IBD
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
34 Terms
Inflammatory Bowel Disease (IBD)
= Ulcerative Colitis (UC) and Crohn’s Disease (CD)
•Chronic relapsing inflammatory conditions of the gastrointestinal tract
•No cure but periods of remission and relapse over many years
•Remission: absence of active disease
•Relapse: presence of active disease
Unpredictable for patients
•Lifetime costs of IBD comparable to coronary heart disease or cancer
•About 300,000-500,000 people in UK with IBD. Currently more common in Caucasian heritage but also increasing within south Asian population
Typical presentation
UC
•Bloody diarrhoea
•Mucus
•Urgency and frequency
•Cramping abdominal pain (associated with need to defaecate)
Crohn’s disease
•Diarrhoea (sometimes with mucus, pus or blood)
•Abdominal pain
•Fatigue
•Weight loss
Investigations after a positive calprotectin test
•Need to establish whether Ulcerative Colitis vs. Crohn’s Disease
•Normally undergo a colonoscopy.
•Site and extent of inflammation
•Severity of disease
A fecal calprotectin test measures the level of a protein (calprotectin) released by white blood cells into the stool when the intestines are inflamed → not a great marker as people don’t normally like giving stool samples. Only up to 40% compliance with stool samples. This can be raised in other healthcare conditions so not very precise. Also can be a difference in level by the time its actually being tested in the lab.
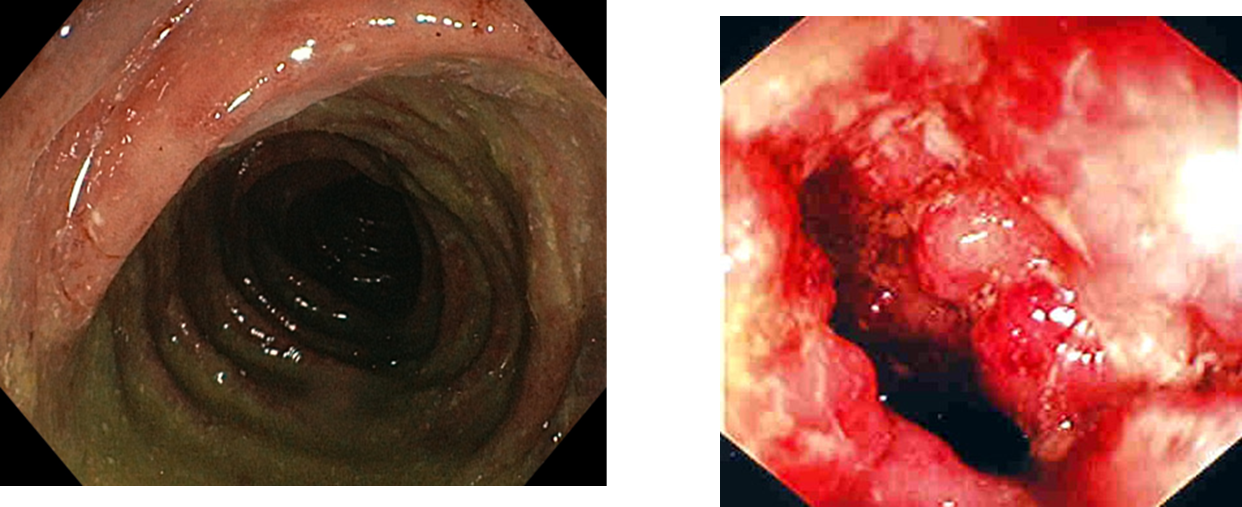
On the left is UC – slight ulceration and inflammation
Right is Crohn's – lots of inflammation and quite narrow due to build up of scar tissue.
Anatomy
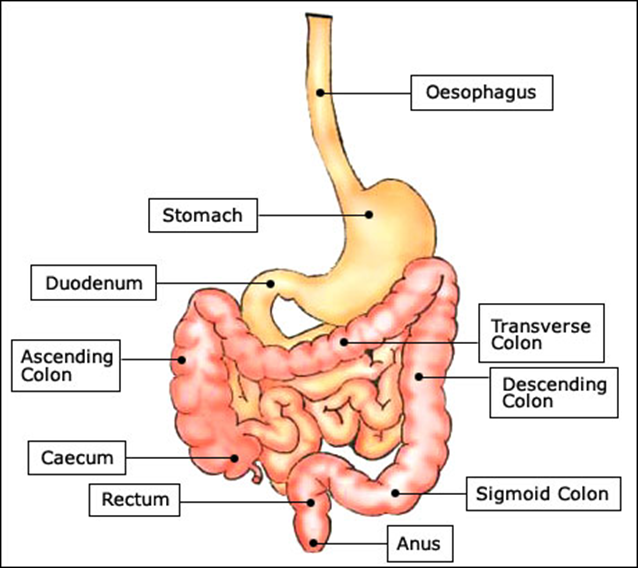
•Ulcerative colitis
•Limited to large bowel (colon) and rectum
•Proctitis (~40%) - rectum only
•Left-sided colitis - descending colon to transverse colon
•Extensive colitis
•Pan- (or total) colitis - entire colon
•Crohn’s disease
•Can affect any part of the GI tract from mouth to anus.
(~45% ileocaecal affected)
•“Skip” lesions – may see one area affected another area that’s fine and then another area that is affected again.
Extra-intestinal symptoms – Symptoms outside the GIT
About 20-30% of patients will present with additional symptoms
More common in colonic disease
•Joint disease
•e.g. ankylosing spondylitis (~5%), arthritis (~10%)
•Skin
•e.g. erythema nodosum (~8%) , pyoderma gangrenosum (~2%)
•Eyes (~10%)
•e.g. iritis, uvetitis
•Hepatobiliary system
•e.g. sclerosing cholangitis (~5%)
•Increased risk of thrombo-embolism
•Increased risk of osteoporosis
•Most common:
•Anaemia
Assessing severity: Ulcerative Colitis
Truelove and Witts Criteria (BMJ 1955)
Mild | Moderate | Severe | |
Bowel movements (no. per day) | Fewer than 4 | 4–6 | 6 or more plus at least one of the features of systemic upset (marked with * below) |
Blood in stools | No more than small amounts of blood | Between mild and severe | Visible blood |
Pyrexia (temperature greater than 37.8°C)* | No | No | Yes |
Pulse rate greater than 90 bpm* | No | No | Yes |
Anaemia* | No | No | Yes |
Erythrocyte sedimentation rate (mm/hour)* | 30 or below | 30 or below | Above 30 |
National Guidelines
•Key NICE Clinical Guidelines
•Crohn’s disease management (NG129) 2019
•Ulcerative Colitis management (NG130) 2019
•
•Plus separate guidance for use of:
•Darvadstrocel
•Tofacitinib
•Ustekinumab
•Vedolizumab
•Infliximab
•Adalimumab
•Filgotinib
•Golimumab
•Ozanimod
•Upadacitinib
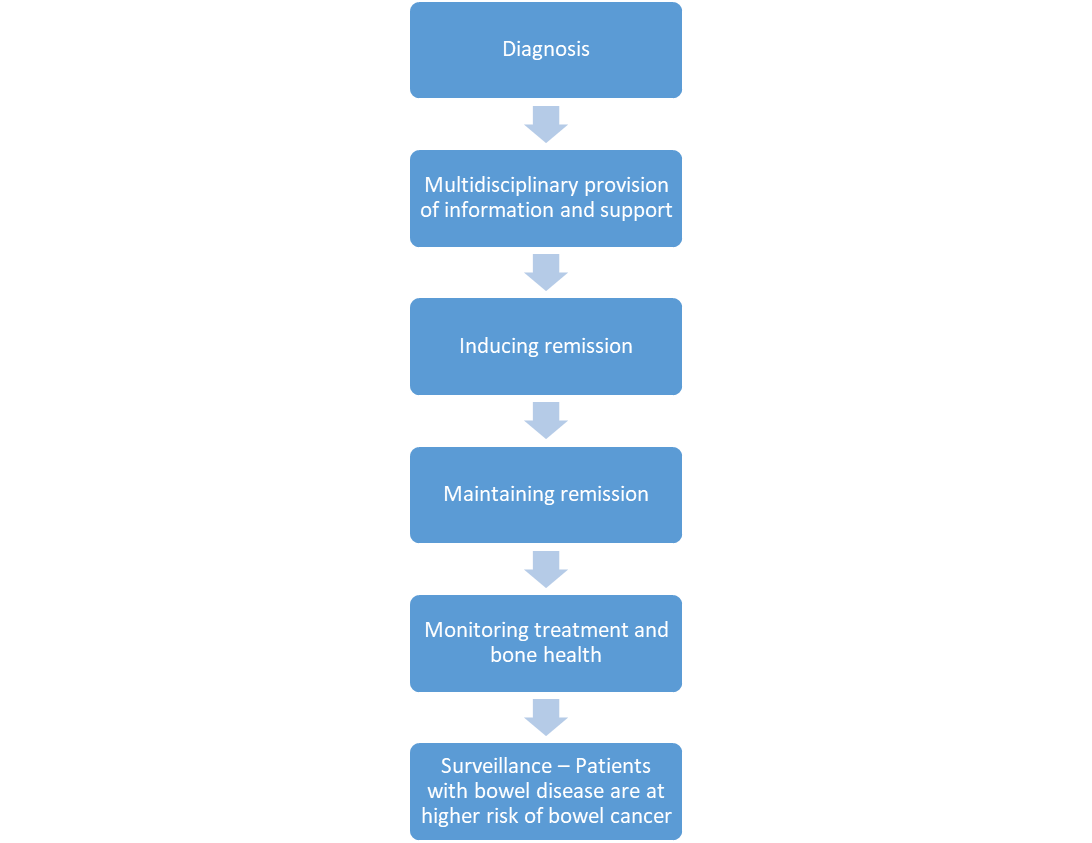
IBD treatment pathway
Overall aims of drug treatment of IBD
•Induce remission
•Maintain remission
•Control symptoms
•Limit drug toxicity
•Modify disease progression
•Limit/avoid complications
Initial assessment
•Pain
•Fluid and electrolytes for dehydration
•Diarrhoea
•Blood loss (Hb)
•Nutritional status
•VTE risk assessment
Main Treatment Options: Inducing remission
UC | Crohn’s | |
Aminosalicylates | y | (y) |
Corticosteroids | y | y |
Ciclosporin | y | x |
Infliximab, adalimumab, golimumab | y | y |
Vedolizumab | y | y |
Ustekinumab | y | y |
Tofacitinib | y | x |
Lots of different treatment options – choice is influenced by which condition they have.
Aminosalicylates
Key clinical management points:
•Preparations are not interchangeable
•Essential counselling on rare, but significant side effects
•Formulation choice is important and is influenced by the site of disease – preparations aren’t interchangeable
•5-ASA (mesalazine) is the active component.
•5-ASA is unstable in acidic conditions \ oral preparations are formulated to withstand the acidic conditions of the stomach.
•Active 5-ASA is released in the colon or ileum to exert its anti inflammatory effect topically
Oral aminosalicylate formulations- examples
Drug Name | Area of Intestine treated |
Sulphasalazine (Salazopyrin®) 5-ASA-Sulphapyridine | Colon (AZO bond cleaved by colonic bacteria) |
Mesalazine (Asacol MR®) 5-ASA (pH dependant coat) | Terminal ileum and colon (Released at pH 7) |
Mesalazine (Pentasa®) 5-ASA (slow release) | Entire small intestine and colon |
Mesalazine XL (Mezavant®) 5-ASA (pH dependant slow release coat) | Terminal ileum and colon (Released at pH 7) |
Mesalazine (Salofalk®) 5-ASA (pH dependant coat) | Ileum and colon (Released at pH 6) |
Olsalazine (Dipentum®) 5-ASA-5-ASA | Colon (AZO bond cleaved by colonic bacteria) |
Balsalazide (Colazide®) 5-ASA-aminobenzoylalanine | Colon (AZO bond cleaved by colonic bacteria) |
Formulation choice is important as each releases the drug in different parts of the intestine
Key counselling points
•Common side effects include: diarrhoea, headache, leucopenia, nausea, rash
•Rare side effects: agranulocytosis, neutropenia, pancreatitis
•
•Report any unexplained bleeding, bruising, purpura, sore throat, fever or malaise that happens during treatment
•
•Renal function will need checking before starting treatment, at 3 months and then annually
•More severe side effects come with use of sulfasalazine and that can be avoided with use of 5 ASA only preparation.
Generally, the more severe side effects that come with sulphasalazine can be avoided by using 5ASA only preparations
Topical (rectal) aminosalicylates
•Often used in conjunction with oral treatment
•All of these reach a different part of the colon
•Suppositories
•Reach rectum
•Foam enemas
•Reach rectum and sigmoid colon
•Liquid enemas
•Reach rectum and rectosigmoid colon
Action: Ensure you know how you would counsel a patient on how to use each of these formulations
Corticosteroids
Key clinical management points:
•Not used to maintain remission due to severe side effects
•Need to be gradually reduced
•
•IV, oral and rectal formulations
•Aim to rapidly achieve remission but limit exposure
•IV should be used in severe disease
•Budesonide associated with less systemic absorption
•Using rectal steroids also minimises systemic absorption
Key counselling points
•If effective then steroids are gradually reduced, so need to ensure patient is confident with regimen
•
•Essential to ensure patients are aware of side effects of long term use of corticosteroids:
•adrenal suppression, Cushing’s, osteoporosis, thin skin, fluid retention, diabetes etc.
•
•Monitoring needed for early signs of adverse effects e.g. regular diabetes checks or bone health checks.
Ciclosporin
Key clinical management points:
•Only used (rarely) in Ulcerative Colitis (not Crohn’s)
•Different brands not interchangeable
•Extensive monitoring requirements
•Therapeutic drug monitoring
•Used in acute severe active UC unresponsive to IV steroids after 72hrs or if symptoms worsen on steroids (but unlicensed)
•Given by intravenous infusion initially
•Can take up to 14 days for response
•If no response ® colectomy
•If effective may be converted to oral therapy for 3-6 months (unlicensed)
•Side effects limit long term use so usually used as a ‘bridge’ to treatment with azathioprine or as a last stage before surgery
Ciclosporin
•Key side effects:
•Renal and hepatic impairment
•Hypertension
•Infections (consider PCP prophylaxis)
•Electrolyte disturbances (K, Mg)
•Monitoring:
•Maintain serum ciclosporin levels 100-200ng/ml
•BP, Mg, K, lipids, FBC, Ur and Cr, LFTs before and during therapy
•Blood pressure
Biologic or targeted cell therapy
•Anti-tumour necrosis factor α (anti-TNF-α) antagonists
•Infliximab
•Adalimumab
•Golimumab
•α4β7 integrin antagonist
•Vedolizumab
•IL-12, IL-23 antagonist
•Ustekinumab
•Tyrosine kinase (JAK1 and JAK3) antagonist
•Tofacitinib
•Sphingosine-1-phosphate (S1P) antagonist
•Ozanimod
•Need to consider:
•Mode of action
•Method of administration
•Speed of onset
•Comorbidities
•Extra-intestinal manifestations
•Supportive therapies
•Shared decision-making approach
Infliximab
Key clinical management points:
•Infection risks
•Hypersensitivity reactions
•Treatment only continued if evidence of response
•Therapeutic Drug Monitoring
•Used to induce remission in:
•Subacute UC
•Acute severe UC unresponsive to steroids and thiopurines
•Severe active UC when ciclosporin is contra-indicated/clinically inappropriate
Infliximab administration
•Two formulations:
•IV infusion
•Subcutaneous (used after 2 initial IV loading doses)
•Given concurrently with immuno-suppressants to reduce antibody formation vs. infliximab (more common in carriers of HLA-DQA1*05) plus synergistic effects
•Monitor infliximab trough levels (target: 3-7mg/ml) to determine whether dose can be increased
•Side effects:
•Headache, rash, dizziness, dry skin, predisposition to infections (TB), hepatoxicity, infusion related reactions (acute or delayed),
•Contraindicated:
•In heart failure and active infection
•Given for 12 months or until treatment failure
•Only continued if evidence of active disease
Adalimumab
Key clinical management points:
•Subcutaneous administration
•Infection risks
•Hypersensitivity reactions
•Levels measured if losing response- dose can be escalated if appropriate
NICE Guidelines:
•Choice of anti-TNF-α agent on individual basis
•Advantages/disadvantages
•Therapeutic need
•Adherence
•Cost
Anti-integrin therapy: Vedolizumab
Interleukin inhibitors: Ustekinumab
Janus kinase inhibitors: Tofacitinib
•Only used if anti-TNF-α agents cannot be tolerated, disease has responded inadequately or lost response to treatment
•Essential monitoring requirements for each therapy to promptly identify potentially significant side effects
•Patient access schemes negotiated between the manufacturers and the NHS to fund treatment
Main Treatment Options: Maintaining remission
UC | Crohn’s | |
Aminosalicylates | a | (a) |
Thiopurines (azathioprine, mercaptopurine) | a | a |
Metronidazole | r | (a) |
Methotrexate | r | a |
Anti TNF therapy (adalimumab, infliximab) | r | (a) |
[Note: Some patients choose not to take any maintenance treatment and it is important to realise that this is their choice to do so]
Thiopurines are the mainstay for maintaining remission.
Aminosalicylates
•To maintain remission after mild-moderate exacerbation of proctitis/proctosigmoiditis (inflammation of the bottom end of the intestine)
•Topical and/or oral
•To maintain remission after mild-moderate exacerbation of left-sided or extensive UC
•Oral only as topical preparation wouldn’t reach far up enough into the colon to reach remission.
•Once daily dosing often recommended even if it says to split as
•Can help adherence
•But may result in more side effects (diarrhoea)
Thiopurines: Azathioprine and 6-mercaptopurine
Key clinical management points:
•TPMT levels must be checked before commencing treatment, varies depending on genotype and affects how efficacious drug is
•Essential counselling on side effects
•Potential for drug interactions
•Steroid sparing properties
•Used in patients having 2 or more exacerbations/year requiring steroids
•Or: started after 1 episode of acute severe UC
•Response in 2-3 months
•\ not suitable alone for acute exacerbations
•Not all patients respond optimally- depends on TPMT activity and genotype
•à More on this in the case study workshop!
Thiopurines
•Side effects:
•Nausea & vomiting (6-mercaptopurine may be better tolerated)
•Increased risk of infections
•Flu like symptoms, leucopenia, hepatoxicity and pancreatitis
•Counselling:
•Report any signs of infection or bruising. Report urgently to nurse or to the GP.
•Monitoring:
•FBC and LFTs weekly for first 2 months then monthly
•Significant interactions:
•Allopurinol and azathioprine
•Trimethoprim and azathioprine
Methotrexate
Key clinical management points:
•Once weekly treatment
•Need for prophylactic weekly folic acid on a different day of administration
•Essential counselling on side effects
•Potential for drug interactions
•Used to maintain remission in chronically active Crohn’s Disease
•Steroid sparing properties
•Not first line
•Used when thiopurines fail or are not tolerated
•Given orally or s/c or i/m once a week
Methotrexate
•Side effects:
•Pneumonitis, hepatotoxicty, bone marrow suppression
•
•Monitoring:
•FBC, CrCl, LFTs 1-2 weekly initially then
every 2-3 months, CXR
Metronidazole
Key clinical management points:
•Ensure not continued long-term
•Essential counselling on side effects
•Potential for drug interactions
•
•Used to maintain remission in ileocolonic Crohn’s disease after complete resection of inflamed bowel
•3 months post-operative treatment with azathioprine
Infliximab and adalimumab
NICE Guidelines: Inducing Remission in Crohn’s Disease:
“Treatment with infliximab or adalimumab should only be continued if there is clear evidence of ongoing active disease as determined by clinical symptoms, biological markers and investigation, including endoscopy if necessary. Specialists should discuss the risks and benefits of continued treatment with patients and consider a trial withdrawal from treatment for all patients who are in stable clinical remission. People who continue treatment with infliximab or adalimumab should have their disease reassessed at least every 12 months to determine whether ongoing treatment is still clinically appropriate. People whose disease relapses after treatment is stopped should have the option to start treatment again”
Other treatments
•NRT
•Smoking has a protective effect on UC (opposite effect on CD), shouldn’t recommend smoking, however some patients who have been prescribed NRT may benefit
•Surgery
•Surgical removal of the colon (colectomy) will cure UC
•Surgery is not curative in CD but 50-80% patients will need surgery due to strictures or obstructions
•Up to 30% of UC patients go on to have surgery
•Colectomy and formation of colostomy or ileostomy(stoma is formed where they have bag attached)
•Ileo-anal pouch – resection of the bowel but maintain the rectum
Future Therapies for IBD?
•Whipworm
•Gut microbiome modulators
•Antibiotics e.g. rifamixin
•Pre-biotics/ Probiotics
•Faecal microbiota transplants
•Autologous stem cell transplant