Neuro 2
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
a CVA/TIA affecting the motor cortex would cause what symptoms
weakness
a CVA/TIA affecting brocas/wernickes area would cause what symptoms
brocas - speech production
wernickes - language comprehension (interpretation of speech)
a CVA/TIA affecting the occipital lobe would cause what symptoms
visual deficits
a CVA/TIA affecting the cerebellum would cause what symptoms
ataxia/dizziness
describe how a stroke occurs
vascular occlusion or bleed in the brain causes rapidly developing focal ± global signs of cerebral dysfunction
Compare onset and timing of stroke vs TIA
Both stroke and TIA are sudden unexpected onset however, stroke symptoms are >24hrs or cause death whereas, TIA symptoms typically last <10mins but are always <24hrs
Most common stroke impairment
Limited ability to undertake physical activities
Identify the 3 most common function losses following a stroke
Motor impairment (70-99%), Sensory impairment (66%), Visual inattention (58%)
Most common MOTOR impairment that limits function in stroke patients
weakness
What are the FAST signs of stroke
Face drooped?
Arms cant be raised?
Speech slurred or confused?
Time is critical, call 000!
Thrombolysis
IV medication to dissolve an ischaemic clot
Endovascular thromboectomy
Mechanical clot retrieval via catheter
A pt has had a thrombolysis, what is the physio relevance in regard to influencing management
Follow post-thrombolysis protocols, monitor BP/neurological change, mobilise only after clearance
A pt has had a endovascular thrombectomy, what is the physio relevance in regard to influencing management
Check groin site, monitor haemodynamics, mobilisation guided by medical protocol
General guidelines for physiotherapy following TPA <12hrs post thrombolysis
Respiratory assessment only - gentle respiratory therapy if required, NO suctioning, NO positive pressure
NO mobilisation
General guidelines for physiotherapy following TPA >12hrs post thrombolysis
Medical clearance required for mobility, consult with medical team to ensure understanding of procedure and outcomes (esp complications), mobilise with caution taking extra precautions to minimise risk of any injury, alert medical team to any bleeding during/following treatment
whta factors should be considered when planning an acute functional assessment
-is the pt medically stable
-is pt alert/cooperative
-does pt have pain
-physical capability to move
-what medical adverse event is pt most at risk of
-is pt at risk of injury
-pt risk factors for falling
-what is goal of assessment
-what level of assistance are you planning to provide
-are there any supportive/protective/safety devices required
minimum requirements for standing in acute stroke management
-medically stable and cleared for mobility
-cooperative with some comprehension
-pain managed
-DVT screen NAD
-strength grade >/= 3 in hip F/E, knee E, ankle PF/DF in at least one LL
-attachments managed
-clinical protocols adhered to
identify an acute measurement tool for coordination
finger nose test
identify an acute measurement tool for tone and spasticity (seperate tools)
Tardieu spasticity
Modified ashworth scale for muscle tone
identify an acute measurement tool for coordination
Ritchie Articular Index (RAI) joint tenderness with PROM of hemiplegic shoulder
What is identified as the strongest predictor of functional outcome following a stroke
Initial stroke severity on admission
Based on the AVERT trial, when should most stroke patients ideally commence out-of-bed mobilization
Between 24 and 48 hours
Which impairment is considered the most significant contributor to reduced physical function post-stroke?
Weakness
List the "4Ds" typically associated with a Vertebrobasilar system stroke.
Diplopia, dysphagia, dysarthria, dizziness
What specific muscle groups should be targeted when using E-stim to prevent or reduce shoulder subluxation
supraspinatus + posterior deltoid
Identify some clinical indicators that suggest poor functional outcomes for a stroke patient
Worse stroke severity on admission
Prior stroke
Older age
High degree of motor loss
Prolonged unconsciousness
Urinary incontinence > 1/52
Cognitive deficits, sensory inattention, neglect
What is the minimum total scheduled daily therapy time (PT and OT combined) recommended for rehabilitation
3 hours total scheduled therapy, with at least 2 hours of active task practice.
List 2 complications associated with bleeding into the subarachnoid space (often from ruptured aneurysm)
Blood mixing with CSF leading to rapid rise in ICP
Blood irritates the meninges causing headache, photophobia and weakness
Define the "Ischaemic Penumbra" and explain its significance in acute medical management
Ischaemic Penumbra is the salvageable brain area surrounding the ischaemic core (tissue destined to die). Restoring blood flow to this area is the goal of rapid medical intervention.
Explain the rehabilitation recommendations for Progressive Resistance Training (PRT) for stroke patients. Include the recommended repetitions, sets, and how it should be combined with other therapy types
Progressive resistance training should be provided for reduced strength. Target 8-12 repetitions maximum (RM) for at least 2 sets. Because it is unclear if PRT alone improves activity, it must be combined with repetitive task practice.
A stroke patient in the sub-acute phase of recovery exhibits a flaccid upper limb with a palpable gap at the glenohumeral joint. They are beginning to experience dull, aching shoulder pain.
-What complication is this patient likely developing?
-Propose a management plan
Use firm support when sitting and a sling during walking
Use E-stim for 30-60 mins/day targeting supraspinatus/posterior deltoid.
Provide education on manual handling to protect the joint.
Cardiorespiratory fitness targets for stroke patients
The recommendation is to aim for 3–5 days per week, for 20–60 minutes per session, at a perceived exertion (RPE) of 11–14
What is the amount of STS repetitions required for effective motor learning
more than 60 reps per day
What must we include in rehabilitation of stroke patients who have difficulty sitting and how can we ensure functional integration, list ways to progress as well
Practice msut include sitting and reaching beyond arms length with supervision/assistance
To ensure functional integration we can make it specific such as reach for cup and take sip etc, key for driving motor learning
Progress trunk control via pertubation and reducing BOS
Vary distance and direction
What must we include in rehabilitation of stroke patients who have difficulty standing and how can we ensure functional integration
Challenge standing balance by weight shifting or reaching as well as incorporating functional training such as stepping, squats or obstacles
When should spasticity be addressed in stroke patients
Not a main driver or activity limitation so only address when it impacts function
Stroke patient contracture prevention/management
Active motor training combined with estim (get them to do what they can while estim working)
Stroke patient has swelling of extremities, what is the recommended management, as well as who is most at risk of swelling
Passive mobilsiation (PROM) and elevation of limb whilst resting
Immobile patients with limbs in gravity dependent positions are at most risk
When does rehabilitation of TBI patient commence
As soon as medically stable
Describe TBI
Single event physical injury to the brain from an external mechanical force that results in permanent or temoporary impairment of cognitive, physical and psychosocial functions with diminished or altered state of consciousness
Contrast primary, secondary and associated injuries in regard to TBI’s
The primary injury refers to damage done at time of impact and is caused by mechanical forces (acceleration/deceleration/rotation) whereas, secondary injury occurs after initial impact and refers to the physiological and biomolecular aftermath of the primary injury (e.g. elevated icp.
Associated injuries are peripheral injuries that occur during the same incident that caused the TBI (e.g. chest, spine etc)
Identify key features associated with secondary injury TBI
Occurs after inital impact
Disrupted autoregulation
Compression
Reduced blood flow
Elevated ICP hypotension
Hypoxia
Identify common somatic complaints in TBI
Headaches, dizziness, pain, sleep disturbances
How is severity outcome of TBI predicted
Using GCS and PTA
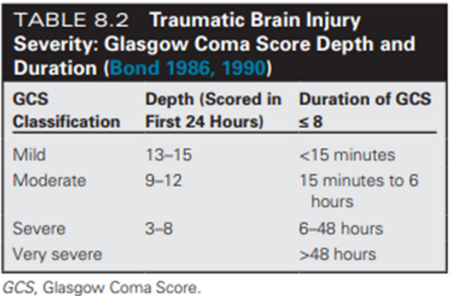
Identify how DEPTH is measured on GCS for predicting TBI severity
Depth is scored in the first 24hrs:
Mild = 13-15
Moderate = 9-12
Severe = 3-8
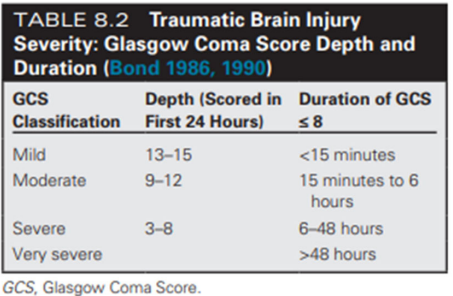
Identify how DURATION is measured on GCS for predicting TBI severity
Duration is scored based on how long GCS is greater than or equal to 8:
Mild = <15mins
Moderate = 15mins to 6hrs
Severe = 6-48hrs
Very severe = >48hrs
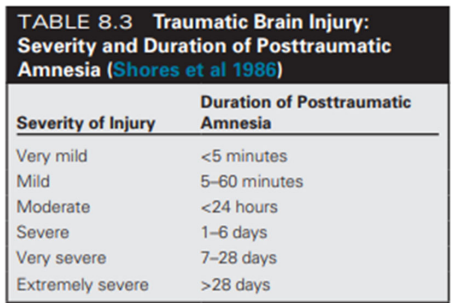
Identify how duration is measured on PTA for predicting TBI severity
Duration of posttraumatic amnesia:
Very mild = <5mins
Mild = 5-60mins
Moderate = <24hrs
Severe = 1-6days
Very severe = 7-28days
Extremely severe = >28days
Definition and features of coma
Coma = </=8GCS
Not obeying commands, uttering words, or opening eyes
What are the 2 best predictors of functional outcome in those who have suffered a TBI
Duration of coma (GCS <8) and length of PTA
Define PTA
Post traumatic amnesia is period from accident until person is oriented to surroundings
Describe ‘vegetable state’ includign features
Wakeful, reduced responsiveness, intermittent periods of wakefulness
Post traumatic confusion or clouding of consciousness in those who have suffered a TBI is often a sign of improvement, identify what features we would see in these individuals
awake most of time, confused, easily distracted, faulty memory, slow consistent responses to stimuli, functional communication emerges in this state
Identify some autonomic changes that occur in someone who has suffered a TBI
HR and RR variability
Temerature and BP changes
Excessive sweating
Dialted pupils
Vomiting
Anxiety, panic disorder, PTSD
Identify some sensory and perceptual changes that occur in someone who has suffered a TBI
Hypersensitivity to light or noise
Loss of hearing or sight
Visual field changes
Numbness and tingling (peripheral nerve injury)
Loss of somatosaensory functions
Dizziness or vertigo
Agnosia
Apraxia
Identify some motor changes that occur in someone who has suffered a TBI
paralysis/paresis - monoplegia/hemiplegia
cranial nerve injury - facial paralysis, dysarthria, dysphagia
poor coordination of movement
abnormal reflexes and muscle tone
loss of selective motor control
poor balance
loss of bowel/bladder control
Identify how a TBI patient may present differently to a CVA patient
Higher prevalence of behavioural, cognitive and perceptual impairments
Disorders of consciousness influence early rehab
More communication issues, agitation, low arousal
Greater likelihood of diffuse injury than focal deficits
Fatigue, headaches, sleep disturbances and sensory hypersensitivity more common
What must be included in patient interview when assessing a TBI patient
Description of TBI event and time period following\
Perception of perceived functional ability
Associated injuries
Falls screen
What must be included in physical assessment for a TBI patient
Associated/concurrant injuries and pain
Posture and balance
Voluntary movement - active, muscle strength, coordination
Involuntary movement (through observation)
Flexibility, tone, spasticity, reflexes
Sensation and visual deficits
Vestibular function
Functional tasks analysis including balance and gait
Cognitive and perceptual deficits e.g. dyspraxia, inattention, neglect
Why do we try to advocate for outpatient or community based rehab for those who have suffered a TBI (applies to any impairment really)
Enables the patient to practice and learn activities in the environment in which they will be applied
Identify common interventions for muscle paresis as the problem
Strength training targetted toward key muscle groups responsible for improved function to optimsie translation to functional gain
Common interventions for movement disorders
Task specific practice (structured practice, mvoement specificity, feedback)
Identify common strategies to optimise physiotherapy outcomes
Practice whole functional tasks
Set concrete goals
Demonstrate the exercises and tasks
High reps
Short frequent sessions
Remove distractions
Reward appropriate behaviour
Simple orders, clear tasks
Whilst testing visual acuity, visual fields and eye mvoements (CN3, 4, 6) you have identified new visual deficits in a patient who has suffered a TBI, what is your next plan of action
Refer for comprehensive assessment by relevant health professional
What occurs in tetraplegia and what deficits would we see
C1-T1 injury - reduction or loss of motor/sensory function in arms, trunk, legs and pelvic organs
What occurs in paraplegia and what deficits would we see
Below T1 injury - reduction or loss of motor/sensory function in trunk, legs and pelvic organs
contrast complete and incomplete SCI
complete has no motor or sensory function below the level of injury whereas incomplete will have some function preserved below the injury
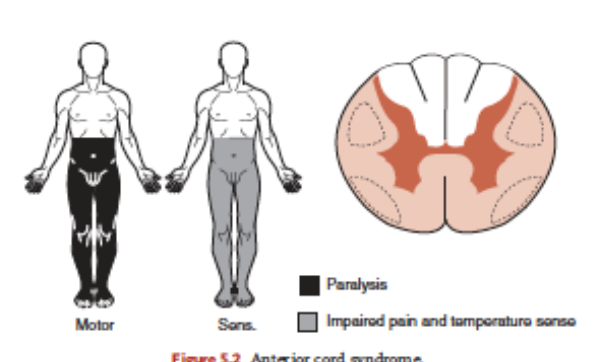
Describe anterior cord syndrome as an incomplete spinal injury
Damage toward front of spinal cord via flexion/dislocation/protrusion
Loss/impairment ability to sense pain, temeprature and touch below level of injury
Motor impairment
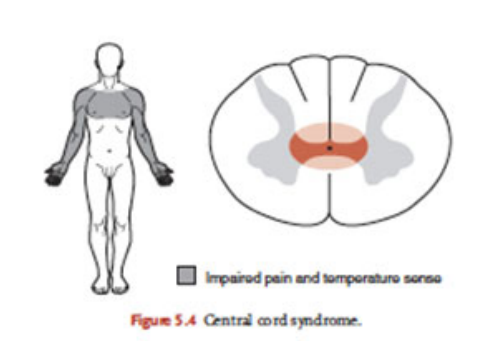
Describe central cord syndrome as an incomplete spinal injury
Damage in centre of cervical spinal cord, common moi is hyperextension
Loss of function in the arms
Function MAY be preserved in legs and bladder/bowel
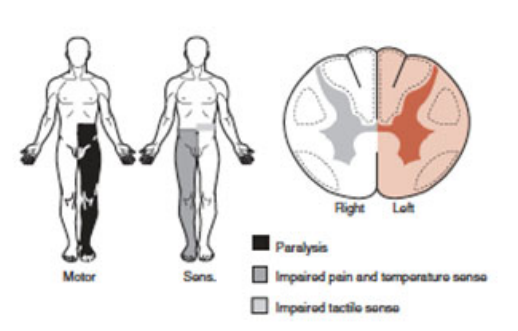
Describe brown-sequard syndrome as an incomplete spinal injury
Damage is on one side of spinal cord
Impairment or loss of movement and proprioception on injured side
Impairment of pain, temperature and touch sensation on opposite side
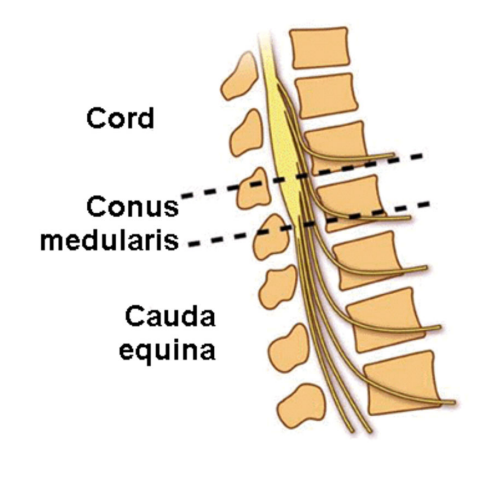
Describe conus medullary syndrome as an incomplete spinal injury
Trauma that affects the spinal cord in the sacral area and lumbar nerve roots
Bladder bowel significantly impaired
Minimal lower extremity impairment
Sensory impairment are symmetrical in saddle area
A person suffers an SCI that is accompanied by respiratory impairments, whta complications could these respiratory impairments cause
Ability of breath compromised from partial paralysis of diaphragm, intercostals and/or abdominals
Difficulty coughing and sneezing means icnreased risk of chest infection
Respiratory failure, pneumonia and pulmonary embolus
Increased risk of atelactasis
spinal cord injuries at what level can cause autonomic dysreflexia
Lesions at or above T6
Autonomic dysreflexia (AD) signs/symptoms
Hypertension, headache, bradycardia, flushed appearance, unusual sweating, shivering, nasal congestion, goosebumps, nausea
Common causes of autonomic dysreflexia
UTI, blocked urine catheter, pressure ulcers, constipation, infection
Management of autonomic dysreflexia
Move pt into upright sitting
Check BP every 5 mins
Loosen tight clothing
Search for cause
Seek medical attention
Autonomic Dysreflexia
-at what level lesion can AD begin to present
-signs/symptoms
-common causes
-management
Lesions at or above T6
symptoms - HTN, headache, bradycardia, flushed appearance, unusual sweating, shivering, nasal congestion, goosebumps, nausea
causes - UTI, pressure ulcers, blocked urine catheter, constipation, infection
management - move pt into upright sitting, check BP every 5 mins, loosen tight clothing, check for cause, seek medical attention
SCI lesion at C1-C3, identify key muscles still functioning, mobility use, and ADL independence
SCM, trapezius, some/no diaphragm
Powerchair for mobility
Fully dependent, ventilator dependent, needs 2A
SCI lesion at C4, identify key muscles still functioning, mobility use, and ADL independence
Full diaphragm function, small shoulder control
Powerchair for mobility
Dependent for all ADL’s
SCI lesion at C5, identify key muscles still functioning, mobility use, and ADL independence
Biceps and deltoids now wokring
Powerchair for mobility, hand control so can drive but no transfer
Independent eating, shaving and grooming with adaptive devices
SCI lesion at C6, identify key muscles still functioning, mobility use, and ADL independence
Wrist extensors, rotator cuff, tendonesis grip
Manual WC possible, often power WC, can drive with modifications
Modified independence in accessible environment
DO NOT STRETCH FINGER FLEXORS
SCI lesion at C7-C8, identify key muscles still functioning, mobility use, and ADL independence
Triceps, finger flexors and extensors
Manual WC, independent transfers
All self care tasks independently
SCI lesion at T1, identify key muscles still functioning, mobility use, and ADL independence
Full UL innervation, trunk paralysis remains
Manual WC, independent transfers
All self care tasks independent
SCI lesion at T2-T12, identify key muscles still functioning, mobility use, and ADL independence
Intercostals (T6+), abdominals (T12), trunk stability
Manual WC, bilateral AFO’s + cane for short distances
Fully independent, some modified ambulation possible
SCI lesion at L2-S5, identify key muscles still functioning, mobility use, and ADL independence
Hip flexors, knee extensors, dorsiflexors, plantarflexors
Community ambulation possible with aids
Fully independent in any environment, rapid recovery
Treatment objectives for those with SCI in acute phase
Manage cardiorespiratory conditions/complications, achieve independent respiratory status if possible
Early mobilsiation, orientation to vertical
Prevent neurological deterioration and facilitate neurological recovery
Prevent and manage secondary complications
Maintain and strengthen all innervated muscle groups
Facilitate functional patterns of activity
When would surgery be indicated in an SCI
If there is displacement or loss of stability in spinal column
Conservative management of SCI in acute phase
4-6 weeks of bracing when mobilised
recumbence (laying down) due to absence of vasomotor reflexes
passive ROM, active exercises for unaffected muscles
cervical injury - traction, assisted cough, arms elevate to prevent edema
before mobilising use tilt table whilst monitoring BP, vital signs, and neurological function every 10 degrees until 80 deg
mobilisation after 4-6 weeks
aim is to protect spinal cord until restoration of biomechanical stability
What should we do before mobilising a pt with an SCI who hasnt orientated to vertical yet
Tilt table whilst monitoring BP, vital signs, and neurological function every 10 degrees until 80 deg
Conservative management of SCI in restoration/subacute phase
Usually in spinal cord injury unit
Interventions following ICF framwork - prevent impairments, activity limitation and participation restrictions
Improve independence in ADL’s
Achieve and maintain community reintegration
Conservative management of SCI in long term/chronic phase
Long term management via coordinated community rehab services
Long term support to meet ongoing needs
Achieve high level mobility goals for community participation
Monitor recovery of function
Physiotherapy interventions for respiratory care in those with SCI
Targeted postural drainage to improve secretion clearance
Combination of mechanically assisted cough and manually assisted cough for those with ineffective cough
People with newly acquired SCI with respiratory muscle weakness should be assessed by a physiotherapist within 24 hours of admission
Physiotherapy interventions for strength training in those with SCI
Shoulder exercises to prevent shoulder pain
People prescribed exercise should receive a hard or electronic copy of individualised program
Focus on upper back, posterior shoulder - lat pulldowns, rowing, incline bench
Dosage = 2-4days a week, 2-3 sets of 8-12 reps, 50-80% 1RM
Physiotherapy interventions for motor skills and mobility in those with SCI
Power wheelchair skills training for those dependent on powerWC for mobility
Walking training should be provided to people with SCI who have lower limb function
Empower those with SCI to manage their injuries and physical rehab
Dosage and modalities of cardiovascular fitness for those with SCI
2-3 days a week, 20-60min sessions, 60-80% peak HR, avoid overuse issues in UL
Arm cranking, wheelchair ergometry, swimming sports, vigorous ambulation
Physiotherapy interventions for pain management in those with SCI
Educate to avoid shoulder overuse and trauma to prevent and treat shoulder pain
Shoulder exercises
Pressure injury and management
Routine skin check, reposition every 2 hours in lying, pressure relief every 30mins in sitting (weight shifting), clean skin from urin/fecal leakage
Pressure mapping and sitting assessment to individualise type and duration of relief, WC tilt, NMES to increase blood flow and reduce ischial pressure, edcuate pt
How should a tetrapelgic be postioned in bed in regard to UL and LL
shoulder abduction, elbow extension, wrist extension 45deg, fingers slight flexion
hips extension and slight abduction, knee extension (avoid hyperext), ankle and toes in dorsiflexion
what are the 5 most common secondary complications in SCI
UTI, AD, pressure ulcers, bone and soft tissue injuries, bowel problems
Describe a grade A SCI on the AIS scale
Complete - no motor or sensory function preserved in S4/S5