MSK UQ Unit 2 COMBO set
1/1020
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
1021 Terms
History components for a shoulder exam
-Age
-Condition (MOI, location, symptoms)
-Occupation/recreational activities
-Hand dominance
-Upper quarter screens
-Medical screen
-Imagine results
-Post op reports, precautions
why is looking at age important for shoulder exam?
different conditions are more common for certain ages
potential referred pain to the shoulder
-Radicular
-Thoracic outlet
-Cervical facets
-cancer
medical screening with shoulder
High risk of thoracic and abdominal referral
lung and breast cancer can cause shoulder pain
Red flag
Outcome measures for the shoulder
-SPADI
-DASH
-Patient specific functional scale (general)
-Simple shoulder test
-UCLA shoulder scale
-Penn shoulder scale
DASH Vs SPADI
Both are UE specific, dont use together
Posture observation for shoulder
look for protective postures, head/neck position, scapular position, thoracic curvatures, muscle symmetry/atrophy(rtc and inter/parascapular muscle)
1cm incision
arthroscopy
Ecchymosis
bruising/staining of the skin due to subcutaneous bleeding caused from muscle tear, joint separation.
edema and shoulder conditions
common from immobilization, from being splinted for protection of injured tissue. Can cause DVT in UE.
How to address edema in shoulder conditions
circulation promotion and edema management
Scapular slide test
Scapular position with regard to spinous process
Start in neutral→hands on hip→shoulder abduction
PROM for shoulder always in what position?
Always in supine
AROM measurements for the shoulder can be done in what position?
seated (against gravity)
what to look for when assessing the quality, quantity, and provocation of joint motion.
-End range symptoms
-Painful arc
-Ratio of IR/ER
-Compensatory movement patterns
painful arc
mid range issue
between 60-120º
GIRD
glenohumeral internal rotation deficit
GIRD may indicate
posterior capsular tightness or shortening
End range symptoms occur when?
when joint tissues are most tense
Painful arc looks for potential symptoms when?
Mid-range
why might we assess scapulo-humeral rhythm anteriorly?
to see gross changes, facial expressions
Why to assess scapulo-humeral rhythm posteriorly?
To view specific scapular movement patterns
what functional motions to assess with shoulder exam?
-Hand behind head (Abd, ER)
-Hand behind back (Ext, Add, IR)
hand behind head - combined abd/ER
note where finger tips touch
Goal is to reach opposite spine of scapula or thoracic SPs
hand behind back - combined ext, add, IR
note where thumb touches
Thumb should reach T8
Subacromial pain tests
-Neers
-Hawkins-Kennedy
Neers test
Shoulder flexion with arm in IR, given OP
Hawkin's-Kennedy
combo of 90 degrees of flexion and IR, grinding greater tuberosity against the acromion
Drop Arm Test
Arm up in 90, actively bring up and try to control the descent. Indicative of Rotator cuff pathology.
muscle performance test for shoulder.
grade strength, and note the symptom response, compare to uninvolved side. Possibly repeated motions for endurance
what to observe when assessing muscle performance for the shoulder
observe quality, motor control. Timing, activation, sequencing, coordination of muscles working together.
supraspinatus strength test
Empty can (thumb down), full can (thumb up). If one hurts or weak, generally both will be.

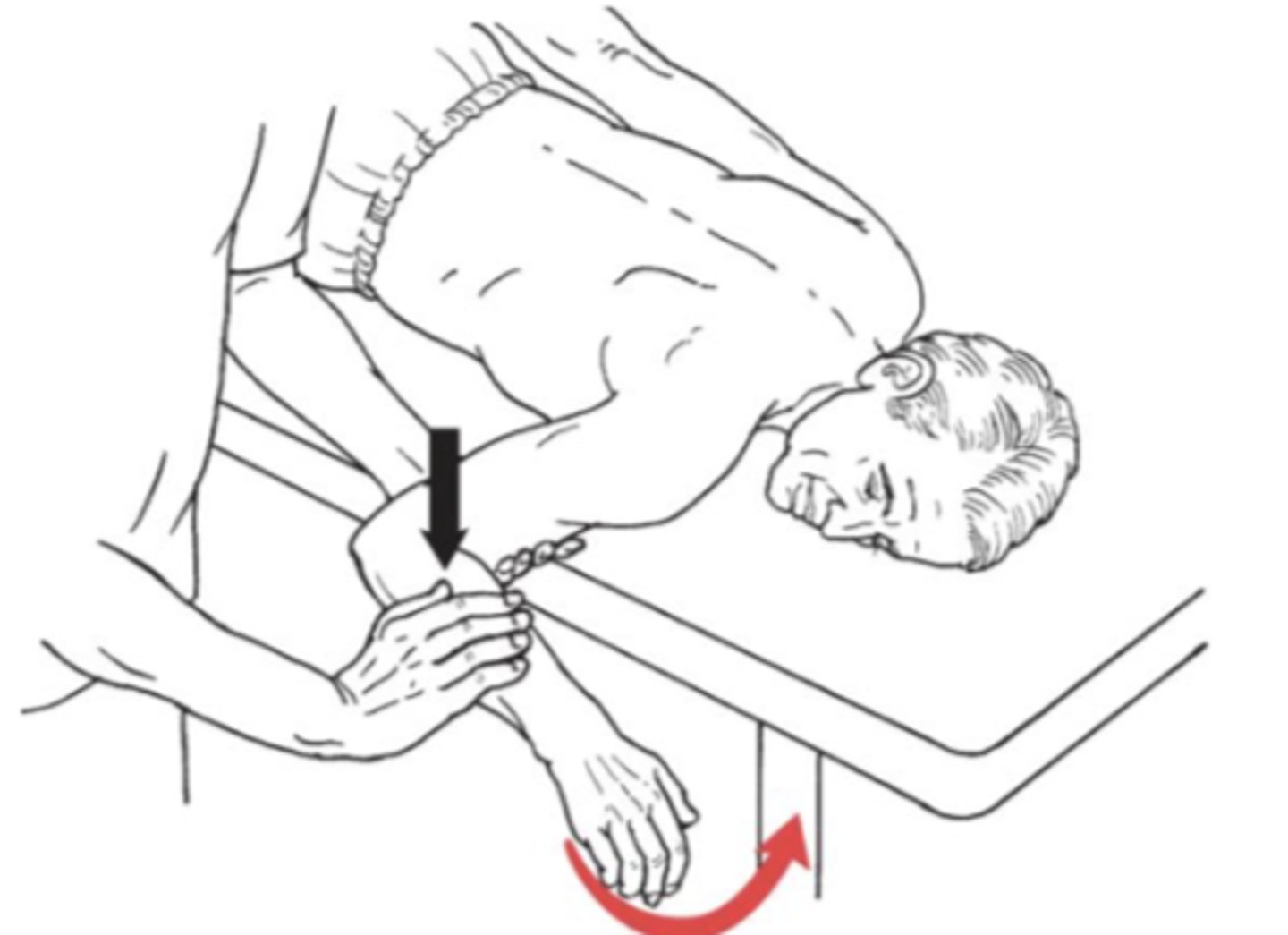
teres minor mmt
An external rotator
Patient position: supine
Test: examiner applies counter pressure to inner aspect of the distal humerus, lateral rotation of the humerus with elbow held at a right angle
Pressure: in the direction of medial rotation (or IR)
**patient's arm is hardly off table, closer to their bodies
infraspinatus strength test
Arms at sides; elbows flexed to 90° with thumbs up, provide resistance as pt presses forearms outward
Positive for bicipital tendinitis and possible rotator cuff tear if weakness present

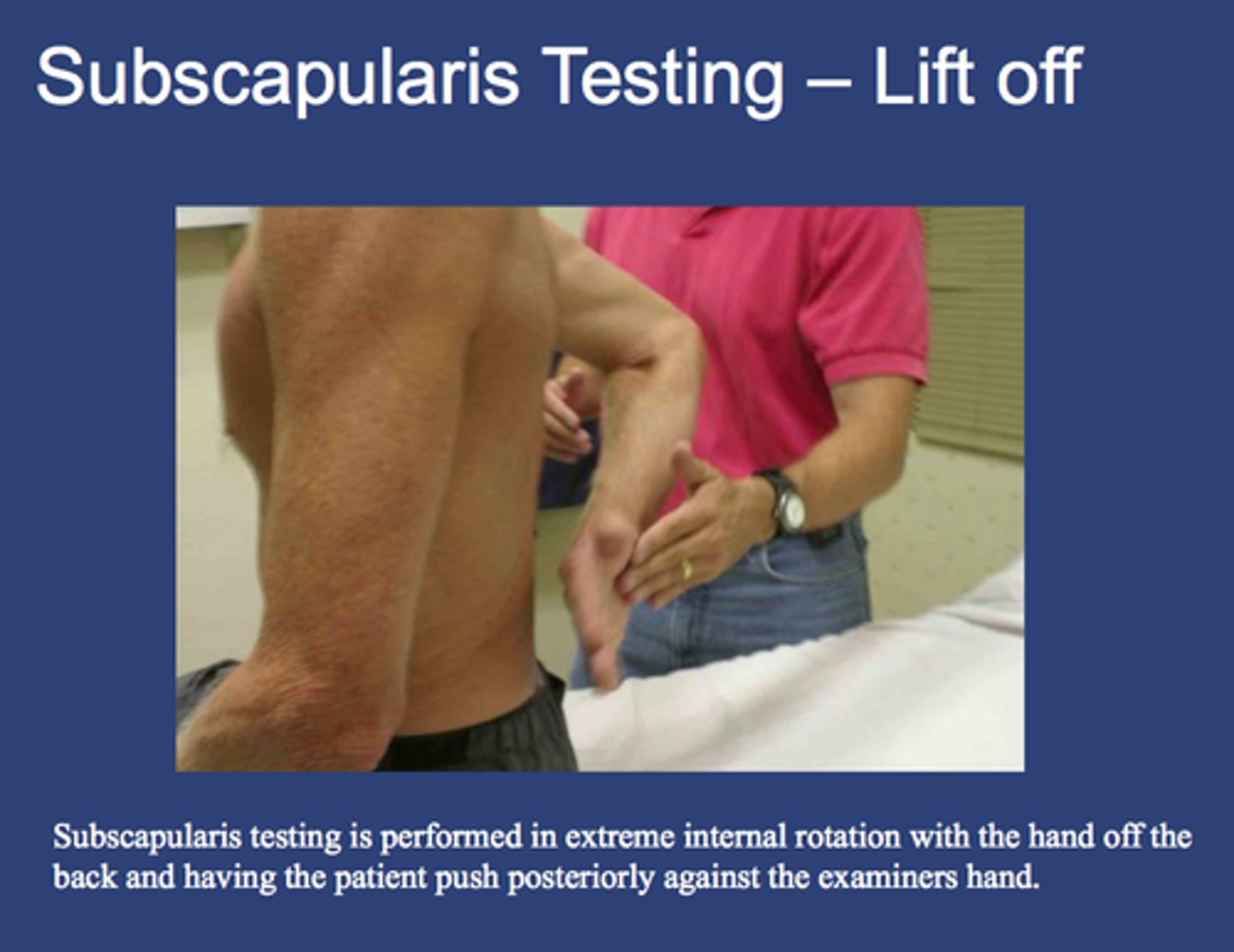
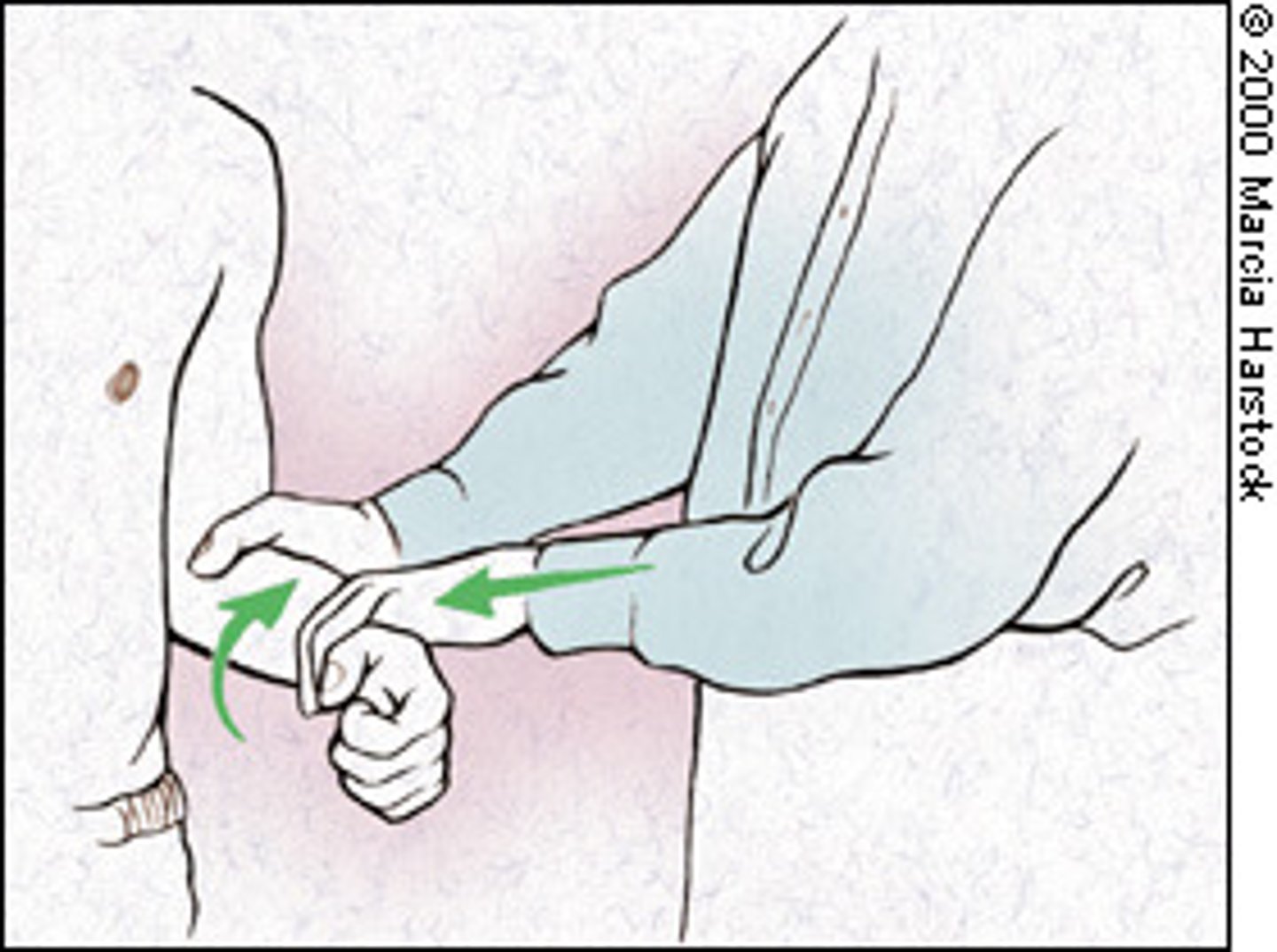
subscapularis test
"lift off" test.
ACJ provocation tests
-Cross body adduction
-Resisted horizontal extension/abduction
Cross body adduction
Horizontal adduction with OP
Resisted horz ext/abd
Horizontal abd and ext w/ resistance looking for provocation
Biceps tendon and ACJ/labrum tests
-Speed's test
-Active compression (Obrien's)
Speed's test
assesses long head bicep, bicipital tendonitis test.
Obrien's test
ACJ pathology and/or labral.
Positive O'Brien's Test
Positive test = hurts when thumb down, not when thumb up.
Bicep test
yergason's test
Yergason's test
Assess the stability of biceps tendon in bicipital groove
- pt flexes elbow to 90 while physician grasps elbow w/ one hand and wrist other pull and physician resists supination of forearm + external rotation of shoulder
(+) Test = pain as biceps tendon pops out of bicipital groove
Where to palpate during shoulder exam
entire shoulder complex, cervicothoracic spine, arm.
what to look for with shoulder palpations
-Soft tissue temp, symmetry, muscle mobility
-scan for provocation
locations of likely tenderness with shoulder pathology
-Sub-acromial space
-supraspinatus tendon
-greater tuberosity
-Bicipital groove
-ACJ line
-Upper trap
-Levator scap
What joints to include in joint mob of the shoulder?
GH, SC, AC, ST, cervical and thoracic spine and ribs
what to assess with joint mobs
quantity, quality, symptom response, end-feel. compare with uninvolved side.
Apprehension test
arm in 90/90, slowly watching for patient response. Will make patient apprehensive as if their shoulder is going to pop out anteriorly.
Relocation test
Applying posterior glide-->ER+ABD. Patient won't feel apprehensive, adds an anterior restraint the patient is lacking
Apprehension / Relocation tests for
anterior instability
Apprehension / Relocation test internal or posterior pain
posterior pain in ER, relief of pain w/ posterior glide
Bicep load test II
shoulder abducted 120 degrees, flexed/supinated elbow, bicep isometric muscle test.
Positive bicep load test II
if patient has labral pathology involving the bicep tendon, this will provoke it by pulling on the tendon attached to the labrum.
Scapular tests are what kind of tests?
alleviating tests to see if there is a scapular control problem causing/contributing to glenohumeral pain.
Scapular assistance test
assisting scapular motion, seeing if ROM improves
Scapular repositioning test
stabilizing the scapula in a retracted and posteriorly tilted position so the GHJ can clear and abduct.
wall pushup assesses what?
Serratus anterior strength/weakness and control. Scapular winging presents with weakness.
differential diagnosis process for the shoulder
1. Pre test probability (patient reported symptoms)
2. Clinical impression (based on experience)
3. Create hypothesis
4. Post-test probability (increased with special tests)
choose what kind of special tests for the shoulder?
Those with appropriate clinical utility and psychometric properties.
general subjective history info during shoulder exam
-Acute, or gradual?
-Instability?
-Catching, locking, mechanical symptoms.
-Neuro symptoms
-location of symptoms
-complaints of stiffness/loss of motion
Red/yellow flags for during shoulder exam
-Pain during sleep
-Insidious onset
-Systemic signs
-Cardiovascular sign
-malignancies
-Kehr's sign
Kehr's sign
spleen referral to the left shoulder
ages 13-20 generally present with what shoulder condition?
Instability
ages 20-40 generally present with what shoulder condition?
Instability, biceps/labral complex, frozen shoulder
ages 40-60 generally present with what shoulder condition?
Rotator cuff, arthritis, frozen shoulder
ages 60+ generally present with what shoulder condition?
rotator cuff, arthritis, fracture
Frozen shoulder most common in
middle-aged women d/t hormonal changes around menopause and those with diabetes and thyroid dz
GHJ ROM Combing hair
ABD 105º-120º
ER 90º
ADD 30°-70°
Perineal Care Sh ROM
ABD 30º-45º
IR 90º+
ABD 75°-90°
Washing contralateral ueROM
FLEX 60º-90º
IR 90°
ADD 60°-120°
Overhead shelf flexion ROM
FLEX 70º-80º
ER 45º
ADD 70°-80°
Internal rotation loss (GIRD)
Glenohumeral internal rotation deficit
GIRD contributing factors
-Bony adaptation
-Scapular posture
-Posterior musculotendinous tightness
-Shoulder fatigue
-Posterior capsule tightness
what bony adaptations contribute to GIRD?
A lot of ER (with throwing) can cause some retroversion at the head of the humerus, causing a lack of IR.
How do the ER's contribute during throwing?
-Concentrically during cocking phase
-Eccentrically decelerate during throwing
static posture observation for the shoulder
-Shoulder height asymmetry
-Hands on hips position
-Muscle development/atrophy
-Scapular posture
what to observe with scapular posture
-asymmetries
-resting and elevation
-dyskinesis (aberrant motion)
Kibler's Type 1
Prominent inferior angle: RTC Tendinopathy
Kibler's Type 2
prominent medial border from GH instability
Kibler's Type 3
Superior migration of medial border from RTC weakness
Thrower's SICK scapula
-Scapular malposition
-Inferior medial border prominence
-Coracoid pain and malposition
-dysKinesis
Labral dyskinesis
Inferior/medial border
RTC Dykinesis
superomedial border
Scapular malposition
-scapular tilting/protraction
-lateral displacement
-scapular abduction
Spinal accessory nerve palsy identified by what?
upper trap atrophy, scapular depression. No medial winging with flexion, or abduction. Flip sign
flip sign
Scapula flips off ribscage
Long thoracic nerve palsy identified by what?
Medial scapular winging with active flexion
common faults with scapular dyskinesia
-Increased anterior tilt
-Increased IR of the scapula
-Decreased upward rotation
With limited upward rotation of the scap, stretch what?
Upper trap, pec minor, levator, rhomboids
With limited upward rotation of the scap, strengthen what?
Serratus anterior, Low trap
With limited posterior tilt of the scap, stretch what?
Pec minor
With limited posterior tilt of the scap, strengthen what?
serratus, low trap
with increased internal rotation of the scap, stretch what?
Pec minor, major
with increased internal rotation of the scap, strengthen what?
Mid and low trap, rhomboids, serratus
A "thrower's" scap often appears how?
protracted, depressed, anteriorly tilted.
with scapular testing, what factors to assess?
-scapular stabilization
-muscular control
-scapulothoracic mobility
scapular assistance test
assist the scap into upward rotation, and look for a decrease in pain
scapular reposition test
assist ER and posterior tilt, and assess strength