Spinothalamic Tract, Spinoreticular Tract
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
27 Terms
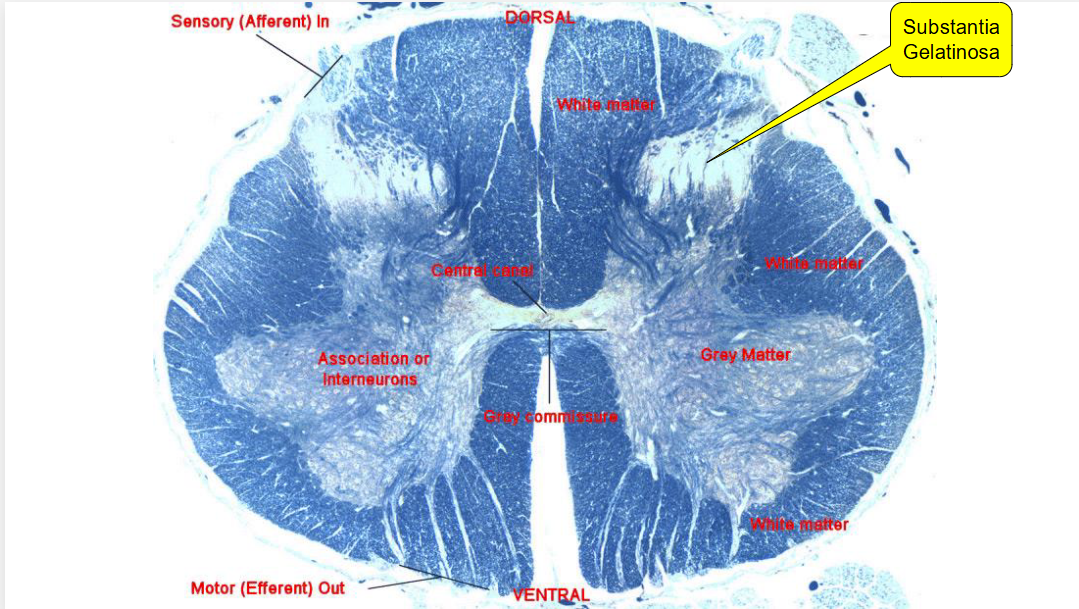
Substantia Gelatinosa
Grey matter region (cell bodies) in the dorsal spinal cord, capping the dorsal horn. Important in pain, temp, and touch sensations.
First-order somatosensory neurons start AP at the axons. This AP then travels to the cell bodies in this region, which initiate first synapse of the spinothalamic tract.
Pain Gate
The name for the substantia gelatinosa because it contains interneurons that can amplify or inhibit pain sensation through enkephalins. Opioids act on this region.
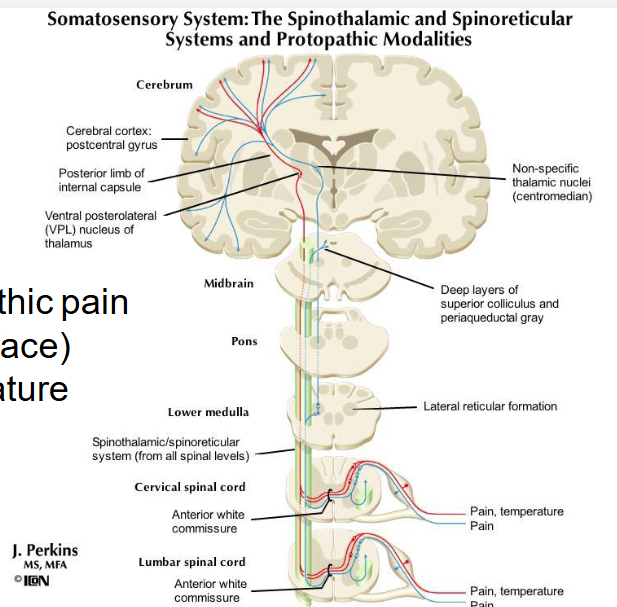
Describe the Spinothalamic Tract
Made up of:
Primary neurons that have an AP at the axons in response to pain, touch, and temp. These then transmit the signal to the cell bodies which are found in the dorsal horn/substantia gelatinosa. The neurons synapse #1 to secondary neurons.
Secondary neurons send signal across the midline/anterior white commisure (decussation), meaning they cross over to the opposite side. They then ascend up the spinothalamic tract to the thalamus (ventral posterior lateral) and synapse #2 tertiary neurons
These tertiary neurons project to the postcentral gyrus, aka the primary somatosensory cortex in the parietal lobe and synapse #3
Speed of Primary vs. Secondary vs. Tertiary neurons
Primary neurons are minimally myelinated or unmyelinated, making them much slower than secondary/tertiary ones
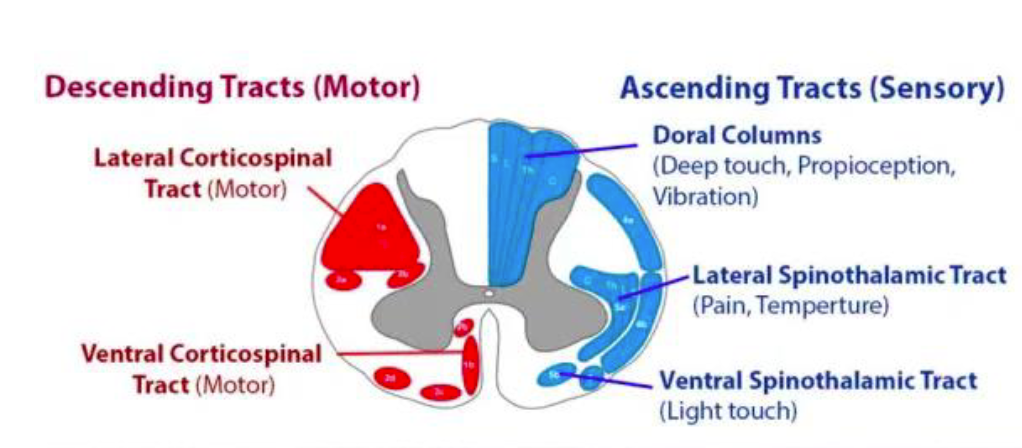
Two Spinothalamic Tracts
Lateral: Ends on the side, or laterally, on a coronal view of the spinal cord. Signals pain and temperature.
Ventral: aka Anterior. Ends on the front, or anterior of the spine on a coronal view. Signals light touch.
What kind of pain does the spinothalamic tract encode?
Protopathic pain (slow onset, minimal localization, lasts even after stimulus ends)
Does NOT encode protopathic pain of the face
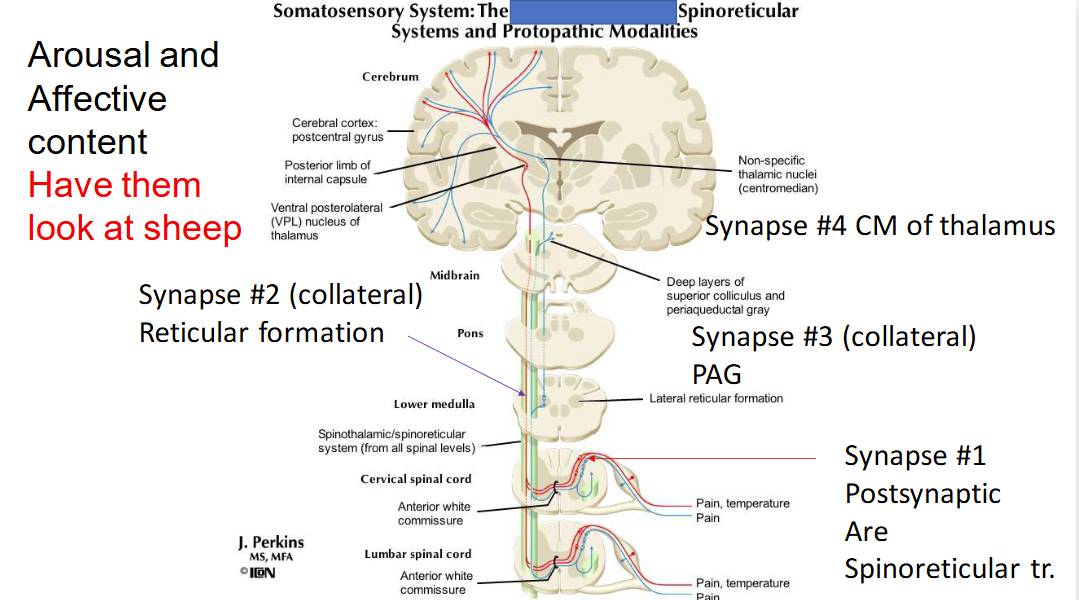
Spinoreticular Tract processes…
Arousal and effective content of pain
Our negative feelings and attentiveness when experiencing it
Describe the spinoreticular tract
Primary neurons have AP at axons which carry to cell bodies in the dorsal horn. These synapse secondary neurons.
The secondary neurons decussate (cross) right at the midline and ascend to the reticular formation. There, a collateral or branch of secondary neurons project and synapse to the periaqueductal gray (PAG), which is involved in pain perception. The secondary neurons also synapse tertiary neurons in the reticular formation, which project to the centromedian nucleus (CM) or middle of the thalamus.
Tertiary neurons in the CM of the thalamus will synapse other cells and generate lots of activity
Where and what is the PAG
A region in the midbrain responsible for fight or flight and pain relief. Primarily composed of cell bodies/gray matter. Surrounds the cerebral aqueduct which connects the third and fourth ventricles. Filled with opioid receptors.
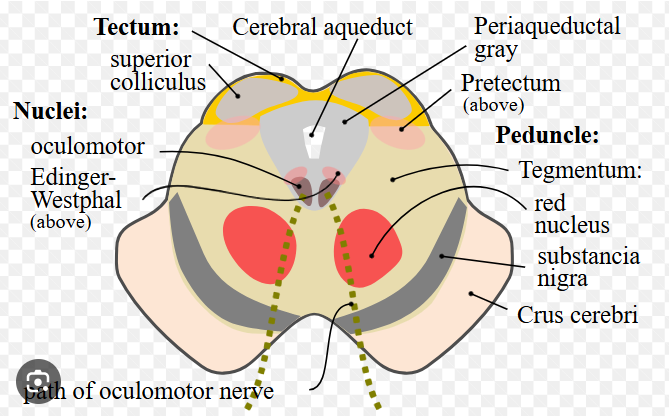
Cerebral peduncles
anterior part of the midbrain that connects the brainstem to the thalami
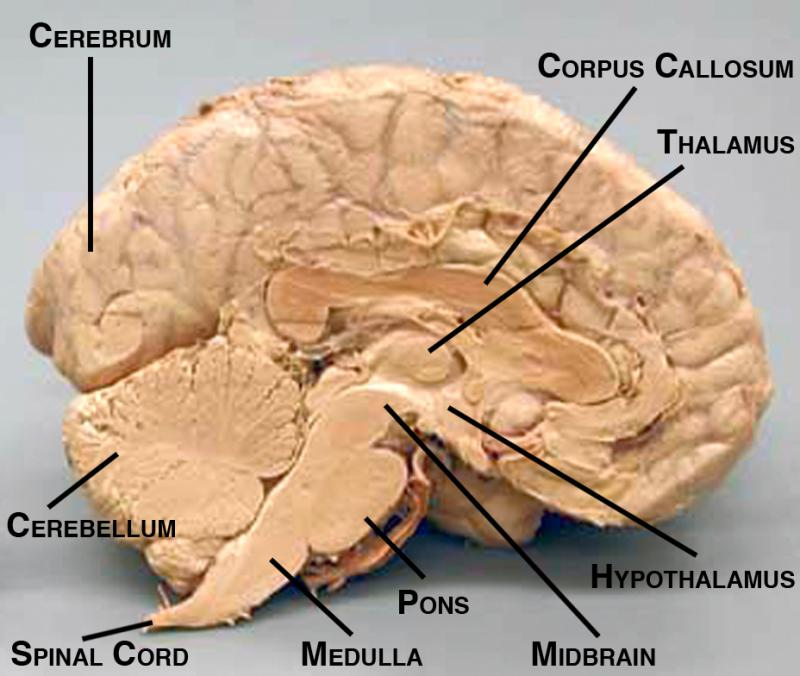
Thalamus
Our body's information relay station. All information from your body's senses (except smell) must be processed through your thalamus before being sent to your brain's cerebral cortex for interpretation
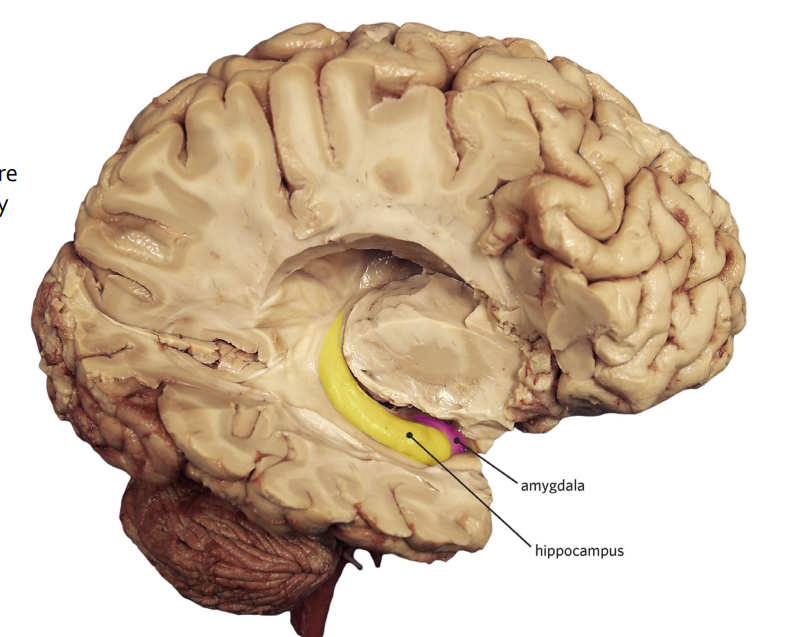
Hippocampus, what and where
Responsible for memory in the brain
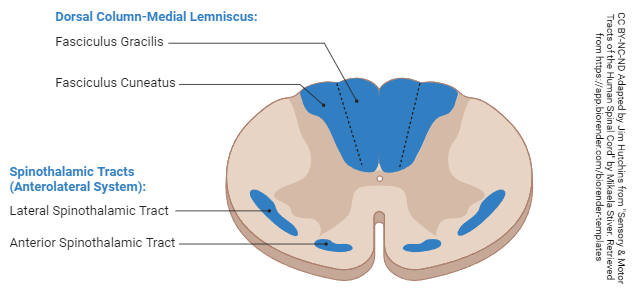
Dorsal column
Located between the two dorsal horns. Somatosensory neurons ascend through here in the Dorsal Column-Medial lemniscus System.
Neurons are segregated by which part of the spine they come in from (sacral, cervical, thoracic, lumbar) and ascend.
Dorsal Column-Medial Lemniscus System encodes…..
Epicritic Pain (well-localized)
Well-localized touch
Kinesthesis/proprioception: perception of one’s own movements and where one’s body is ins pace, ex: standing on one leg with eyes closed/moving head is hard
2-point tactile: Perception of two different points of contact, ex: closing tweezers on hand vs. shoulder
Stereognosis: Recognize shape or object only using touch, ex: shape traced on your back
Vibration
Dorsal Column-Medial Lemniscus System is also called the
Posterior Column System
Pathway of Dorsal Column-Medial Lemniscus System
First-order neurons are well-myelinated and large. They have AP in the axon which is transmitted to the cell body. These neurons go through the dorsal horn, and turn 90 degrees to ascend straight up. They synapse for the first time at the nucleus gracilis or nucleus cuneatus. These are in the myelencephalon.
The second-order then cross over and decussate in the medulla (this is also where the nucleus gracilis/cuneatus are) and ascend to the ventral posterolateral (VPL) of the thalamus. They synapse here.
The third-order neurons project to the somatosensory cortex/post-central gyrus and synapse here.

fasciculus cuneatus vs fasciculus gracilis
gracilis is more medial
Tabes dorsalis definition and symptoms
An effect of syphillis. The dorsal column cells die off. Disrupts sensation of fine touch vibration, two-point tactile, stereognosis, and proprioception.

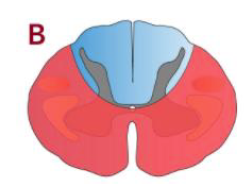
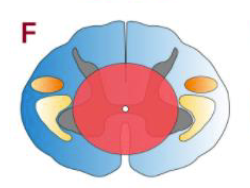
Describe the effects of this lesion
Corticospinal tract is lesioned, ventral horns are lesioned = spastic paralysis (damage to upper-motor neurons)
Lateral spinothalamic tract is lesioned = no pain or temperature sensation
This will happen bilaterally because lesions are on both sides. Effects will impact the segment and any sensory processing in the segments below, because the go up to that segment.
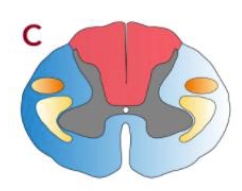
Describe the effects of the lesion
Dorsal columns are lesioned = no well-localized touch sensation, no kinesthesis/proprioception, no two-point tactile, no vibration, no stereognosis
Occurs at level and below.
This lesion can be caused by syphillis

Describe the effects of the lesion
Dorsal columns are lesioned = no well-localized touch sensation, no kinesthesis/proprioception, no two-point tactile, no vibration, no stereognosis
Happens bilaterally (if just one side, would be ipsilateral)
Corticospinal tract is lesioned = spastic paralysis on both sides since upper motor neurons are damaged
Happens bilaterally (if just one side, would be ipsilateral)

Describe the effects of the lesion
Ventral horn is damaged = flaccid paralysis (only lower motor neurons are damaged), muscle atrophy, loss of Babinski reflex, reduced reflexes
This lesion can be caused by polio
Describe the effects of the lesion
Lateral spinothalamic tract neurons cross over at the midline. They will be lesioned = no pain or temperature sensation on both sides of the body at the lesioned level
Ventral horn is partially lesioned = some flaccid paralysis, muscle loss at that level
Dorsal horn is partially lesioned = some loss of proprioception, localized touch sensation, etc. at that level
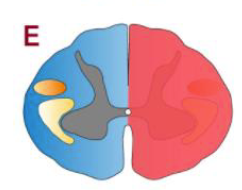
Describe the effects of the lesion
Spinothalamic tract is lesioned, which crosses over at the midline right away = contralateral effects (loss of pain and temp sensation)
DCML pathway is lesioned, which doesn’t cross over until the medulla in the brain = ipsilateral effects (loss of fine touch, vibration, stereognosis, two point tactile, proprioception)
corticospinal tract is lesioned, which doesn’t cross over until the medulla in the brain = ipsilateral effects (spastic paralysis)
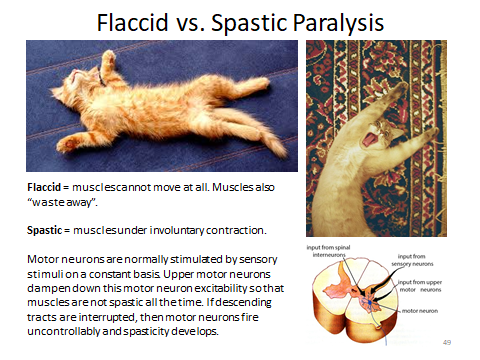
Flaccid vs Spastic Paralysis
Flaccid paralysis: Caused by lesions to the lower motor neurons. Results in limpness, atrophy of muscle tone, loss of reflex
Spastic paralysis: Caused by lesions to the upper motor neurons. Results in stiff and contracting muscles that spasm. Increased muscle tone and reflexes.
Double Pain (Tract & Process)
A delta fiber: myelinated, fast, localized, pain resides quickly (DORSAL COLUMN)
C: unmyelinated, slow, dull, prolonged throbbing (SPINOTHALAMIC)
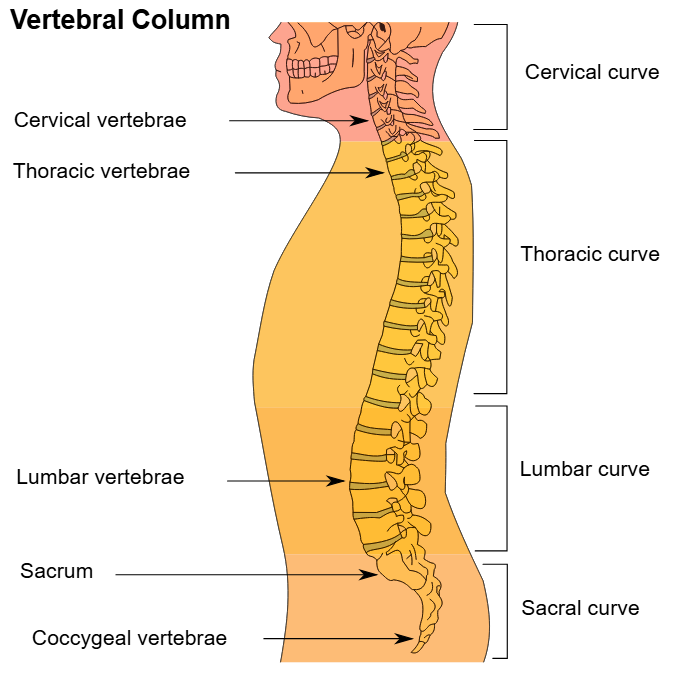
Order of Spinal Parts
CTLS
cervical thoracic lumbar sacral