Peds Exam #3 Cardiac/Neuro
1/70
Earn XP
Description and Tags
Cardiac and Neuro
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Key principles of congenital heart defects
-pressure gradients, flow, and resistance w/i circulation all play a role in physiology of each congenital defect
-blood flows form an area of
high pressure to one of low pressure
take the path of least resistance
-RIGHT side of the heart is the LOWER pressure system
-LEFT side of the heart is the HIGHER pressure system
-resistance in the pulmonary circulation is less than the resistance in systemic circulation
Types of cardiac defects
Congenital:
-anatomic = abnormal function present at birth
Acquired:
-due to disease process = infection, autoimmune disease environmental factors, familial tendencies
Cardiovascular dysfunction assessment
Hx and Physical exam:
-poor feeding
-tachypnea/ tachycardia
-failure to thrive/ poor weight gain
-activity intolerance, developmental delays
-positive prenatal hx
-positive family hx of cardiac delays
Assessment:
-Nutritional status = failure to thrive
-color = cyanosis and pallor
-chest deformities = results of an enlarged heart
-unusual pulsations = at times you will see visible pulsations of the neck
-respiratory excursion = tachypnea, dyspnea, grunting, retractions
-clubbing of fingers = associated w/ prolonged cyanosis
Auscultation and Palpation:
-heart rate and rhythm = tachycardia, bradycardia, irregular rhythms
-character of the sounds = distinct or muffled sounds, murmurs, additional heart sounds
-abdomen palpation = hepato/splenomegaly may be present
-thrills = in a child, are typically always associated w/ heart disease
vibratory sensation felt on the skin overlying an area of turbulence and indicates a loud heart murmur usually caused by an incompetent heart valve
-peripheral pulses = rate, regularity, and amplitude (strength)
Cardiac Catheterization
-diagnostic, interventional, electrophysiology
Pre-op:
-education
-NPO 4-6hrs prior to procedure; sedation may vary w/ patients
Post-Op:
-check pulses!!! Especially below cath site
-inspect temp and color of affected extremity
-assess BP, HR = any signs of hypotension, bradycardia, dysrhythmias
-check for bleeding; if bleeding, apply direct, firm continuous pressure 1 inch above insertion site
-educate family
Congenital heart disease
-major ccause of death in the first year of life (after prematurity)
-most common anomaly is ventricular septal defect (VSD)
-often associated w/ other genetic and syndrome anomalies
Trisomy 21, 13, 18
DiGeorge, Noonan, Williams, Holt-Oram
Classification of defects
-blood flows from an area of HIGER pressure to one of LOWER pressure
-blood takes the path of LEAST resistance
Acyanotic:
-LEFT TO RIGHT SHUNT
Atrial septal defect (ASD)
Ventricular Septal defect (VSD)
Patent Ductus Arteriosus (PDA)
Cyanotic:
-RIGHT TO LEFT SHUNT
Tetrology of Fallot
Defect of Pulmonary Veins
Blood flow patterns in the heart:
increased pulmonary blood flow
decreased pulmonary blood flow
obstruction to blood flow out of the heart
valvular = occurs at the site of the valve (mitral, pulmonic, aortic, etc.)
subvalvular = narrowing in the ventricle below the valve
supravalvular = narrowing of great artery above the valve
mixed blood flow
Defects w/ increased pulmonary blood flow
-abnormal opening/connection btwn the two sides of the heart
-increased blood volume shunted back to the right side of the heart
-increased pulmonary blood flow
-decreased systemic blood flow
-ASD, VSD, AV Canal, PDA
Atrial septal defect
-abnormal opening btwn the atria
-left to right shunt (acyanotic)
-may be asymptomatic; depends on size of defect
-HF if large
condition in which the heart can’t pump enough blood to meet the body’s needs
-murmur
-at risk for dysrhythmias, may be treated w/ anticoagulants
-may watch, surgical, cardiac cath
Ventricular septal defect
-abnormal opening btwn the ventricles
-left to right shunt (acyanotic)
-blood will typically shunt from the left to right and to the pulmonary artery
-pulmonary overload! Right ventricular hypertrophy!
-HF is common, loud murmur
-surgical management or cardiac catheterization placement of Dacron Patch
Atrioventricular canal defect
-incomplete fusion of the endocardial cushion. Low ASD, high VSD. Clefts of the mitral and tricuspid valves
-blood flows btwn all chambers of the heart
-direction of blood flow will be determined by systemic and pulmonary resistance
-left to right shunting
-moderate to severe HF, loud systolic murmur, mild cyanosis that increases w/ crying
-complete surgical repair
Patent Ductus Arteriosus (PDA)
-failure of the fetal ductus arteriosus (artery connecting the aorta and pulmonary artery) to close w/i the first weeks of life
-patency of the vessel allows blood to flow from the higher-pressure aorta to the lower-pressure pulmonary artery
-left to right shunt
-machinery like murmur
-closure w/ Indomethacin (50% rate of NEC), Neoprofen, or Surgical Ligation
-high rate in premature infants
Defects w/ decreased pulmonary blood flow
-obstruction of pulmonary blood flow and an anatomic defect btwn the right and left side of the heart
-since blood has difficulty exiting the right ventricle via the pulmonary artery, pressure on the right side increases, exceeding left sided pressure
-deoxygenated blood shunts to the left side of the heart and is sent out into the systemic
-hypoxia and cyanotic
-Tertralogy or Fallot, Tricuspid Atresia
Tetralogy of Fallot
-VSD, PS, overriding aorta, RV hypertrophy
-shunting of blood will be dependent on pulmonary and systemic resistance
-PS will decrease blood flow to the lungs = decreased oxygenated blood
-depending on the location of the aorta, blood from both ventricles may be sent to the systemic
Manifestations and Treatment:
-acute to mild cyanosis dependent on the severity of each defect and the amount of shunting
-acute episodes of cyanosis and hypoxia called “blue spells” or “tet spells”
-palliative surgery until large enough to undergo full repair
Blalock-Taussig shunt will provide blood flow to the pulmonary arteries. An end-to-side anastomosis (or connection w/ a small Gore-Tex tube) of the subclavian artery and the pulmonary artery
-complete repair w/i the first year of life. Goals are:
relief of RVOT obstruction
complete separation btwn the pulmonary and systemic circulations
preservation of RV function
minimize postprocedure pulmonary valvular incompetence
-dysrhythmias, HF, and surgical heart block are concerns pot op from complete repair
-the surgery consists of patch closure of the ventricular septal defect and enlargement of the ROVT, relieving obstructed pulmonary flow. RVOT enlargement is accomplished by relieving pulmonary stenosis, resecting infundibular and sub-infundibular muscle bundles, and if necessary by a transannular patch, creating unobstructed flow from RV into the PAs
Relieving hypercyanotic spells
-use a calm, comforting, approach
-place the infant or child in a knee-to-chest position
-provide supplemental oxygen
-administer morphine sulfate (0.1mg/kg IV, IM, or SQ), Supply IV fluids
-administer propranolol (0.1mg/kg IV)
Tricuspid Atresia
-tricuspid valve (btwn right atrium and ventricle) fails to develop in utero
NO COMMUNICATION BTWN RIGHT ATRIUM AND VENTRICLE
-blood will flow through an ASD or PFO to the left side of the heart, then through a VSD to get to the pulmonary arteries
-often seen w/ pulmonic stenosis or Transposition of the Great Arteries
-mixing of blood in the left ventricle causes systemic desaturation
Manifestations:
-mild symptoms at first due to PDA allowing blood to flow to the lungs
-cyanosis, dyspnea, tachycardia
Treatment:
-for infants whose pulmonary blood flow is dependent on the PDA, prostaglandin E is continuously infused until surgical correction
-palliation w/ Blalock-Taussing shunt or pulmonary artery banding may be performed
-increase pulmonary blood flow w/ Glenn Procedure around 3-6 months of age, widen the ASD if necessary. Move to a Fontan procedure for long term correction around 2-5 years old
Obstructive Defects
-blood exiting the heart, meets an area of narrowing or stenosis; therefore impeding systemic blood flow
-pressure in the ventricle and the artery below the narrowing have increased pressures
-increased intracardiac pressures w/ ↓ cardiac output
-typically, the children will show signs of HF
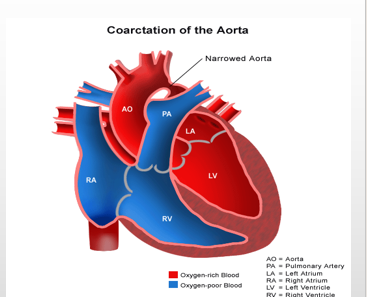
Coarctation of the aorta
-localized narrowing of the aorta, typically at the level of the ductus arteriosus
-increased pressures to the head and upper extremities, decreased pressure to the lower extremities
-bounding upper pulses, lower or absent lower pulses. CHECK FEMORAL PULSES
-high BP of arms, low BP of legs, cool limbs, headache, dizziness, fainting, epistaxis
-if undiagnosed, we fear RUPTURED AORTA
-surgical repair before 6mo
-resection of the narrowed portion, followed by end-to-end reanastomosis
Aortic stenosis
-stricture of the aortic valve, causing decreased cardiac output and increased pressure on the left ventricle
-LV hypertrophy = which can lead to pulmonary HTN (pulmonary vascular congestion), coronary artery perfusion (MI)
-typical fusion of the cusps
-faint pulses, hypotension w/ tachycardia, poor feeding, chest pain, dizziness when standing
-surgical correction = aortic valvotomy
Pulmonic stenosis
-narrowing at the entrance to the pulmonary artery
-RV hypertrophy and decreased pulmonary blood flow
-PDA may help to shunt blood from aorta to the pulmonary artery
-if severe cyanotic and cardiomegaly
-balloon angioplasty
Mixed defects
-complex defects where there is a mixing of pulmonary and systemic circulations
-desaturation of the systemic blood flow
-these pts have a variable picture that depends on the severity of the defect
-there will always be some degree of desaturation but w/o cyanosis
-HF
Transposition of the Great vessels
-pulmonary artery and the aorta are transposed from their normal positions
-the aorta arises from the right ventricle instead of the left ventricle and the pulmonary artery arises from the left ventricle instead of the right ventricle
-often the ductus arteriosus remains patent, allowing for some mixing of blood
-IV prostaglandin indicated for temporary maintenance of ductus arteriosus patency
-corrective surgery is usually performed by age 4-7days
Total anomalous pulmonary venous return (TAPVR)
-failure of the pulmonary veins to join up w/ left atrium
-mixed blood is returned to right atrium and shunted right to left through ASD
-cyanosis early in life w/ rapid deterioration. Death w/o intervention
-surgical = pulmonary veins are anastomosed back to the left atrium
Truncus Arteriosus
-failure of the pulmonary artery and aorta to divide
-single vessel that overrides both ventricles
-there is mixed blood w/ a greater portion going to the pulmonary artery versus out the aorta
-variable cyanosis, poor growth, activity intolerance
-surgical repair in 1st month of life
Hypoplastic left heart
-underdevelopment of the left side of the heart causing hypoplastic left heart and aortic atresia
-these pts cannot oxygenate the systemic
-dependent ASD and PDA
-ventilated at birth
-heart transplant is the treatment of choice
-three step surgery (Norwood, Glenn, Fontan)
-death rates are still very high
Congestive Heart failure
-inability of the heart to pump an adequate amount of blood to the systemic circulation at normal filing pressures to meet the body’s metabolic demand
-mainly, secondary to structural abnormalities
-myocardial failure which impairs contractility of the ventricles (cardiomyopathy, dysrhythmias, severe electrolyte disturbances)
-excessive demands = severe anemia, sepsis
-categorized as right sided and left sided
Manifestations:
-impaired myocardial function = sweating, tachycardia, fatigue, pallor, cool extremities w/ weak pulses, hypotension, gallop rhythm, cardiomegaly
-pulmonary congestion = tachypnea, dyspnea, retractions, nasal flaring, grunting, wheezing, cyanosis, cough, orthopnea, exercise intolerance
-systemic venous congestion = hepatomegaly, peripheral edema, ascites, neck vein distention, periorbital edema, weight gain
HF management
-improve cardiac function
digoxin for increased contractility
in an infant withhold digoxin if HR < 90
in children withhold digoxin if HR < 70
BBs and ACE inhibitors to reduce cardiac afterload, antihypertensives if needed
-remove accumulated fluid and sodium
diuretics
-decrease cardiac demands
treat fevers and infection
prevent cold or heat stress
reducing the effort of breathing
sedating an irritable child
rest
-improve tissue oxygenation
Hypoxemia
-condition in which arterial oxygen pressure (PaO2) is less than normal. Decreased arterial O2 sat
-decreased tissue oxygenation
-decreased oxygenation of the blood
cyanosis = blue discoloration of the mucous membranes, skin, and nail beds w/ reduced oxygen saturation
polycythemia = due to chronic hypoxia. Increased risk of blood clot formation
clubbing of fingernails bc of hypoxia and polycythemia
Infective endocarditis (bacterial)
-an infection of the inner lining of the endocardium (inner lining of the heart). Typically involves the VALVES
-most often a result of bacteremia paired w/ acquired or congenital anomalies
-especially children w/ prosthetic valves, shunts, recent cardiac surgery w/ invasive lines, and rheumatic heart disease w/ valve involvement
-agents = staph, strep, candida
-if pt is in the high risk group = prophylaxis antibiotics 1hr prior to dental and invasive procedure
Rheumatic fever
-inflammatory disease that occurs after infections w/ GABHS pharyngitis w/i 2 to 6 wks
-often in late school age children and adolescents
-self limited illness that involves the joints, skin, brain, serous surfaces, and heart
-often causes cardiac valve damage (referred to as RHEUMATIC HEART DISEASE) is the most significant complication. Most often the MITRAL VALVE
-due to improved treatment of GABHS, rheumatic fever and heart disease are uncommon
-prevention and treatment of GABHS infections prevents RF
-diagnosed based on modified Jones criteria
-throat culture for GABHS = currently recommend screen all school-aged children who have sore throats
-blood antistreptolysin O titer = elevated or rising titer, most reliable diagnostic test
-CRP elevated in response to an inflammatory reaction
-ESR elevated in response to an inflammatory reaction
Rheumatic fever diagnostics/ Management
Modified Jones Criteria:
-the child should demonstrate the presence of two major criteria or the presence of one major criteria and two minor criteria following an acute infections w/ GABHS
-Major Criteria
carditis
subcutaneous nodules = abnormal bumps or masses appear in the fatty layer under the skin of the legs, thighs, and buttocks. In some cases the arms, abdomen, and/or face may be involved. Usually 1-2 cm wide and may be either painful and tender or painless
polyarthritis = 5+ joints affected w/ joint pain
rash (erythema marginatum)
chorea = movement disorder that causes involuntary, irregular, unpredictable muscle movements. The disorder can make you look like you’re dancing or look restless or fidgety
-Minor criteria
fever
arthralgia
Management:
-eradication of the hemolytic streptococci
-prevention of recurrent streptococci
-prevention of permanent cardiac damage
-supportive therapy of other symptoms
-prophylactic treatment against recurrent RF:
monthly IM injections of penicillin VK, or
once daily dose of sulfadiazine
Cardiac dysrhythmias
-can occur in children w/ normal hearts
-common after cardiac surgery (especially right sided)
-secondary to metabolic and electrolyte disturbances
Cardiomyopathy
-abnormality of the myocardium in which the cardiac muscle’s ability to contract is impaired
-causes
infection, cardiac dysfunction, secondary to medications
kawasaki disease
D. muscular dystrophy
-Treatment = is IRREVERSIBLE. Treatment is centered on managing their heart failure
Pulmonary Hypertension (PAH)
-high blood pressure in the arteries of the lungs that is a progressive and eventually fatal disease
-there is no cure
Manifestations:
-dyspnea w/ exercise
-chest pain
-syncope
Diagnosis:
-CXR, electrocardiogram, echocardiogram, cardiac cath
Management:
-prepare the child and family for possible lung transplantation
-educate family to avoid high altitude areas bc of hypoxia
-consider supplemental O2 therapy
Kawasaki Disease
-acute systemic vasculitis of unknown cause
-20% of children develop coronary artery dilation or aneurysm formation
-etiology is unknown and it is not spread by person-to-person contact
-extensive inflammation of the arterioles, venules, and capillaries
Manifestations:
-polymorphous rash w/ edema and erythema of the palms and soles that peels in later stages
-bilateral conjunctiva infection
-erythema of the oral mucous membranes s/a the lips “strawberry tongue” large papillae are exposed
-cervical lymphadenopathy
-fever greater than 39.9 celsius of at least 5 days duration that is unresponsive to treatment
-chills, headache, joint pain, abdominal pain, malaise, extreme irritability, vomiting, diarrhea
Kawasaki management
-the disease itself is self-limiting w/ treatment centered on supportive therapy
-anticipate administration of aspirin and immunoglobulin
-monitoring for the extent of cardiac involvement
-screen for heart disease as child ages
blood cholesterol testing
blood pressure monitoring
periodic imaging of the heart
long term follow up is determined based on if there was coronary damage
Shock
CIRCULATORY FAILURE
-cardiogenic shock results from impaired cardiac function that leads to a ↓ in circulation
cardiogenic shock can be seen in children following cardiac surgery and w/ acute dysrhythmias, congestive HF, trauma, or cardiomyopathy
-anaphylactic shock results from a hypersensitivity to a foreign substance that leads to massive vasodilation and capillary leak and can occur in response to an allergy to latex or drugs, insect stings, or blood transfusions
anaphylaxis can be seen in children who have allergies, asthma, or a family hx of anaphylaxis
-while the causes may differ, the physiologic consequences are the same = hypotension, tissue hypoxia, metabolic acidosis
Symptoms:
-dyspnea
-breath sounds w/ crackles
-grunting
-hypotension
-tachycardia
-weak peripheral pulses
Shock management
-Ventilation
establish airway; prepared for intubation
administer O2 at 100%
-Fluid Administration
restore fluid volumes as ordered
-Cardiovascular support
administer epinephrine 1:1000 SC or IV
-General support
keep child flat w/ legs raised above heart level
keep warm and calm
Pediatric neuro differences
-neural tube develops w/i the first 3-4 weeks of gestation: infection, trauma, teratogens, and poor nutrition during this period can result in malformations of the brain and spine development
-at birth, cranial bones are not fused
-brain is more vascular = capillaries and major vessels are fragile. Preemies at high risk for IVH
-myelination is not complete
myelinization proceeds in the cephalocaudal direction. For example, infants can control the head and neck before the trunk and extremities
-brain takes up less room in the cranium. Fontanels allow for brain growth after birth
-head circumference: measure at the largest point until age 2-3 and plot on growth chart
-fontanels: anterior and posterior
Level of Consciousness (LOC)
-full consciousness: a stste in which the child is awake and alert; is oriented to time, place, and person; and exhibits age-appropriate behaviors
-confusion
-obtunded: a state in which the child has limited responses to the environment and falls asleep unless stimulation is provided
-stupor: when the child responds to vigorous stimulation
-coma: a state in which the child cannot be aroused, even w/ painful stimuli
-parents often first to notice changes in their child’s LOC
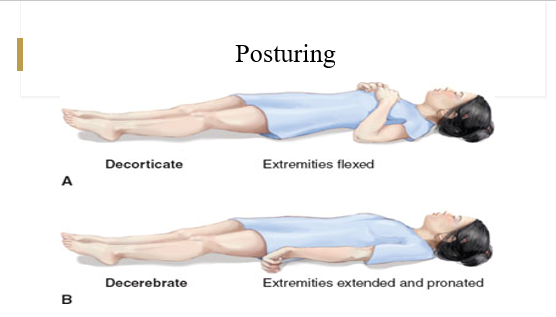
Posturing
-an involuntary flexion or extension of the arms and legs, indicating severe brain injury
Seizures
-abnormal excessive electrical impulses
-up to 10% of all children experience a seizure
-most are caused by disorders that originate outside the brain = high fever, infection, head trauma, hypoxia toxins, cardiac arrhythmias
-most children outgrow seizures w/o negative repercussions
-classified according to their type and etiology
focal seizures involve one area of the brain
generalized seizures involve the entire brain
Risk factors:
-fever, cerebral edema, intracranial infection or hemorrhage
-brain tumors/cysts, anoxia, toxins or drugs
-lead poisoning, tetanus, shigella, salmonella, hypoglycemia, hypocalcemia, alkalosis, hyponatremia, hypernatremia, hypomagnesemia
Febrile seizures
-usually last less than 1 minute
-seen in children less than 5 years of age
-associated w/ a fever that is not the result of an intracranial infection or metabolic imbalance and are usually related to viral illness
-usually benign w/ no long-term effects
-when a child has a febrile seizure, you must look for underlying dangerous infection (meningitis, etc.)
-usually associated w/ how quickly the fever spikes not necessarily how high the fever is
-look for underlying illness however most are viral related
-there are rectal, buccal, and intranasal medication options to stop seizures
-very frightening to parents
Neonatal seizures
-seizures that occur w/i the first 4 weeks of life (most commonly the first 10 days)
-the immature brain is more prone to seizure activity and metabolic, infectious, structural, and toxic diseases = ischemic encephalopathy, hypoglycemia, meningitis, cerebral infarction, intracranial hemorrhage
-research does indicate that neonatal seizures place the child at risk for further cognitive impairment = cognitive delays, behavioral problems, epileptic complications later in life
-most are associated w/ a specific underlying cause s/a hypoxic ischemic encephalopathy (most common), metabolic disorders (hypoglycemia and hypocalcemia), neonatal infection (meningitis and encehalitis), cerebral infarction, and intracranial hemorrhage
-can often mimic normal newborn behaviors = sucking, stretching, etc.
-treat the underlying cause, treat aggressively to mitigate long-term effects of repeated seizures. Phenobarbital is often used in the initial management of neonatal seizures
-the prognosis depends mainly on the underlying cause of the siezures and the severity of the insult
Tonic clonic seizures
-previously called gran mal seizures
-have 3 phases = tonic, clonic, and post-ictal
-aura sometimes
-most prevalent type
-tongue biting
-seizures lasting 5 minutes will typically go at least 30 if left untreated = permanent damage results w/ a 30 minute seizure, orders to treat after 5 min
Absence seizures
-onset btwn ages of 4-12 years and ceases usually by adolescnece
-loss of consciousness lasting 5-10 seconds
-motionless, blank stare
-minimal or no change in behavior
-resembles daydreaming or inattentiveness
-automatisms: lip smacking, twitching of eyelids or face, or slight hand movements
-unable to recall episodes, but can be momentarily confused
-can immediately resume previous activities
Focal seizures
-Aversive seizure (most common): eyes and head turn away from the side of focus, w/ or w/o loss of consciousness
-Rolandic (Sylvan) seizure: tonic-clonic movements involving the face, salivation, arrested sleep, and most common during sleep
-inability to respond to the environment
-impaired consciousness but regains in less than 5 min
-confusion and inability to recall event
-aura: warning of onset of seizure activity that can be a a strange feeling in the throat, and odor, or taste. It can also produce auditory or visual hallucinations, feelings of fear, distorted sense of time and self
Epilepsy
-seizures are triggered (chronic) recurrently from w/i the brain. A diagnosis of epilepsy is made if a client has two unprovoked seizures at least 24hrs apart
-acquired, brain injury, familial tendency, many cases unknown
-management will focus on controlling seizures or reducing their frequency
-teach the family, child, and those involved in care how to manage the pt during an active seizure
-emotional support = devastating impact on quality of life
Patient education during seizure
-remain calm
-ease the child to the ground and place on side, MAINTAIN AIRWAY
-time the seizure episode
-remove anything tight around the neck
-do not restrain the child
-remove hazards
-do not forcibly open jaw w/ tongue blade, spoon, fingers, etc
-document = length, movements, cyanosis, loss of bladder control
-remain w/ child until fully conscious
When to call EMS:
-first seizure
-stops breathing
-unresponsive
-any injury has occurred or occurred in the water
-seizure lasts longer than 5 min
-unequal pupils following seizure
-vomiting (30 mins continuously after end of seizure)
Nursing care of seizures
-Labs: lead level, CBC, blood glucose, serum electrolytes, metabolic panel, toxicology screen, chromosomal analysis
-Diagnostics: EEG, MRI, LP, CT
-Medications: Diazepam, phenytoin, carbamazepine, valproic acid, and fodphenytoing sodium, topiramate, lamotrigine, clonazepam = usually starts w/ a single dose (low) then increases until seizures are controlled. Sometimes will add another medication
-Surgical: VNS, brain surgery
Ketogenic diet (Seizures)
-this diet is a special high-fat, low-carb diet that helps to control seizures in some people w/ epilepsy
-ketone are formed when the body uses fat for its source of energy
-usually the body uses carb for its fuel. Bc the ketogenic diet is very low in carbs, fats become the primary fuel instead
-ketones can be detected in the urine, blood, and breath
-ketones are one of the more likely mechanisms of actions of the diet, w. higher ketone levels often leading to improved seizure control
Status epilepticus
-prolonged seizure = usually over 30 min
-requires urgent intervention to prevent brain anoxia and long term complications
-maintain airway
-IV access
-loading dose of lorazepam or diazepam followed by an antiepileptic
-draw labs
Meningitis
-inflammation of the crebrospinal fluid and meninges (connective tissue that cover the brain and spinal cord)
-Viral: CMV, adenovirus, mumps, herpes simplex, arbovirus
-Bacterial:
meningococal, strep pneumoniae, HIB, E. coli. Incidence of bacterial meningitis has significantly decreased since the introduction of Hib and pneumococcal vaccine
injuries that provide direct access to CSF (skull fx, pentrating head wound)
crowded living conditions
-in developed countries, disease resulting from Hib once the most common cause of bacterial meningitis in children, has decreased dramatically since introduction of Hib vaccine
-no significant decrease found in infants less than 2 months
-bacterial meningitis is a medical emergency and requires prompt hospitalization and treatment. Deterioration may be rapid and occur in less than 24hrs
Meningitis manifestations
-suden onset
-preceding respiratory illness
-photophobia
-N/V, irritability, headache, stiff neck
-rash = petechial or purple rasj (purpura) indicative of meningococcemia = EMERGENCY
-drowsiness, lethargy
-muscle rigidity
-seizures
-bulging fontanel
Meningitis Assessment
Newborn:
-no illness present at birth, butit progresses w/i a few days
-manifestations are vague and hardest to diagnose
poor muscle tone, weak cry, poor suck, refuses feeding, vomiting, diarrhea
possible fever or hypothermia
-neck is supple w/o nuchal rigidity (early)
-bulging fontanels/nuchal rigidity are late signs
3mo- 2yo:
-seizures, fever, weak cry, irritability
-bulging fontanels, possible nuchal rigidity, poor feeding
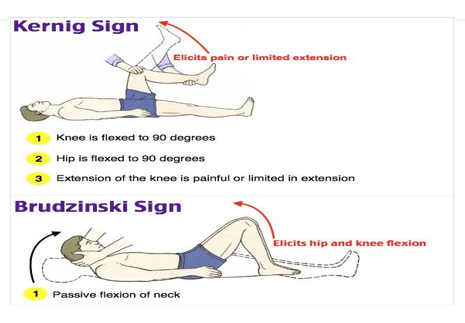
-vomiting, Brudzinski’s sign and Kernigs sign are not reliable
2yo - Adolescence:
-seizures, nuchal rigidity, positive Brudzinski and Kernig signs
-fever and chills, headache, vomiting, irritability and restlessness
-petechiae or purpuric rash = does NOT blanche
Lumbar puncture
-definitive diagnostic for meningitis
-withdrawal of CSF from the subarachnoid space for analysis
-nurses need to be able to assist w/ proper positioning
-apply EMLA cream to punture site 30-60min prior to procedure
-strict asespsis
-collection and transport of sample (hand deliver to lab) usually 3-5 tubes
-keep child flat for 1hr if ordered
-bacterial:
cloudy color, elevated WBC, elevated protein count, decreased glucose count, positive gram stain
-viral:
clear color, slightly elevated WBC, normal or slightly elevated protein count, normal glucose, negative gram stain
Neonatal:
Meningitis management
-petechiae or purpuric type rash requires immediate medical attention
-isolate (droplet precautions) the pt as soon as meningitis is suspected
-Labs: CBC, blood cultures
-Diagnostics: lumbar puncture, CT, MRI
-Infants: daily head circumference measurement
-frequent vitals, fluid status, neurologic status, pain level
-restrict fluids until no evidence of increased IOP and serum sodium levels are WNL
-reducing fevers is improtant to help maintain optimal cerebral perfusion by reducing the metabolic needs of the brain
-a low temp can be indicative of infection in infants = serious infections like meningitis or sepsis can cause low body temps in infants
Medications:
-Viral
supportive therapy only; analgesics
-Bacterial:
antibiotics = typically 10 days of IV antibiotics
dexamethasone = initial management of increased ICP
analgesics = make sure to check temp before administering to ensure you are not masking fevers
Meningitis complications
-increased ICP
-Headache, vomiting, bulging fontanels, distended scalp veins, high-pitched cry, brady cardia, increased irritability
-hearing loss
-provide interventions to reduce ICP = minimize straining, coughing, decrease stimuli, promote rest
Hydrocephalus
-not a specific illness yet a result of an underlying cause
-imbalance of production and absoprtion of CSF
-enlarged ventricles
-increased ICP
-noncommunicating
flow of CSF from the ventricles to subaracnoid space is obstructed
-communicating
flow is not obstructed, but CSF is inadequately reabsorbed in the subarachnoid space
VP shunt = typical treatment
Chiari malformation
-structural defects where the lower part of your brain presses on and through an opening in the base of the skull and cerebellum into the brain that controls balance
-symptoms include pain and trouble swallowing
-treatment may involve monitoring and surgery. Medication may be given to manage symptoms like pain
Increased ICP
-monitor w/ any child w/ potential or suspected neurological disorder
head trauma, birth injury, infection, hydrocephalus, brain tumors
-as ICP increases, LOC decreases and the s/sx become more pronounced
-early recognition is key w/ immediate intervention
-prevention of long-term damage
Early signs:
-headache, vomiting (possibly projectile), dizziness, decreased pulse and respirations
-blurred vision, pupil rxn time decreased or unequal
-sunsetting of the eyes
-increased BP and pulse pressure
-changes i LOC, irritability, seizure activity
-infant = bulging fontanel, widened sutures, high pithed cry, dilated scalp veins
Late signs:
-low LOC
-decreased motor and sensory response
-bradycardia, irregular respiration, cheyne-stokes respiration
-decerebrate and decorticate posturing
-fixed and dilated pupils
Management Increased ICP
-keep head midline w/ HOB elevated 30 degrees
-avoid extreme flexion, extension, or rotation
-minimize oral suctioning
-instruct the pt to avoid coughing, blowing the nose, straining
-REST
Reye syndrome
-primarily effects liver and brain that ultimately leads to liver failure and cerebral edema = could result in death in hours from onset
-not completely understood
-high association btwn using aspirin to treat a fever caused by a viral illness (influenza, gastritis, varicella)
Symptoms:
-recent viral illness or use of aspirin or aspirin containing products w/i 3 weeks of onset (Alka Seltzer, Pepto-Bismol, ASA)
-lethargy, irritability, combativeness
-confusion, delirium, profuse vomiting, seizures, loss of consciousness, death
Reye syndrome management
-Labs: liver enzymes (ALT and AST), serum ammonia levels, serum electrolytes, clotting factors
-liver biopsy
-CSF to rule out meningitis
-assess and maintain airway
-restrict fluids - risk of ↑ICP
-monitor pain, position for comfort
-seizure precautions
-osmotic diuretic: mannitol = to decrease cerebral swelling
-vitamin K = improves blood clotting
-interprofessional care for post deficits if needed = OT, PT, dietician
-elevated liver function tests and elevated serum ammonia level can confirm diagnosis
-Nursing management is aimed at maintaining cerebral perfusion, managing and preventing ↑ICP, providing safety measures due to changes in LOC and risk for seizures, and monitoring fluid status to prevent dehydration and overhydration
Head Injuries
-larger head size in relation to body coupled w/ a higher center of gravity, causes the child to hit his or her head more readily when involved in motor vehicle accidents, bicycle accidents, and falls
-spinal cord injuries can result also
Findings (severe ↑ICP)
-bulging fontanels, cheyne-stoke respirations
-posturing, bradycardia, decreased LOC, coma, pupillary response alterations
Progression of Injury:
-marked changes in vital signs
-altered mental status
-focal neurologic deficits
-increased agitation
-vomiting
Monitoring severe injury:
-↑ICP
-Infants = bulging fontanels, separation of cranial sutures, irritability, increased sleeping, high-pitched cry, poor feeding, sun-setting sign
-Children = nausea, headache, forceful vomiting, blurred vision, increased sleeping, inability to follow simple commands, seizures
Concussion
-type of traumatic brain injury (TBI) that is caused by a bump, blow, jolt, jarring, or shaking and results in disruption or malfunction of the electrical activities of he brain
-most common head injury
-confusion and amnesia after the head injury are seen
-loss of consciousness may or may not occur
-noted symptoms may include increased distractibility and difficulty w/ concentration
-treatment includes rest and monitoring for neurologic changes that could indicate a more severe injury, s/a increased sleepiness, worsening headache, increased vomiting, worsening confusion, difficulty walking or talking, changes in LOC, and seizures require immediate follow up
CSF (head injury)
-if clear fluid is noted raining from the ears or nose, notify the physician immediately
-if fluid test postive for glucose, this is indicative of leaking CSF
Sub-setting eyes
-clinical phenomenon encountered in infants and young children w/ raised ICP (seen in up to 40% of children w/ obstructive hydrocephalus and 13% of children w/ shunt dysfunction)
-consists of an up-gaze paresis w/ the eyes appearing driven downward
Management of Head injuries
-Labs: ABGs, blood alcohol and toxicology, CBC, liver function
-Cervical spine xrays
-CT, MRI
-measurement of ICP
Therapeutic Interventions:
-transfontanel percutaneous aspiration
-subdural drains
-placement of burr hole
-craniotomy
involves removal of part of the skull
the bone is replaced once the edema has resolved
-for depressed fractues, surgery to elevate the depression
Prevention:
-wear helments when riding bike, scooter, shateborading, ATV, motorcycle, skiing, playing football
-seat belts
-avoiding dangerous activities
-never shake a body
-keep children well supervised
Head injury complications
-epidural hematoma: bleeding btwn the dura and the skull
-subdural hematoma: bleeding btwn the dura and the arachnoid space
-cerebral edema/ increased ICP
-brain herniation: loss of blinking reflex; cushing triand
hypertension, bradycardia, respiratory distress
Shaken Baby Syndrome (SBS)
-the infants large head size an weak neck muscles place then at an increased risk for head trauma due to violent shaking or cranial impacts
-the full appearance of neurologic deficits resulting from nonaccidental head trauma may take several years to be identified and recovery can be very slow
-be alert to any discrepancies btwn the physical injuries and the hx of injury
-a serious brain injury resulting from forcefully shaking and infant or toddler. It’s also known as abusive head trauma, shaken impact syndrome, inflicted head injury, or whiplash shaken infnat syndrome
-injuries that might not be immediately seen include bleeding in the brain and eyes, spinal cord damage, and fracture of the ribs, skull, legs, and other bones
-many children w/ shaken baby syndrome show s/sx of prior child abuse
Down syndrome
-most common chromosomal abnormality
-AMA
-increased risk for leukemia
-cardiac anomalies
-thyroid dysfunction
-ocular and earing deficiencies
Expected findings:
-separated saggital suture, enlarged anterior fontanel, small round head
-occipital are of head flattened, upward/outward slant to eyes
-small nose w/ depressed nasal bridge (saddle nose)
-small ears w/ short pinna
-epicanthal folds observed in ocular areas, high arched narrow palate
-protruding tongue, short/broad neck, shortened rib cage
-possible congenital heart defects, protruding abdomen
-incurved fifth finger (clinodactyly)
-broad, short feet and hands w/ stubby toes and fingers
-transverse palmar crease
-large space btwn big and second toes w/ plantar crease
-short stature
-hyperfelxibility, muscle weakness, and hypotonia
-dry skin that cracks easily