Anesthesia CP 1 Exam 3
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
#1
Compressed O2 tank
green drop line
holds pure oxygen which is carrier gas
2,200 psi
#2
Pressure Regulator
reduces and controls amount of oxygen leaving tanks
3
pressure gauge
tells amount of O2 in tank
if tank is below 500 psi start watching
4
O2 flow meter
looks like thermometer
controls amount of O2 to patient
connected to vaporizer
L/min
stop turning when ball reaches bottom to turn off (do not tighten)
never set O2 meter below 0.5 L/min causes vaporizer to not work properly
5
O2 flush
bypasses vaporizer
allows delivery of pure oxygen to patient
6
vaporizer
hold liquid GA
vaporizes and delivers precise amounts of GA to patient
in %
isoflurane and sevoflurane most common GA
6A
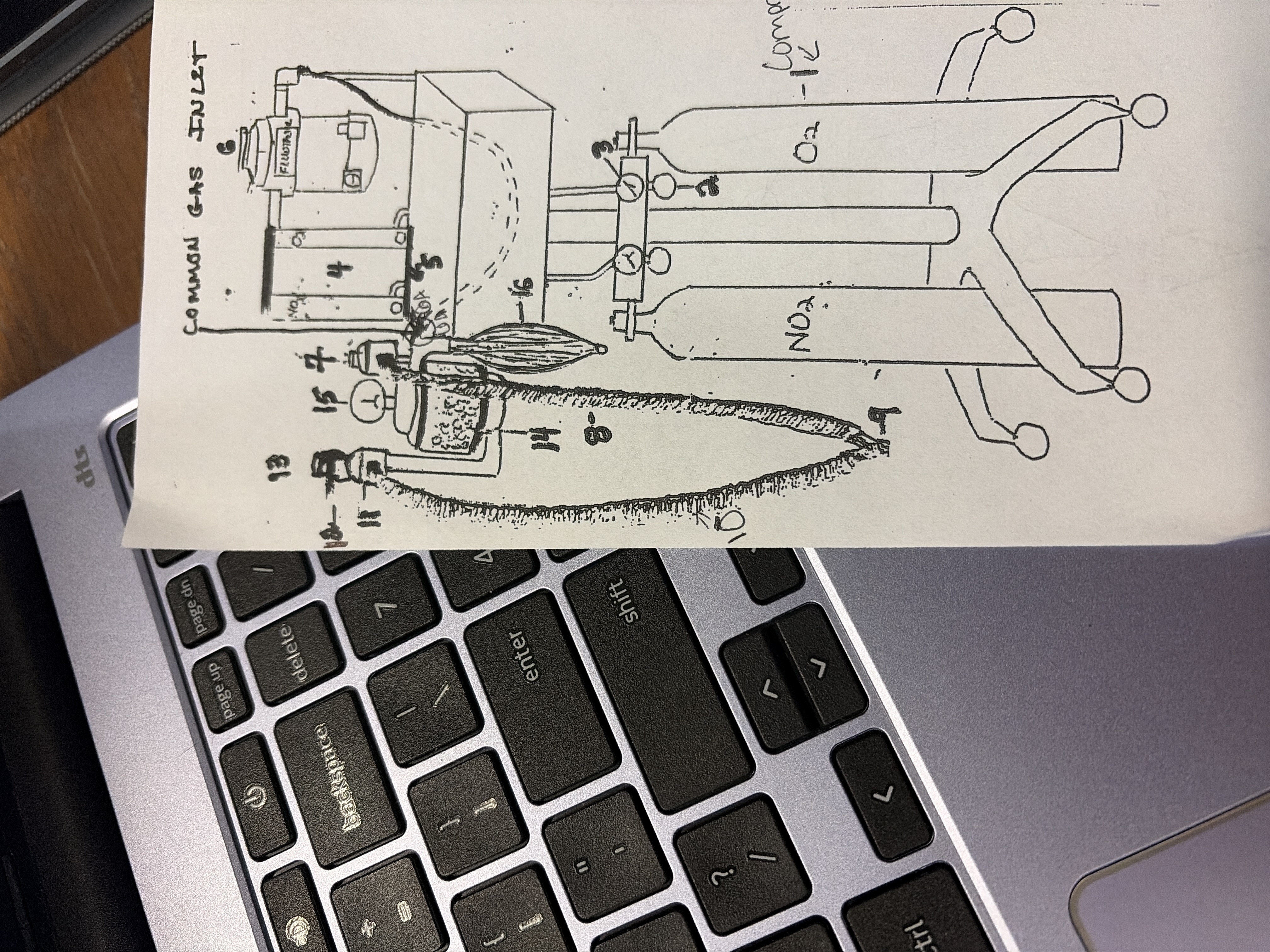
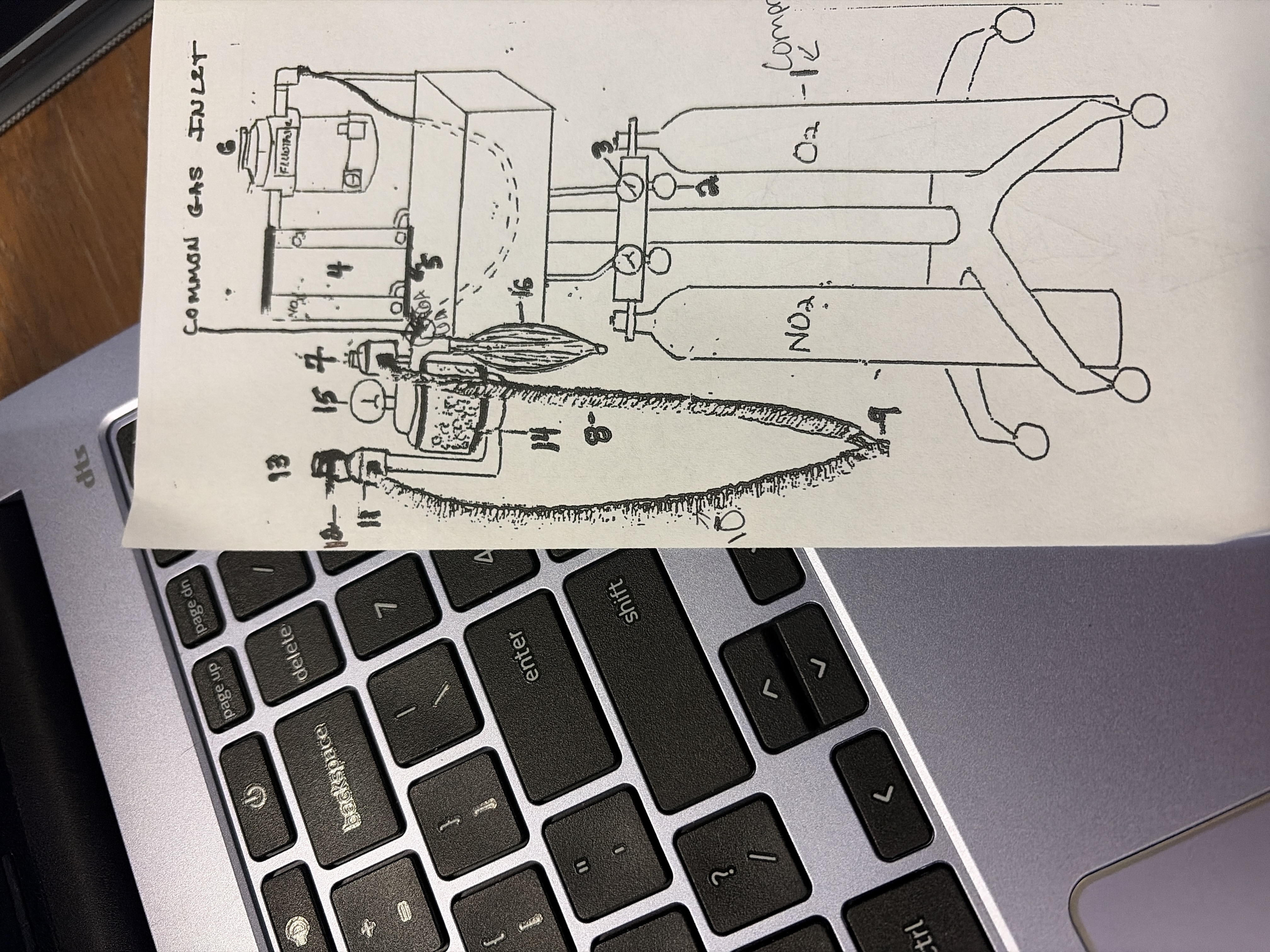
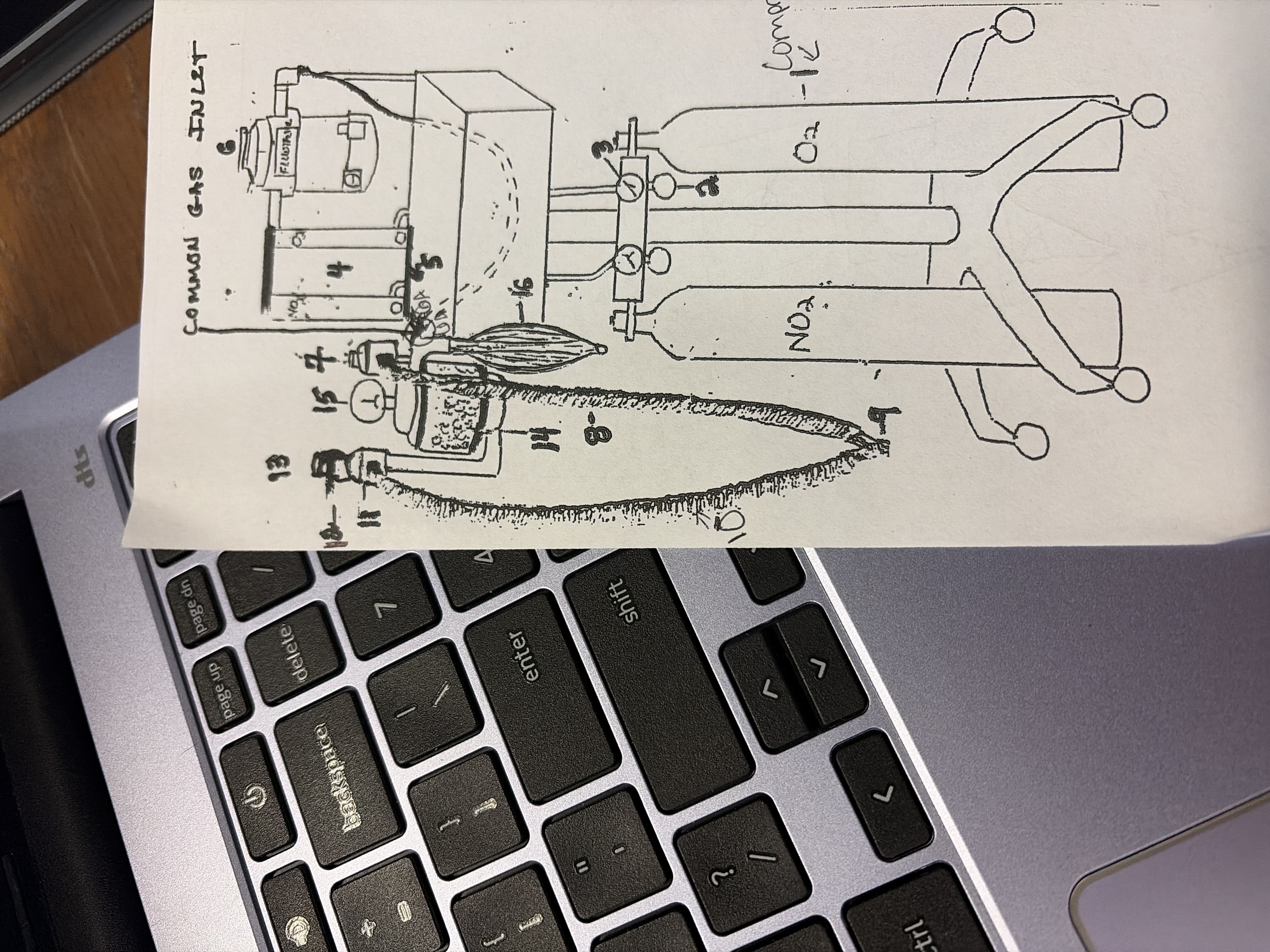
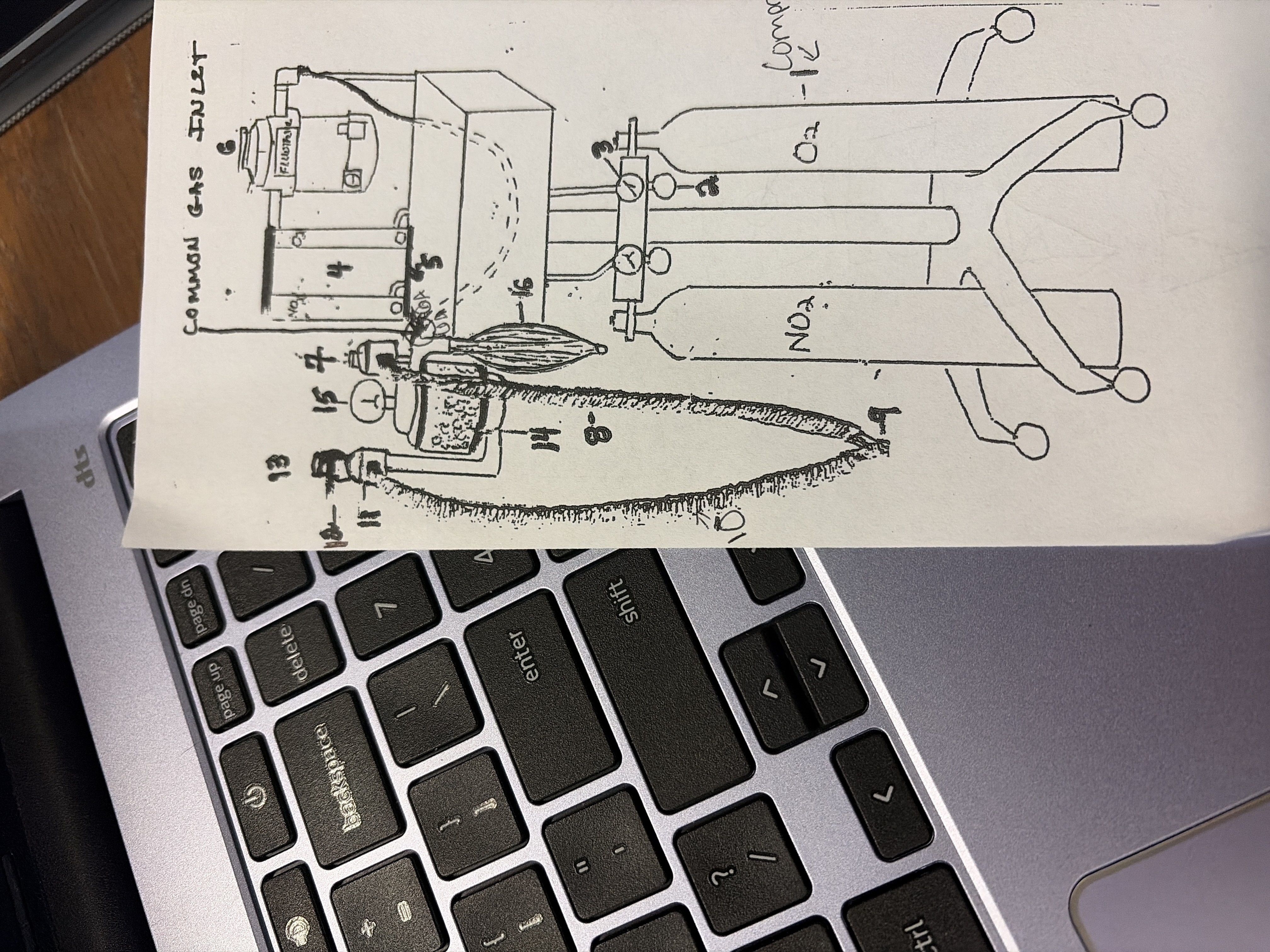
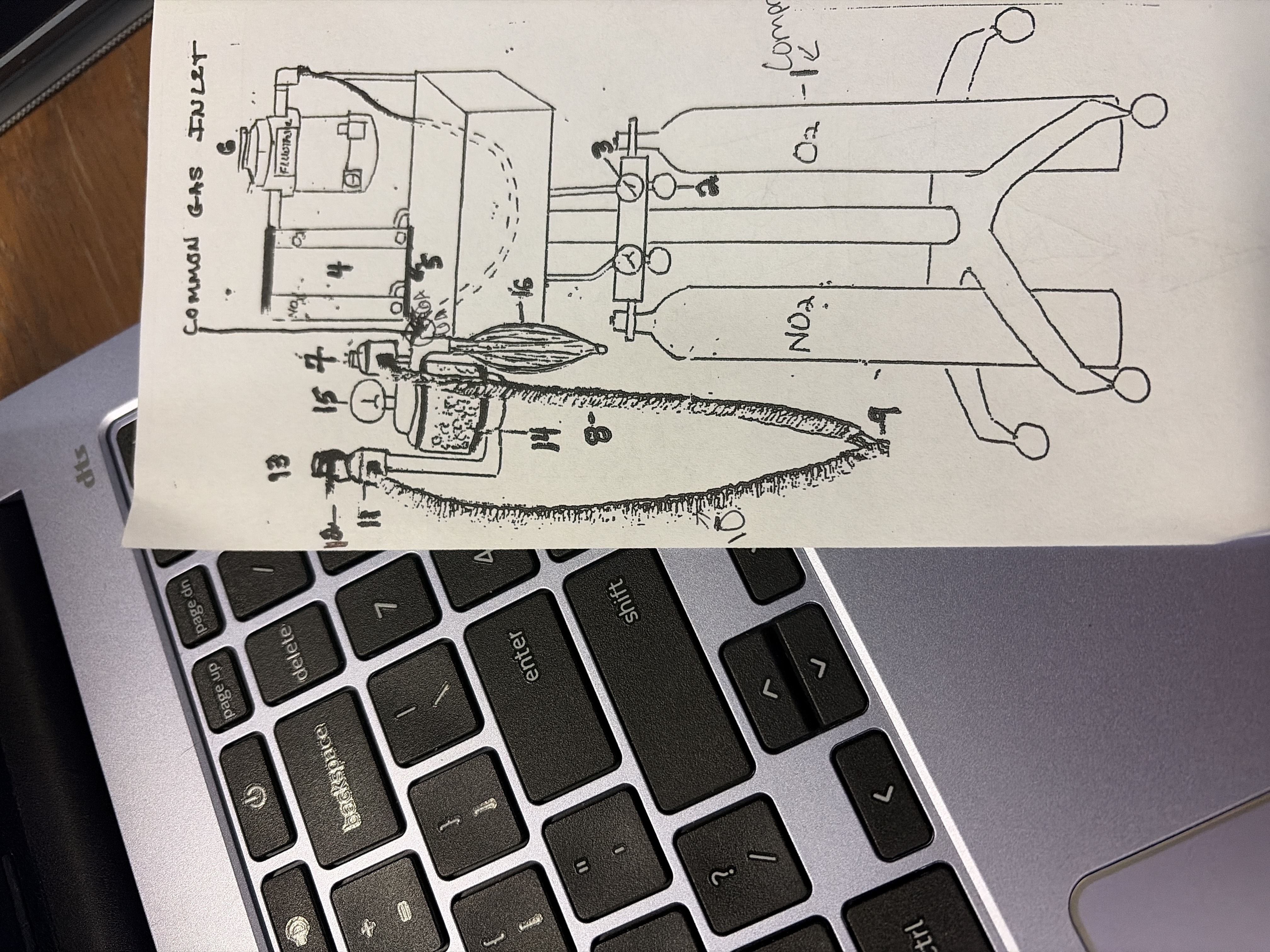
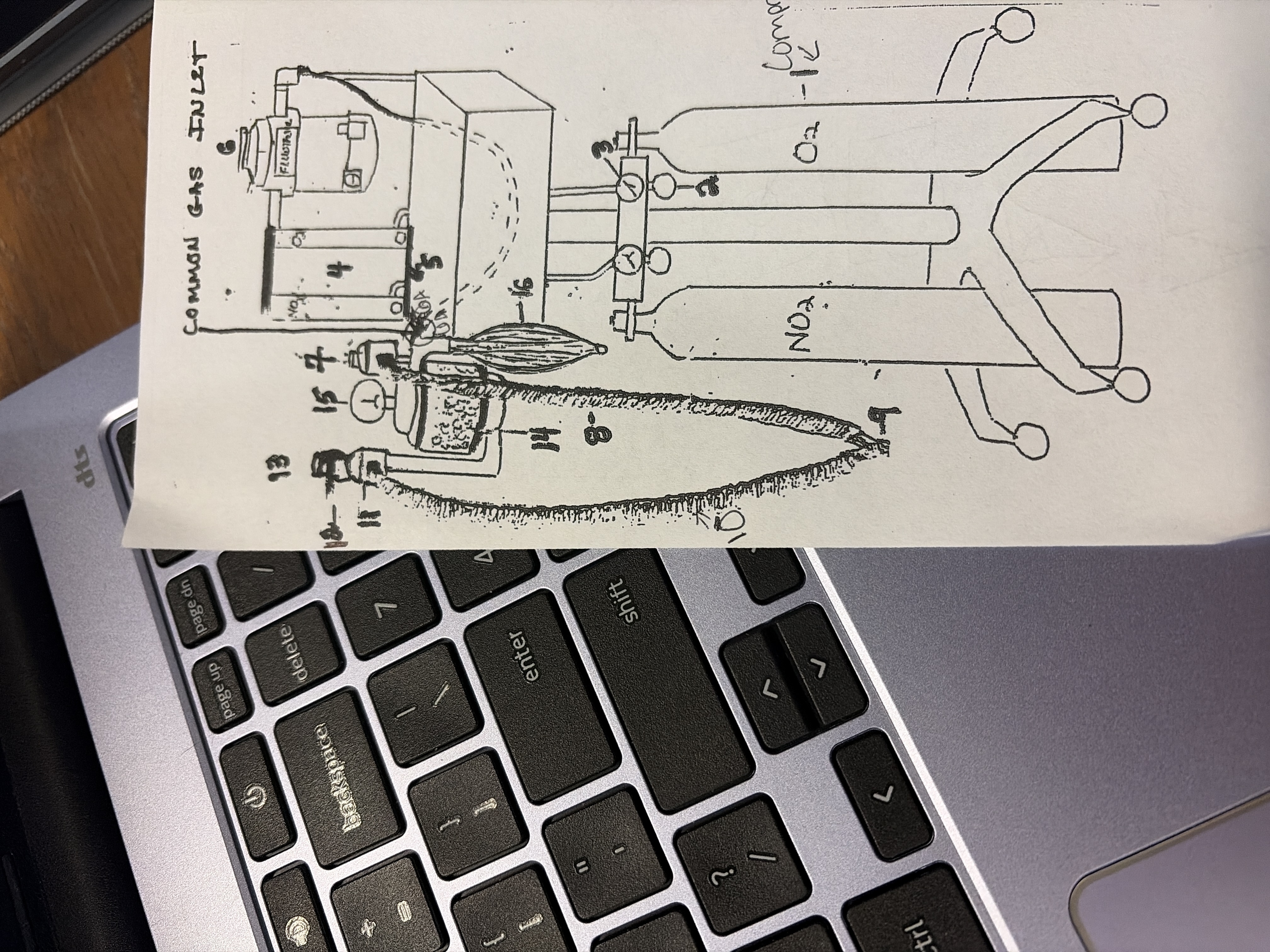
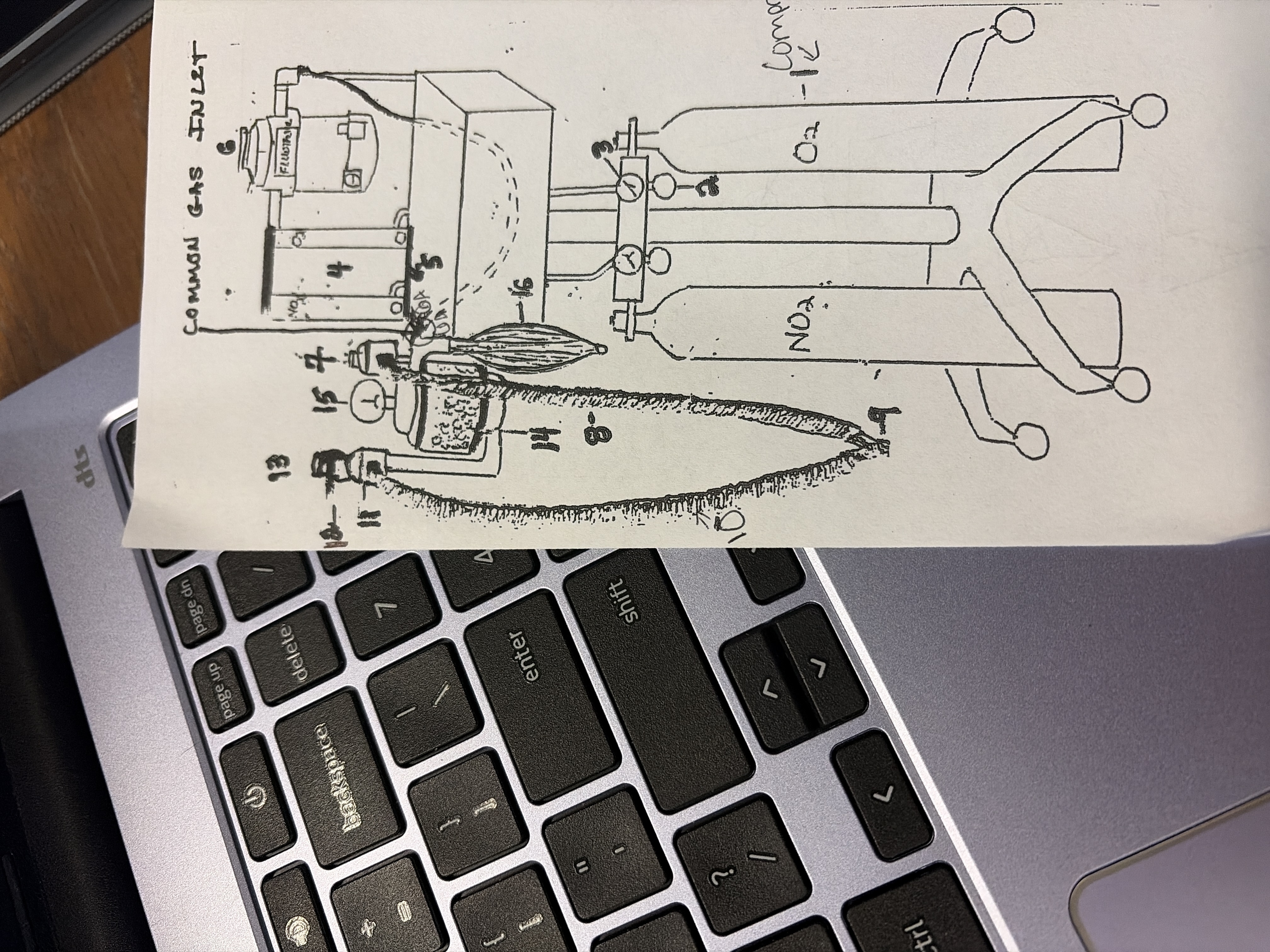
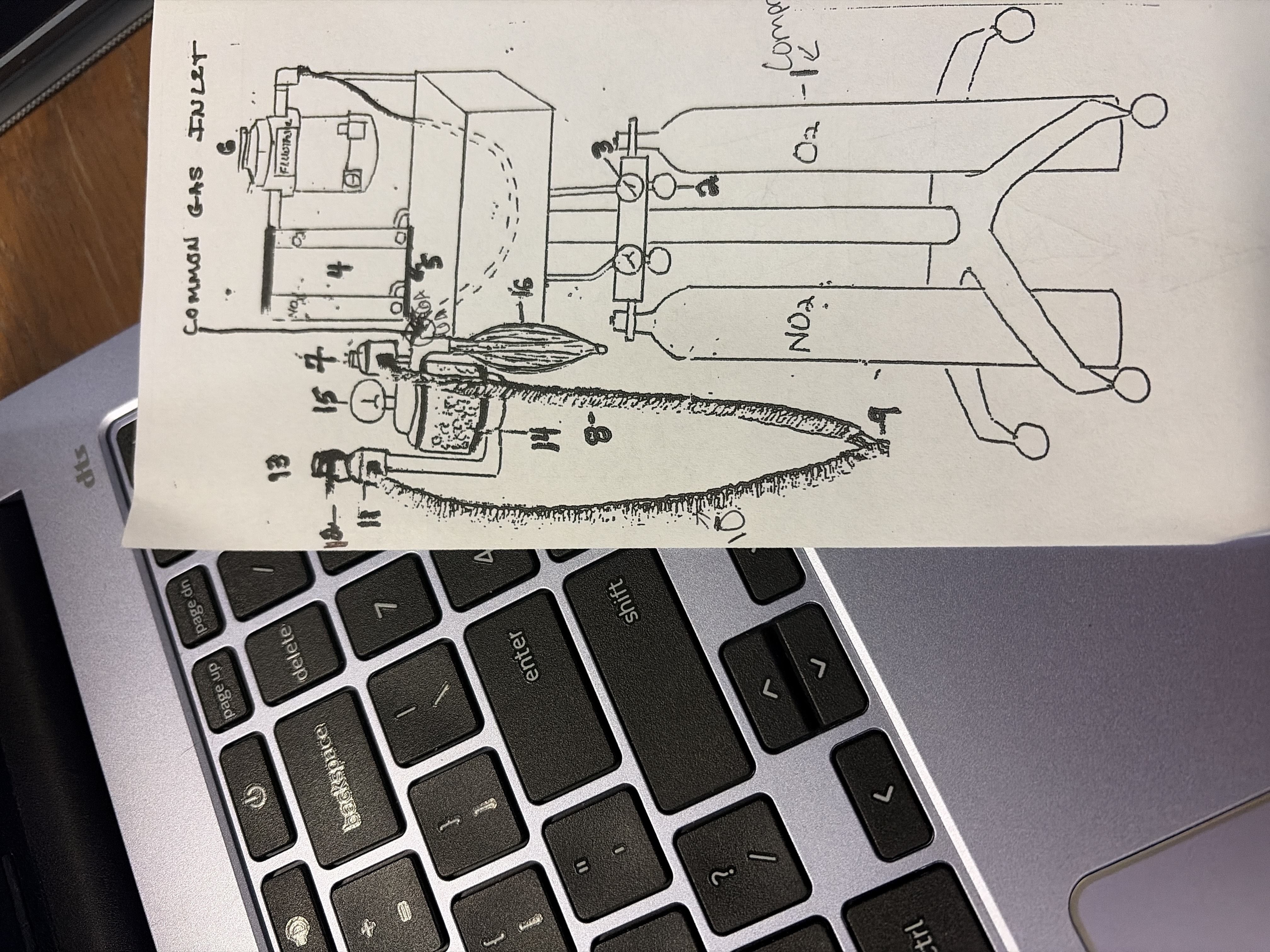
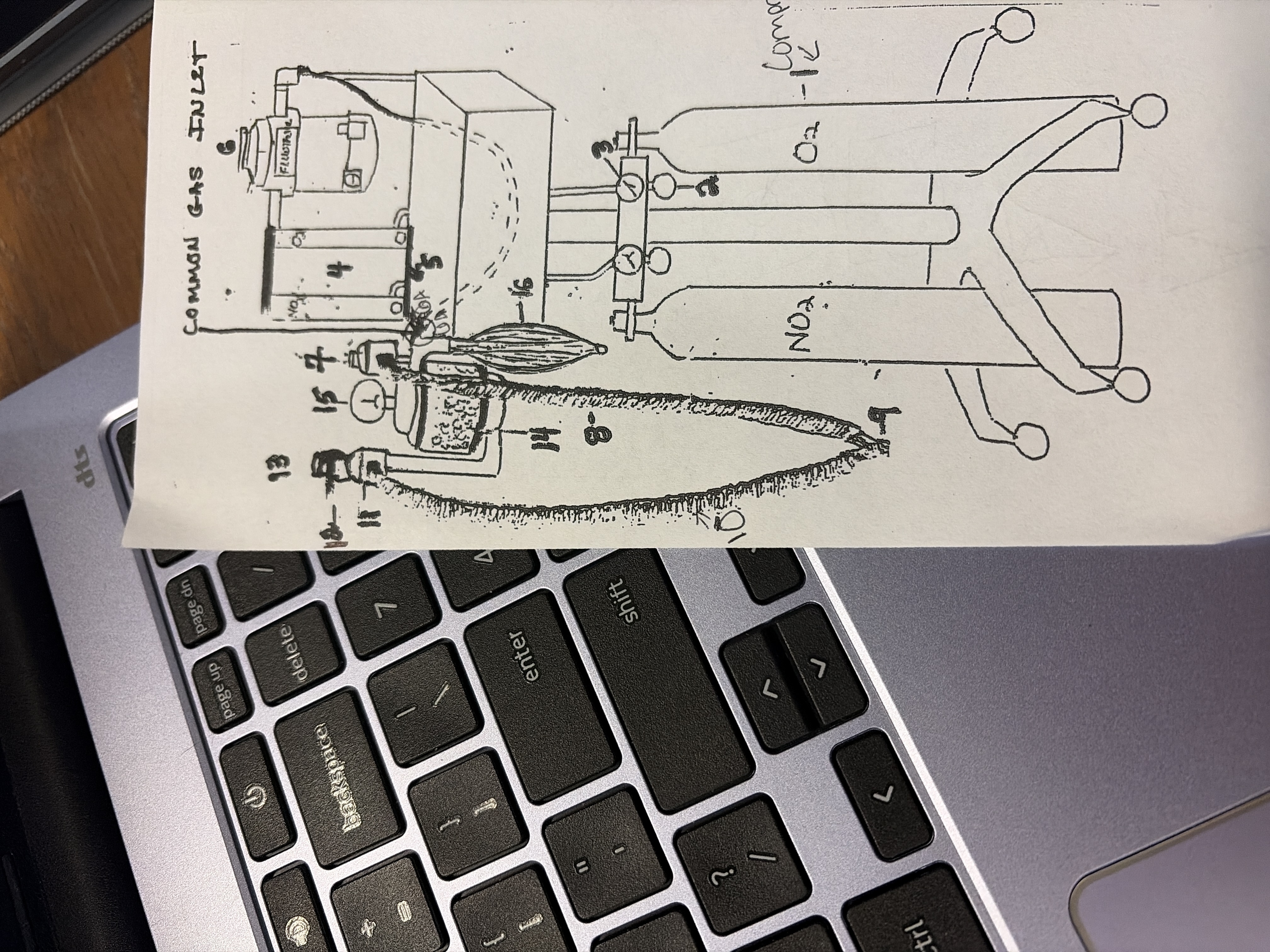
Common gas inlet
port below inhalation valve
shared pathway for pure O2 from O2 flush and GA mixture from vaporizer
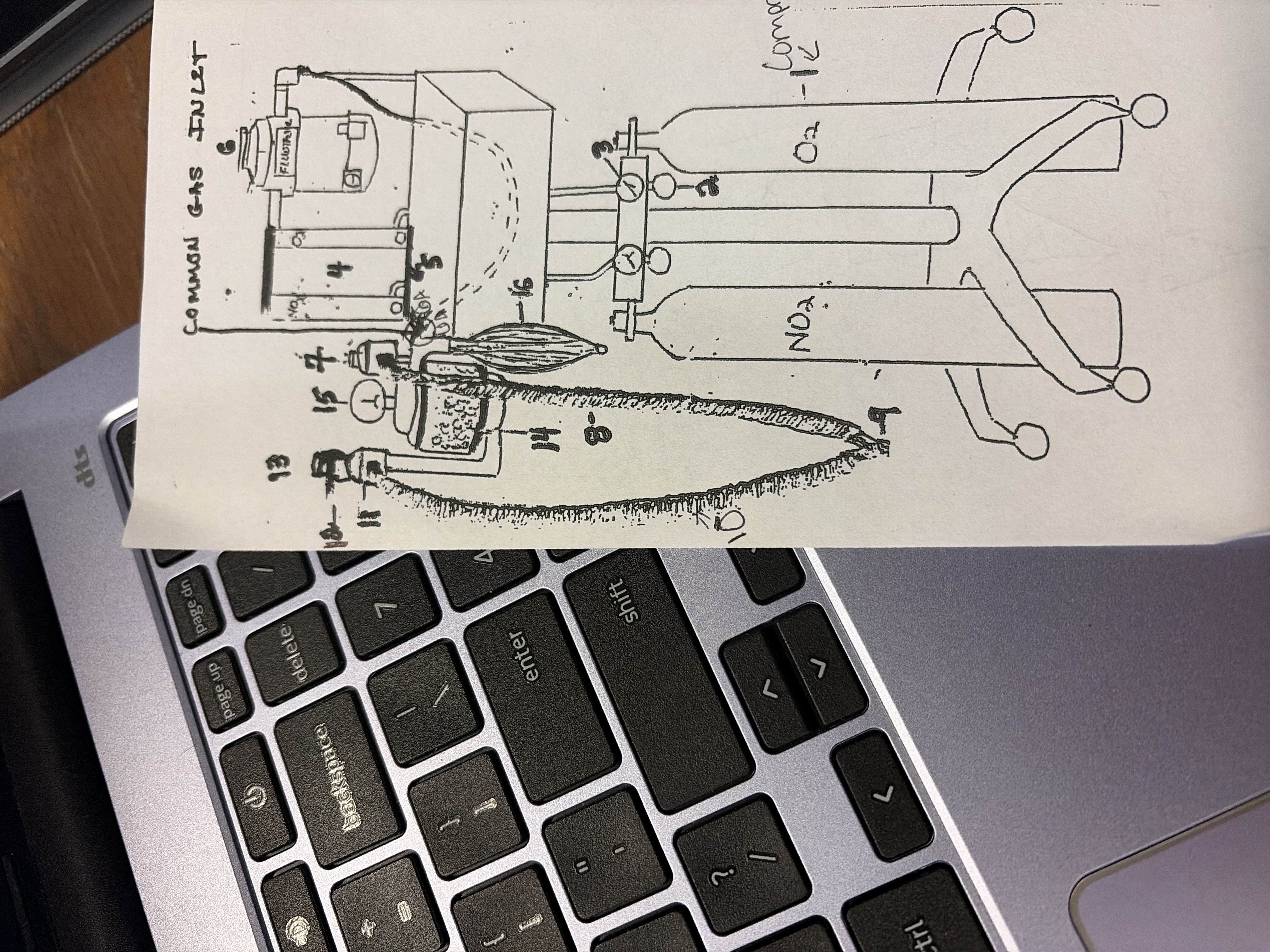
7
unidirectional inhalation flutter valve
ensures one way flow of gasses towards patient
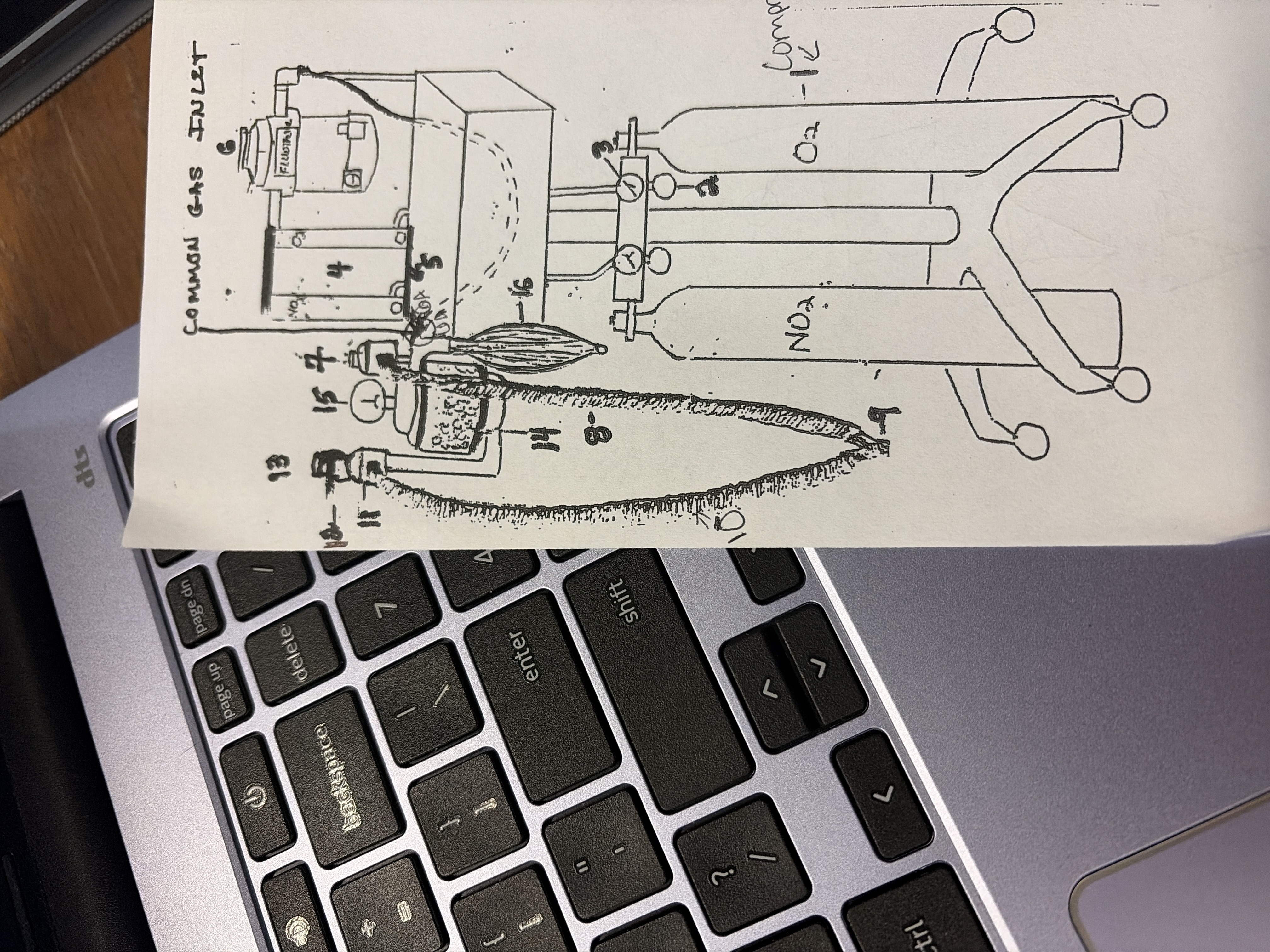
8,9, 10
Breathing circuit
inhalation tube 8
y piece 9
exhalation tube 10
carries gases to and from patient
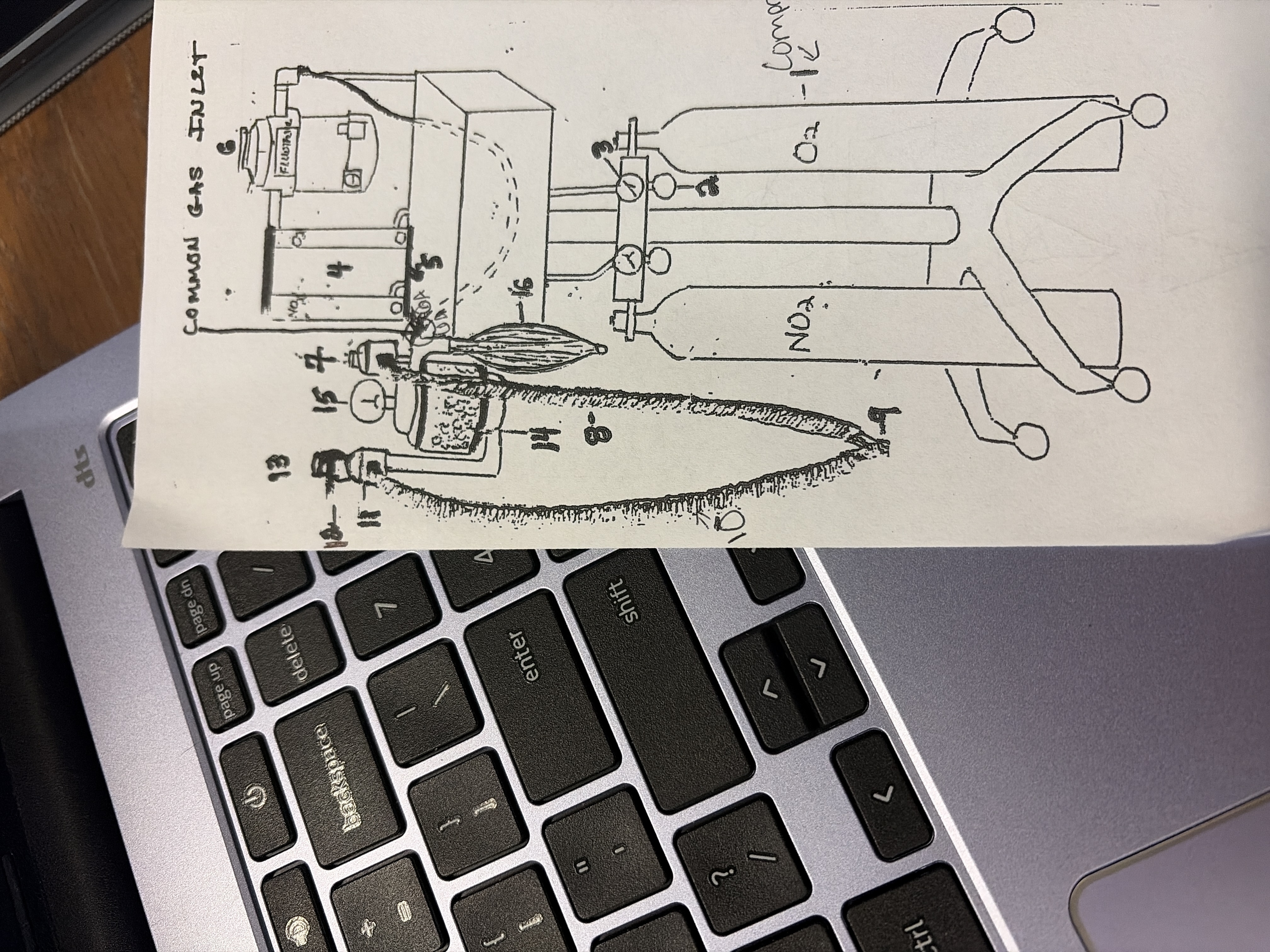
11
unidirectional exhalation flutter valve
ensures one way flow of gases away from patient
12
scavenger port'
exit for waste gases
Active- vaccuum system
passive- F/AIR container
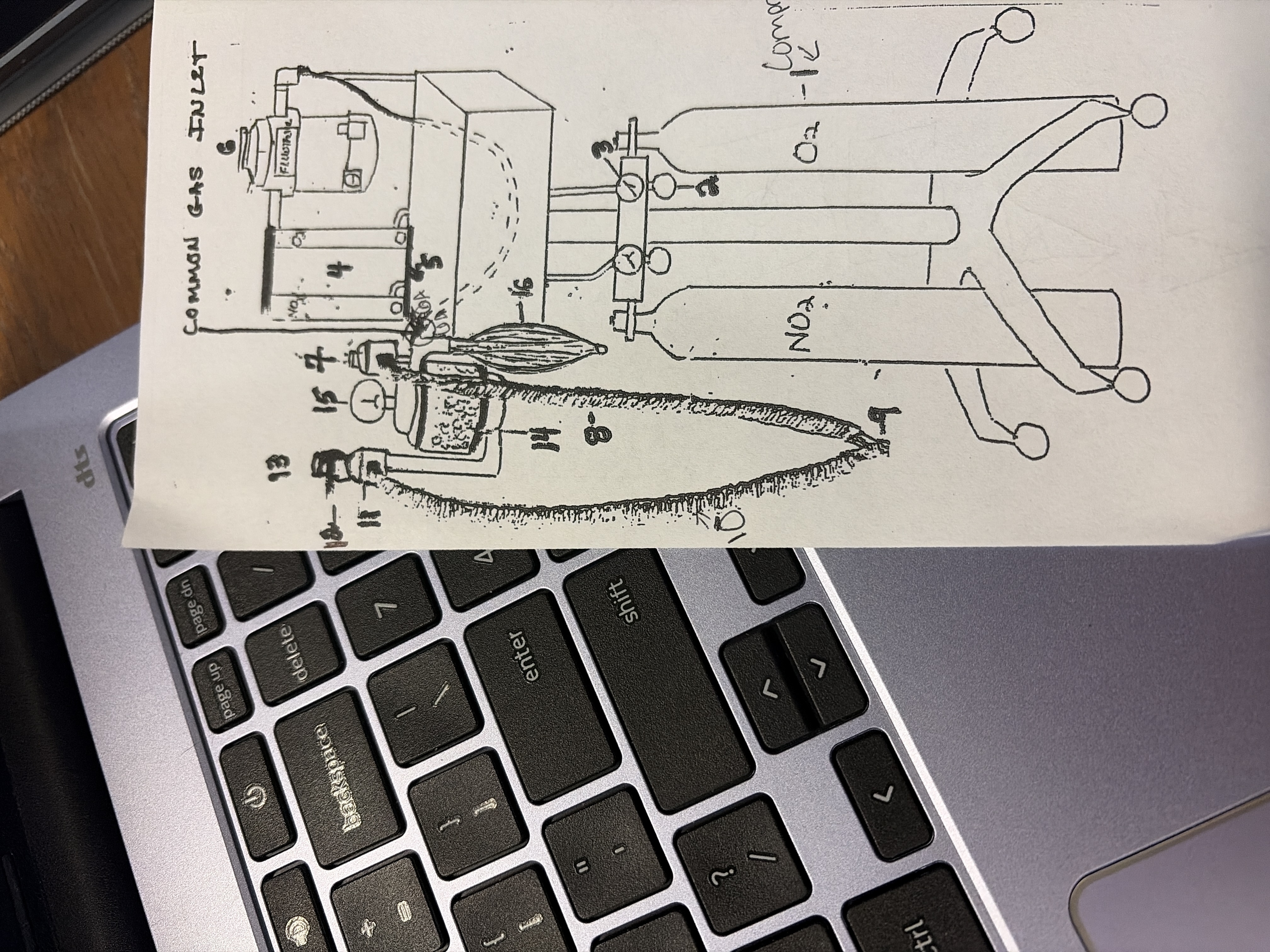
13
Pop off Valve
position determines how much of exhaled gases go out to scavenger and CO2 absorber
Close- only CO2 absorber
do not run anesthesia with closed bc of CO2 toxicity
Open- allows access to CO2 absorber and scavenger
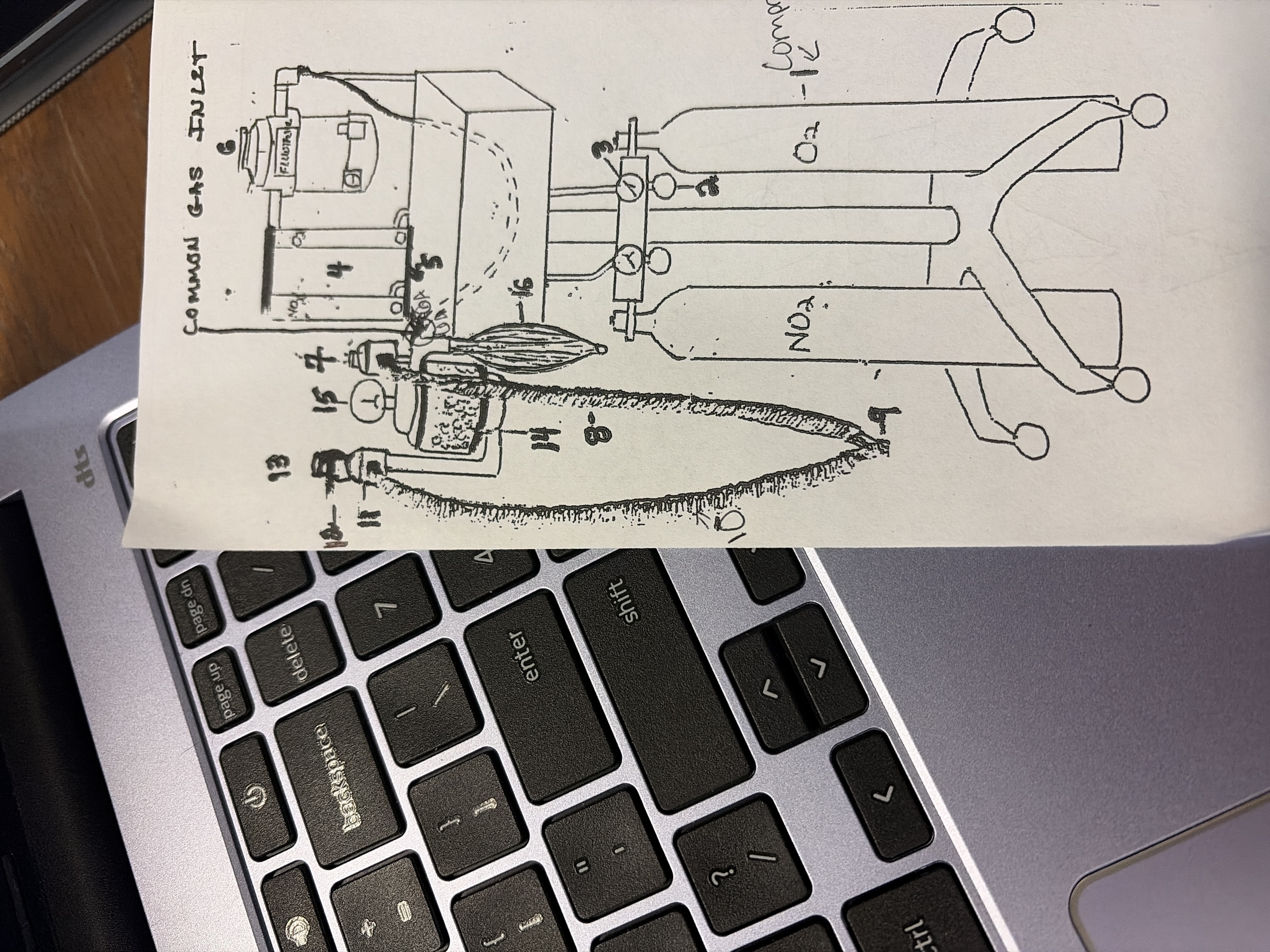
14
CO2 absorber
granules absorbs CO2 from gases exhaled by patient so that GA gases can be recycled
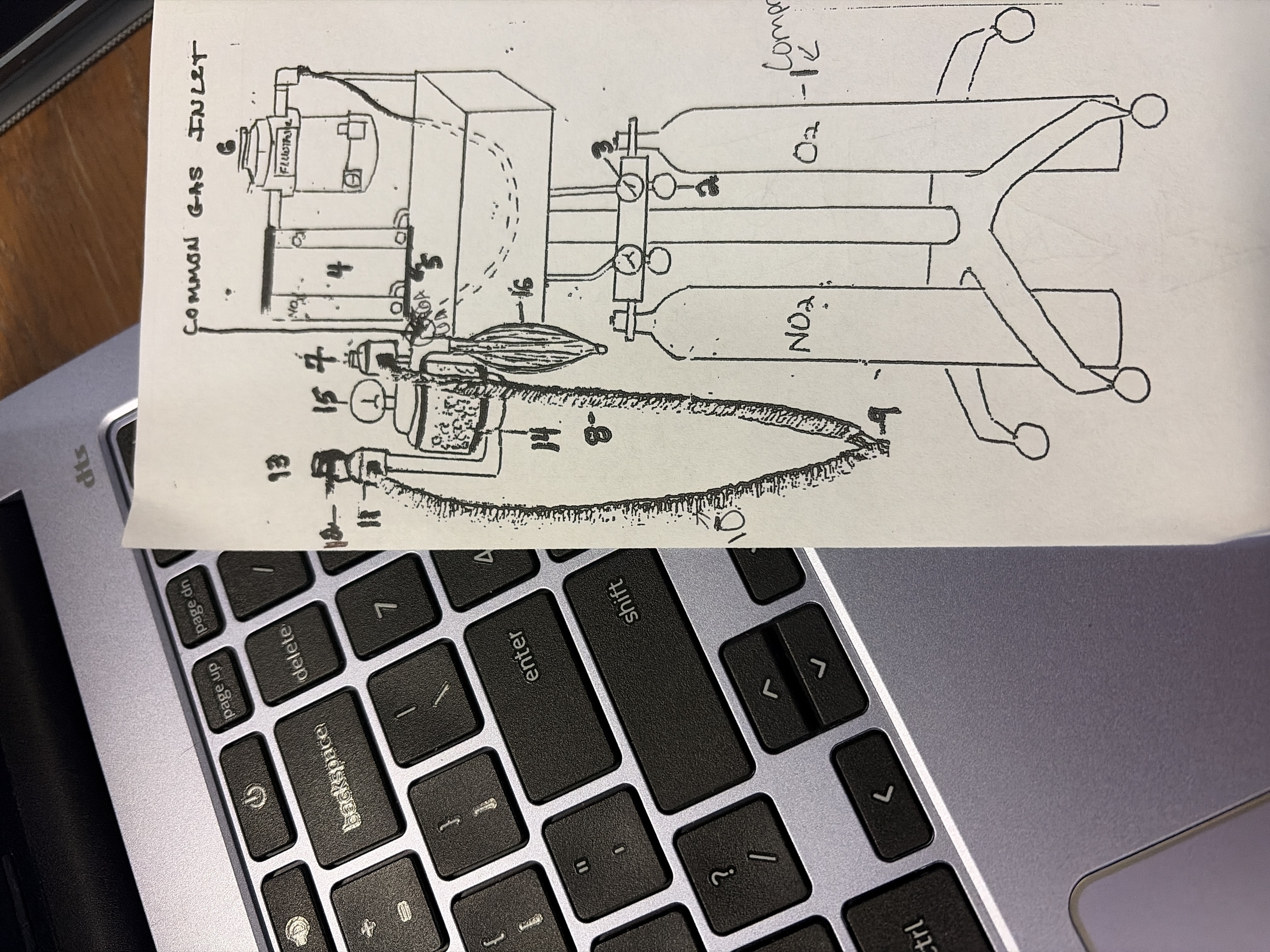
15
pressure manometer
tells how much pressure in breathing circuit
never go above 20 cm of water
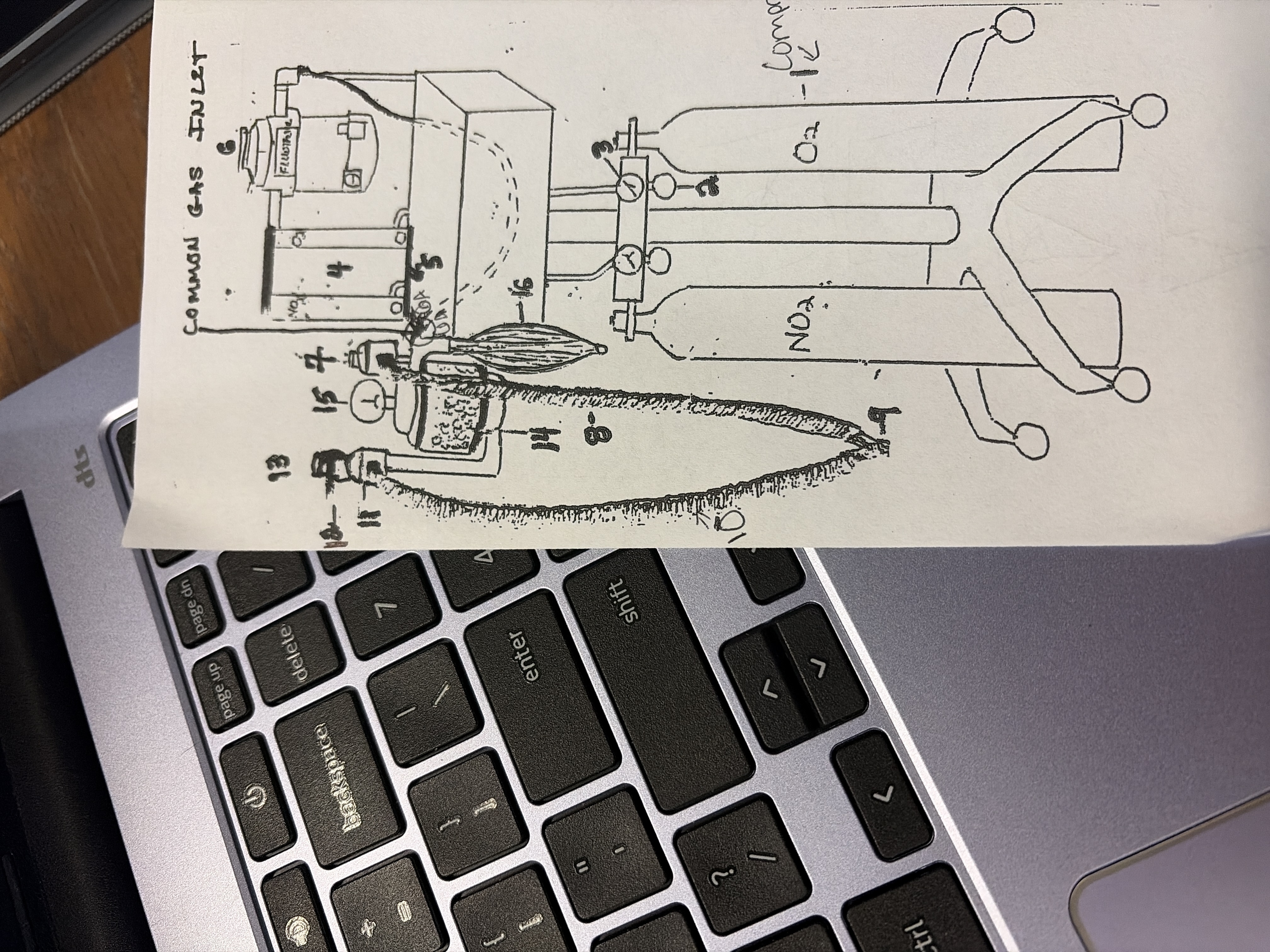
16
rebreathing/reservoir bag
liter bags
reserve for gases
never be empty or overly full
also helps tell excessive pressure in system
Reasons to bag/ventilate
prevent atelectasis (collapsing of alveoli) occurs when taking smaller breaths not using them can cause loss
remove any buildup of CO2 in lungs
rescue breathing for animals in respiratory arrest (close pop off valve, give pure O2)
How to bag
bag every 5-15 min
do not squeeze too much
bag with O2- become lighter
bag with GA- go deeper
Circle rebreathing
patients over 15 lbs
partial rebreathing of exhaled gases
pop off open
requires all components of machine
30 mL/kg/min O2 flow rate
slow change in anesthesia
less costly
low waste
good with heat and moisture conservation
non rebreathing
patients under 15 lbs
only requires O2, Vaporizer, and scavenger
O2 flow rate: 100-300 mL/kg/min
fast change in anesthesia
costly
high waste
poor heat and moisture conservation
anesthesia
total loss of sensation in a body part or entire body resulting from administration of a drug that supplies the activity of part or all of nervous system
general anesthesia
loss of sensations in the entire body
local anesthetic
loss of sensation in a body part
Anesthesia uses
restraint
elimination of pain
seizure control
humane euthanasia
pre-anesthetics
pre meds
calms patient
induction agents
render unconscious
maintenance agents
maintains unconsciousness
Why do you want to use a combo of anesthetic drugs
to eliminate unwanted side effects
Drug categories
anticholinergics
tranquilizers
sedatives
opioids
dissociative agents
gas anesthetics
pre-anesthetic reasons
aid restraint
reduce anxiety
smooth induction and recovery
less need for potentially more harmful drugs
counteract undesirable effects of concurrently used drugs
Anticholinergics (6)
prevent or reduce brachycardia (they increase HR)
prevent excessive salivation and reduce upper airway secretions (drying effect)
do not affect level of consciousness
do not provide analgesia (pain relief)
LA- ruminants- contraindicated (not used) bc of worry of thickening airway secretions and making obstructions
Horse- contraindicated bc can mess up GI tract (avoid cholic)
Popular Anticholinergics (2)
Atropine- cheaper
Glycopyrolate- expensive, longer duration, less risk of cardiac arrhythmia, does not cross placental barrier, and less suppression of GI tract
Tranquilizers (3)
aid restraint
reduce anxiety
reduce struggling (slows motor activity)
popular Tranquilizers (2)
Acepromazine (phenothiazine family): does not provide analgesia, contraindicated in patients with liver disease and history of seizures
Benzodiazepine family (diazepam, midazolam, zolazepam): not used alone (hyperexcitability), enhances effects of opioids, enhances muscle relaxation, minimal cardiopulmonary effects, anticonvulsants (stops seizures) (good for pediatrics, geriatrics, and cardiac patients
Sedatives (5)
drowsiness
muscle relaxation
analgesia
significant cardiac effects
decreased thermoregulation
popular sedatives (2)
xylazine - LA reversal yohimbine
dexdomitor: SA reversal: antisedan (commonly drops HR below minimally acceptable)
minimal acceptable HR
dogs: 60 bpm
cats: 100 bpm
Opioids (8)
powerful analgesics
sedation
used in pure form
can cause excitibility on own
bradycardia
causes respiratory depression
apnea
decrease thermoregulation
popular opioids(4)
fentanyl
hydromorphine
oxymorphone
reversal: nalaxone
neuroleptanalgesia
state of profound CNS depression due to combo of opioid with tranquilizer or sedative
dissociative agents (6)
causes excessive drooling on own
muscle rigidity
superficial analgesia
only used alone to immobilize fractious animals
light and noise sensitive
avoid with liver and kidney disease
popular dissociative agents (2)
ketamine- stimulates multiple areas of brain (do not use with seizures)
tiletamine- mixed with zolazepam (also called Telazol)
Induction Agents (7)
propafol (only thing given IV that is not clear)’
rapid loss of consiousness
rapidly metabolized
can rapidly wake up
given slowly to effect
transient cardiopulmonary depression dependent on dose
apnea
Gas anesthetics (9)
isoflurane and sevoflurane most common
maintains unconsciousness
can induce using GAs alone (not common bc of excitement stage)
eliminated with exhale (not metabolized)
any animal with good lungs can use
provides analgesia until woken
significant drop in HR and RR
requires machine
Sevoflurane is more potent and works quicker
Stage 1 (5)
disoriented
normal RR and HR
eyeball central
light response
good muscle tone and reflexes
Stage 2 (5)
excitatory stage
irregular respiration
HR may increase
eyeball central (possible nystagmus)
possible exaggerated reflexes
normal HR
Dog- 60-160 bpm
cats- 140-220 bpm
normal RR
dogs- 10-30 brpm
cats- 20-30 brpm
Stage 3 Plane 1 (5)
light anesthesia
may respond to movement
central or rotated eye position
light response
good muscle tone, swallowing poor or diminished
Stage 3 Plane 2 (8)
surgical anesthesia
regular RR could be shallow
HR greater than 90 bpm
moderate depth
eyes rotated ventrally
sluggish light response
relaxed muscle tone
some reflexes absent some present (like an ear flick)
Stage 3 Plane 3 (7)
shallow RR
HR 60-90 bpm
deep depth
central eyeball may rotate ventrally
very sluggish or absent light response
greatly reduced muscle tone
all reflexes absent
Stage 4(7)
jerky RR
HR less than 60 bpm
overdose
central eye position
unresponsive to light
flaccid muscle tone
no reflexes
stage 5
death
normal acceptable RR
dogs and cats 8 brpm
cardiovascular system (6)
listen to heart (esophageal stethoscope)
HR and rhythm
brachycardia common
report any arrhythmia
sinus arrhythmia normal in dogs (speed up at inhale, slow at exhale)
Ways to tell Bp: direct measure, mucus membrane color, capillary Refill Time (2 sec or less), pulse strength
depth
shallow/ rapid breaths- too light anesthesia
shallow breaths/ decreased RR- too deep, approaching respiratory arrest
deep/rapid breathing- too light, response to pain (also propafol)
noise
assess any lung sounds
common for cats to build up airway secretions (if no condensation in ET tube no airway movement); also turn blue
Body temp
normal- 100-102 F
take every 15 min
report if drop below 97 F
usually occurs within 20 minutes (become concerned if 92 F or under)
Hyperthermia- rare, cats, any temp over 103 F is concern, address vet on next steps ( mostly due to seizures)
Preventative rewarming: (heating blankets, water bottles, warm IV fluids)
CNS: palpebral reflex
blink reflex
deep- absent
present- light anesthesia
very sluggish or absent- moderate depth
lightly tap corner of eye
CNS: Swallowing reflex
present- light anesthesia
absent- moderate anesthesia and deep
CNS: pedal reflex
pinch toes
should flinch or retract
absent- moderate depth and deep
present- light anesthesia
pupil size
constricted- light anesthesia
gradually larger- moderate anesthesia
widely dilated-deep anesthesia
CNS: ear flick reflex
only cats
touch outside of ear
should flick
present'/sluggish- moderate level
absent- deep depth
over use will lose reflex
CNS: watch tail (cats)
no movement- moderate depth
slight movement- too light
resistance to drop not deep enough
CNS: corneal reflex
not routine
drop of liquid into eye
eye should recoil
no recoil- too deep
present- light and moderate depth
LA
Jaw tone
easily open
not flaccid
resistance- too light
anal tone
normally shut
relaxes and can open
should not be gaping
eye
central- too light or deep
look down and in- moderate depth
Continuously monitor (8)
RR
depth
HR
mucus membranes and CRT
jaw tone
palpebral reflex
eye positoin
temp
total rebreathing system
10 mL/kg/min
pop off valve closed, all CO2 gets rebreathed