PSYCH 101 Chap 15: Psychological Disorders
1/29
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
Mental Disorders in Canada
1/5 Canadians have a mental disorder
affects everyone, leading cause of disability in Canada
$51 billion/year, direct(doctor, hospitals) and indirect (not going to work because child is sick) costs
Psychopathology
multi-component definition: (ASDMDB)
a-typical, statistically rare
socially unacceptable (behaviours not typically acceptable, ex going through trash, disheveled, broken glasses)
behaviour causes distress to person or others (may/may not have lack of insight towards one’s own health)
maladaptive - behaviours harmful/non-productive (ex. suicidal)
often product of distorted cognition (may not be aware or becomes aware then changes, ex. FBI after them)
biological dysfunction (strong biological underpinning may require medication)
Models of Psychopathology
models of maladjustment form basis, concerned with assessment, treatment, and prevention (DSCPHEMB)
Demonic: middle ages, illness from the devil and evil spirits inhabiting the body, exorcisms to get demons out, bloodletting
Medical-Biological: physiological abnormality that explains everything, assumes can be diagnosed, treated, and cured
Psychodynamic: Freud, results from anxiety from unresolved conflicts, engaging in too many defense mechanisms, stuck in one psychosexual stage
Humanistic: individual uniqueness and decision making, assumes maladjustment occurs when needs are not met, doesn’t look at more severe conditions
Behavioural: learned through selective reinforcement punishment (ex. if touch wall 3 times when come into a room, anxiety reduces, so reinforced to do it every time)
Cognitive: engage in both prosocial and maladjusted behaviours because of their thoughts (ex. low mood, thoughts associated with those is negative about self, so related to developing of depressive symptoms)
Sociocultural: family, community, and society, maladjustment in context of those things (ex. parent with anxiety behaviour, so excessive worry about being near insects, so child picks up that behaviours after observing)
Evolutionary: may be expressions of behaviour that would once have been normal in history, to protect ourselves
Best Approach/Model
(Psychopathology)
an eclectic approach choosing the model that seems to fit the problem
a biopsychosocial approach combines biology, psychology, and social factors
3 Main Considerations about Mental Illness
most people do recover from mental illness
few people with mental illness are violent
most people with mental illness bear their pain privately
Misconceptions about Mental Illness
psychiatric diagnosis is nothing more than pigeonholing (labelling);
are unreliable;
are invalid;
stigmatize people
Diagnostic and Statistical Manual of Mental Disorders (DSM)
DSM-5 TR(text revision) is the most recent
published by American Psychiatric Association
manual to help guide diagnosis, a system for diagnosing maladjusted behaviour
takes into consideration if it’s malingering (fake symptoms), there is a physical cause (substance use, thyroid issues, etc.), culture rates, gender, etc.
Criticisms of DSM-5
validity; doesn’t always follow Robin & Guze’s 3 stage way/criteria for validity
high level of comorbidity - 2 or more disorders are present at the same time (anxiety + depression)
reliance on categorical rather than dimension model of psychopathology: “have it or don’t”, no in between
vulnerable to political and social influences (homosexuality was originally in there, gender dysphoria still is (trans/nonbinary))
Multiaxial
(DSM)
DSM-5 no longer multiaxial (CIGPEG)
I. Clinical disorders
II. Personality disorders (harder to treat) + intellectual development disorders (problems with functioning, less then 70 IQ)
III. General medical conditions
IV. Psychosocial or environmental problems
V. Global assessment of functioning (GAF) (1-100 of functioning ability)
Generalized Anxiety Disorder (GAD)
(Types of Anxiety)
continuous anxiety, about multiple things, for at least 6 months
physiological symptoms, concentration difficulty, fatigue, usually trouble sleeping, etc
ex. laying down for bed, thinking about boss looking at you, maybe multiple times, see computer screen not about work, maybe he thinks you never work, etc, etc, → can’t sleep, not awake next day, affect performace
3% of population, 1/3 develop after major stressor
Panic Disorder
(Types of Anxiety)
repeated, unexpected panic attacks, out of the blue, usually not triggered
ex. in shower all of a sudden start sweating, heart race, can’t breathe
symptoms: heart palpitations, sweating, dizziness, choking, sitting/pressure on chest, derealization, nausea, cold or hot
can develop concern about happening again, they persist → change in personal behaviour in attempt to avoid them
Agoraphobia
(Types of Anxiety)
fear and avoidance of being alone in a place in which escape may be difficult or embarrassing
symptoms: hyperventilation, extreme tension, cognitive disorganization
Social Anxiety Disorder
(Types of Anxiety)
fear of and desire to avoid situations where one might be scrutinized by others, both positive and negative evaluations
avoidance and impairment
ex. don’t go in big groups, don’t date, no family gatherings
Specific Phobias
(Types of Anxiety)
persistent and irrational fear of particular object or situation, and avoiding it which is impairing, excessive concerns about that thing
ex. blood phobia, needle phobia, claustrophobia
Obsessive-Compulsive Disorder (OCD)
(Types of Anxiety)
2 components:
obsessions: persistent and uncontrollable thoughts (anxiety provoking) + irrational beliefs
compulsions: actions, compulsive rituals that interfere with daily life → reduce tension/anxiety
severity associated with time spent on compulsions, aware of it but not able to stop
Explanations for Anxiety Disorders
(COLAB)
learning models focus on acquiring fears via classical conditioning, then maintaining them through operant conditioning, ex. this brought relief last time, so do it again
observing, ex. parent avoid insects, so kids pick up on excessive worrying/avoidance
catastrophic thinking, ex. “it’s really windy, there’s got to be a tornado because there was a tornado near here once”
anxiety sensitivity - aware of bodily changes that could mean something is wrong, ex. heart racing, “something is wrong, what is it?”
biological - genetics
OCD Perspectives
Freud: believed OCD originated from difficulties in the anal stage of development where they learn to control themselves (if stuck, become controlling of other things
Learning theorists: order in a person’s environment reduces uncertainty/anxiety, thus reinforces
Biopsychologists: genetic component to OCD, leading to a drug treatment
learning component, neurochemicals, genetic components
Covid Stress Syndrome
Dr. Asmundson (UoRegina), Dr. Taylor (UBC)
longitudinal study, population-based, sample of Canadians + Americans, administered 3 times, multi-faceted
5 aspects: (DSPTC)
danger + contamination fears
socio-economic consequences
xenophobia (of foreigners that may be carrying infection)
traumatic stress syndrome (some people more concerned about getting covid than experiencing death)
compulsive checking + reassurance seeking
Covid Stress Scales assess these, 12 language translations
Major Depression Disorder
12% prevalence rate
must have at least 5 of 9 symptoms, including depressed mood or loss of interest/pleasure
symptoms must be present for at least 2 weeks and represent change from previous functioning, cause clinically significant distress or impairment
first episode prior to age 40, after one episode, more likely to have another, average length is 6 months to 1 year
1.3 million Canadians affected each year, women 2x more likely to be diagnosed (reaching out, symptom/presentation difference, hormonal changes, victimization)
Symptoms of Major Depression Disorder
At least 5: (ACEND DIAL) or (CAD DENIAL)
*depressed mood
*loss of interest and pleasure in usual activities
insomnia (can be not getting to sleep, not staying asleep, not able to wake up early)
shift in activity level (lethargic or agitated)
poor appetite + weight loss, or increased + weight gain
loss of energy, fatigue
negative self-concept, self-reproach/blame, worthlessness, guilt
complaints or evidence of difficulty in concentrating (slowed thinking, indecisiveness)
reccurrent thoughts of death or suicide (not just fear of death, but serious considerations/plans)
Causes of Major Depression Disorder
Biological theories: both genetics + neurotransmitters underlie
monoamine theory- results from deficiencies of monoamines or inefficient receptors (serotonin, norepinephrine, dopamine)
Cognitive theories:
Beck:
1. Negative Triad - depressed people have negative views of themselves, environment, and future
2. Negative schemas - negative way to evaluate things
3. Cognitive Distortions - supports 1^ and 2^, certain ways of thinking about things, “negative glasses”, Black and white (all good/bad), ignoring positiveLearned helplessness: Seligman, no control in situations, so give up
Biopsychosocial Model:
vulnerability: person’s diminished ability to deal with life events (biological, genetic predisposition)
the more vulnerable, the more likely to develop, but still need environment/stress to initiate depression
diathesis-stress model: link between vulnerability and stress, with high vulnerability, only need small environmental change to trigger
Learned Helplessness
(Theories of Major Depression Disorder)
behaviour of giving up or not responding when exposed to negative consequences which they feel they have no control over
Seligman suggested people’s beliefs about the causes of failure (attributions) determines whether they will become depressed
if we think “my fault or someone else’s”, more likely to develop → Internally attributed
Bipolar Disorder
2 extremes:
depression - major depressive episode
mania - rapid speech, inflated self-esteem (extremely brilliant), impulsiveness (little thought/care for consequences), euphoria (limited touch with reality), decreased need for sleep (days on end)
equally common in men/women, 1-2% of population, strong genetic component
Bipolar II only goes up into hypo-mania then depressive, no full mania
Dissociative Disorders
characterized by: sudden, temporary, alteration in consciousness, identity, behaviour, and/or memory
Includes:
Dissociative amnesia - sudden and extensive inability to recall important personal info
Dissociative fugue (not in DSM-5) - suddenly leave home/work and assumes new identity
Dissociative Identity Disorder (DID) (previously Multiple Personality Disorder) - existence of 2 or more distinct personality or ego states with different ways of interacting, idea that once had a traumatic physical/sexual abuse experience (often caregiver) and can’t escape, so creates ego states to cope
Schizophrenia
affects 1% of the population, lack of reality testing (what real is), deterioration of social + cognitive functioning, inability to meet life demands
(+)Positive symptoms: don’t occur those without, but do in those with schizophrenia, adds to the presentation, ex. delusions, hallucinations
(-)Negative symptoms: normally occur, but not in those with schizophrenia, absent from presentation, ex. flat affect (saying “I’m very scared” but no visible change)
Schizophrenia Characteristics
Delusions: incorrect beliefs, ex. “I am god”, “I am being stalked by the FBI”
Hallucinations: compelling perceptual experiences without any actual physical stimulations
across all modalities: visual, auditory (most common), tactile, olfactory (smell), gustatory (taste)
Distortions in emotional expression: (FAID)
inappropriate affect - emotional response not appropriate in the circumstance, ex. laugh at a death
flat affect - ex. saying “I’m very scared” but no visible change
ambivalent affect - showing wide range of emotions in a brief period
disorganized thinking/speech - onto new topics constantly or “word salad”, words strung together
First sign: non-specific symptoms of anxiety, mood difficulties, isolation, difficulty maintaining logical thought and coherent conversation (prodromal period/phase)
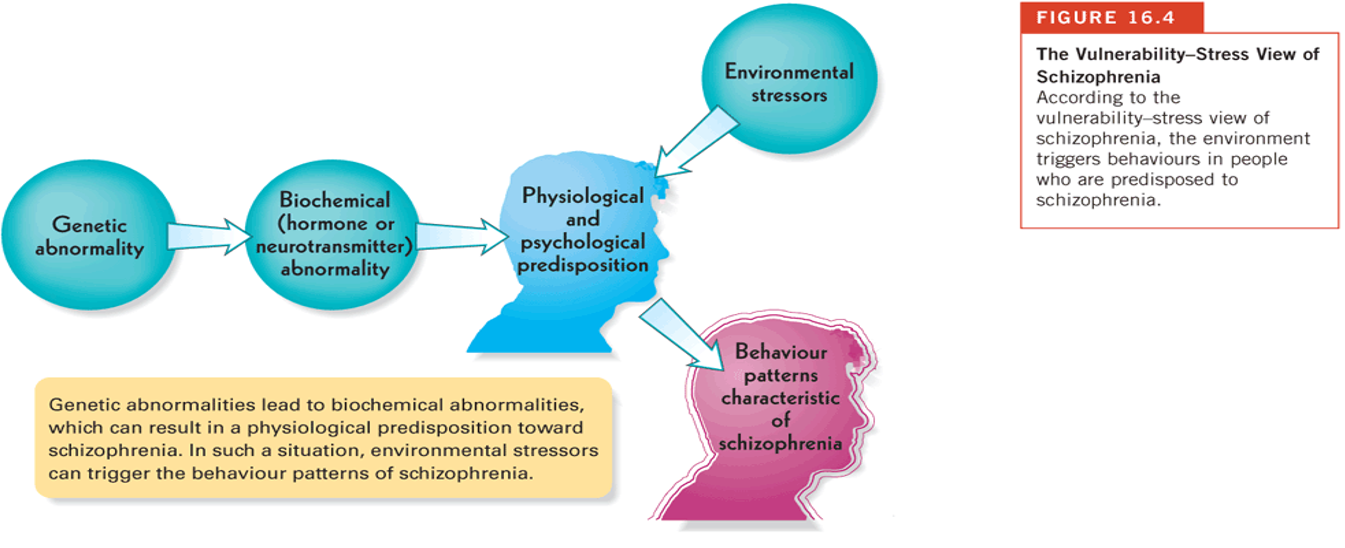
Causes of Schizophrenia
most theorists adopt diathesis-stress model
genetic or biological vulnerability underlies schizophrenia
life stress interacts with vulnerability to produce schizophrenia
Biological:
brain abnormalities - enlarged ventricles, increased sulci size, hypofrontality
neurotransmitter dysfunction - dopamine and serotonin
genetic - 48% concordance with monozygotic twins
No Environmental:
“schizophrenia mother” (parents confusing children, difficulty communicating, or give inconsistent messages) is a myth
Personality Disorders
described people with long-standing, inflexible, maladaptive behaviours that cause stress and social/occupational difficulties
(BAD PHAN)
Paranoid personality disorder
pervasive pattern of odd/eccentric behaviour, distrust/suspicion of others
Borderline personality disorder
instability in mood, identity, impulse control, often high self-destructive, trouble with relationships, mainly women, ~2% of population
Histrionic personality disorder
emotionality, attention seeking by exaggerating situations in their lives
Narcissistic personality disorder
grandiosity, need for admiration, lack of empathy, exaggerated sense of self-importance
Antisocial personality disorder
disregard for and violation of right of others, impulsivity, self-centered
Avoidant personality disorder
social inhibition, feelings of inadequacy, hypersensitivity to negative evaluation
Dependent personality disorder
need to be taken care of, submissiveness and clinging behaviours, fears of separation
Violence and Mental Disorders
most are not violent, delusions and manic phase of Bipolar Disorder may have greater risk
more likely to be danger to themselves, suicide
Warning Signs for Suicide
depression
verbal statements like “You’d be better off without me”
expressions of hopelessness and helplessness
daring and risk-taking behaviour that is atypcial
personality changes like withdrawal, aggression, moodiness
giving away prized possessions
lack of interest in the future