PSY 341 Exam 3
1/149
Earn XP
Description and Tags
UNR Dr. Fisher
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
150 Terms
Anorexia nervosa
Extreme weight loss. Restriction of calorie intake below energy requirements. Intense fear of weight gain accompanied by body image distortion
Subgroups in the US that are higher at risk for developing anorexia nervosa
Restricting and Binge-eating-purging
Most effective treatment for anorexia nervosa
Psychoeducation: Behavioral and cognitive interventions, Target food, weight, body image, thought, and emotion.
Motivational interviewing: Helps individual resolve ambivalent feelings and insecurities about changing their behavior
Bulimia nervosa
Eating excess amounts of food in a discrete period of time. Eating disorder involving alternation between eating large amounts of food in a short time, then compensating by vomiting or other extreme actions to avoid weight gain.
Most effective treatment for bulimia nervosa
Cognitive-behavioral therapy (most evidence based approach) = Treatment of choice. Principal focus is on the distorted evaluation of body shape and weight and on maladaptive attempts to control weight in the form of strict dieting and compensatory activities. Promotes regular eating behavior. Focused on altering dysfunctional thoughts and attitudes regarding body shape, weight, and eating.
Binge-eating disorder
Individuals may binge repeatedly and find it distressing, but they do not attempt to purge the food. Eating excess amounts of food in a discrete period of time. Perceived as ‘out of control’ or uncontrollable. May be associated with guilt, shame, or regret. May hide the behavior from family
Most effective treatment for binge-eating disorder
Cognitive-behavior therapy. Similar format to bulimia Interpersonal psychotherapy. As effective as CBT. Medications, SSRIs (e.g., Prozac, Zoloft) No benefit
Night eating syndrome
Patients get up during the night to eat. Associated with obesity, binge eating, and psychological distress
Obesity
Considered BMI of 30+. Not DSM disorder, but may be a consequence.
Most effective treatment for obesity
Efficacy: Moderate success with adults. Greater success with children and adolescents. Recent study suggests that the combination of: Restricted caloric intake, Increased physical activity, and Behavior therapy tends to lead to more weight loss than any of these components on their own. Treatment progression- from least to most intrusive options
Cultural influences associated with the risk of developing eating disorders
North American populations: highest prevalence rates found among white middle and upper middle class females.
Immigrants to western cultures: Increase in western culture. Increase in obesity
Cultural values linked to standards for body image
“The symptoms of anorexia nervosa are usually ego-syntonic and hence persons who meet criteria for anorexia nervosa are not motivated to participate in treatment”.
Ego-syntonic: Unlike other disorders, patients often feel consistent with one's identity; patients don't feel that treatment is necessary.
Motivational interviewing
Helps individuals to resolve ambivalent feelings and insecurities about changing their behavior
Motivational interviewing for anorexia nervosa
Helps individuals resolve ambivalent feelings and insecurities about changing their behavior in regard to eating more/less
Motivational interviewing for bulimia nervosa
Helps people become motivated to change the behaviors that are preventing them from making healthier choices.
Goals of family therapy for anorexia nervosa
Two goals:
Eliminate negative and dysfunctional communication surrounding food and eating.
Promote healthier attitudes toward body shape and body image
Goal of hospitalization for the treatment of anorexia nervosa
Majority of those hospitalized respond to treatment achieving weight restoration is generally the cornerstone of inpatient treatment given its centrality to recovery
What are the long-term outcomes for persons receiving inpatient treatment for anorexia nervosa?
Most programs employ a multidisciplinary team approach combining individual, family, and group psychotherapy. Despite progress while in hospital, relapse rates range from 30-70% following inpatient care
Prevalence of obesity in the US
In 2000, 30.5% for adults. In 2023, 40.3% for adults. Children (ages 2-19) 19.7% in 2023
Why is obesity considered to be occurring at epidemic levels in the United States?
Due to a combination of factors, including lifestyle, environmental influences, and genetic predispositions.
How has access to electronic media affected the prevalence of obesity?
It promotes inactive, sedentary lifestyle.
Stepped-care approach to treatment of obesity
First step: Self-directed weight loss program.
Second step: Commercial self-help programs.
Third step: CBT - most effective non-surgical treatment.
Last step: Bariatric surgery - results in greater weight loss than non-surgical treatment
Purging techniques
Self-induced vomiting after eating. Use of medications. Excessive exercise
Purging disorder
Most common compensatory behavior. Person purges their food after eating
Bariatric surgery
Procedure include gastric bypass, sleeve gastrectomy, gastric band and duodenal switch Results in greater weight loss than non-surgical treatment
Phases of sexual response cycle
Desire, arousal, orgasm, and resolution
Sexual disorders associated with desire
Male hypoactive sexual desire disorder, erectile disorder
Sexual disorders associated with arousal
Female sexual interest/arousal disorder, paraphilic disorder, voyeurism, exhibitionism, transvestic disorder,
Sexual disorders associated with orgasm phases
Female orgasmic disorder, paraphilic disorder
What are the most common complaints among women who seek therapy for sexual problems?
Women has significantly difficulty achieving orgasm
What are the most common complaints among men who seek therapy for sexual problems?
Men have a difficulty achieving or maintaining an erection
Biological factors to sexual dysfunction
Physical diseases, chronic illness, prescription medication, alcohol and drugs
Psychological factors to sexual dysfunction
People with sexual dysfunction are more likely to experience anxiety and negative thoughts about sexual encounters. May actively avoid awareness of sexual cues
Commonly used medications that can have adverse effects on sexual functioning
Antihypertensive medication, antidepressants SSRIs
Short term effects of alcohol on sexual functioning
Difficulty achieving or maintaining an erection, delayed ejaculation, decreased sexual sensitivity, and potentially lowered inhibitions
Long term effects of alcohol on sexual functioning
Delirium tremens – Hallucinations and tremors brought on by withdrawal from severe alcohol use.
Fetal alcohol syndrome – Problems in fetus from alcohol use during pregnancy. Alcohol crosses the placenta. Potential consequences of alcohol use in pregnancy: Impaired growth and life-long cognitive difficulties of child.
Medical treatments for sexual dysfunction
Male Erectile dysfunction = vasodilators, Injection of vasodilating drugs into the penis, testosterone, penile prothesis or implants, vascular surgery, vacuum device therapy.
Female sexual dysfunction = Levitra
Psychological treatments for sexual dysfunction
Education about sexual responses/foreplay, sensate focus and nondemand pleasuring, sexual activity with the goal of focusing on sensations without trying to acheive orgasm, “homework”
Why is it difficult to obtain accurate data regarding the prevalence of the paraphilias?
People often have a difficult time reporting these atypical behaviors because of social concerns.
Role of anxiety in voyeurism
Risks in association to intensify sexual arousal
Role of anxiety in exhibitionism
Element of thrill and risk is necessary for sexual arousal
Sexual dysfunction
Problems with sexual responses
Male hypoactive sexual desire disorder
Little or no interest in any type of sexual activity. Masturbation, sexual fantasies, and intercourse are rare. Accounts for half of all complaints at sexuality clinics. affects 5% of men
Female sexual interest/arousal disorder
Lack of or significantly reduced sexual interest/arousal. Typically manifesting in reduced sexual interest, reduced sexual activity, fewer sexual thoughts, reduced arousal to sexual cues, reduced pleasure or sensations during almost all sexual encounters
Erectile disorder
Difficulty achieving or maintaining an erection, sexual desire is usually intact, most common problem for which men seek treatment, prevalence increases with age (60% of men over 60 experience erectile dysfunction)
Female orgasmic disorder
Marked delayed, absence, or decreased intensity of orgasm in almost all sexual encounters, Not explained by relationship distress or other significant stressors, 1 in 4 women has significant difficulty achieving orgasm
Delayed ejaculation
A condition that makes it difficult or impossible for a man to achieve orgasm, despite having sexual desire and stimulation
Premature ejaculation
Ejaculation occurring within ~1 minute of penetration and before it is desired. Most prevalent sexual dysfunction in adult males. Affects 21% of all adult males. Most common in younger, inexperienced males. Problem tends to decline with age.
Genito-pelvic pain/penetration disorder
In females, difficulty with vaginal penetration during intercourse, associated with one or more of the following: pain during intercourse or penetration attempts, fear/anxiety about pain during sexual activity, tensing of pelvic floor muscles in anticipation of sexual activity
Vaginismus
Pelvic muscles in the outer third of the vagina undergo involuntary spasms when intercourse is attempted
Vulvodynia
Classified as a genito-pelvic pain/penetration disorder. Chronic pain in the area on the outside of a woman’s genitals.
Sexual pain disorders
Common in women. Described with sensations of burning, rawness, or stinging. Associated with tensing and tightening of the pelvic floor muscle during intercourse
Directed masturbation
A sex therapy strategy in which the therapist advises the client on how to masturbation activities to help overcome a sexual problem
Sensate focus
A sex therapy technique that helps people explore their bodies and sexual sensations without the pressure of performance or orgasm
Fear of performance
Performance anxiety that affects sexual activity in particular. A person who has this condition will often be overcome by a fear that they'll be unable to perform either before sexual activities or during them.
Orgasmic reconditioning
A behavioral treatment aimed at altering the deviant sexual preferences of individuals who commit sex offenses, including rape, pedophilia, and child molestation
Paraphilic disorders
Repeated and intense sexual urges or fantasies in response to objects or situations that society deems inappropriate; may behave inappropriately
Fetishistic disorder
Sexual attraction to nonhuman objects. Objects can be inanimate/or tactile.
Frotteruristic disorder
Persistent pattern of seeking sexual gratification from rubbing up against unwilling others. Often occurs in crowds and/or confining situations from which the other person cannot escape
Voyeuristic disorder
Observing an unsuspecting individual undressing, naked or engaged in sexual activity. Risk associated with “peeping” may intensify sexual arousal
Exhibitionistic disorder
Exposure of genitals to unsuspecting strangers. Element of thrill and risk is necessary for sexual arousal
Sexual sadism
Inflicting pain or humiliation to attain sexual gratification
Sexual masochism
Suffering pain or humiliation to attain sexual gratification
Incest
Sexual activity between close relatives
Pedophilia
Sexual attraction to prepubescent children. Vast majority of sufferers are male. Pedophilic urges are limited to incest. Many suffers do not act on desires.
Covert sensitization
In which client imagines engaging in behavior and then facing negative consequences, such as being caught, arrested, losing job
Penile plethysmorgraphy
Device for measuring sexual arousal in males. Measures circumference changes
Orgasmic reconditioning
Behavioral treatment that aims to change sexual preferences and behaviors
Diagnostic criteria for substance use disorder
Taking moderate amounts of a substance in a way that doesn’t interfere with functioning
Diagnostic criteria for physiological substance dependence
Defined by drug-seeking behavior. Tolerance and withdrawal. Taking more of the substance than intended. Desire to cut down use. Excessive time spent using/acquiring/recovering. Craving for the substance. Role disruption (e.g. can’t perform at work, effectively parent). Interpersonal problems
Tolerance
Needing more of a substance to get the same effect/reduced effects from the same amount
Substance withdrawal
Physical response when substance is discontinued after regular use
5 main categories for substances
Depressants, stimulants, opiates, hallucinogens, and other drugs of use
Depressants
Behavioral sedation
Stimulants
Increase alertness and elevate mood
Opiates
Produce analgesia and euphoria
Hallucinogens
Alter sensory preception
Other drugs of abuse
Include inhalants, anabolic steroids, and medications
Adverse physiological effects of alcohol abuse
Central nervous system depressant. Initially depresses inhibitory centers in the brain. More areas of brain are depressed as drinking continues. Influences several neurotransmitter systems specifically targeting GABA.
What is the evidence for environmental/cultural influences on the risk of developing substance related disorders?
Exposure to drugs is a prerequisite for use of drugs. Media, family, peers can influence exposure to drugs. Parents and the family appear critical. The role of cultural factors: Influence the manifestation of substance abuse. Some cultures expect heavy drinking at certain social occasions. Cultural expectancies of substances may influence drug-related behavior
Association between alcohol and violence
Alcohol consumption is strongly linked to violence, and can increase the risk of being a victim or perpetrator of violence
Effects of alcohol use and violence
Drinking does not cause violence, but may increase the likelihood of impulsive behavior (domestic violence, suicide, homicide
How have the rates of opioid-related deaths increased over the past 2 decades?
Mortality rates are high for opioid addicts. High risk for HIV infection due to shared needles
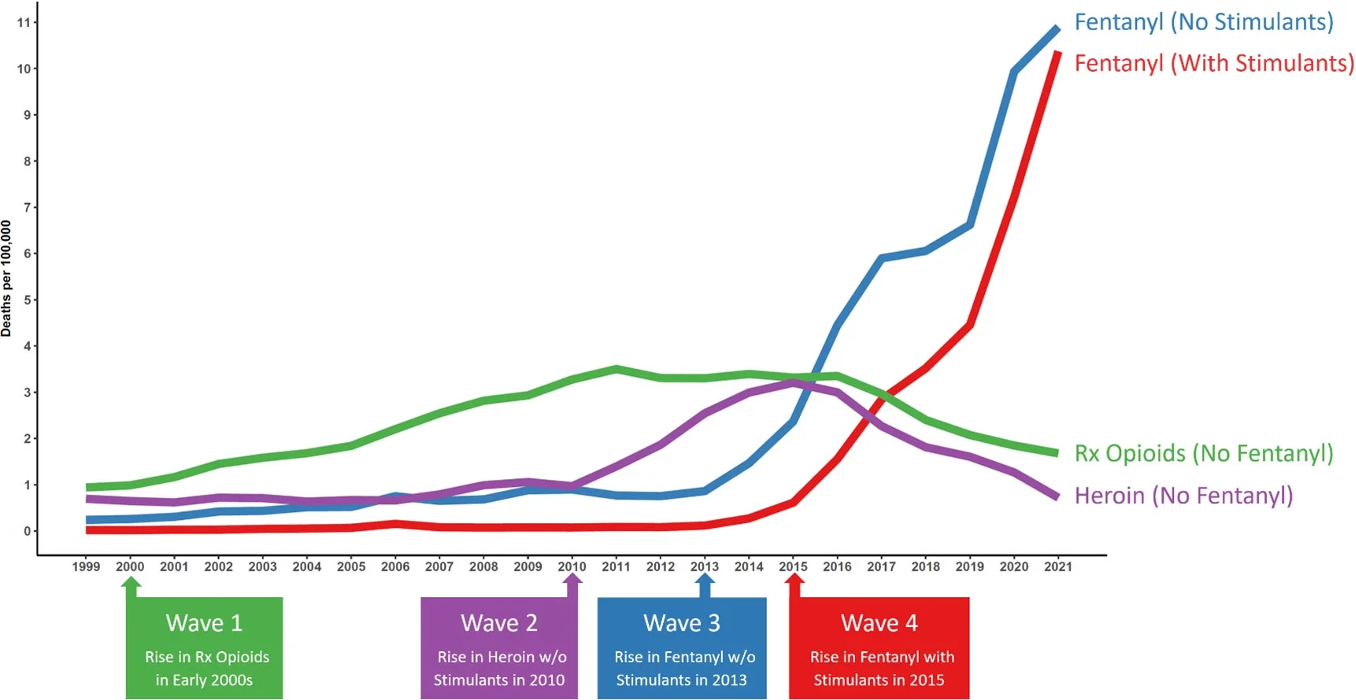
Which type of opioid has accounted for the largest increase in deaths?
Fentanyl
Agonist based treatment
Drugs called agonists to activate specific receptors in the brain
Antagonist based treatment
Drugs that block or counteract the positive effects of substances. Examples include naltrexone for opiate and alcohol problems
Aversion therapy methods for substance abuse
Drugs that make use of substances extremely unpleasant. Examples include antabuse and silver nitrate. Antabuse causes intense nausea and vomiting if the person ingests alcohol
“Alcohol is a central nervous system depressant”
A drug that slows down brain activity
Substance use
Taking moderate amounts of a substance in a way that doesn’t interfere with functioning
Substance intoxication
Physical reaction to a substance (e.g., being intoxicated)
Psychoactive substance
Alter mood, behavior, or both
Substance use disorder
Use in a way that is dangerous or causes substantial impairment (e.g., affecting job or relationships)
Substance abuse
Excessive use of a drug in a way that is detrimental to self, society, or both
Physiological dependence
A condition that occurs when the body becomes accustomed to a substance and has trouble functioning without it
Polydrug abuse
Use of more than one drug or type of drug at the same time or one after another.
What are the roles of positive and negative reinforcement in the development and maintenance of substance related disorders?
Early on, drug use may involve seeking a euphoric high (positive reinforcement)
Later, drug use will be motivated by escape from withdrawal/crash (negative reinforcement)
Opponent process theory (Substance abuse)
Drugs themselves are easiest way to alleviate feelings of withdrawal
Amphetamines
A CNS stimulant. Amphetamines stimulate CNS by stimulating the release of norepinephrine and dopamine. Also block reuptake.
Alcohol use disorder
A chronic brain disease that causes a person to be unable to control their alcohol use, even when it causes negative consequences
Relapse prevention
Cognitive-behavioral approaches to learning new habits that make relapse less likely.