Amyotrophic Lateral Sclerosis
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
true
TRUE OR FALSE: A hallmark sign of ALS is a mixed UMN and LMN presentation.
true
TRUE OR FALSE: Sensation is usually not impaired in individuals with ALS.
amyotrophic lateral sclerosis (ALS)
progressive neurodegenerative disease - results in motor neuron death
LMN--> anterior horn cells, brainstem nuclei of CN V, VII, IX, X, XII (oculomotor nuclei spared)
UMN--> cerebral cortex, brainstem, spinal cord
false (5-10%)
TRUE OR FALSE: Most cases of ALS are inherited.
sporadic (idiopathic), familial (5-10%)
What are the two types of ALS?
ALS epidemiology
- most common motor neuron disorder
- average age of diagnosis: 55-65 y/o
- males > females
- military veterans (Gulf War) 2x as likely to develop ALS compared to non-military age matched norms
ALS pathophysiology
varies based on type
(FALS vs sporadic)
- aggregate build up of protein inclusion bodies--> toxicity and motor neuron cell death
- increased extracellular glutamate
- oxidative stress
false (unilaterally)
TRUE OR FALSE: ALS usually presents with symptoms presenting bilaterally and distally.
ALS clinical manifestations
combo of UMN/LMN signs and symptoms
limb onset (most common)--> weakness begins distally and unilaterally, UE extensors, LE flexors
bulbar onset--> weakness of mms involved with speech, swallow, facial expression
progressive--> cervical extensors, respiratory
*cognitive dysfunction (50%): more common with bulbar onset
SPARED--> sensory, eye muscles, sexual function, bowel and bladder
pseudobulbar palsy/affect
emotional lability, emotional outburst, pathologic laughing/crying, dysarthria, dysphagia, facial & tongue weakness
*results from spastic bulbar palsy (corticobulbar fibers from speech, mastication, swallowing centers affected)
respiratory failure
What is the most common cause of death in individuals with ALS?
ALS diagnosis
CLINICAL DIAGNOSIS = signs and symptoms of UMN and LMN loss
- steady progression of symptoms in one body region spreading to other body regions
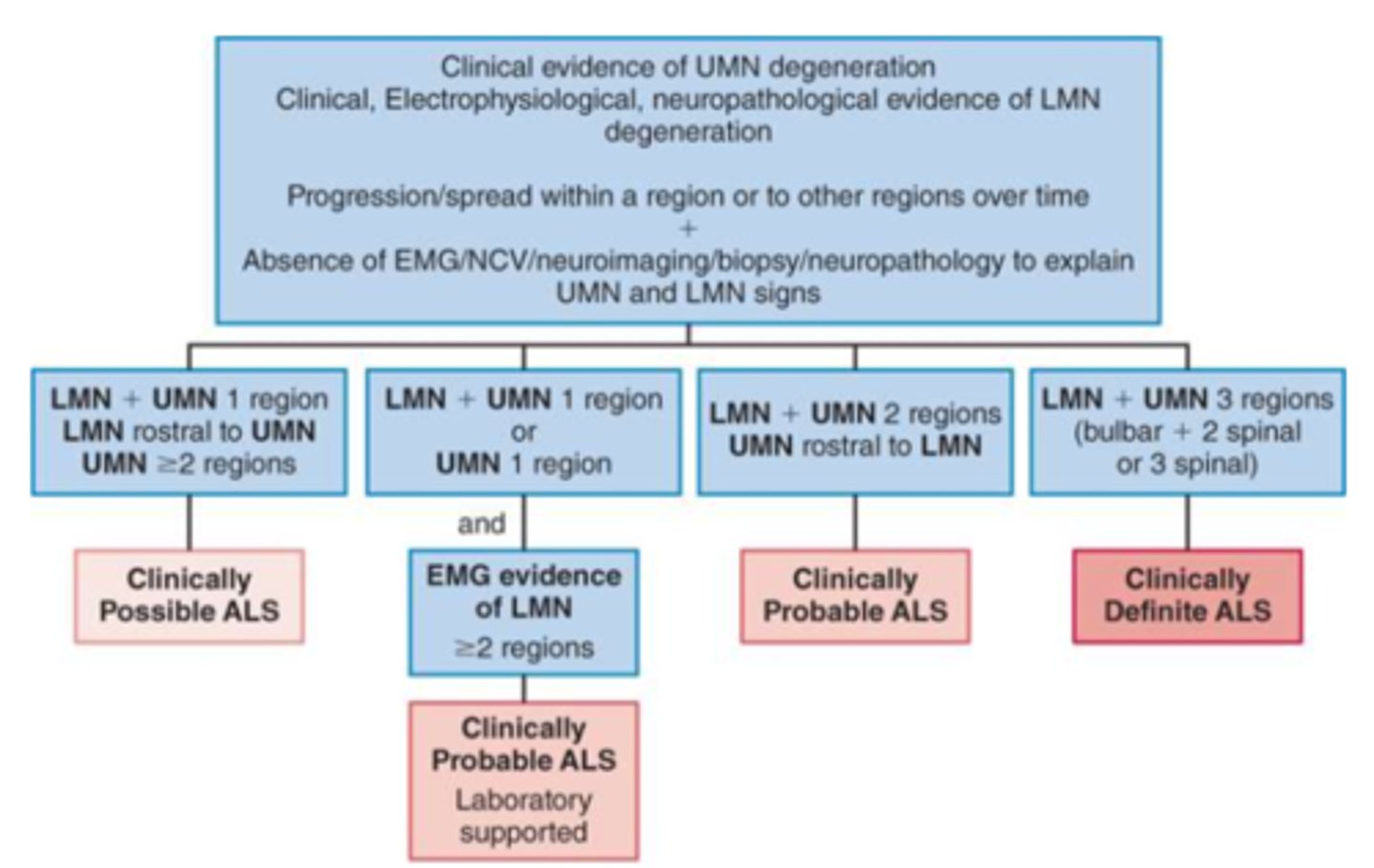
*El Escorial Criteria
DIAGNOSTIC TESTS:
(support diagnosis and exclude other diseases)
- imaging (MRI)
- lab studies
- EMG
- myelogram
- muscle/nerve biopsy
- biomarkers
El Escorial Criteria
used for ALS diagnosis
ALS prognosis
mean survival: 2-5 years
BETTER:
1) younger age of onset
2) limb onset
3) psychological wellbeing
WORSE:
1) bulbar muscle weakness onset
*life sustaining measures (respirator, feeding tube) to prolong life is a patient/family decision
ALS practice parameters
multidisciplinary centers are BEST
LEVEL A:
- Riluzole should be offered to slow disease progression
LEVEL B:
- PEG should be considered to stabilize weight & prolong survival in patients with ALS
- non-invasive ventilation (NIV) should be considered to treat respiratory insufficiency in order to lengthen survival
LEVEL C:
- NIV to slow decline of forced vital capacity and improve QOL
- early NIV may increase compliance
- insufflation/exsufflation to help clear secretions
disease modifying agents
ALS PHARMACOLOGY
aim to change the natural progression of the disease
1) Rilozule
(discontinue treatment if fatigue occurs)
2) Radicava
3) Relyvrio
4) Qalsody
symptomatic treatment
ALS PHARMACOLOGY
"palliative" - aimed at improving QOL through prevention and relief of suffering
- fatigue
- pain
- pseudobulbar palsy/affect
- depression
- constipation
- sailorrhea (drooling)
ALS PT exam
ACTIVITY:
ALS functional rating scale--> monitors functional change in a patient over time
- measures speech, salivation, swallowing, handwriting, cutting food and handling utensils, dressing & hygiene, turning in bed and adjusting bed clothes, walking, climbing stairs, breathing
PARTICIPATION:
ALS Assessment Questionnaire--> health related QOL
- measures physical mobility, ADLs, eating and drinking, communication, emotional functioning
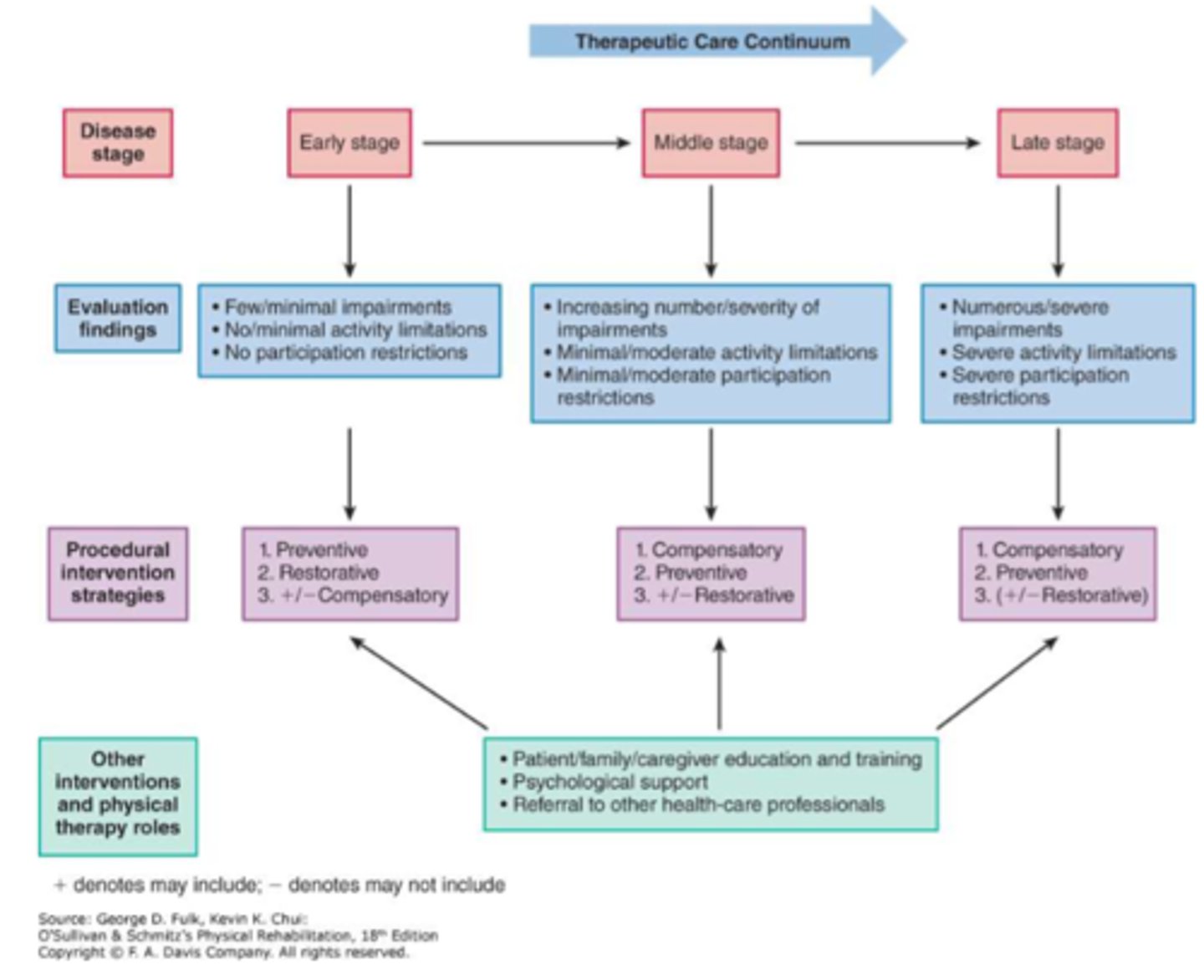
ALS PT intervention
STAGE SPECIFIC
1) EARLY - minimal disruption of ADLs function
preventative/restorative--> strengthening (must have at least 3/5 MMT score), stretching, A/AAROM, endurance (60-85% HR max 10 min bouts or continuous for 30)
AVOID-FATIGUE/OVERUSE
compensatory--> energy conservation, support group, adaptive equipment, ADs, environmental modifications
2) MIDDLE - W/C needed for long distances
preventative--> anti-pressure devices
restorative--> strengthening, stretching, endurance, A/AROM
compensatory--> adaptation of environment, support weak muscles (sling, braces, orthoses), ADs (w/c), caregiver training
3) LATE - W/C dependent or bed bound
compensatory--> caregiver training, mechanical lift
preventative--> pressure relieving devices (mattress for hospital bed, w/c), pulmonary/skin hygiene, PROM
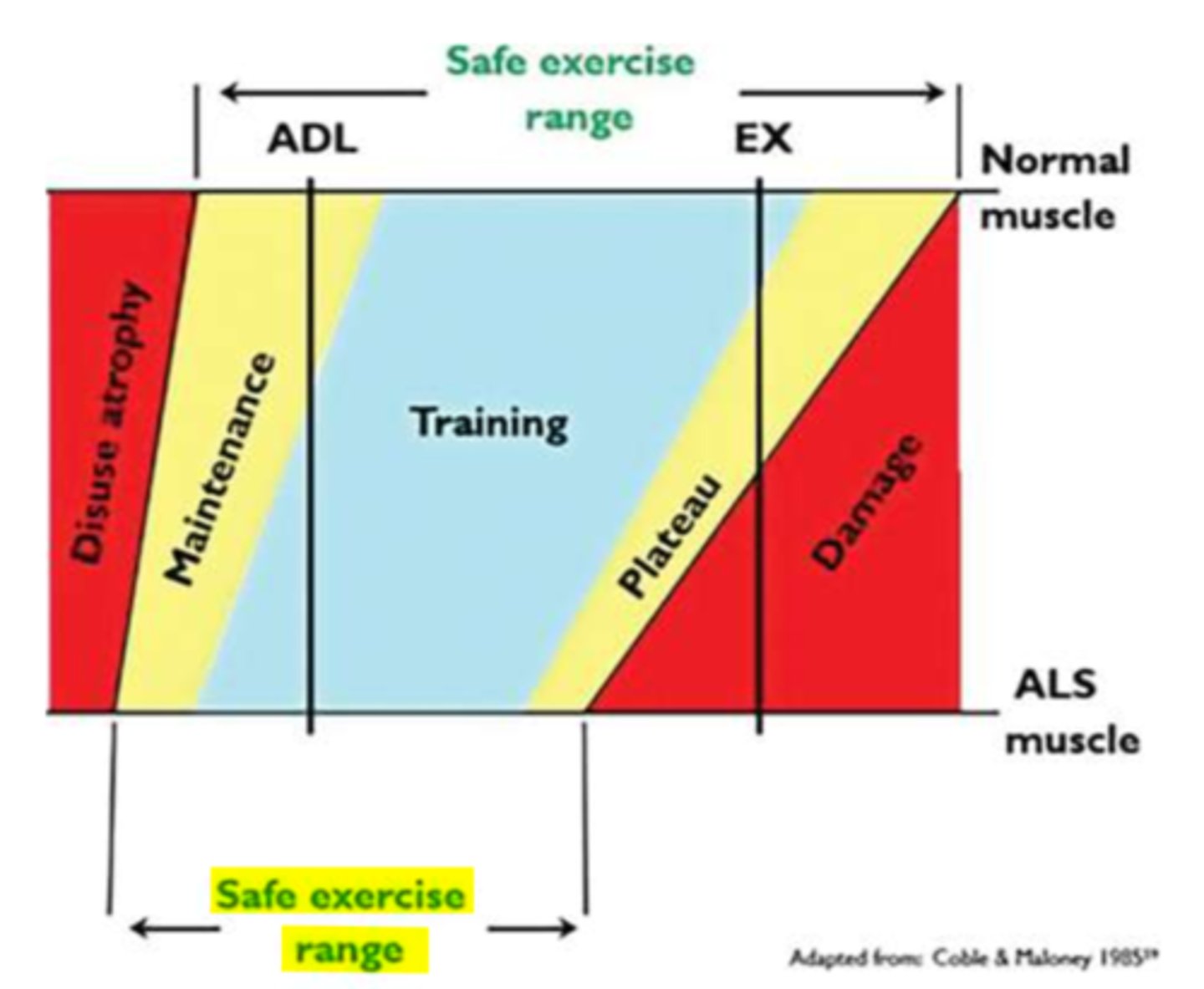
affected muscle group must have at least 3/5 MMT
What is the most important consideration for strengthening a patient with ALS?
rehab framework for progressive diseases
REFER TO IMAGE