PHAR 211 Exam 2 (RENAL and HOMEOSTASIS)
1/166
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
167 Terms
Renal Cortex
The outer wall
nephrons found here
blood filtration, urine formation, fluid homeostasis
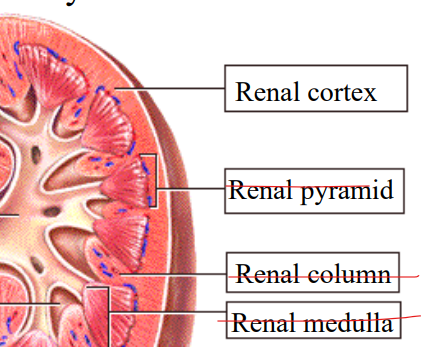
Renal pyramid
triangles
concentrate urine, maintain salt-water balance, transporting urine to the renal pelvis

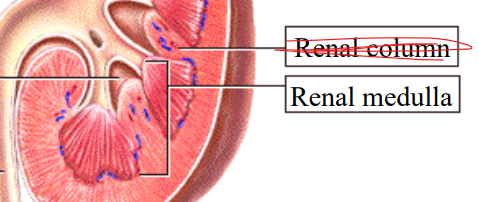
Renal column
the little channel spaces in between each triangle
structural support, conduits (channels)
supply blood to the nephrons and urine formation

Renal medulla
nephrons here (in inner medulla)
concentrate urine and maintain body water and electrolyte homeostasis
utilizes loop of Henle
Ureter
Transport tube
primary transport highway for urine from the kidney to the bladder
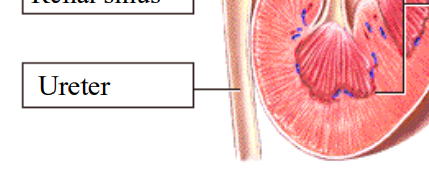
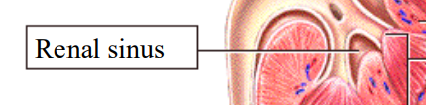
Renal Sinus
the spaces between the tubes, triangles, and columns
protective, structural, and vascular channel
houses the renal pelvis, calyces, renal artery/veins, nerves, and lymphatic vessels
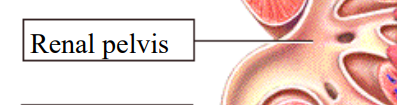
Renal Pelvis
where all the tubes meet up before moving to the ureter
Funnel shaped reservoir, collects urine from major calyces and directs it to the ureter for transport to the bladder
Major calyces
major channel in the kidneys
collects urine from the minor calyces
directs urine into the renal pelvis
Nephrons
The filtering component of urine
Found in
Renal cortex (Cortical nephrons)
80-85% of nephrons
Renal cortex and inner renal medulla (Juxtaglomerular Nephrons)
15-20% of nephrons
Yellow things that have the glomerulus, bowman’s capsule, PCT, loop of Henle, DCT, collecting duct, etc
Urine flow through kidney
Nephrons → pyramids → pelvis → ureter → bladder
Renal Corpuscle
The initial blood-filtering component of the nephron, located in the renal cortex (1 million per kidney)
component’s include:
Bowman’s capsule
Glomerulus
Bowman’s space
Epithelial layers of nephron
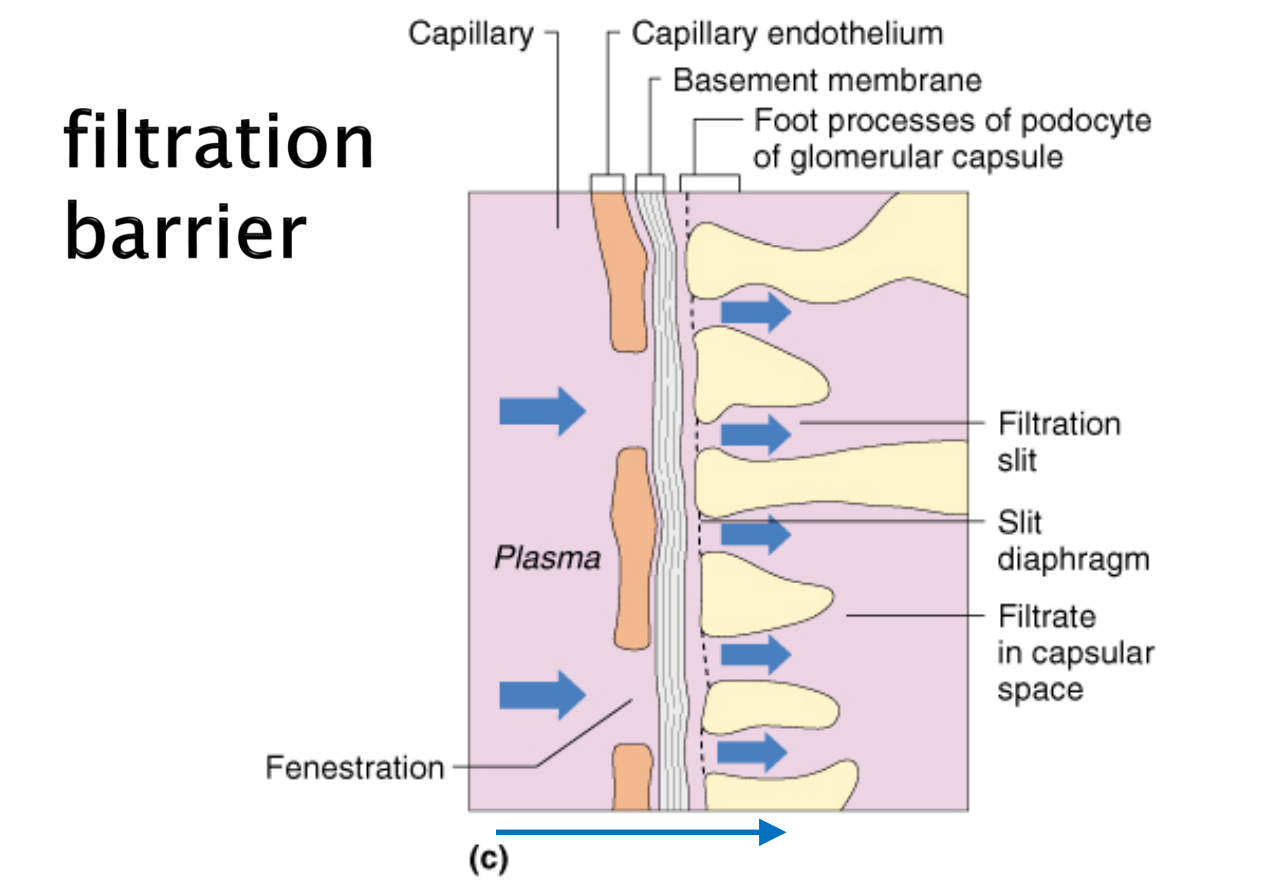
Filtration membrane
Components of the filtration barrier
Capillary
Basement membrane
Podocytes cells processes
Filtration
from glomerulus into bowman’s space
Reabsorption
Back to the blood
ex. glucose needs to go back to the blood
Secretion
From blood to tubule (nephron)
waste products to be excreted into urine
Macula Densa
Located in the DCT
Monitors NaCl concentration of filtrate and BP through osmoreceptors
when NaCl or BP drops, MD cells signals Juxtaglomerular cells to release RENIN
too much NaCl? vasoconstriction to slow down
MD can also tell JG cells to change its renin release (slow it down, b/c renin incr. NaCl and BP
MD CELLS ALSO MONITOR O2
secrete erythropoietin in response to low O2
allows for proliferation and helps mature RBCs to incr oxygen delivery
Renin
an enzyme that primarily acts a hormone (in the RAAS system specifically)
Renin triggers the Renin-angiotensin-aldosterone system (RAAS), which increases BP and adjusts diameter of the arterioles to maintain a stable glomerular filtration rate (GFR)
Secreted by JG cells
RAAS (system)
Renin triggers the formation of angiotensin II and aldosterone, which increase NaCl and water reabsorption in the proximal tubules and collecting ducts to raise blood pressure.
Renin also increases BP by changing diameter of ducts
Glycoprotein cover
Traps water in the ascending limb of the loop of Henle and the early DCT
ADH
Antidiuretic Hormone
Made by the SON (supraoptic nucluei in the posterior pituitary gland)
Leaves through the posterior lobe (one of two main lobes of the pituitary gland)
Allows Kidneys to Reabsorb water (back to blood)
Directly opens aquaporins (water channels) in the kidneys to reabsorb pure water (Doesn’t rely on salt to move the water)
helps to prevent dehydration
carried to the tubules of the nephron by the PT capillaries
Aldosterone
tells kidneys to reabsorb sodium (salt) back to the blood, with water following behind (osmosis)
ALSO secretes K+ (back to nephron)
Sodium leaves the urine and goes back to the blood at the expense of K+, which is secreted into to the urine
ALDOSTERONE IS STIMULATED BY LOW BP, LOW NA+, AND HIGH K+ (IN THE BLOOD)
High Na = High Osmolality
idk why this one’s blank
why’d you flip it over, it’s blank
Excretion
= Filtrate - reabsorption + secretion
= (Whatever was filtered - what was absorbed + what was secreted)
Glomerular filtration
Movement of large qty of water and solutes from the glomeruli into bowman’s space
ex. ions (Na+, K+, Cl-), nitrogenous waste (urea, uric acid, creatinine), and organic molecules (glucose, AAs)
Glomerular filtration is a passive process, that is dependent on Hydrostatic blood pressure (the force exerted by blood against the vessel walls, generate by heart’s pumping actions)
Qty in L of the amount of liquid that passes from plasma into the filtrate
180 L
protein too large to pass through to filtrate, too much protein in urine can be sign of greater issue
Glomerular capilaries
First layer of the filtration barrier
has fenestrations
endothelial cells that carry negative charges
Basement Membrane
Second layer of the filtration barrier
Meshwork of collagen and proteoglycan that has large spaces
strong negative electrical charge
The primary barrier to filtration
Podocytes
Third layer of the filtration membrane
has negative charges
hinders the passages of proteins (large molecules that are negatively charged in the kidneys, which helps repel from negative charge of the filtration barrier layers)
Things that are not filtered…
…Are not excreted through urination because they cannot pass through to the tubules of the nephrons
Things that cannot be filtered include:
large charged molecules (ex. proteins)
Filtered (no secretion or absorption)
On track to becoming urine
ex. Inulin (an indigestible prebiotic fiber derived from plants like chicory root, used to boost digestion)
inulin is useful in measuring GFR
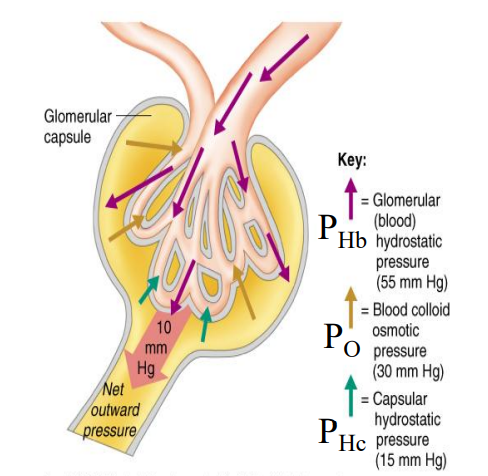
PHB
Glomerular (blood) hydrostatic pressure
blood moving into the glomerulus
55 mmHg
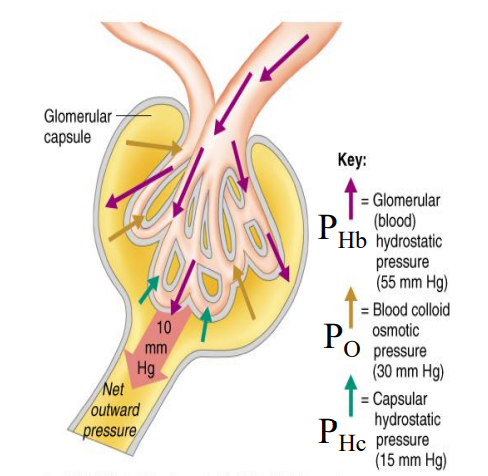
PO
Blood Colloid Osmotic Pressure
Pressure pushing against the glomerulus from Bowman’s space
30 mmHg
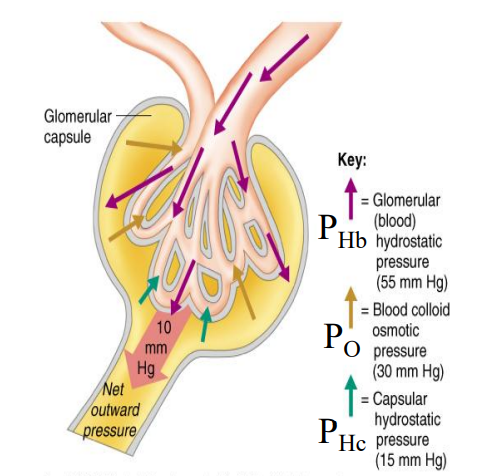
PHC
Capsular Hydrostatic Pressure
Pressure pushing against the glomerulus near the tubule, which pushes with PO
15 mmHg
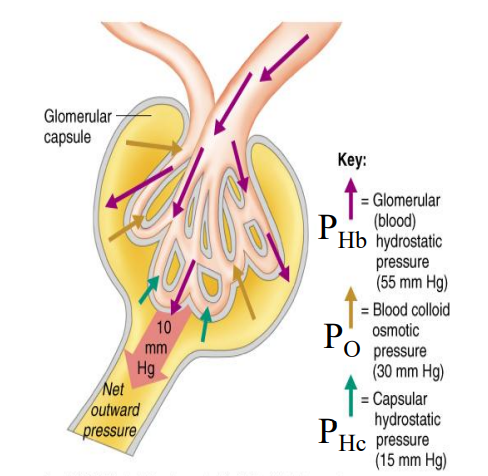
Net pressure out of the glomerulus into the tubules (Net Filtration Pressure)
NFP = PHb - (PO + PHc)
55 - 30 - 15 = Net 10 mmHg
PCT Reabsorption
Proximal Convoluted Tubule
Na/K pump on the basal membrane sets up gradient
low na inside the cell
lots of things here use na cotransport (ex. glucose, AAs, proteins)
water follows the solutes across the membranes in between the cells (osmosis; passive)
Filtered, Partial reabsorption (in PCT)
Most electrolytes are partially reabsorbed
Na+, Cl-, HCO3-
Filtered, complete reabsorption (in PCT)
Most nutritional substances
ex. AAs, glucose)
Hyperglycemia
glucose >200 mg/dL (prolly don’t need to know this part)
BUT, carrier protein for glucose protein becomes saturated, leading to excretion of glucose
diuretic effect (polyuria, b/c incr. vol. of water; more water follows glucose)
polyuria —(leads to)—> polydipsia (dehydration) —> polyphagia (hungry)
Glucose movement (PCT)
Apical (luminal membrane); cotransport with Na+
Basal (BV side); Facilitated diffusion (down concentration gradient)
Na+ movement (PCT)
REABSORBED!
Apical; Cotransport with other molecules
Basal; Na/K ATPase, creates concentration gradient
uses ATP (then becomes ADP)
K+ movement (PCT)
REABSORBED!!
Apical: Cotransport w/ Na+
Basal: Facilitated diffusion (high to low conc.)
Cl- movement (PCT)
REABSORBED!!
Apical: Cotransport w/ Cl-
Basal: cotransport w/ Na+
AA movement (PCT)
Amino acids
VERY IMPORTANT!! NEEDS TO BE REABSORBED!!
Apical: Cotransport w/ Na+
Basal: Facilitated diffusion
Water (PCT)
Water follows the osmotic gradient created by reabsorption of solutes (primarily sodium)
~65% reabsorbed
What supplies blood to cortical nephrons?
Peritubular capillaries
What supplies blood to Juxtamedullary nephrons?
both the PT capillaries and vasa recta
vasa recta supplies the loop of Henle that reaches deeper into the inner medulla
highly porous
acts to cycle salt
sluggish blood flow here (receives 10% of renal blood flow, 90% of blood flow is in the cortex)
Flow of blood in the vasa recta near loop of Henle
Ascending limb of vasa recta runs parallel to the descending limb of the loop of Henle
interstitial fluid runs in between
vice versa
water moves out of the descending limb of the loop of Henle, through the interstitial fluid and into the ascending vasa recta by osmosis
water does not move in the interstitial fluid between the ascending limb (loop of Henle) and descending vasa recta due to the glycoprotein cover on the ascending limb
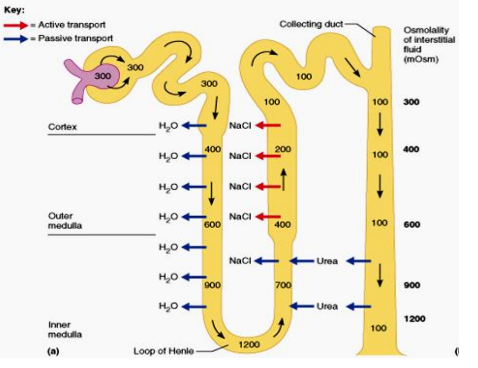
Flow of filtrate in the loop of Henle
Filtrate moves down in descending limb of the loop of Henle, and up in the ascending
Descending limb of the loop of Henle
Filtrate moves down
permeable to water (water can leave to Interstitial fluid, then vasa recta)
passive?
Ascending limb of the loop of Henle
Thin then thick segment of the loop of Henle
Glycoprotein cover; traps water inside the tubule, but solutes can diffuse through to the vasa recta
What can leave the ascending limb of the loop of Henle?
Na, K, Cl, H2O
NKCC pump; on apical membrane
uses sodium’s energy to move into the cell
one sodium, needs one K and 2 cl- in order to work
Na/K-ATPase on basal membrane creates gradient
na/k pump costs energy (ATP—>ADP)
Cl and K leaves the cells through facilitated diffusion (down their gradients)
Water cannot leave the tubule cells due to glycoprotein cover
Hydrogen Secretion
Secreted into PCT (see Renal 3 slide 26) by antiport mechanism (Na reabsorbed while H+ secreted; apical membrane)
comes into the cell from blood then leaves into tubule
Same in DCT
secreted in both PCT and DCT
Potassium Secretion
secreted in DCT
comes into tubule cell through antiporter with Na
leaves through tubule cell through antiporter with Na
see renal 3 slide 27
Movement of CO2 in PCT
comes from blood into the cell, cell has carbonic anhydrase inside, catalyzes reaction between CO2 and water, dissociates into H+ and HCO3- (bicarb)
When further away from the fast moving blood vessels of the fast moving blood vessels in the cortex ______________.
the slower things get back to the blood
salts don’t build up in cortex because of the fast moving blood vessels, so salt content here is similar to blood
Concentration gradient of the medulla
salts build up in the bottom of the medulla
salts don’t build up in cortex because of the fast moving blood vessels, so salt content there is similar to blood
Which part of the tubule system of the nephron has the highest salt content?
The space where the descending and ascending limb of the loop of Henle meet (1200 mOsm)
What amount of water is reabsorbed in the PCT?
65%
What leaves the descending limb of the loop of Henle? And where does it go? What is it impermeable to?
Water! (Passive transport)
Into the interstitial space then into the ascending vasa recta
Impermeable to salt!!
Is the filtrate in the descending limb of the loop of Henle Hypertonic or Hypotonic?
Hypertonic
Filtrate in the descending limb becomes salty (concentrated?)
BC WATER IS LEAVING
What leaves in the Ascending limb of the loop of Henle? Where does it go? What cant pass through?
NaCl leaves the thin segment (beginning) of the ascending limb of the loop of Henle through Passive transport
NaCl leaves the thick portion of the ascending limb leaves through active transport.
The salts leave into the interstitial fluid, unlikely to be picked up by vasa recta due to high salt concentration already
(Water is trapped due to the glycoprotein cover!)
Is the filtrate in the Ascending limb of the loop of Henle Hypertonic or Hypotonic?
Hypotonic
filtrate in the tubule becomes very dilute
BC SOLUTES ARE BEING REABSORBED!!
Blood moves ____ in the Cortex (HINT: speed)
Fast
When drinking water is not available, the kidney can produce a _____ volume of super concentrated urine. (HINT: quantity)
small
What happens when you drink a large amount of water?
Diluted urine
blood osmolarity drops
ADH levels decreased lower than normal, decreases amount of aquaporins
NaCl can leave the collecting duct to prevent large loss of electrolytes
Can cause temporary increase in BP
RAAS mechanism
Renin-Angiotensin-Aldosterone Mechanism
Kidneys detect decreased BP, results in incr. renin secretion (from JG cells)
Renin converts Angiotensinogen (protein from liver) to angiotensin I
Angiotensin-converting enzyme in the lungs convert angiotensin I to angiotensin II
Angiotensin II is a potent vasoconstrictor, results in incr. BP
Angiotensin II stimulates the adrenal cortex to secrete aldosterone
ANH
Atrial Natriuretic Hormone
produced by heart when BP incr.
inhibits release of ADH (incrs water reabsorption), Aldosterone (promotes retention of sodium and water, incr K secretion) and Renin (stimulates RAAS system, which incrs. water and salt retention)
Promotes Na and water excretion by the kidney (reduces kidneys’ ability to concentrate urine)
Results in decreased BV (blood vol) —> decreased BP
basically does the opposite of ADH, aldosterone, and renin (‘s downstream effects)
The concentration of the renal interstitial fluid is:
A. constant throughout the kidney
B. the greatest in the cortex
C. The greatest in the outer medulla
D. The greatest in the inner medulla
D. The greatest in the inner medulla
Renal blood flow is ___:
A. Constant throughout the kidney
B. the greatest in the cortex
C. The greatest in the outer medulla
D. The greatest in in inner medulla
B.
(inner medulla has sluggish blood flow)
Blood flow around the nephron (cortical nephron in this example, should be similarish to Juxtamedullary nephrons)
Blood comes inside through the arcuate artery → afferent arteriole → glomerulus → efferent arteriole —(then PT capillaries)→ down parallel to the ascending limb of the loop of Henle —(becomes blue here)→ then upwards parallel to the descending limb of the loop of Henle → arcuate vein
GFR equation
GFR = [PHb - (Po+PHc)] x Fc
PURPOSE: GFR must remain constant over a range of dif. BPs
GFR = Glomerular filtration rate
the total volume of fluid filtered from the glomerular capillaries into Bowman’s capsule per unit of time
PHb = Hydrostatic Pressure of Blood
PO = Osmotic Pressure
PHc = Hydrostatic pressure of capsule
Fc = Filtration coefficient
PHb
Hydrostatic Pressure of Blood
the push force from the blood pressure within the glomerular capillaries that drives fluid into the kidney’s filters
PO
Osmotic Pressure
The pull force exerted by proteins (like albumin) in the blood that tries to keep fluid inside the capillaries
PHc
Hydrostatic pressure of capsule
The back-pressure from fluid already inside Bowman’s capsule that opposes further filtration
Fc
Filtration Coefficient
A constant that represents the permeability and surface area of the filtration membrane
capillary permeability multiplied by surface area
_______ sometimes block fenestrations in the filtration barrier, which can affect filtration.
Antibodies
If qty of nephrons decrease, total surface area ________. What does that affect?
decreases
affects Fc
How do small changes in GFR affect salt and water excretion?
large changes in salt and water secretion
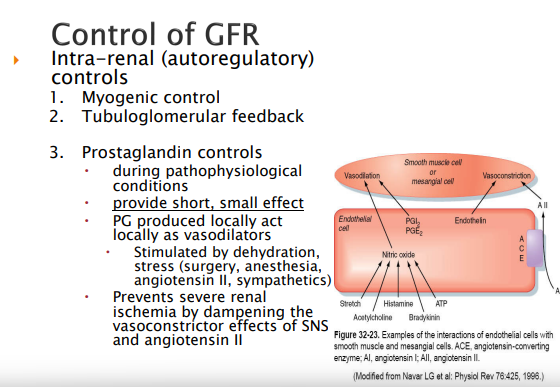
Intra-renal control of GFR
Myogenic control; vascular smooth muscle to respond to pressure changes
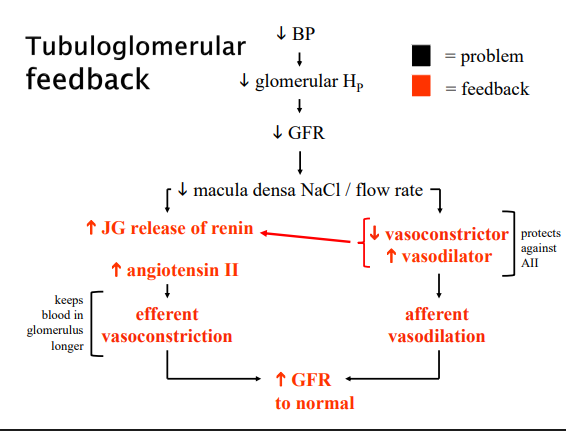
Tubuloglomerular controls; MD (Macula Densa Cells)
Prostaglandins; Can act locally to allow for vasodilation of the smooth muscle that makes up the blood cell. Provide short, small effect. Stimulated by body stress such as dehydration, stress(surgery, anesthesia, angiotensin II, sympathetic)
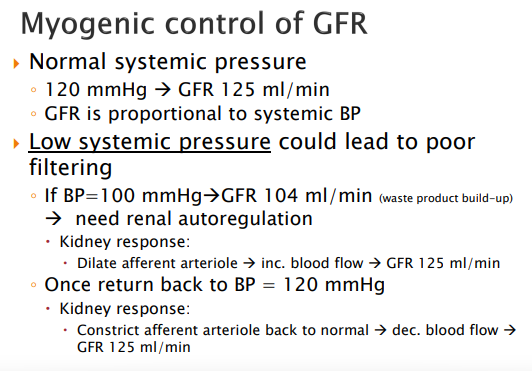
Myogenic Control of GFR
Tubuloglomerular feedback
High systemic pressure (response by Myogenic control of GFR)
146ml/min urine produced if BP is 140 mmHg
kidney responds by constricting afferent arterial (incr. resistance, flow in of blood), GFR returns to normal 125 mL/min
Once back to BP of 120 mmHg —> dilation of afferent arteriole
Normal Systemic pressure
120 mmHg (BP)
125 mL/min (GFR)
Low systemic pressure (response by myogenic control of GFR)
if bp = 100 mmHg (very low), GFR = 104 ml/min (waste product build up)
kidney responds by dilating the afferent arteriole to increase blood flow —> GFR to 125 ml/min,
once BP back at 120 mmHg, kidney responds by constricting afferent arteriole (decr. blood flow)
What produces renin? (HINT: Cell Type)
JG cells (juxtaglomerular cells) (endocrine cell)
Adenosine tells JG cells to ______ Renin production
Decrease
should lead to decreased retention of water b/c decr. RAAS stimulation
Less aldosterone = _____ sodium reabsorption
A. more
B. less
B. less
What happens when LOW NA+ is detected by the MD cells
Macula Densa cells
less adenosine released (by MD cells)(decreased vasoconstriction, so vasodilation) → allows for more filtration, more things flow into bowman’s capsule
less adenosine also means JG cells incr. renin production
→ which then increases amount of sodium reabsorbed
less adenosine →
adenosine = ATP??
JG cells are found ______________ (no nathan it is not the kidneys)(i mean technically yes but that’s not what the question is asking)
within the wall of the afferent arteriole near the glomerulus and renal corpuscle, forming the JGA (Juxtaglomerular apparatus)
Diuretic
Increases urine volume
Natriuretic
increases renal sodium excretion
Aquaretic
increases excretion of solute-free water
promotes water excretion without electrolyte loss
If mannitol is found in the PCT, water ____
water remains with mannitol, leading to less water reabsorption in the PCT
summary: water is normally reabsorbed in the descending limb, but can be trapped in the presence of mannitol
Mannitol is not commonly used therapeutically
can be taken orally but not absorbed well in the GI tract
causes incr. diarrhea
better if given IV
How much water per day is reabsorbed from PCT through solute reabsorption?
FYI SLIDE
108 L/day
NHE3
Sodium Hydrogen ion antiporter (apical membrane)
Na from lumen to inside cell, H from inside cell to lumen
H ions come from the blood
(there is also a Na/K-ATPase on the basal membrane that sets up the gradient)
SGLT2
Sodium Glucose transporter found on the apical membrane
Carbonic Anhydrase (in the PCT)
Can be found on the apical membrane and inside the cell
CA inhibitor
Carbonic anhydrase inhibitor
traps sodium and bicarbonate in lumen
not k sparing
meaning this is a diuretic
ex. acetazolamide is a CA inhib.
Less HCO3 reabsorbed and less H+ secreted leaves the blood _______ (HINT: Think about blood pH)
Acidosis
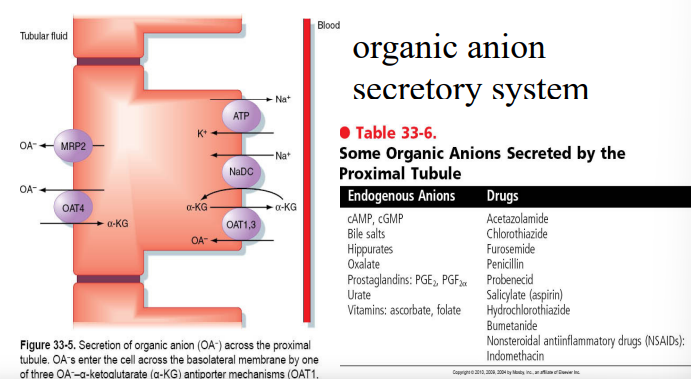
Endogenous Anions
Anything you want to dump from the blood to urine to be excreted
here’s the pic if u want idk