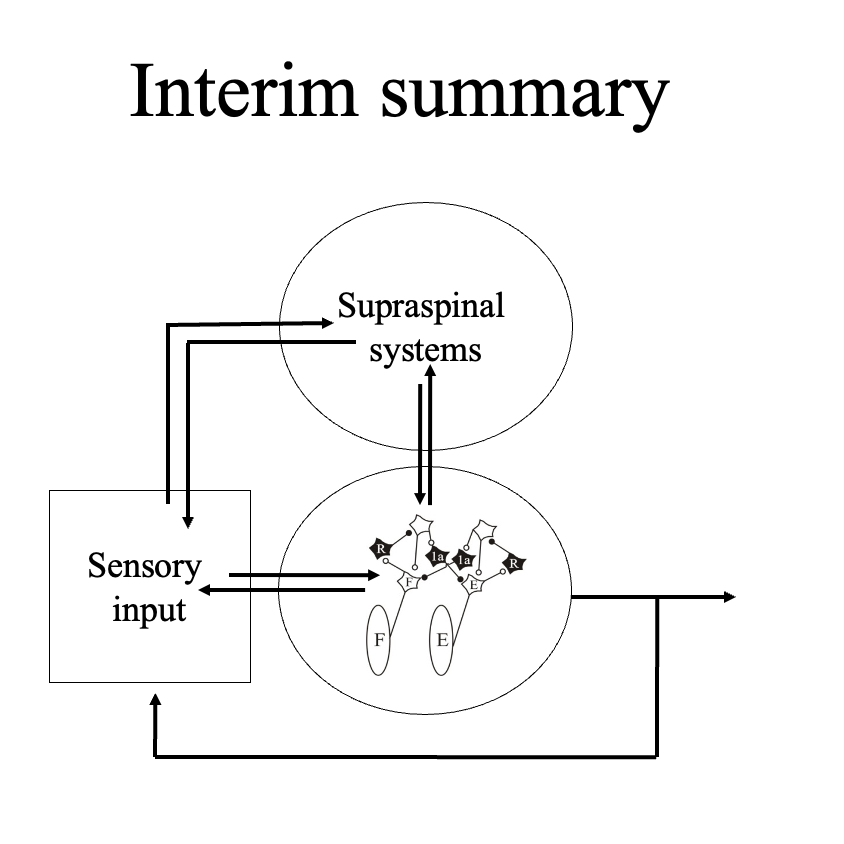
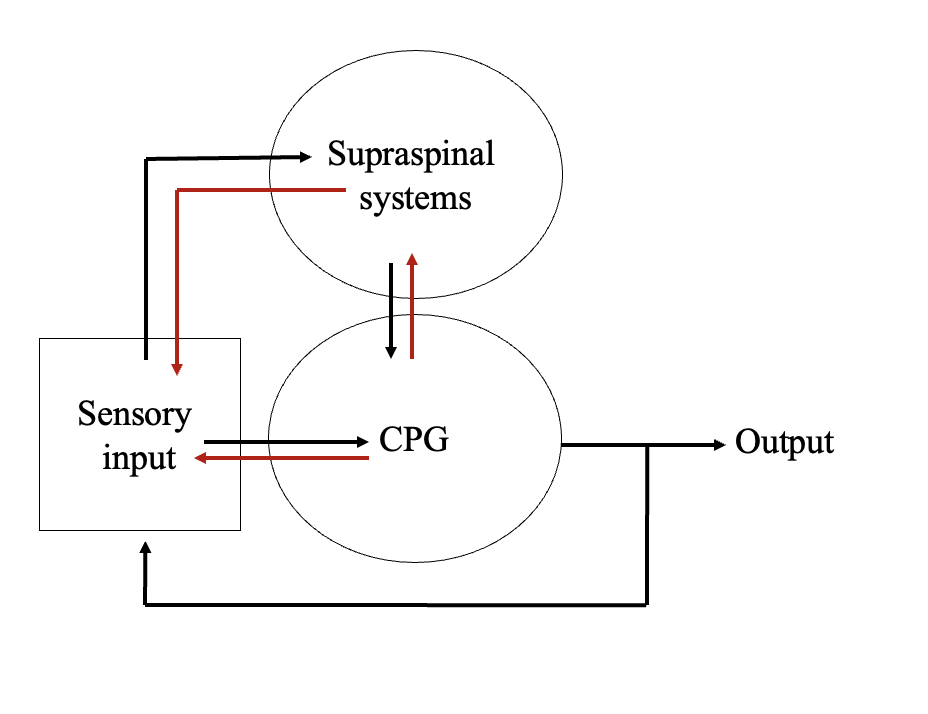
Overall what do the fast pathways show us (in terms of hertarchy)
Supraspinal ← → Sensory input
Supraspinal ← → CPG
Sensory input← → CPG
SLOW decesning pathways: what designates slow vs fast pathways
the relative speed of onset of their effects and duration of action
Largely reflected in synaptic transmission:
Ionotropic→ fast
Metabotropic→ slow
Characteristic of slow pathways
does not affect directly
create longer lasting modulatory responses
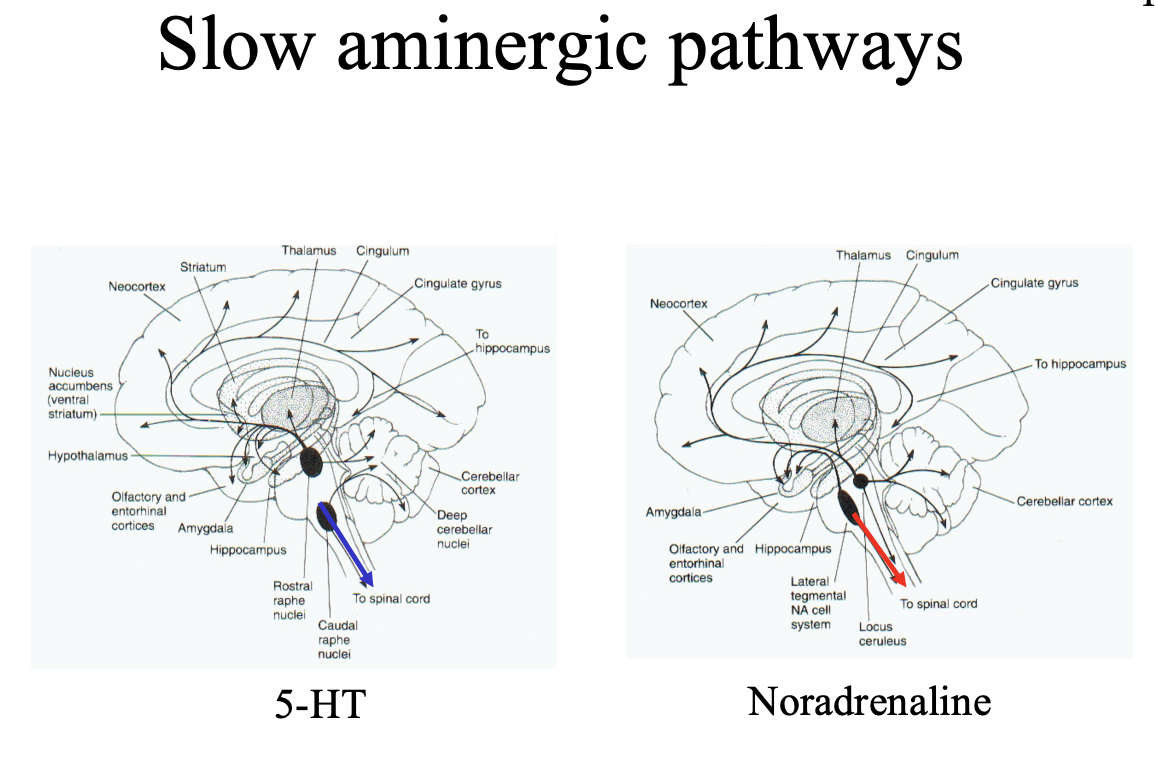
Slow pathways NTs and Neuropeptides
Predominantly→ Aminergic
5-HT from Raphe nucleus
NA from locus coeruleus
Some use neuro peptides:
Substance P
galanin
thyrotophin-releasing hormone
NA
neuropeptide Y
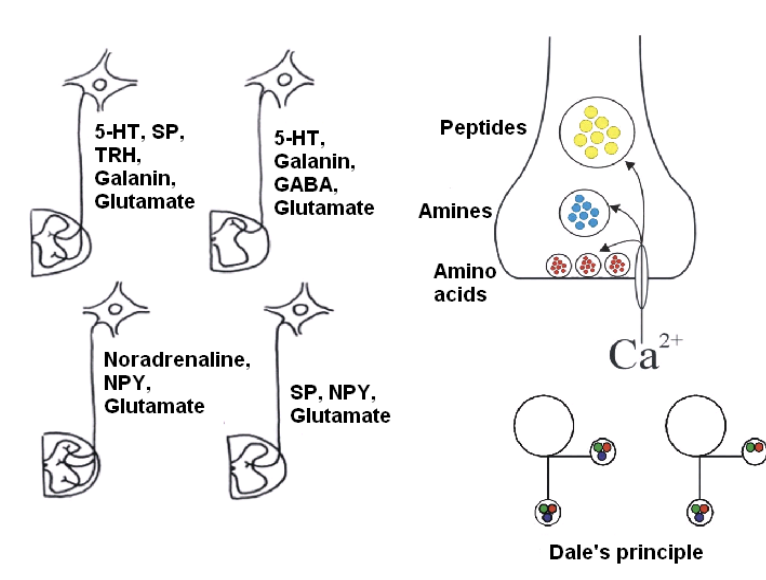
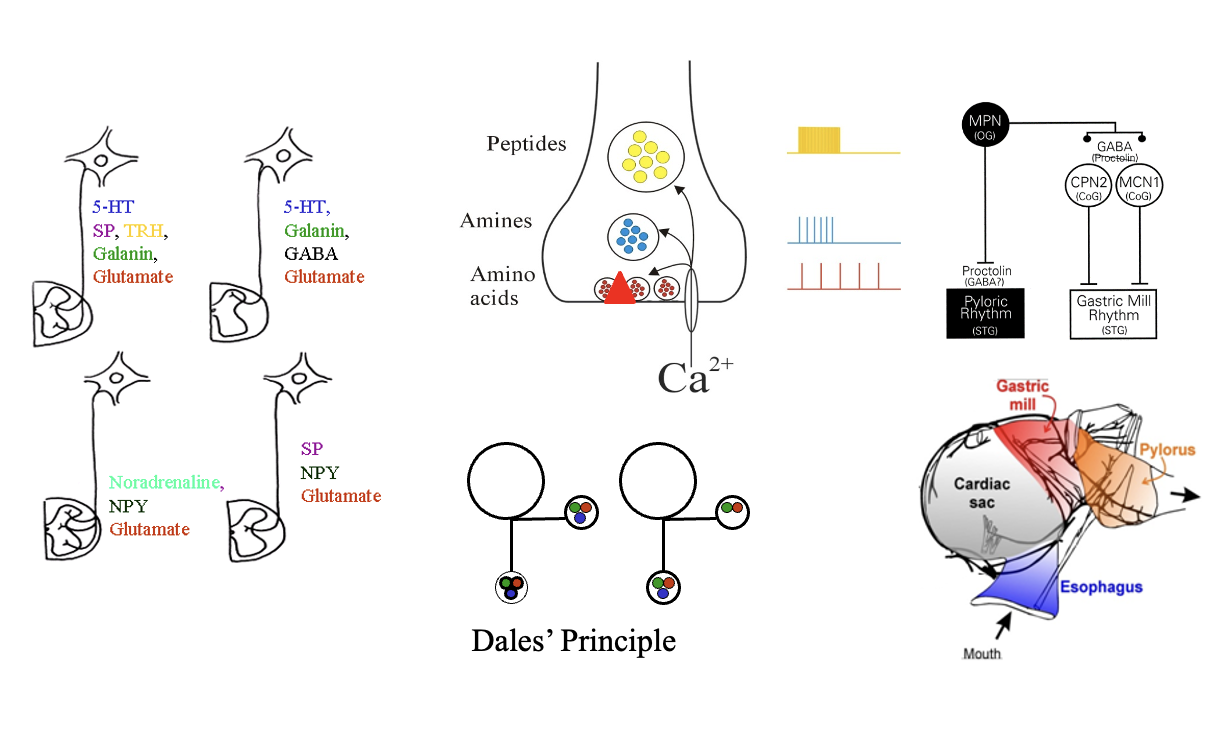
Slow pathways showed evidence for co-localisation of transmitters
loads of transmitters in one neuron
if single neuron is stimulated→ can release more than one transmitter
single neurons can co-localise and release multiple vescicles
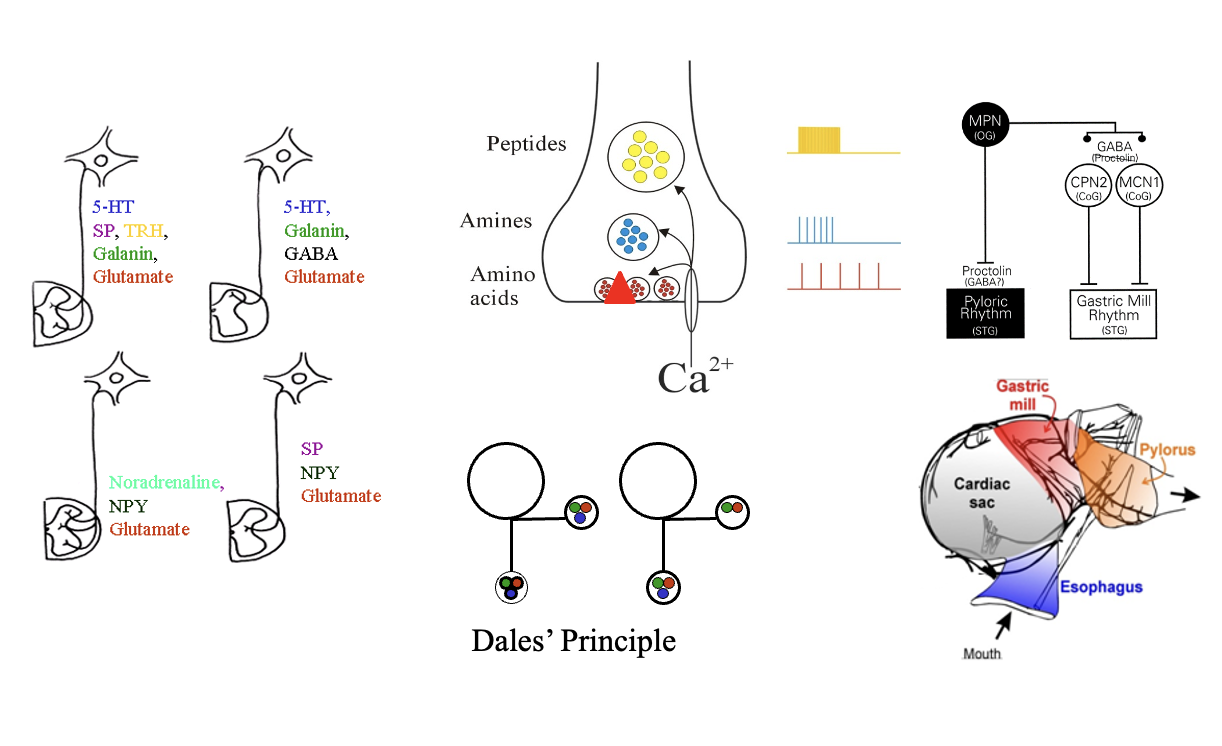
How are these different NTs/Neuropeptides arranged in the neuron
From closest to terminus towards the axon:
Amino acids (glutamate)
Amines (larger vesicles)
Peptides (substance B)→ larger and even further from the active surface
Their release is dependent on the activity
Low Ca2+ freq signal→ only release one closest (amino acids)
As increase the freq signal→ the amino and peptides etc are also released too
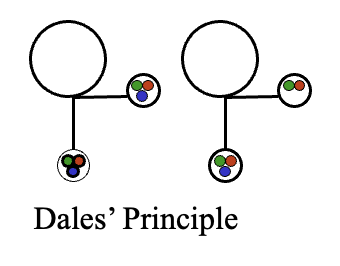
THEREFORE: Dale’s principle is negatied (that single neuron contains a single transmitter)
note: Dale never actually named it (was Eccles in honour of Dale )
at one terminal→ can release different NTs
Eccles then changed the principle
the same transmitters would be found at all branches of a neuron
not that a neurone release only one transmitter
HOWEVER: there have been some exceptions to this
Amines and peptides act via
G-protein-coupled receptors
intracellular pathways
→ Alter cellular and synaptic properties of spinal cord neurons
i.e locomotoer CPG or sensory inputs
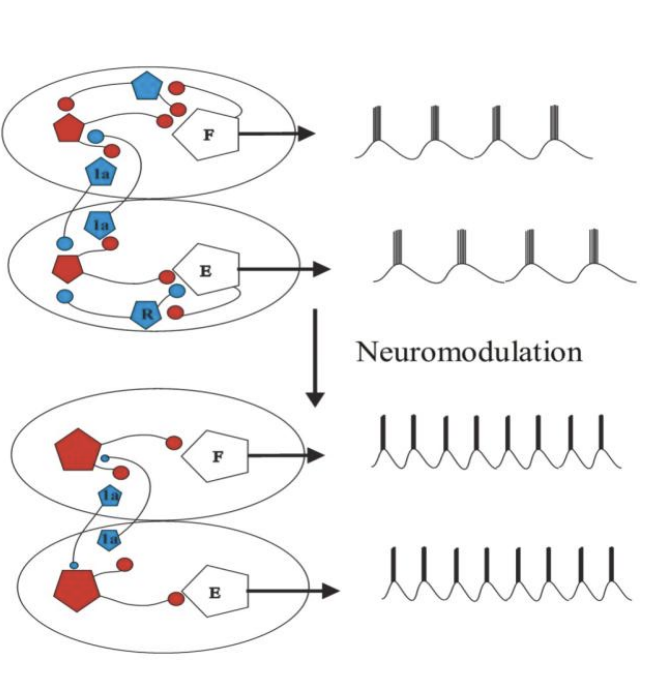
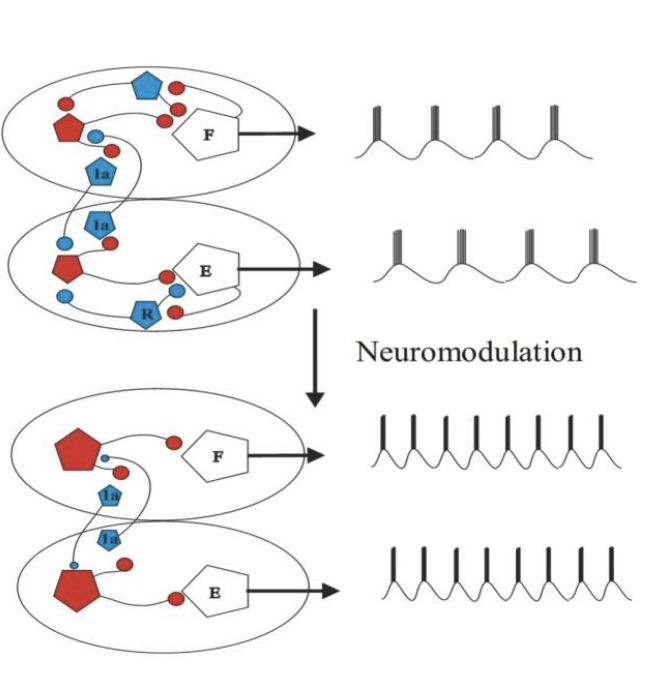
This is Neuromodulation
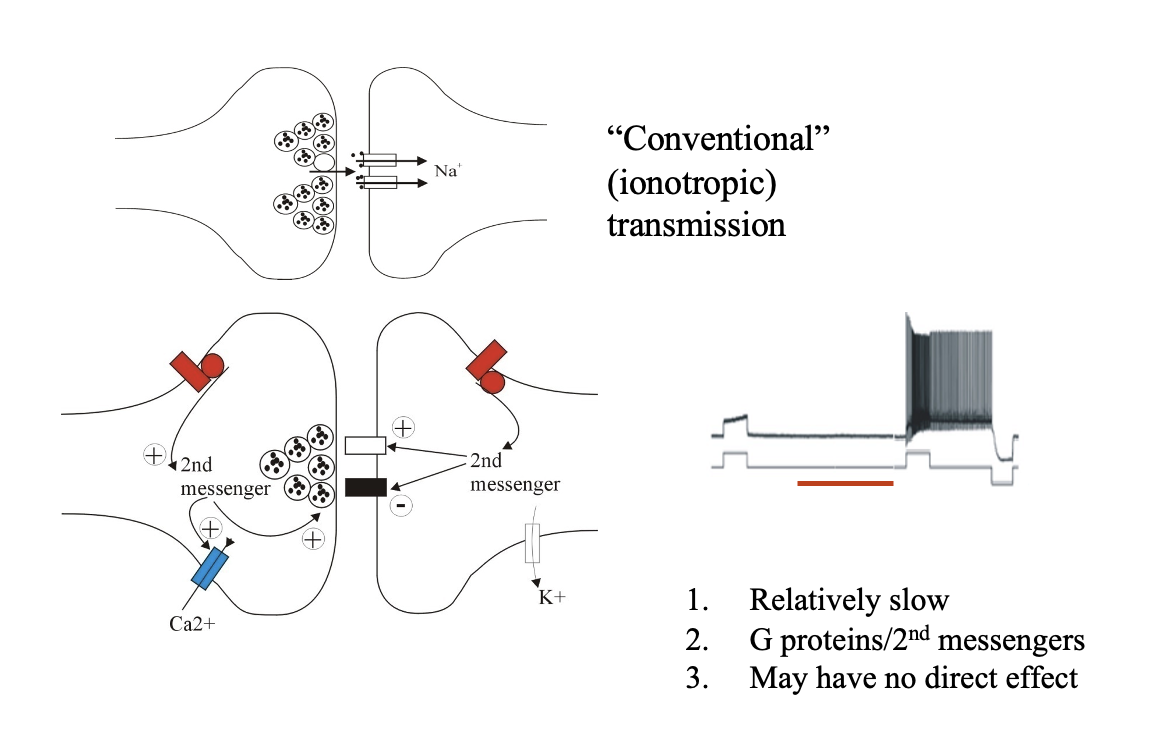
Example of neuromodulation: 5-HT
5-HT converts a cell that is silent in response to a depolarising input
positive current injected into the cell
to one generating a high frequency train of action potentials
‘plateau potential’
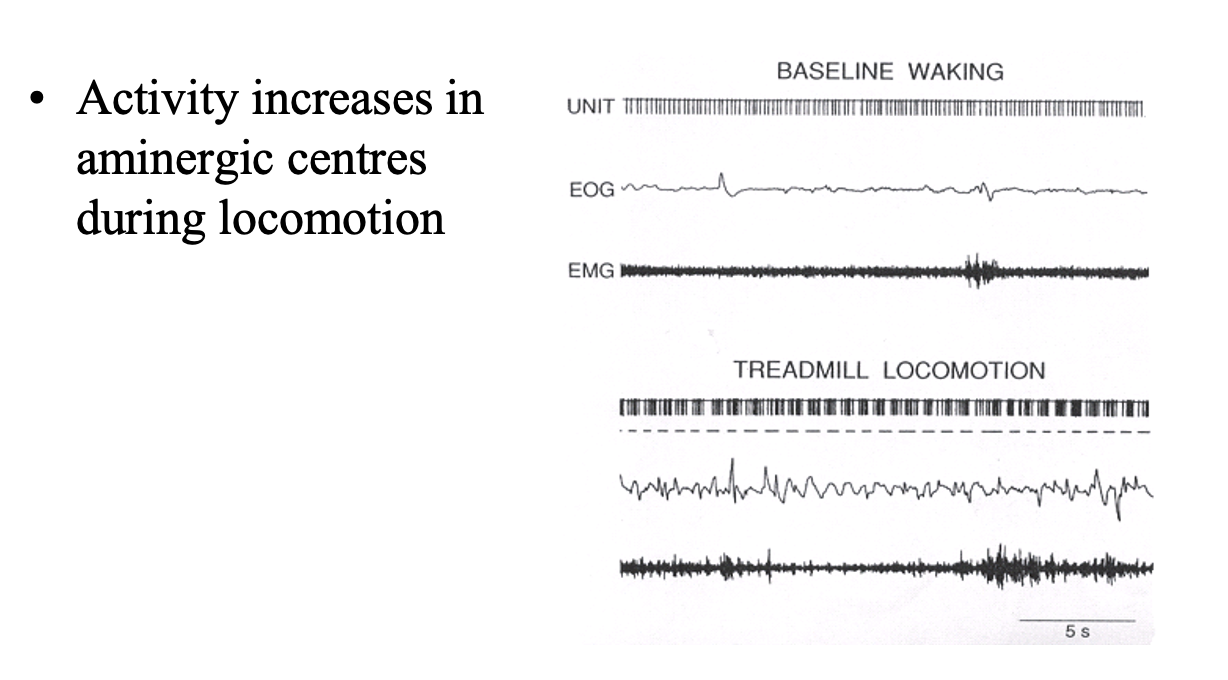
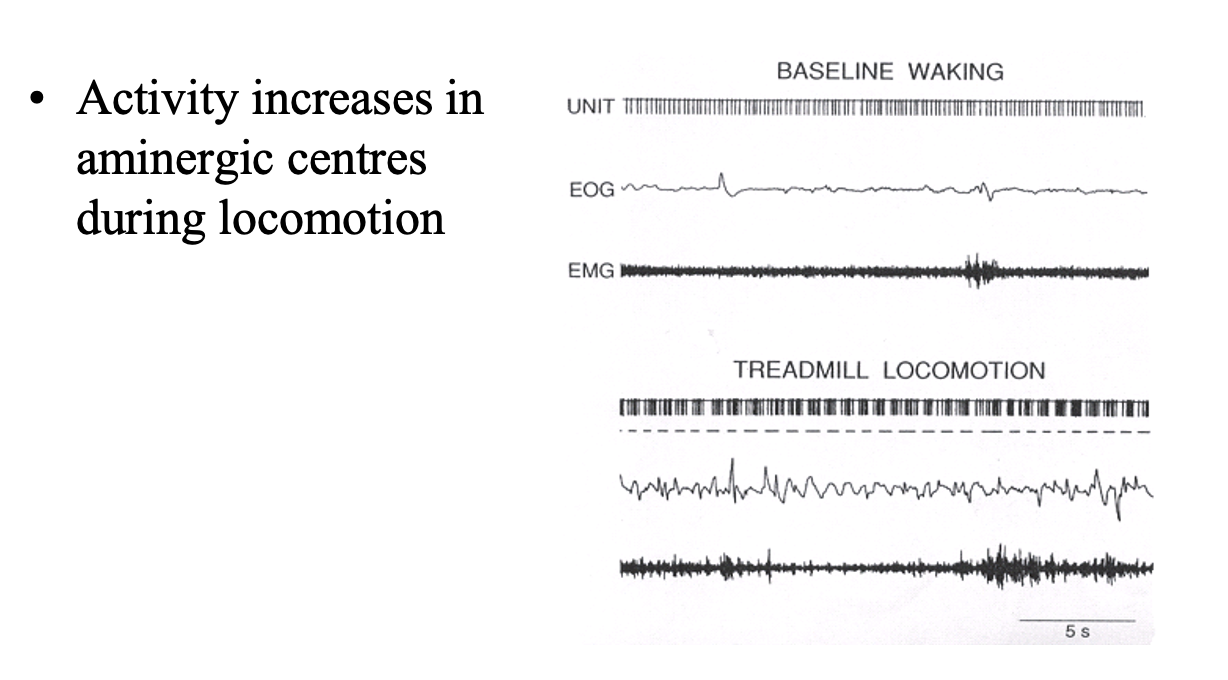
Descending modulatory pathways are activated when
During locomotion
degree of activity increases as the demands of the task increase
At rest→ Raphe neurons fire tonically at low frequency
During locomotion→ high freq burst of APs develop (this is most effective in releasing amines and neuropeptides)
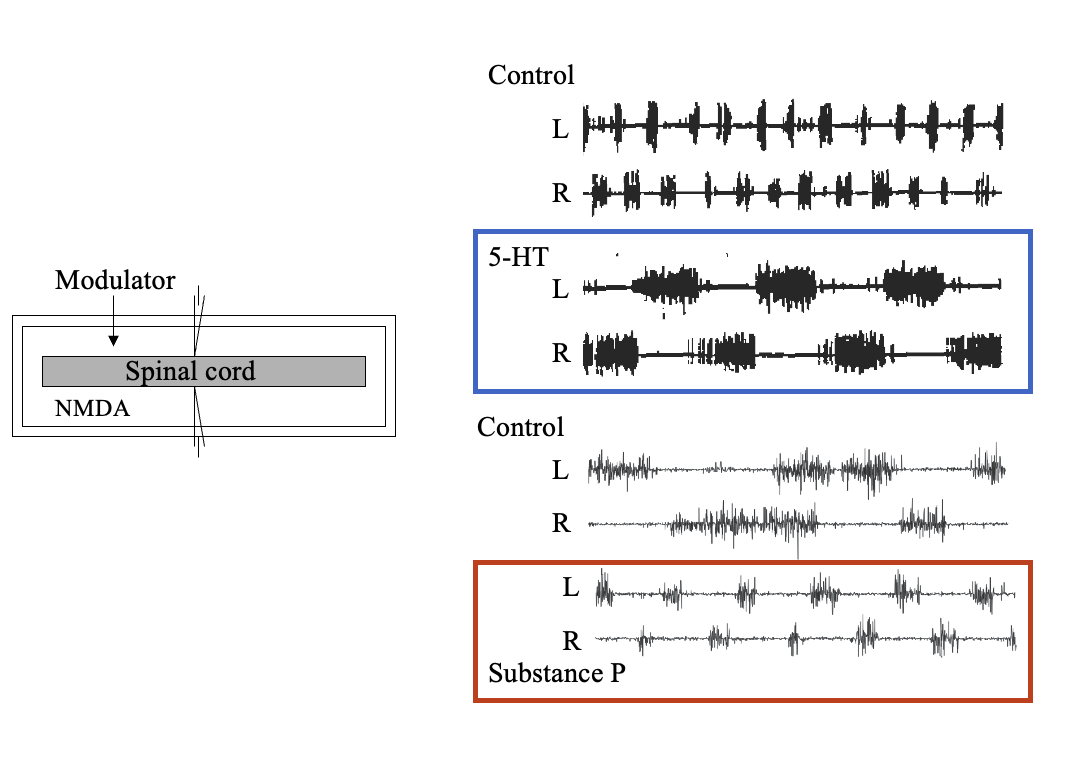
Modulatory effects of transmitters released by slow descending pathways on the activity in spinal CPGs have been studied using
Fictive locomotion:
Procedure:
add NMDA to switch spinal cord on
Add whatever transmitter you are interested in
Results:
5-HT→ slows the locomotor activity in the lamprey locomotor CPG
(the network was activated by the glutamate receptor agonist NMDA applied to the isolated spinal cord)
substance P (neuropeptide)→ increase the freq of network activity and better coordinated
Therefore this shows:
descending systems can use transmitter systems that act on the locomotor network to very the output of the locomotor CPG
How is this modulation happening?
Modulatory transmitters and their receptors alter the properties of neurons in the spinal CPG to functionally recoonfigure the CPG:
Altering different tpyes of neurons
THEREFORE→ alters the motor output
How are a large number of spinal motor patterns from a single hard-wired network provided
larger number of transmitters in descending pathways
different types of receptors that they act on (over 30 5-HT receptors)
How do spinal cord injury show the role of descending inputs to the spinal cord
injury→ paralysis and other dysfunction (spasticity, chronic pain etc)
where the descending inputs have been lost
therefore: shows how descending inputs are needed to activate and modulate locomotor activity
therefore: to treat spinal cord injury→ need to attempt to restore these inputs
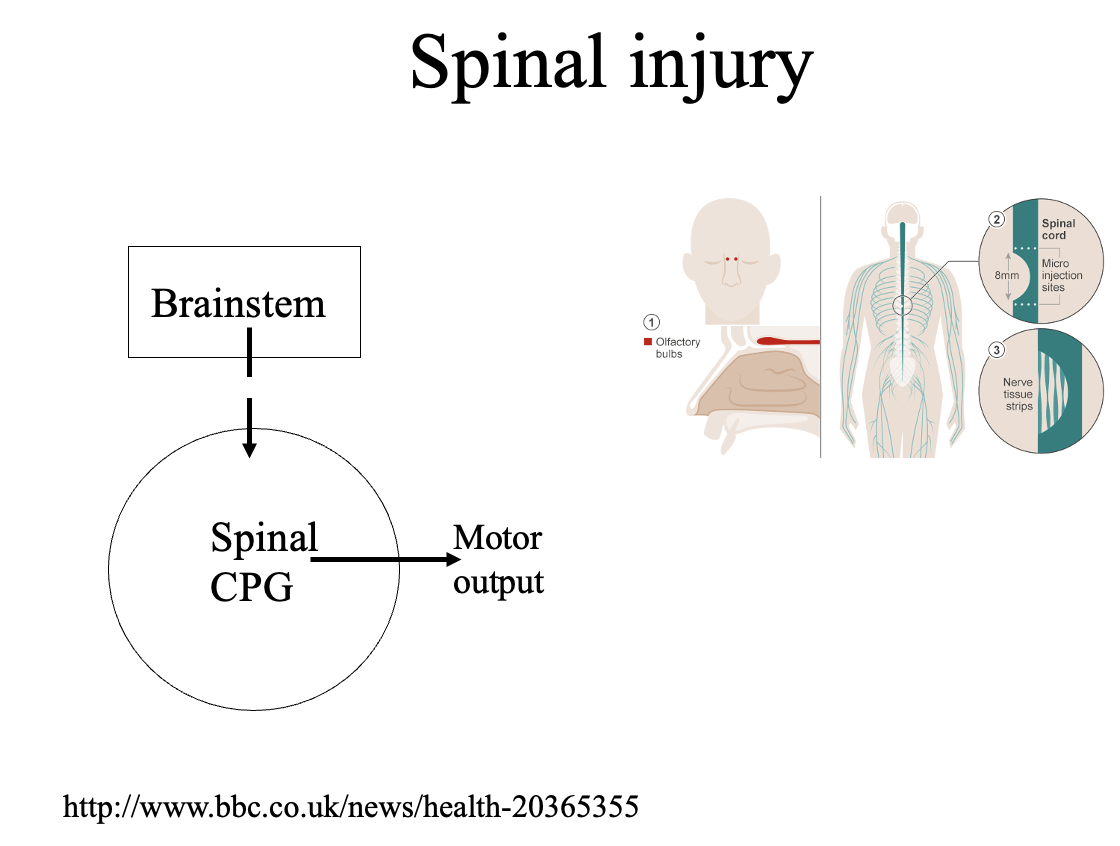
Effective treatment→ making axons grow?
neurons can regrow
however→ they are inhibited (we do not know why)
need to find inhibitory factors and switch them off
e.g Olfactory neurons re-grow when they are made from the nasal epithelium down a permissive pathway
cells that allow the axons to grow→ chiefing cells?
can transplant these in and see what happens
some evidence for this but not been translated to effective treatment so far
What happens to the locomotor networks in the spinal cord below the lesion site
not lost after injury
but the lack the input needed for their activation and modulation
Therefore this suggested some therapeutic options:
the role of drugs in activating (e.g glutamte) or modulating (5-HT) locomotor CPGs
suggests that drugs that mimic effects of transmitters released naturally from descending neurons could help compensate for the effects of spinal injury
Results: using 5-HT or glutamte agonist as therapy
in cats→ improve locomotor performance
sifure shows movement of the limbs and muscle activity in an intact animals
with receptor complete spinal lesion and in the same lesioned cat 2 min after applying noradrenergic agonist clonidine
RESULT→ dramatically improved the locomotor pattern
BUT→pharmological approaches have had mixed success
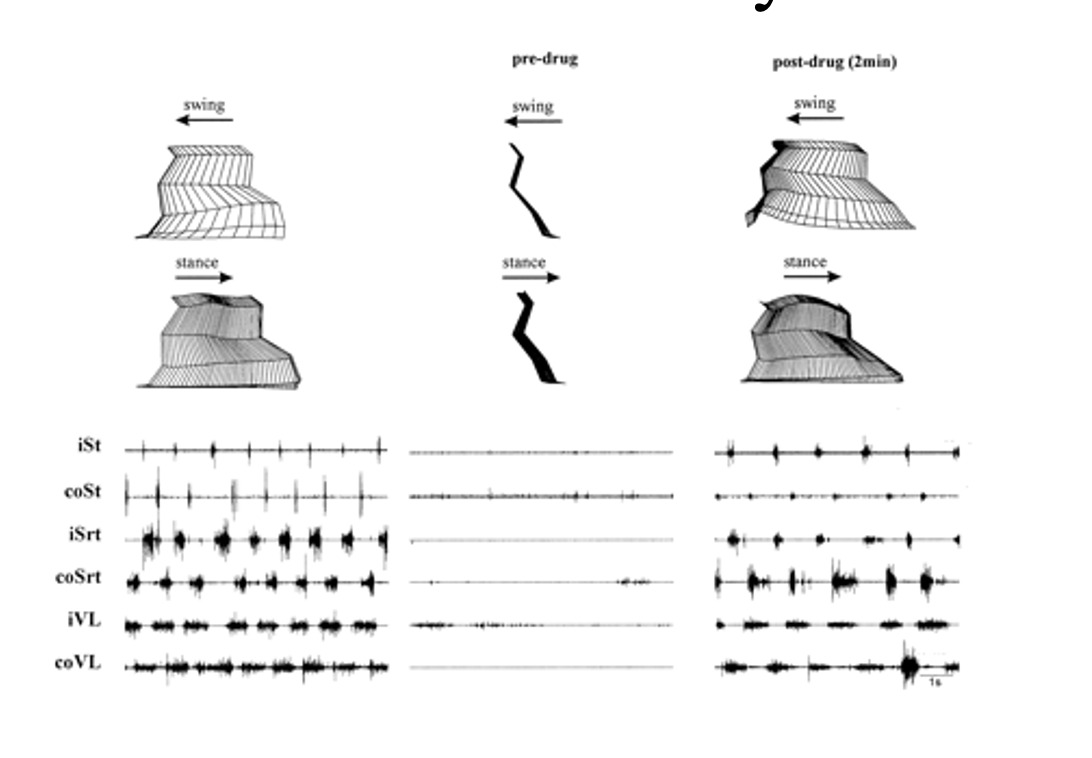
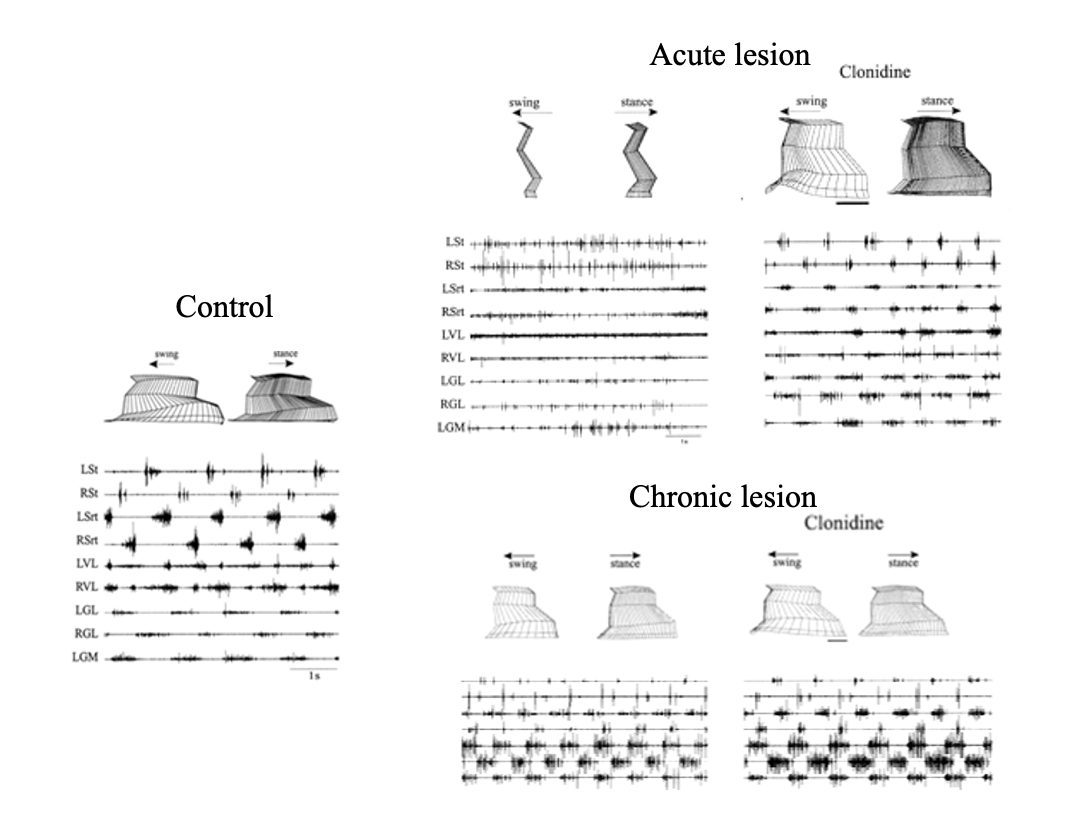
There is considerable variability in drug effects depending on
extent of injury
time after injury→ Chlonidine is only effective soon after a spinal lesion (acute vs chronic lesions)
Reliable experimetntal effects may not be translated to the clinic
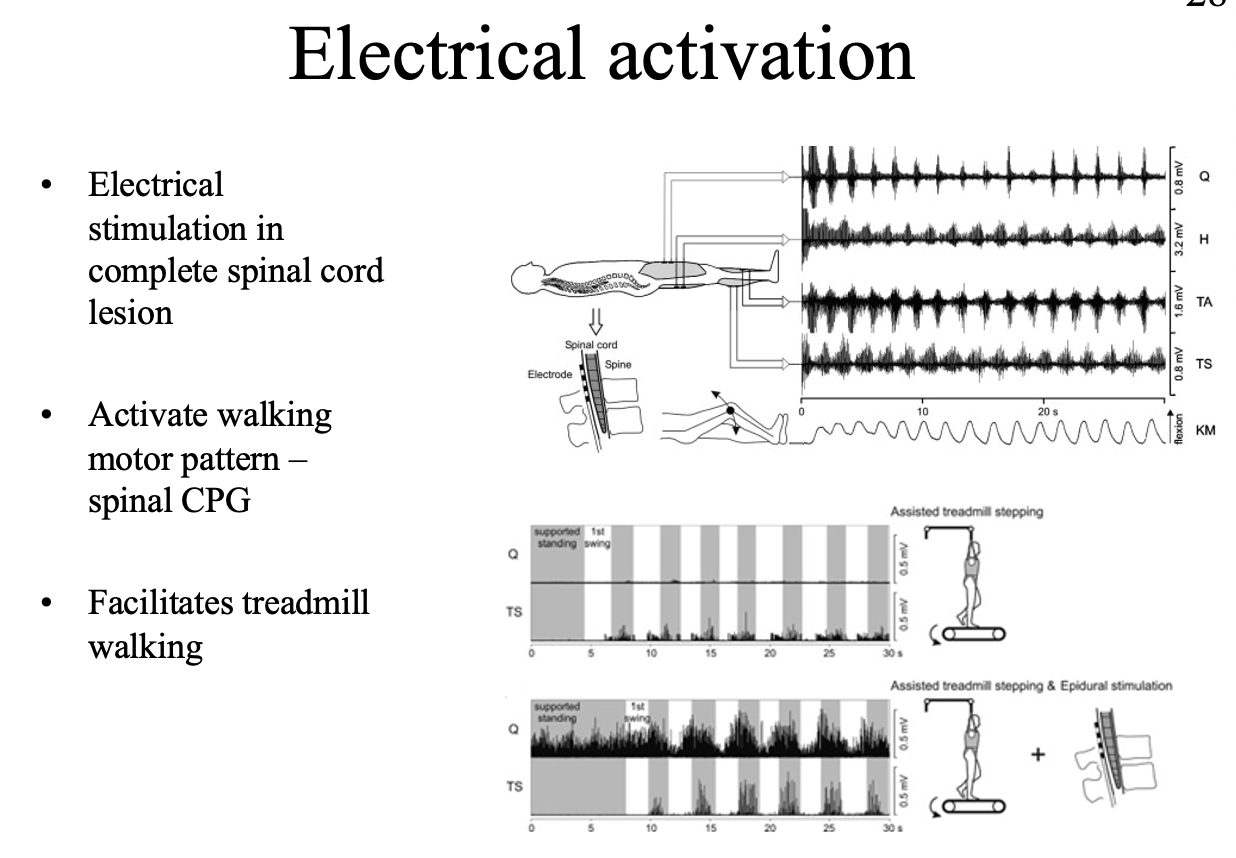
What else can be used as a treatment?
Electrical stimulation:
stimulation to substitude for descending inputs
BUT→ to generate actual locomotion some connection to the brain is needed
Therefore what does this suggest is needed for therapy
combination of
regeneration with pharmalogical and electrical stimulation and locomotor traning tailored to the specific needs of individuals
Overall why is is so difficult to get these threapies to work
Heterachy network:
cannot just dump in a load of stem cells/ NTs etc
complex network that has to be re-wired
Summary of descending inputs
Descending pathways convey supraspinal signals to spinal CPGs to influence the development and function of spinal networks.
Ventromedial systems are principally concerned with control of proximal muscles.
Dorsolateral systems are principally concerned with control of distal muscles.
Slow pathways have global modulatory effects.