Management of Impacted Teeth
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
tooth agenesis
-developmental absence of one or more teeth in the mouth
-occurs when the tooth fails to form during the growth process, typically due to genetic, environmental, or systemic factors
tooth malposition
-tooth in an abnormal position
tooth impaction
-tooth that fails to erupt into the dental arch within the usual range of expected time
why do teeth get impacted?
-we don’t really know
-differential growth rate of roots causes under or over rotation leading to impaction
-arch length: impacted third molars are larger than erupting third molars
-ectopic position: abnormal germ position puts teeth in contact with a denser external oblique ridge
-later mineralization: tooth growth lags behind maturation of jaws due to decreased influence of resorption of jaw
-attrition: softer diet leads to less attrition retaining mesiodistal space
options for ectopic teeth
-remove
-facilitate eruption
-monitor
indications for treatment- active surveillance
-if the tooth is malposed but not impacted and may possibly erupt given the patient’s age
-absence of symptoms
indications for treatment- facilitate eruption
-if the tooth is malposed but close to the arch and the patient has passed the age of normal eruption
-if the orthodontist thinks they can bring into the arch
-if there is adequate space in the arch
indications for treatment- prophylactic removal
-preventing periodontal disease
-preventing caries
-preventing pericoronitis
-preventing root resorption
-facilitation of orthodontic treatment
-prevention of odontogenic cysts and tumors
-prevention of jaw fractures
indications for treatment- symptomatic removal
-treating periodontal disease
-treating caries
-treating pericoronitis
-treating root resorption
-unexplained pain
information gathering
-CC
-HPI: OLDCARTS
-PMH
-PSH
-allergies
-medications
-social history
-family history with anesthesia
physical exam
-vitals- bp, SpO2, hr, rr, height, weight
-cranial nerve exam- V2/V3
-LAD
-swellings
-maximum incisal opening
-vestibular swelling
-erythema
-uvula position
-floor of mouth elevation
-palpate for impacted tooth
-probing depths
-oral hygiene
airway exam
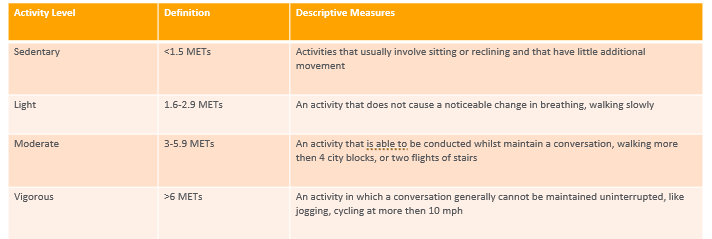
-metabolic equivalent tasks
-neck range of motion
-thyromental distance
-neck circumference
-maximum incisal opening
-facial hair
-heart and lung sounds
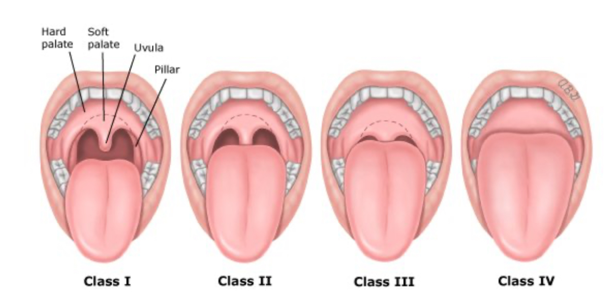
-Mallampati score
-impacted teeth are generally more difficult to take out- many times requires sedation
-important to do airway exam to determine if they are an appropriate candidate for in-office sedation v. the operating room
METS- activity level, definition, descriptive measures
Mallampati
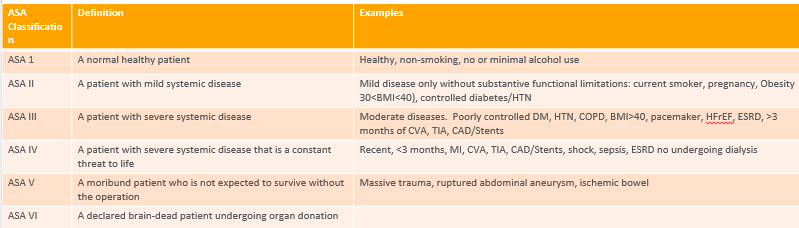
ASA classification, definition, examples
radiographic predictors of difficulty
-size of the follicular sac
-density of surrounding bone
-contact with mandibular second molar
-relationship to vital structures
-depth of impaction
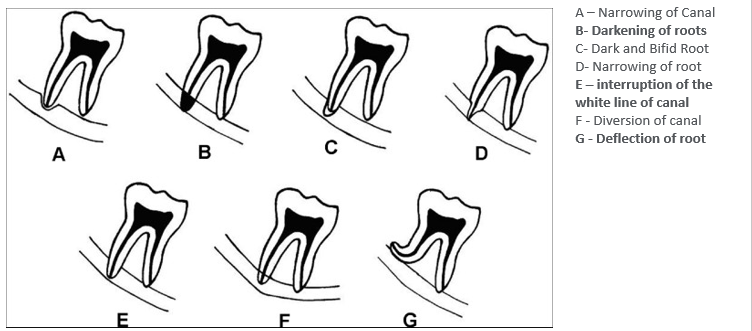
Rood’s criteria (prediction of IAN injury)
nature of overlying tissue
-PBI: tooth partially erupted but still stuck in bone
-FBI: tooth fully in bone
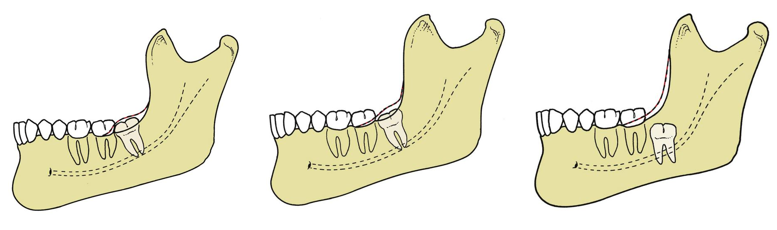
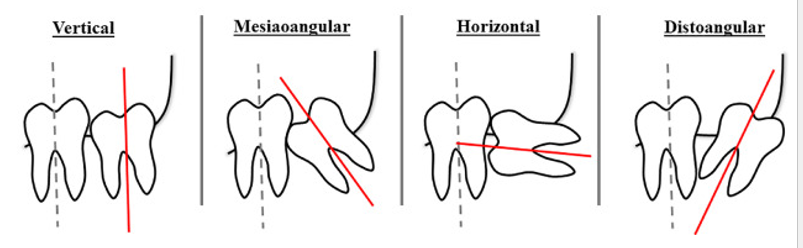
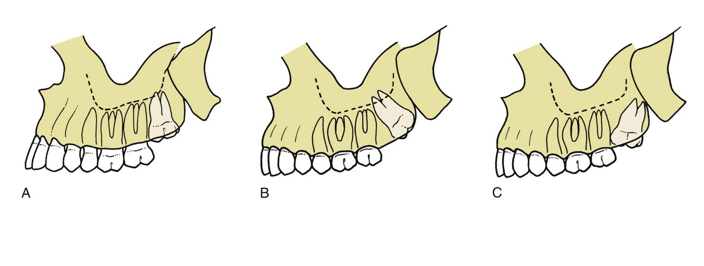
Winter’s classification of impaction
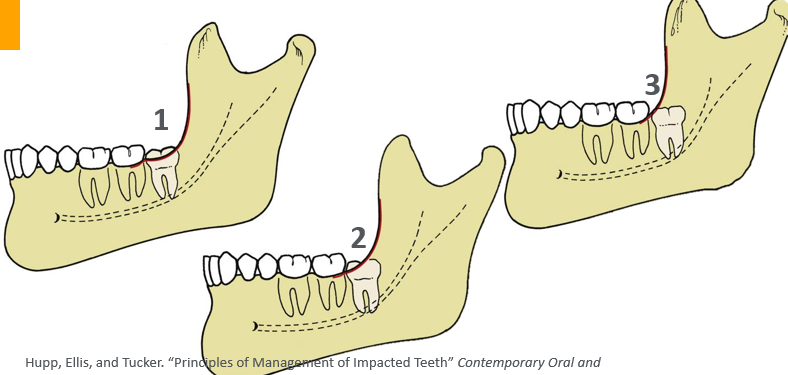
Pell and Gregory classification
-relates impaction to location of mandibular ramus
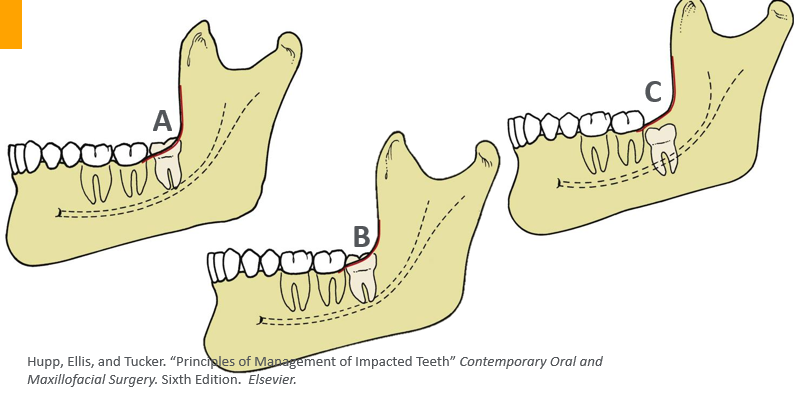
Pell and Gregory classification- ABC
-relates depth of impaction to second molar
classification systems for maxillary third molar impactions
factors that make impaction surgery less difficult
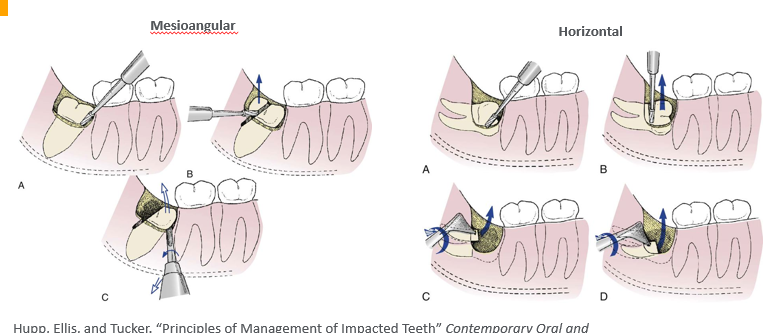
-mesioangular position
-pell and gregory class 1 ramus
-pell and gregory class A depth
-roots 1/3 to 2/3 formed (young pt)
-fused conical roots
-wide PDL (young pt)
-large follicle (young pt)
-elastic bone (young pt)
-separated from second molar
-separated from IAN (young pt)
-soft tissue impaction
factors that make impaction surgery more difficult
-distoangular position
-pell and gregory class 2 or 3 ramus
-pell and gregory class B or C depth
-long, thin roots (older patients)
-divergent curved roots
-narrow PDL
-thin follicle (older patients)
-dense, inelastic bone (older patients)
-contact with second molar
-close to inferior alveolar canal
-complete bony impaction (older patients)
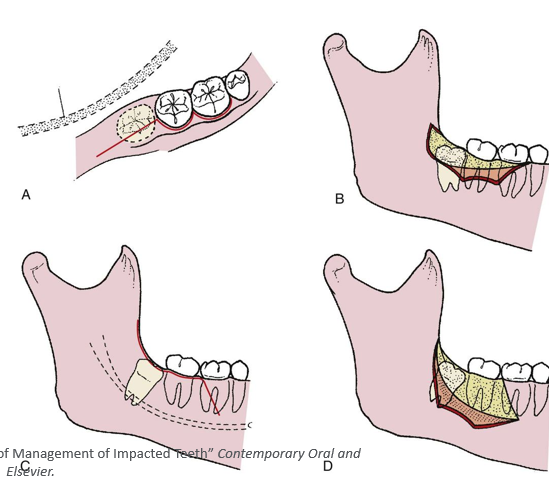
surgical procedure
-exposure
-bone removal
-tooth sectioning
-tooth removal
-surgical site closure
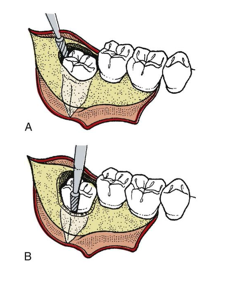
procedure- step 1
-access
procedure- step 2
-bone removal
procedure- step 3
-section tooth
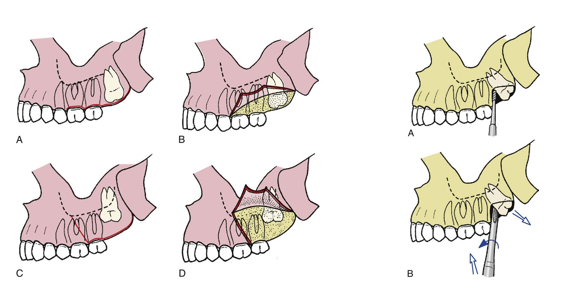
maxillary extractions
procedure- step 4
-surgical site closure
coronectomy
-removal all enamel
-3mm below buccal bone
-no mobile roots
post op care
-pain medication: ibuprofen 600 mg q6 PO, acetaminophen 500mg q6 PO, oxycodone 5 mg q6 PO x 6 tabs, amoxicillin 500mg TID x5 days?
-follow up one week
complications
-intra-op: tooth/root displacement (sinus, sublingual space, IAN canal, infratemporal fossa), mandible fracture, bleeding, nerve injury
-early: ecchymosis, thermal injury, bleeding, alveolar osteitis
-late: infection, osteomyelitis