LAB: RADIOGRAPH
1/30
Earn XP
Description and Tags
from lab manual
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
enamel & dentin
enamel → most radiopaque structure
dentin → should be uniform in density
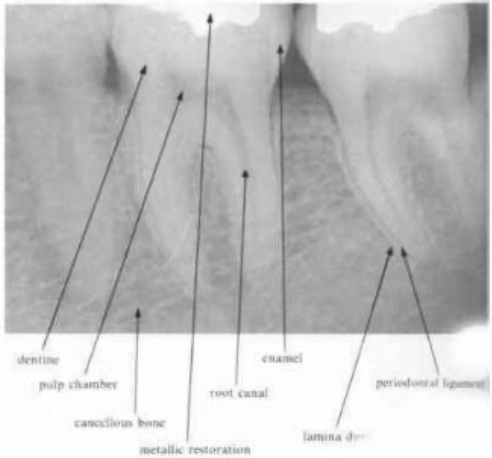
cementum
cannot be seen radiographically
is observed commonly and may be mistaken for caries
note the “burnt out” appearance around the enamo-dentinal junction in the radiograph
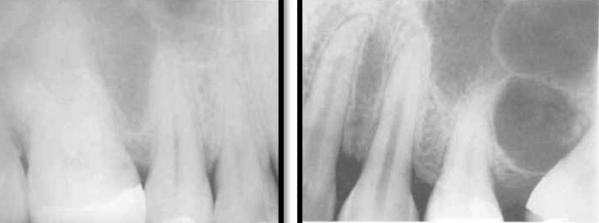
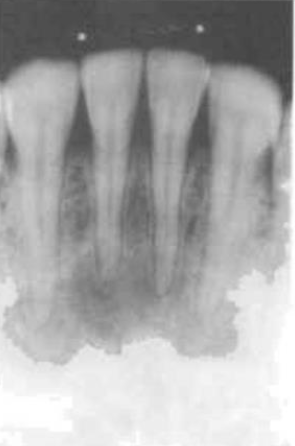
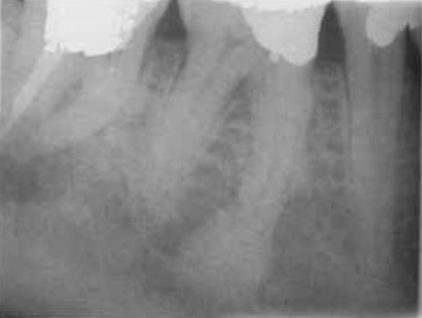
cancellous bone
the bony trabeculae have a coarser pattern and run horizontally in MN
compare with the finer lace-like pattern in MX
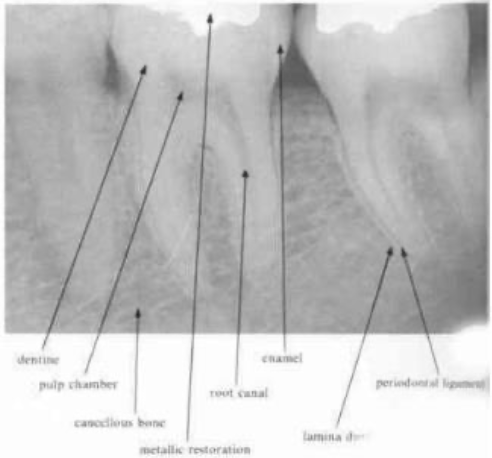
periodontal ligament space
any definite widening in this area suggests the presence of pathology
should be narrow and even around the whole of the root surface that lies within the bone
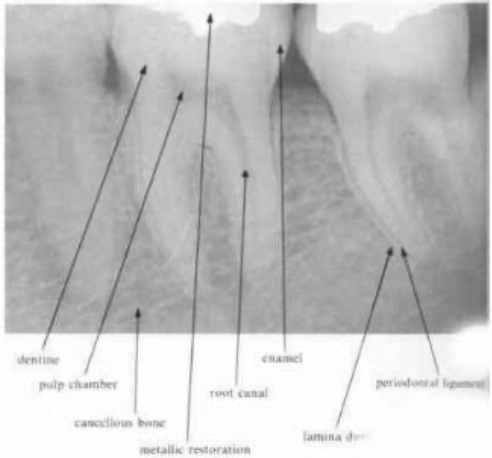
lamina dura
is a radiographic artifact and it would be unwise to place to critical an interpretation on the variation in its appearance in diagnosis
despite the definite appearance of a white line surrounding the roots of teeth within bone, investigation has revealed that there is no increase in mineralization of the cancellous bone lining the tooth socket
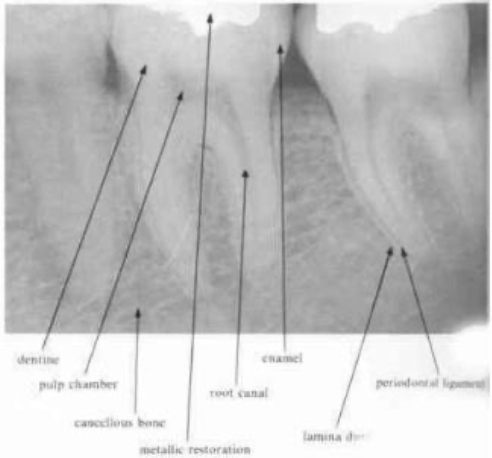
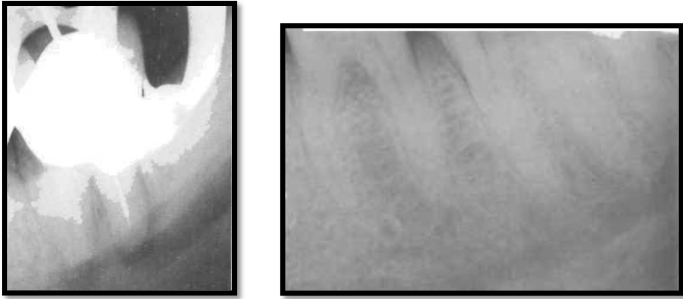
pulp and pulp stones
are clinically evident in both molar teeth
present few problems, their removal is easy from the chamber, although if they become lodged in a root canal they can present difficulties
pulp chamber & larger canals → readily visible on the radiograph
finer canals → those in the DB canal of the MX 1st molar may be more difficult to see
—root canals will never become completely sclerosed in the apical portion of the root
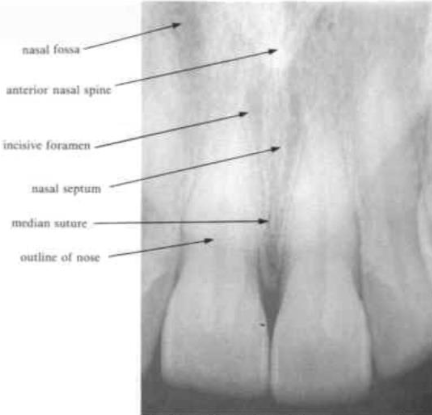
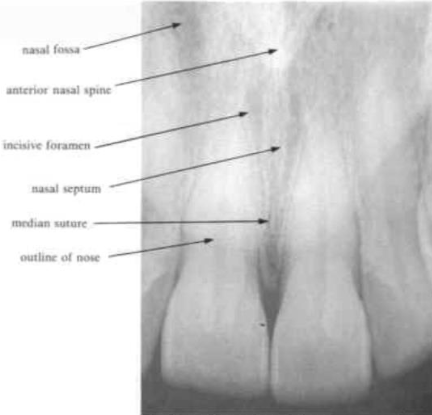
median suture
appears a radiolucent line between the central incisors in the maxilla
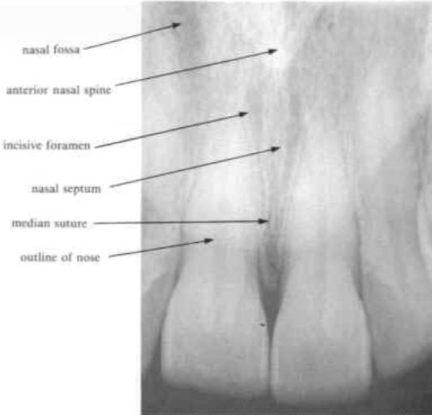
anterior nasal spine
appears as a V- shaped radiopacity which lies above or is superimposed on the incisive foramen
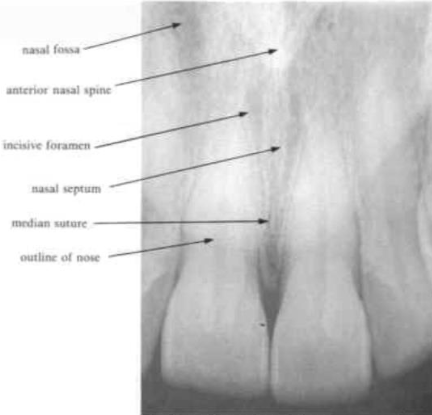
nasal septum
separates the two nasal fossae
is seen as a radiopaque white line
nose and lip line
is a definite line across the radiograph
a similar line in both upper and lower anterior radiographs often represents the lip line
maxillary antrum
may extend from the premolars to the tuberosity
the apices of the 2nd premolar and 1st molar lie close to
the floor of this may dip between the roots & may be oculated giving the appearance of a cyst
incisive foramen
the radiolucent circular shadow of this foramen may be superimposed over the apex of a central incisor and so be mistaken for a periapical lesion

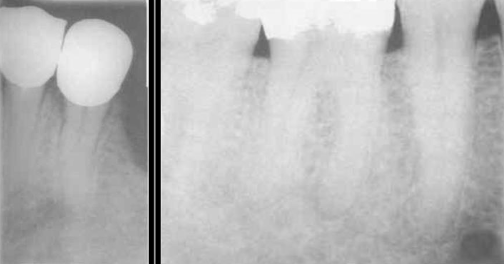
mandibular canal
aka: inferior dental canal
runs from the mandibular foramen in the ramus to the mental foramen
seen as a radiolucent band and may lie in close association with the apices of molar and 2nd premolar teeth
extrusion of medicaments and root canal filling materials may damage the inferior dental bundle
mental foramen
located below and distal to the apex of the 1st premolar
may be mistaken for a pathological lesion when it appears close to the apex of one of the premolars, which is due to the angle at which the radiograph is taken
lingual foramen
may be seen as white radiopaque area with a small central radiolucent dot in radiographs of the lower incisor area

nutrient canal
contain blood vessels supplying the bone and occur in both mandible and maxilla
lies between the central and lateral incisors as a vertical radiolucent line
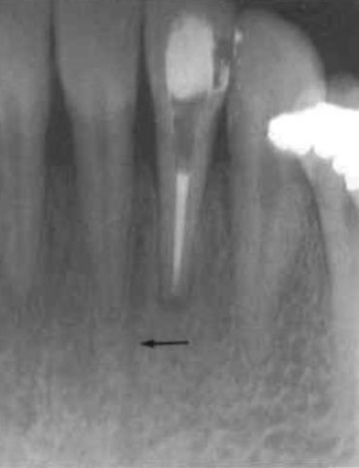
periapical radiolucencies
around the tip of the tooth root
important in endodontic diagnosis
most common radiolucency in the jaws
usually caused by pulpal (nerve) disease
recent lesions in periapical:
no radiopaque border
grow faster
long-standing lesions in periapical:
surrounded by a radiopaque (white) line
grow slowly
—radiographs cannot confirm if a lesion is a cyst

very early periapical changes
some early changes can be reversible
pulp vitality may still be maintained
seen in cancellous bone around the root apex
changes include:
altered trabecular bone pattern
slight increase in radiopacity
periodontal ligament (PDL) changes
widened PDL space is an early sign of disease
can be seen:
around the root apex
in the furcation area
often linked to pulpal pathology
lateral radiolucencies
not associated with the apex
occur along the side of the root
commonly caused by lateral canals
can appear even after endodontic treatment
root fractures and perforations
root fractures → often hard to detect on x-ray
perforations of root or furcation cause:
rapid bone loss
diagnosis may be clearer after extraction
condensing osteitis
may not always be of dental origin
not a radiolucency → it is a radiopacity
caused by:
low-grade infection
excessive biting forces
features:
no symptoms
less radiopaque than enamel
advanced periodontal disease
teeth are usually vital
causes bone loss and bony pockets
seen as lateral bone loss on radiographs
bone loss is due to periodontal pocketing, not pulp disease
a round radiolucent area may appear over the apex, but:
PDL space is narrow and even
suggests the lesion is not related to the root
stage one – early cementoma
teeth remain vital
no treatment needed
appears as a radiolucent area
develops slowly over about 6 years
commonly found near:
MN incisors
stage two – mixed appearance
tooth is vital
no treatment needed
typical around lower 1st molar region
shows a radiopaque area within the lesion
PDL space remains continuous around roots
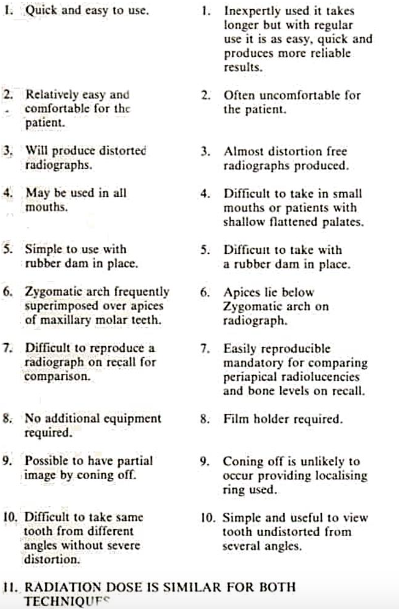
2 main methods used to take periapical radiographs
bisecting angle technique
paralleling technique
bisecting angle technique
the X-ray cone is directed at right angles to this bisecting line
film is placed close to the lingual or palatal surface of the tooth
an imaginary line is drawn:
between the long axis of the tooth
and the plane of the film
commonly used when:
film placement parallel to the tooth is difficult
paralleling technique
film is placed parallel to the long axis of the tooth
the X-ray cone is directed at right angles to the film
the X-ray tube is positioned further from the patient than in the bisecting technique
to achieve this:
the film must be held away from the tooth, especially in the maxilla
significance of longer distance in paralleling technique
reduces image magnification
produces a more accurate image
allows more parallel x-rays to reach the film
extended cone
often used to help aim the x-ray beam accurately
this led to the incorrect term “long cone technique”
correct name: paralleling technique
advantage & disadvantage of bisecting & paralleling technique