Anatomy Immune system
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Immune System
Protects us from infectious agents and harmful substances
provide immunity
Two types of immunity
Innate and Adaptive
Innate Immunity
Skin and mucosal + Nonspecific internal defenses ([7]Cells, Chemicals, and Physiologic responses)
present at the time of birth (do not need prior exposure)
Adaptive immunity
T-lymphocytes (cell-mediated immunity) and B-lymphocytes (humoral immunity + plasma cells (synthesize and release antibodies))
What is the purpose of innate immunity?
Responds nonspecfically to a range of harmful substances
What is the first line of defense for Innate Immunity?
skin and mucosal membrane
What is the second line of defense for Innate Immunity?
internal processes
neutrophils, macrophages, dendritic cells, eosinophils, basophils, mast cells, and non-killer cells
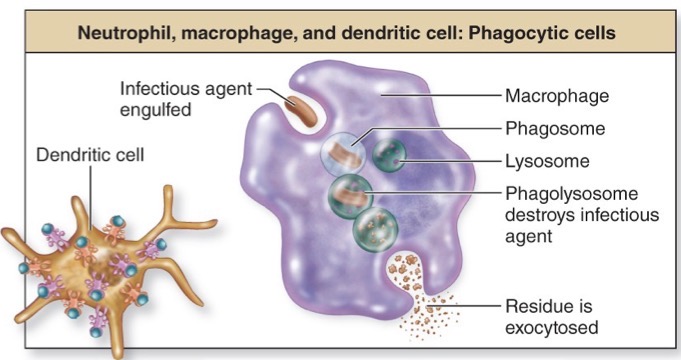
Phagocytic cells
Neutrophil, macrophage, and dendritic cells
engulf infectious agents
Phagosome: membrane lined sac housing bacteria
Lysosome: membrane bound intracellular vesicle containing lysosomal enzymes → breaking down and destroying the bacterial after destruction occurs
Phagolysosomes: contains both the bacteria and lysosomal enzymes
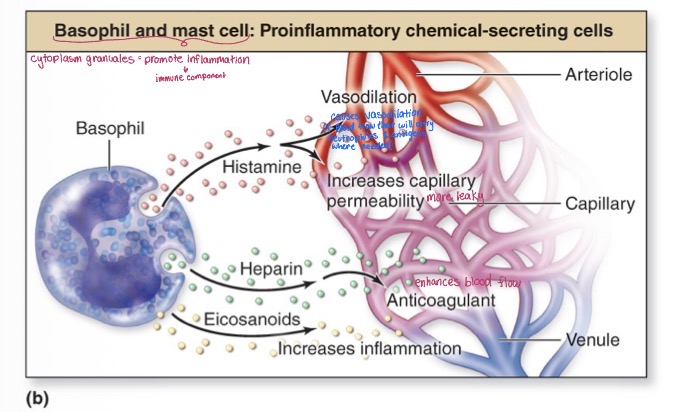
Proinflammatory chemical-secreting cells
Basophils and mast cells
promotes inflammation
Basophils release histamine (vasodilation + increases capillary permeability), heparin (enhances blood flow + anticoagulant), and eicosanoids (increases inflammation)
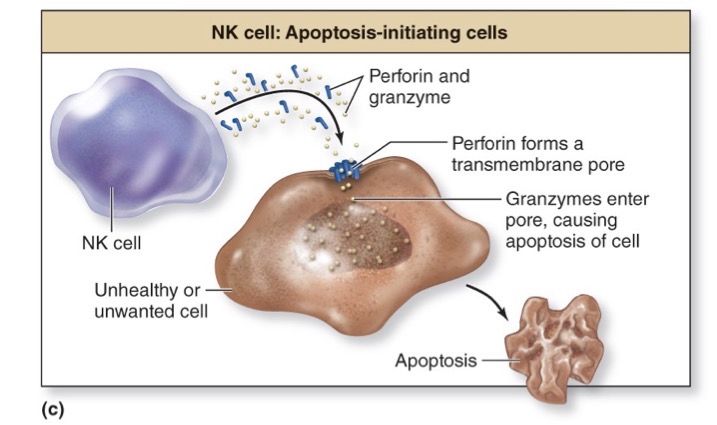
Apoptosis-initiating cells
NK cells (releases perforin and granzyme)
kills unwanted or unhealthy cells like virally infected cells or tumor cells
The virus needs to invade the host cell in order to replicate/must take over the host cell because it cannot replicate on its own
It does this by inserting its own DNA into the DNA of the cell and takes over the coding of the host cells or replicate
Perforin- causes perforation or pore on the cellular membrane
This allows the granzyme to enter → causes apoptosis (breaks down intracellular components
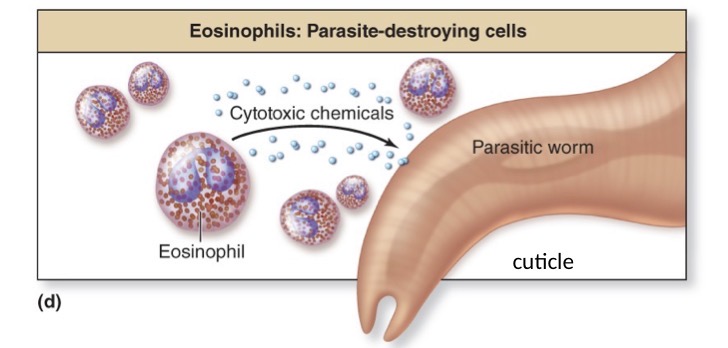
Parasite-destroying cells
Eosinophils
releases cytotoxic chemicals (destroys the outer protective covering of the parasite which is known as the cuticle)
Once the cuticle is destroyed, the parasite’s ability to control its internal environment has been ceased
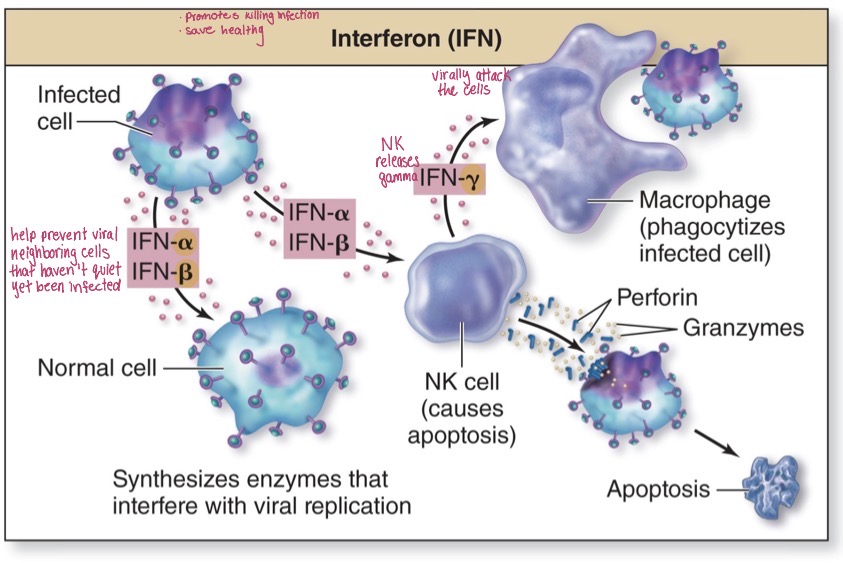
Interferon (IFN)
Nonspecific and viral protein
helps prevent viral neighboring cells that haven’t quiet yet been infected
releases IFN alpha + beta + gamma
Alpha and beta get released from the viral infected cells and travels to normal cells
NK cell causes apoptosis within virally infected cells
IN gamma from the NK cell promotes macrophages and phagocytizes the infected cell
Complement system
group of over 30 plasma proteins that work along with antibodies
synthesized by liver and releases in inactive form (enzyme cascade activates them)
What are the two complement activation pathways?
Classical pathway and Alternative pathway
Classical pathway
Antibody attaches to foreign substance and then complement binds to antibody (this is what activates other complement proteins)
Alternative pathway
Complement binds to polysaccharides of bacterial or fungal cell wall (takes out the middleman > antigen complex is not needed for activation)
Opsonization
complement protein (opsonin = CODED) binds to pathogen and enhances likelihood of phagocytosis of pathogenic cell (makes bacteria more readily recognizable = making it easier to be phagocytosed)
Inflammation
enhanced by complement, activated mast cells and basophils, and attracts neutrophils and macrophages
Cytolysis
complement triggers destruction of target cells and form membrane attack complex (MAC) that creates a channel in target cell’s membrane (group of complement fragments will band together to join complexes = MAC)
attach to bacteria + able to break through cell membrane + fluid rushes in and pressure breaks down the cell
Elimination of immune complexes
complement links antigen-antibody complexes to erythrocytes and cells move to liver and spleen where complexes are stripped off
Activated complement protein attach to the antibody on one side and receptors on the erythrocytes — macrophages will phagocytose the immune complex with the bacteria and erythrocyte will continue —- RBC transport mechanism for the elimination of immune complexes and bacteria
Process of inflammation
tissue damage
Release of inflammatory and chemotactic factors (mast cells + basophil = responds to something that is not normal/wanted)
Vascular changes: vasodilation of arterioles (increased blood flow), increase in capillary permeability (more flow of immune cells), and display of CAMS (proteins that are present within the lining of endothelial cells)
Recruitment of immune cells: margination (“pull over”, leukocytes and platelets can’t stay in/move out of the blood flow), diapedesis (white blood cells can pass through capillary walls and into interstitial tissue), and chemotaxis (neutrophils migrate from capillary to site of tissue damage due to the chemical gradient)
Delivery of plasma proteins (allows excess fluid to escape)
Lymphatic capillary “cleans up the excess” → more fluid within the tissues and will be picked up by the lymphatic capillary as well
Signs of inflammation
Redness- increased blood flow
Swelling- increases fluid loss from capillaries
Heat- increased blood flow and metabolic activity
Pain- stimulation of pain receptors
Loss of function
Fever (pyrexia)
abnormal body temperature elevation
results from the release of pyrogens from immune cells or infectious agents
100.4ºF — 38ºC
Prostaglandins: causes thermoregulation set point to increase → generates heat in order to bring body to this new set point
Ex: fever — shiver — peripheral vessels constrict — additional blanket
Events of a fever (mainly where it takes place and what gets released)
Pyrogens circulate through blood and target hypothalamus
Hypothalamus releases prostaglandin E2
Hypothalamus raises temperature set point leading to fever
when body temperature is elevated, the virus will not be able to be as detrimental
Benefits of a fever
Inhibits reproduction of bacteria and viruses
Promotes interferon activity
Increases activity of adaptive immunity
Accelerates tissue repair
Increases CAMs on endothelium of capillaries in lymph nodes
Adaptive immunity involves lymphocytes to attack foreign agents; due to the increased metabolic activity, proliferation of lymphocytes will occur
Accelerates tissue repair — produce more adhesion molecules on surface = more immune cells marginating and exiting capillaries → more immune cells will be in circulation of the lymph filtering out unwanted substances
What is the purpose of adaptive immunity?
Involves specific lymphocyte responses to an antigen
contact with antigen causes lymphocyte proliferation
Plasma cells release antibodies so B-lymphocyte forms plasma cells when stimulated
Which response time is quicker; innate or adaptive immunity?
Innate Immunity
What are the two branched os adaptive immunity?
Cell-mediated immunity (T-lymphocytes; effective against antigen within cells and requires antigen-presenting cell) and Humoral immunity (B-lymphocytes, plasma cells, and antibodies; effective against antigen outside cells and does NOT require antigen-presenting cell)
Antigen
substance that binds a T-lymphocyte or antibody
usually a protein or large polysaccharide
Example of antigen:
capsid- protein protective layer of viruses
Bacterial toxins- as they replicate, they release toxins which are recognizable
Antigenic determinant (a.k.a epitope)
Specific site on antigen recognized by immune system
each as different shape and multiple determinants
Specific region on an antigen that is bound to by an antibody
Immunogen
Not only something that is recognizable, but also provokes an immune response
antigen that induces an immune response
Immunogenicity
ability to trigger response (how rapid and vigorous is the response)
increases with antigen’s degree of foreignness, size, complexity, or quantity
Haptens
small foreign molecules that induce immune response when attached to a carrier molecule in host (hypersensitivity reactions)
an antigen, but is not an immunogenicity bc it is too small to create an immune response
Can be recognized and bound to
What type of contact do B-lymphocytes make with antigens?
Direct contact
What type of contact do T-lymphocytes make with antigens?
Indirect → antigen is processed and presented by another cell type
T-lymphocyte subtype
Cytotoxic T-lymphocytes
release chemicals that destroy other cells
CD8 allows for proper alignment of antigen presenting cell to the t-cell receptor
Helper T-lymphocytes
assist in cell-mediated, humoral, and innate immunity
Contain T-cell receptors embedded within their membranes
Each one of these receptors is identical and has an attachment point for specific antigens
CD4 protein aids in allowing proper alignment of the antigen presenting cell to the TCR
Antigen presentation
cells display antigen on plasma membrane so T-cells can recognize it
To recognize cells are present…all nucleated cells of the body and antigen-presenting cells (APC’s)
Attach antigen to MHC
MHC- major histocompatibility complex
Bound together and always embedded in the membrane
These antigens that are going to be presented must be attached to the MHC complex in order to be recognized and bounded
T-Lymphocytes with MHC molecules
Helper → CD4 → MHC Class II
Cytotoxic → CD8 → MHC Class I
Class I and II- Immune cells, dendritic cells, macrophages, and B-lymphocytes
Only class I- epithelial cell
Three main events in life of lymphocytes
Formation and maturation of lymphocytes
Primary lymphatic structures (red bone marrow + thymus)
Recognize one specific foreign antigen
Activation of lymphocytes
Secondary lymphatic structures is the location where lymphocytes are exposed to antigens/site of lymphocyte activation
Effector response: action of lymphocytes to eliminate antigen
T-lymphocytes migrate to site of infection
B-lymphocytes stay in secondary structures (plasma cells)
Lymphocytes that are replicated will resemble the OG one and contains the same receptors to attack the specific antigen
Formation of Lymphocytes
B-cells become fully functional/mature in bone marrow
Red bone marrow = responsible for production
T-lymphocytes are released from the bone marrow as pre-t-lymphocytes and travel to the thymus to complete maturation (gain their specific receptors)
Both of these cells after maturing are naive immunocompetent cells and have not been exposed to their specific antigens
Activation of Lymphocytes and Effector Response
Secondary lymphatic structures house B- & T-lymphocytes
The activated lymphocytes will travel to the site of infection
Helper T-lymphocytes release cytokines to enhance immune response
Cytotoxic T-lymphocytes destroy infected cells via apoptosis
B-lymphocytes form plasma cells which produce antibodies
Antigen challenge
First encounter between antigen and lymphocytes (Usually occurs in secondary lymphatic structures)
due to broad distribution of secondary lymphatic structures, it is inevitable that our bodies will have antigen challenge
Clonal selection
Forming clones in response to an antigen
all formed cells have same TCR or BCR that matches specific antigen
A given lymphocyte is being specific end from the entire population bc of its superficial receptor for a given antigen → that type of lymphocyte is going to replicate
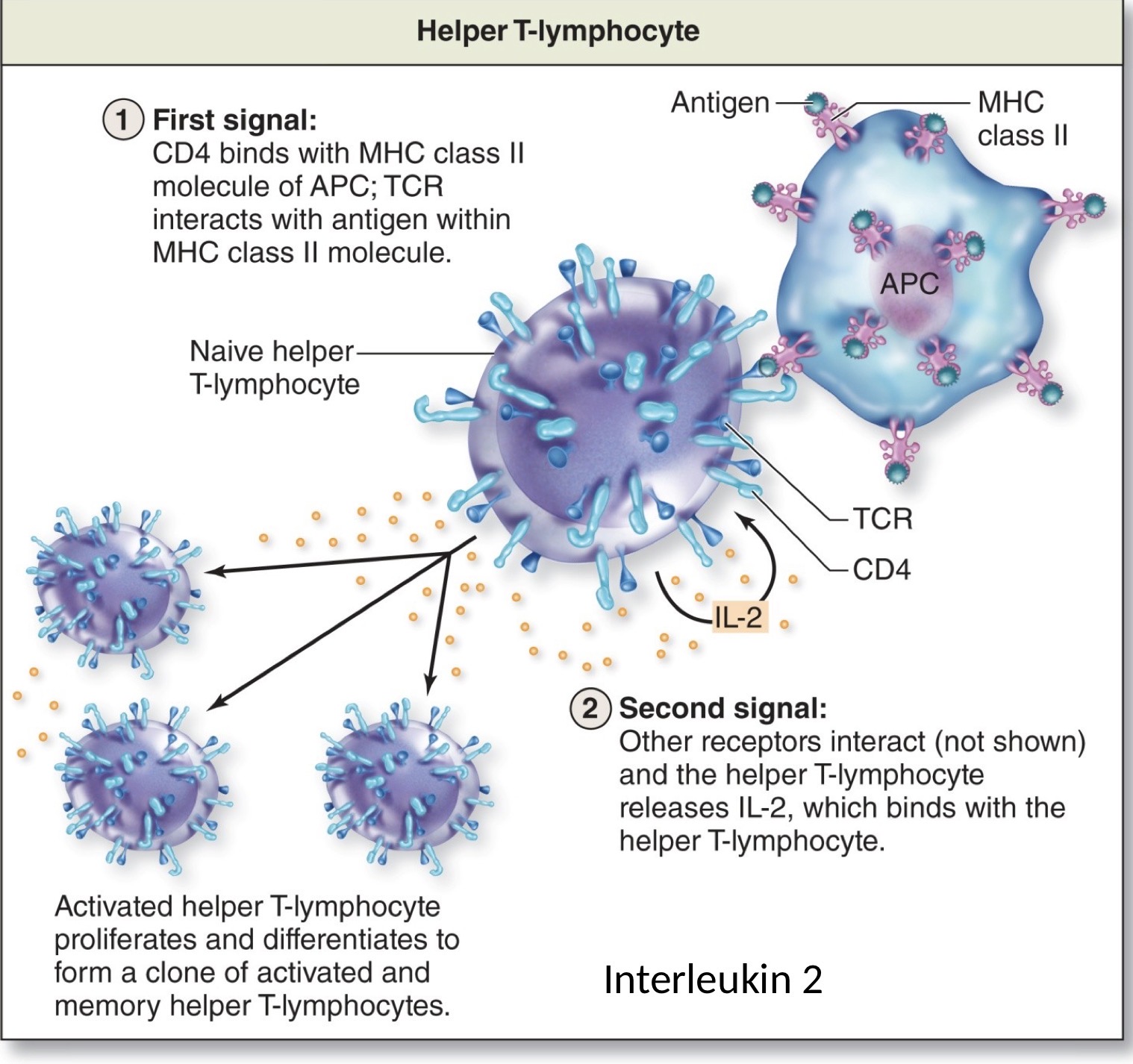
Activation T-lymphocytes
First signal: CD4 binds with MHC class II molecule APC; TCR interacts with antigen within MHC class II molecule
Physical attachment of the helper t-cell to the antigen coreceptor binds to the MHC on the antigen → that union provides the proper alignment so now the t-cell can bind to the antigen
Second signal: Other receptors interact and the helper T-lymphocyte releases IL-2, which binds with the helper T-lymphocyte
Activated helper T-lymphocyte proliferates and differentiates to form a clone of activated and memory helper T-lymphocytes
Binding of the t-cell to the antigen causes the helper to-cell to release a specific type of cytokines known as interleukin 2
IL-2 binds to the interleukin binding receptor on the surface of the helper t-cell → causes the proliferation of helper t-cells to enhance immune response memory helper t-cells will respond quickly to the pathogen that they have been previously exposed to beforee the pathogen can replicate and affect the body
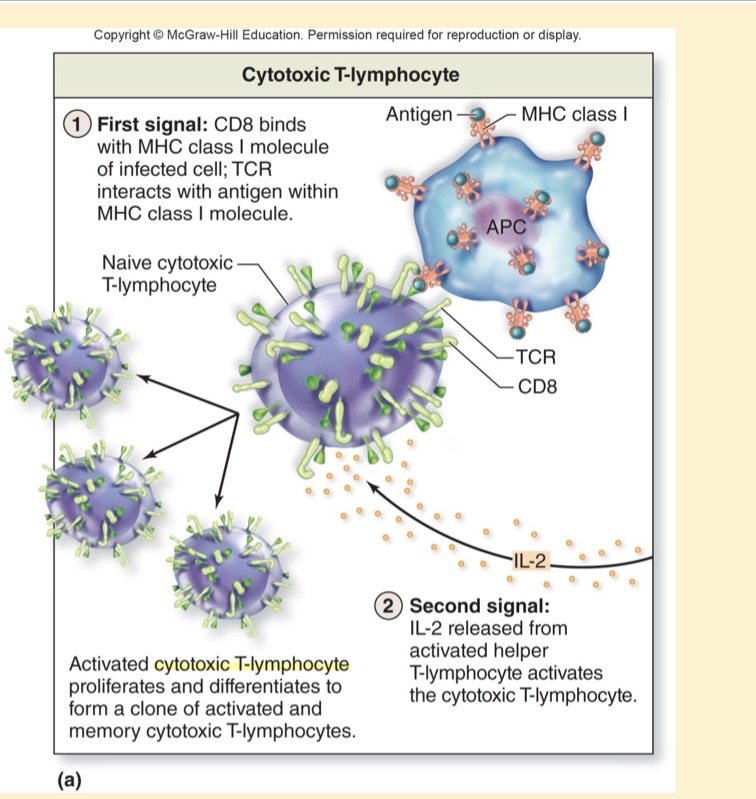
Activation of Cytotoxic T-lymphocyte
First signal: CD8 binds with MHC class I molecule of infected cell; TCR interacts with antigen within MHC class I molecule
Second signal: IL-2 released from activated helper T-lymphocyte activates the cytotoxic T-lymphocyte
IL-2 is being released from helper t-cells and will activate the cytotoxic cell as well as enhancing the immune response
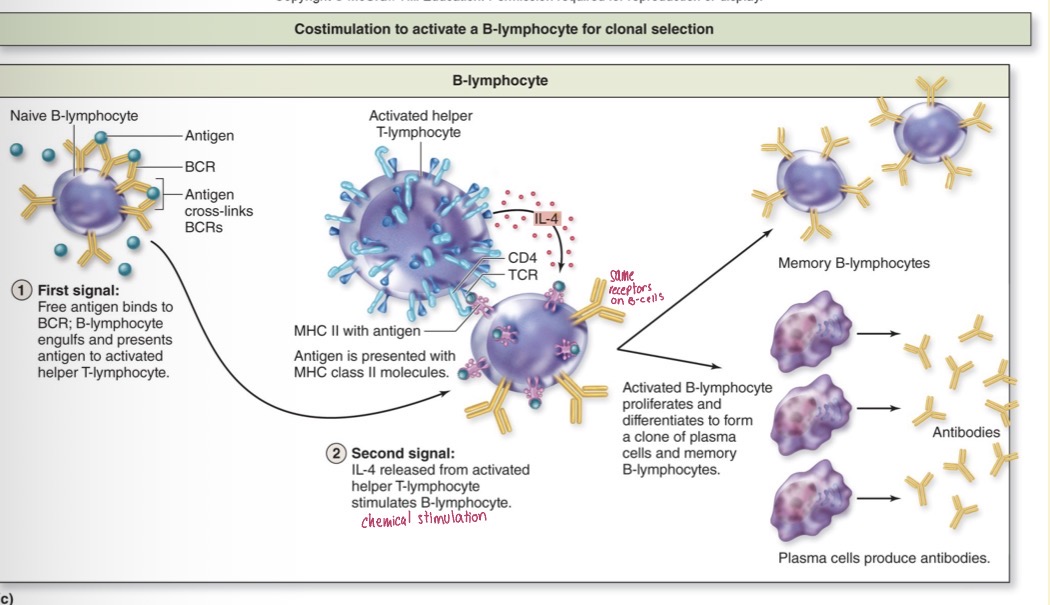
Activation of B-lymphocyte
First signal: Free antigen binds to BCR; B-lymphocyte engulfs and presents antigen to activated helper T-lymphocyte
B-lymphocyte have the ability to bind directly to the antigen and does not need the antigen presenting on the surface
Second signal: IL-4 released from activated helper T-lymphocyte stimulates B-lymphocyte
IL-4 is the specific type of cytokines known released for B-lymphocytes. B-lymphocytes will proliferate to form plasma cells that have these antibodies attached to them.
Some B-lymphocytes will not for plasma cells → they will remain as memory B-lymphocytes instead.
Effector response
Mechanism used by lymphocytes to help eliminate antigen
Each lymphocyte has its own type
Effector response for helper T-lymphocyte
Release IL-2, IL-4, and other cytokines
After exposure To antigen → activated and memory helper T-cells migrate to infection site
Help activate B-lymphocyte
Stimulate activity of innate immune system cells
Regulate and enhance cells of adaptive and innate immunity (does not destroy infected cells themselves)
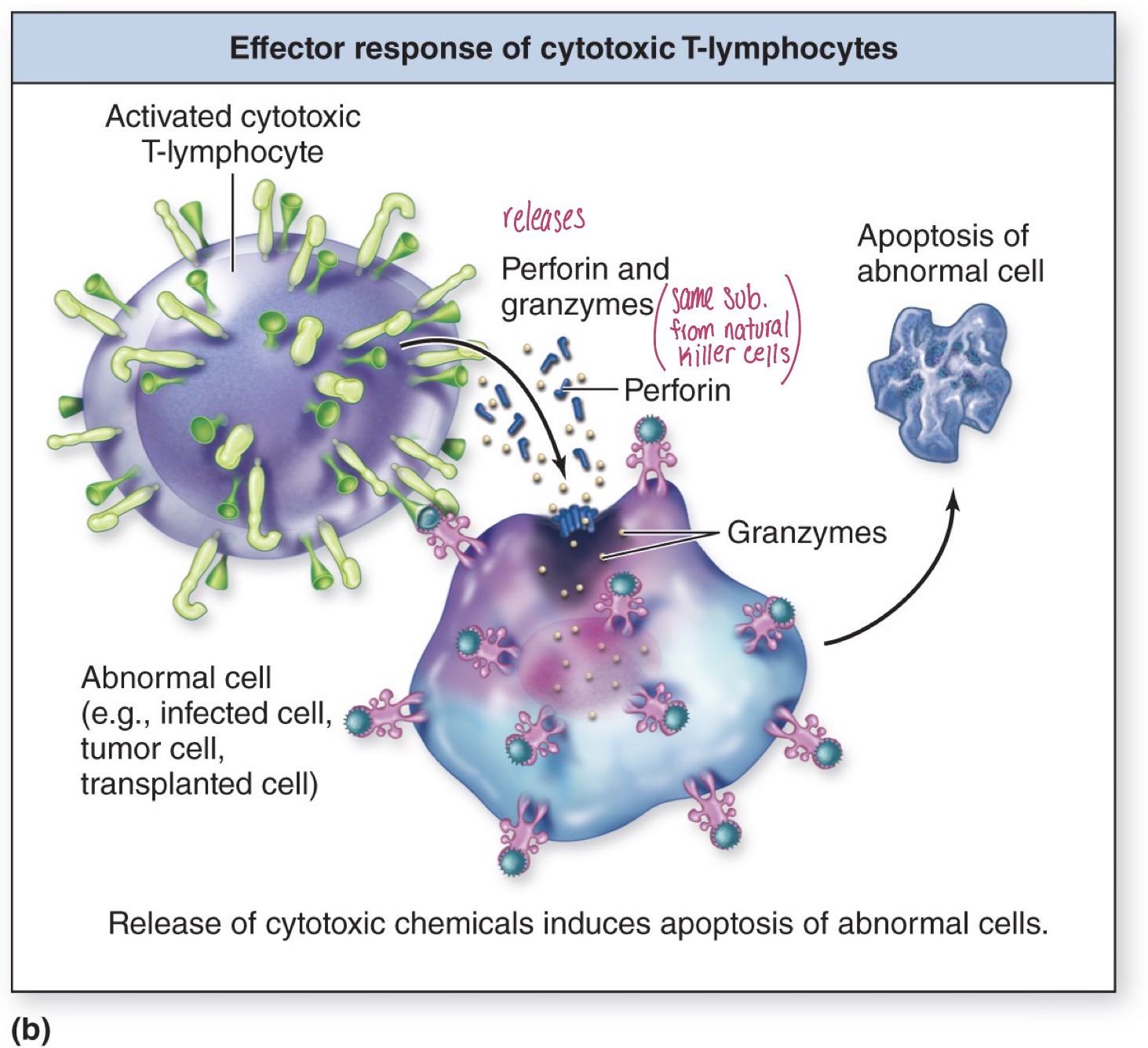
Effector response for cytotoxic T-lymphocyte
Destroy unhealthy cels by apoptosis
Attachment of the cytotoxic t-lymphocyte to the antigen causes the release of perforin and granzymes → same chemicals released by NK cells
Perforin attaches to the membrane of the abnormal cell and perforates the membrane allowing granzymes to enter the cell
Granzymes can break down a nucleus, destroy the function of organelles, etc., leading to apoptosis of the abnormal cell
Effector response for plasma cells (differentiated B-lymphocyte)
Produce antibodies
Most activated B-lymphocytes become plasma cells
Plasma cells release antibodies
Antibodies circulate through lymph and blood until encountering antigen
Antibody titer
Circulating blood concentration of antibody against a specific antigen
Antibodies
Immunoglobulin proteins produced against a particular antigen
Gamma globulins = antibodies
Not directly causing the removal of the antigen but they “tag” pathogens for destruction by immune cells
No antigen presenting cell on the surface is necessary for the binding of antibodies
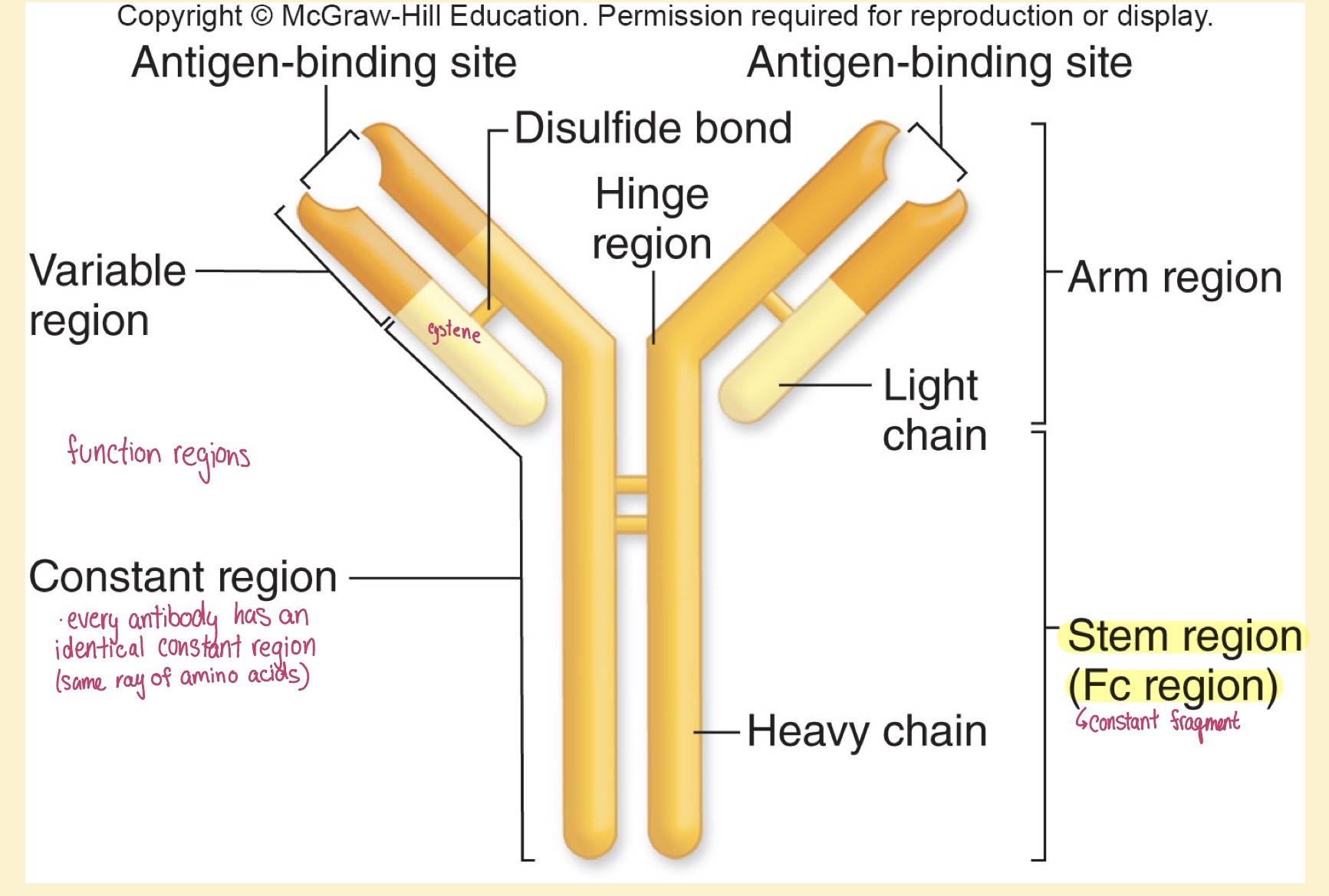
Antibody structure
Light chain- shorter and lower MW (lower part of floating arm)
Light and heavy chain are bound together by disulfide bond
Hinge region- the arms of the antibodies are able to adjust their angle in order to properly bind to the specific antigen
Functional regions- variable and constant region
Constant region- every single antibody within a single class will have identical constant region
Variable region- every single antibody will have a difference variable region; give antibodies their specificity; where the antigen-binding site is located
Binding of antigen-binding site of an antibody with antigen causes
Neutralization, agglutination, precipitation
they are grouped together because it is antigen-binding site that is involved
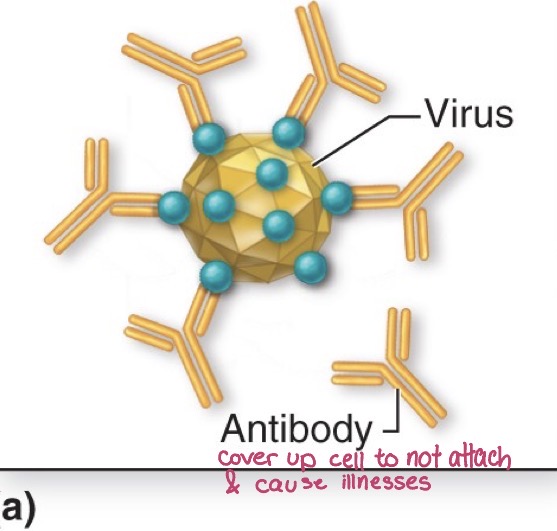
Neutralization
Antibody covers biologically active portion of microbe or toxin
binding of the antibodies covers up the biologically active parts of the cell, which causes the blockage of pathogens to attach the cell and take it over
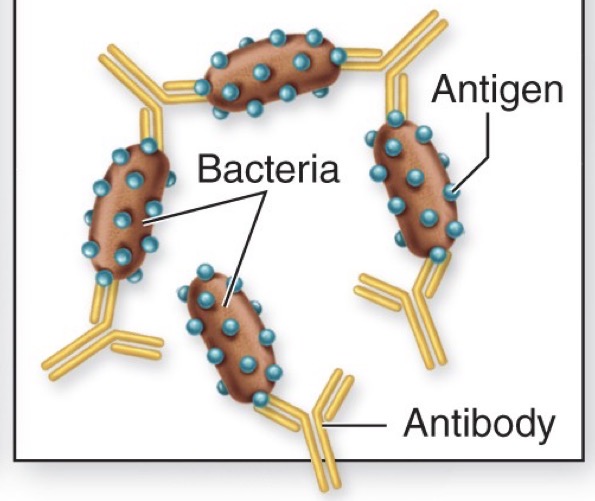
Agglutination
antibody cross-links cells (CLUMPING)
allows phagocytosis to be done more efficiently → multiple bacteria cells are clumped together
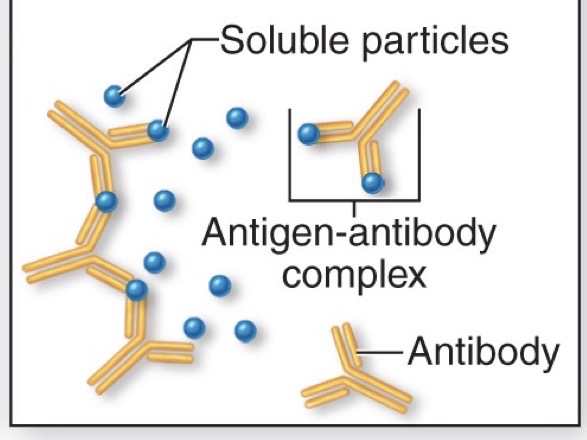
Precipitation
Antibody cross-links circulating particles forming an insoluble antigen-antibody complex
can’t be invaded by bacteria
Exposed Fc portion following antigen binding by antibody promotes
Complement fixation, opsonization, activation of NK cells
grouped together because the action is taking place at the Fc region of the antibody
Complement fixation
Fc region of antibody binds complement proteins; complement is activated
Fc region is able to bind to complement proteins; triggers cascade effect
Opsonization
Fc region of antibody binds to receptors of phagocytic cells, triggering phagocytosis
means it is covered in something
Allows phagocytosis to occur more efficiently; there are Fc receptors found on phagocytes and receptors which bind to the Fc region of antibodies, allowing phagocytosis
Activation of NK cells
Fc region of antibody binds to of an NK cell, triggering release of cytotoxic release of cytotoxic chemicals
these NK cells release perforin and granzymes to break down affected cells and cause apoptosis to occur
Where are IgG Imunoglobulins found?
Found in body fluids including blood, lymph, cerebrospinal fluid, serous fluid, peritoneal fluid, breast milk
able to participate in all 6 effector responses
What is the action of IgG?
Neutralization, agglutination, precipitation, complement activation, opsonization, NK activation
Percent of IgG
75-85%
IgM
Has 10 binding sites which makes it best at agglutination
IgE
In response to parasitism chemotactically draws eosinophils to the site of the parasite; eosinophils releases the contents of its granules and breaks down the functioning parasite
in response to allergies, IgE antibodies attach to the antigen via its binding site; the Fc binds to a Fc receptor on a mast cell or basophil cause it to release the contents of its granules → this release causes many inflammatory responses such as itchy eyes, bronchoconstriction, etc.
IgA
areas exposed to environment; best at neutralization
IgE
Allergy & parasitism; degranulation of basophils & mast cells; chemotactic for eosinophils
Effector Response (Cell-mediated immunity)
Activated helper T-lymphocyte releases cytokines to stimulate activity of B=lymphocytes, and regulates cells of innate immunity.
Activated cytotoxic T-lymphocytes release cytotoxic molecules (perforin and granzymes) causing apoptosis of foreign or abnormal cells
Effector Response (Humoral immunity)
Fab region of antibody binds to antigen to cause several consequences including neutralization of microbial cells and particles; agglutination of cells and precipitation of particles
Fc region of antibody serves as point of interaction with several structures including complement to cause complement activation, binding of phagocytic cells to cause phagocytosis of an unwanted substance or cell and binding of NK cells to induce apoptosis of an unwanted cell
Immunologic Memory: Memory
Memory results from formation of a long-lived army of lymphocytes upon immune activation
Immunologic Memory: Activation
Activation leads to formation of many memory cells against specific antigen
initial exposure of an antibody to its specific antigen which leads to the cloning of many identical cells; some are utilized to fight the antigen at the time of exposure while others are utilized as memory cells to decrease the effect that this antigen has if it enters the body at a later date
Immunologic Memory: Adaptive immunity
Adaptive immunity activation requires contact between lymphocyte and antigen
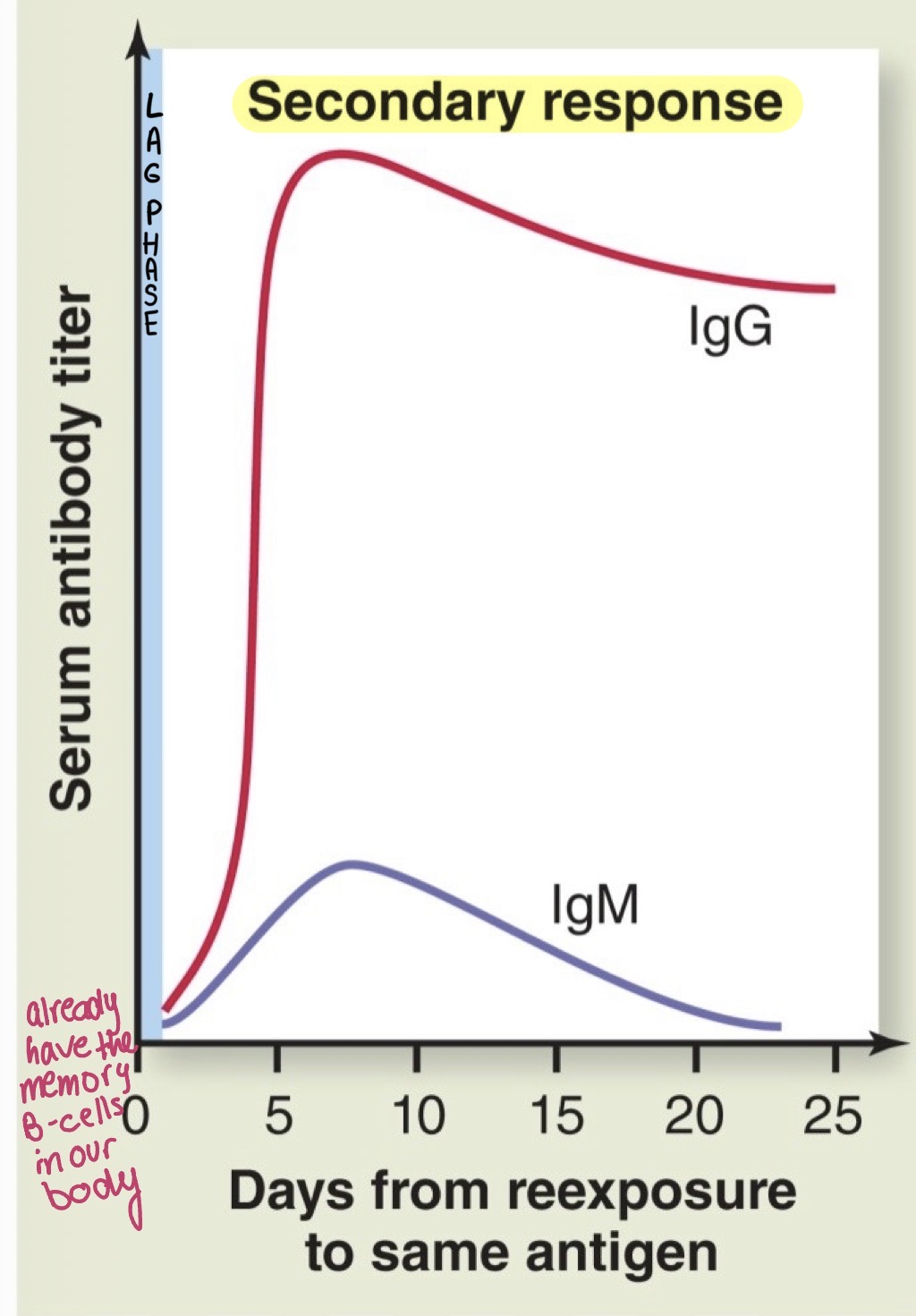
lag time between first exposure of the host and direct contact with the lymphocyte (leg time is quicker [less time for antibodies to show up after exposure] ad the response is of greater magnitude infection is removed before a person is even able to show symptoms
Secondary response
Pathogen typically eliminated before disease symptoms develop
Vaccines provoke the production of memory cells
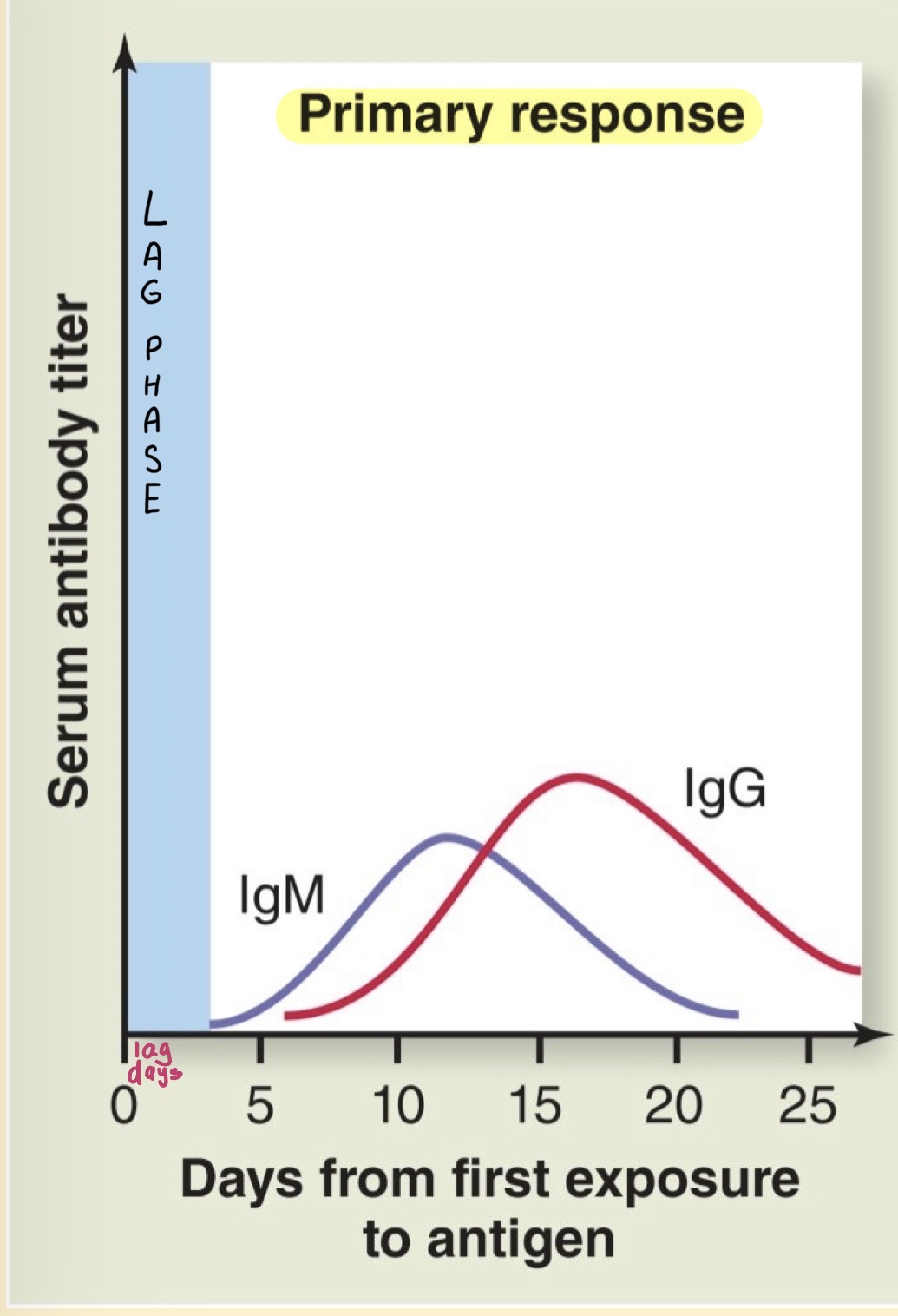
Antibody titer
A measure of immunologic memory/antibody concentration
Primary Response
Secondary Response
Active Immunity
Production of memory cells due to contact with antigen
Active immunity: naturally acquired
Direct exposure to antigen
Active immunity: Artificially acquired
Antigen exposure from vaccine
Passive immunity
No production of memory cells; antibodies from another person or animal
Passive immunity: naturally acquired
Transfer is mother to child across the placenta or in breast milk
Passive immunity: artificially acquired
Transfer of serum containing antibody from another person or animal