Advanced surgery, wound care and bariatrics
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
What is Enhanced Recovery?
Evidence-based approach to enable faster recovery after major surgery
Begins pre-operatively and continues with patient after discharge
Involves multidisciplinary team
Medical; surgeon, anaesthetist, frailty
Therapies; nutrition, home environment, mobility, limitations
Pharmacist; meds rec, peri-op meds changes, optimising diabetes, anaemia, pain
Nurse; bloods, history taking, counselling
What needs to be right post-op to ensure Enhanced Recovery?
Optimise anaemia; reduce need for blood transfusions
Avoid anxiolytics/sedating medication
Optimise pain control, reduce opioids
Compression stockings
Make decisions on intra-operative medicines choices
Antibiotic prophylaxis
Anaesthetic choice; general versus spinal
PONV – APFEL scoring
What should be reviewed on a surgical drug chart
Pre-op
during surgical management
Post-op
Medicines reconciliation; optimise medicines pre-op including holding where appropriate
Pain relief, PONV, laxatives, anti-emetics, VTE-P, nutritional drinks
•Start new medicines dependent on operation
•Stop medicines no longer needed
•Counsel patient on new medication, acute and chronic
State the different classifications of obesity.
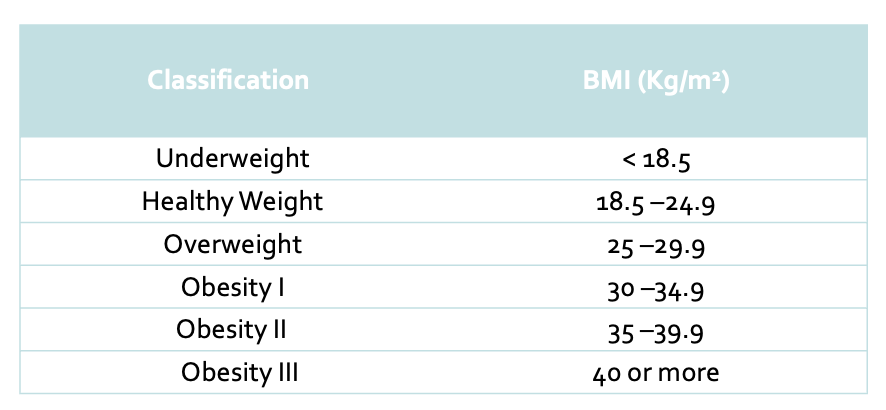
What is obesity?
BMI 30 and over
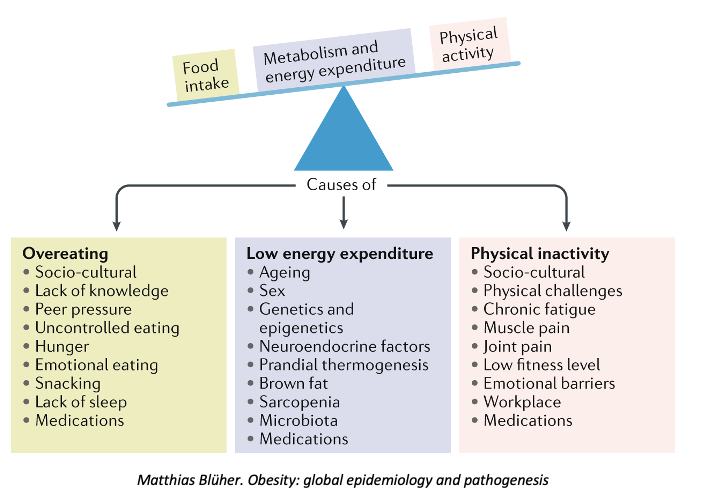
The pathogenesis of obesity has been recently understood as not simply an imbalance between calories consumed and energy expended, with metabolic parameters and appetite regulation via gastric and peripheral nervous systems understood to play a significant role
Describe the Pathogenesis of Obesity on a diagram
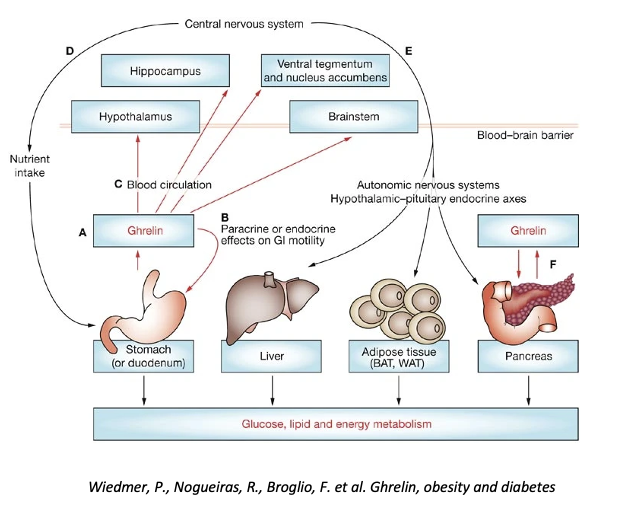
Describe and explain what GI hormone are involved in the Pathogenesis of Obesity.
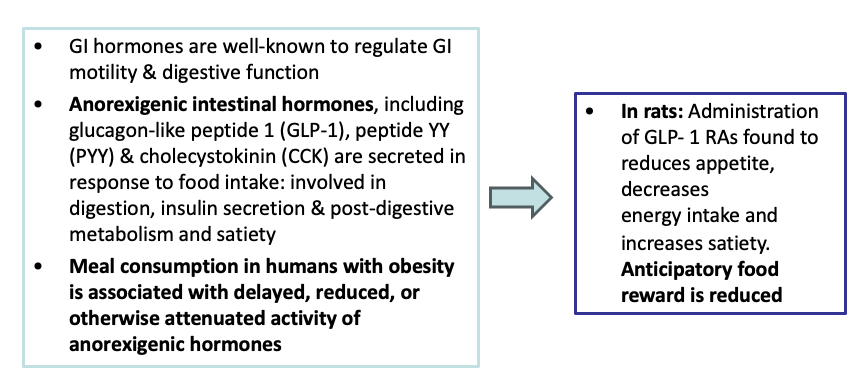
GI hormones are well-known to regulate GI motility & digestive function
Ghrelin is primary produced in the gastric fundus and is responsible for appetite stimulation
Obesity is associated with reduced post-prandial ghrelin suppression
Anorexigenic intestinal hormones, including glucagon-like peptide 1(GLP1), peptide YY (PYY) & cholecystokinin (CCK) are secreted in response to food intake: involved in digestion, insulin secretion & post-digestive metabolism and satiety
Meal consumption in humans with obesity is associated with delayed, reduced, or otherwise attenuated activity of anorexigenic hormones
Leptin is predominantly secreted by white adipose tissue
Circulating levels correlate with fat mass and represent a hormonal signal of body energy stores
In individuals with more body fat, serum, plasma and CSF leptin levels are elevated
What are the treatments for obesity?
What is Liraglutide?
is a GLP-1 analogue with an attached acyl chain which allows non-covalent binding to albumin. This delays both the inactivation of liraglutide by dipeptidyl peptidase 4 and renal clearance, extending the half-life of GLP-1 from one to two minutes for native GLP-1 to 11–15 hours allowing once daily administration. In T2DM, liraglutide has been shown to improve glycaemic control, reducing glycosylated haemoglobin A1c (HbA1c), and reducing body weight
Liraglutide is recommended as an option for managing overweight and obesity alongside a reduced-calorie diet and increased physical activity in adults, only if:
They have a body mass index (BMI) of at least 35 kg/m2 (or at least 32.5 kg/m2 for members of minority ethnic groups known to be at equivalent risk of the consequences of obesity at a lower BMI than the white population) and
They have non-diabetic hyperglycaemia (defined as a haemoglobin A1c level of 42 mmol/mol to 47 mmol/mol [6.0% to 6.4%] or a fasting plasma glucose level of 5.5 mmol/litre to 6.9 mmol/litre) and
They have a high risk of cardiovascular disease based on risk factors such as hypertension and dyslipidaemia and
It is prescribed in secondary care by a specialist multidisciplinary tier 3 weight management service
Semaglutide is recommended as an option for weight management, including weight loss and weight maintenance, alongside a reduced-calorie diet and increased physical activity in adults, only if:
It is used for a maximum of 2 years, and within a specialist weight management service providing multidisciplinary management of overweight or obesity (including but not limited to tiers 3 and 4), and
They have at least 1 weight-related comorbidity and:
A body mass index (BMI) of at least 35.0 kg/m2, or
A BMI of 30.0 kg/m2 to 34.9 kg/m2 and meet the criteria for referral to specialist weight management services
Use lower BMI thresholds (usually reduced by 2.5 kg/m2) for people from South Asian, Chinese, other Asian, Middle Eastern, Black African or African-Caribbean family backgrounds
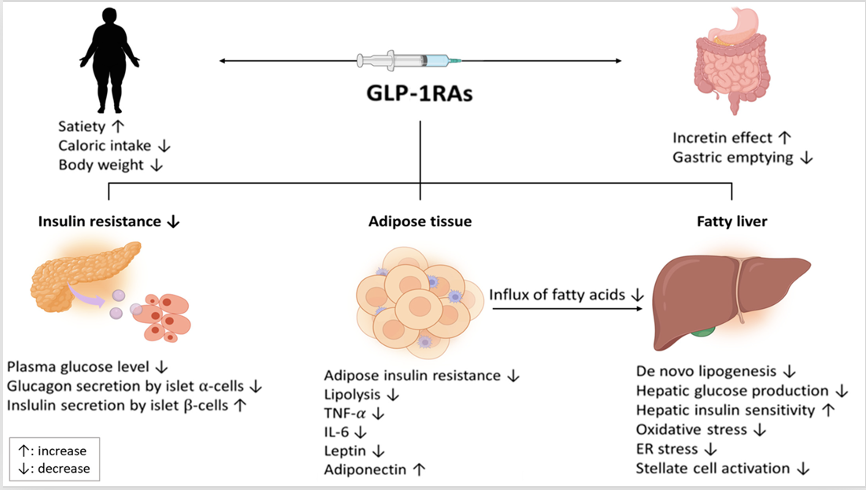
Describe the mechanism and theory of using Anorexigenic intestinal hormones (GLP 1) in the treatment of obesity
Draw a diagram to summarise the mechanism and theory of using Anorexigenic intestinal hormones (GLP 1) in the treatment of obesity
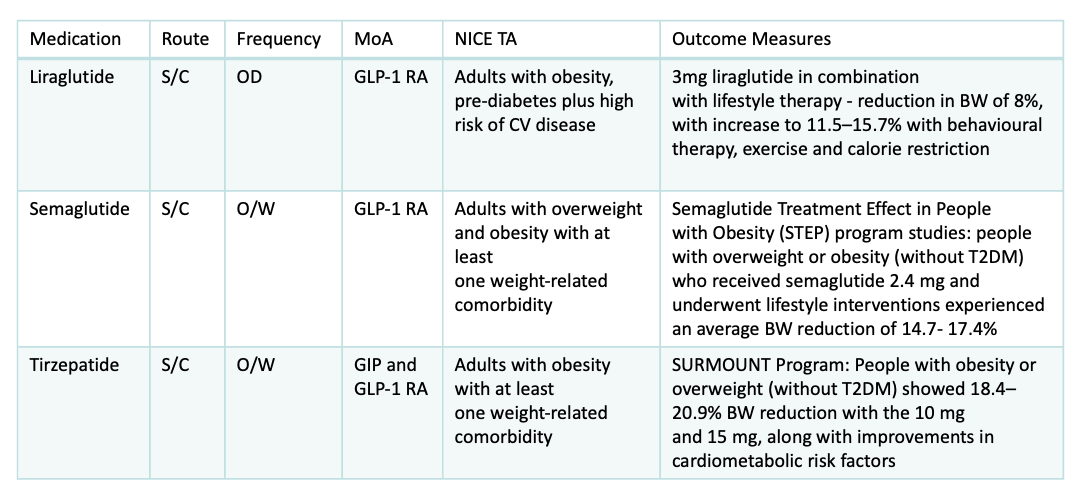
Fill in the missing gaps in the table.
What are the main pharmacokinetic properties of GLP-1 Receptor Agonists
Absorption: SC, ensuring rapid absorption and achieving peak concentrations within hours.
Distribution: GLP-1 RAs exhibit a low volume of distribution, predominantly remaining in the bloodstream. These agents selectively target GLP-1 receptors in various tissues involved in glucose regulation, with specific affinity for pancreatic cells and other metabolic control sites.
Metabolism: Many GLP-1s undergo proteolytic cleavage in various tissues, akin to the metabolism of large proteins.
Excretion: Renal elimination primarily governs the clearance of GLP-1 RAs
What are the adverse effects of GLP-1 Receptor Agonists?
Nausea
Vomiting
Diarrhoea
Dyspepsia
Injection Site Reactions
Hypoglycaemia
Dizziness
Cholecystitis
Pancreatitis
When is bariatric surgery considered in the obesity care pathway?
They have a BMI of 40 kg/m2 or more, or between 35 kg/m2 and 40 kg/m2 and other significant disease (for example, type 2 diabetes or high blood pressure) that could be improved if they lost weight
All appropriate non-surgical measures have been tried but the person has not achieved or maintained adequate, clinically beneficial weight loss
The person has been receiving or will receive intensive management in a tier 3 service
The person is generally fit for anaesthesia and surgery
The person commits to the need for long-term follow-up
Who makes up the Bariatric Team?
Surgeons
Bariatric Practitioner
Dietician
Bariatric Specialist Nurse
Bariatric Pharmacist
Psychologists
Endocrine and Weight Loss Physicians
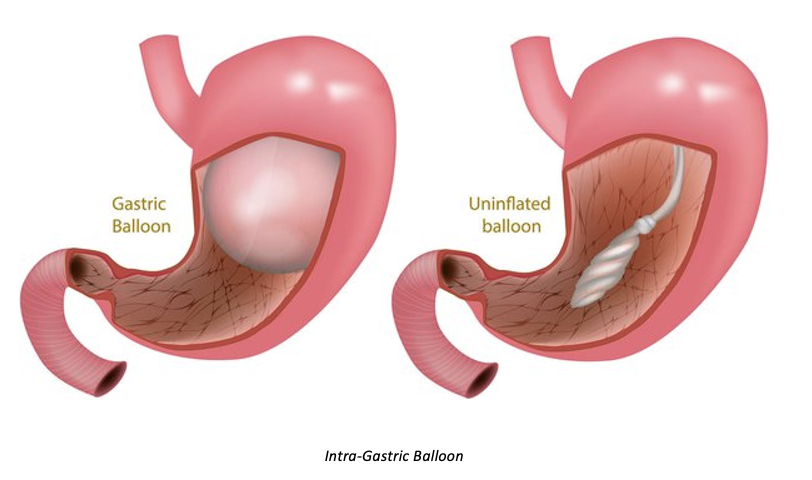
What is a Intra-Gastric Balloon: Gastric Restriction?
Not NICE
6 months only
Endoscopically inserted
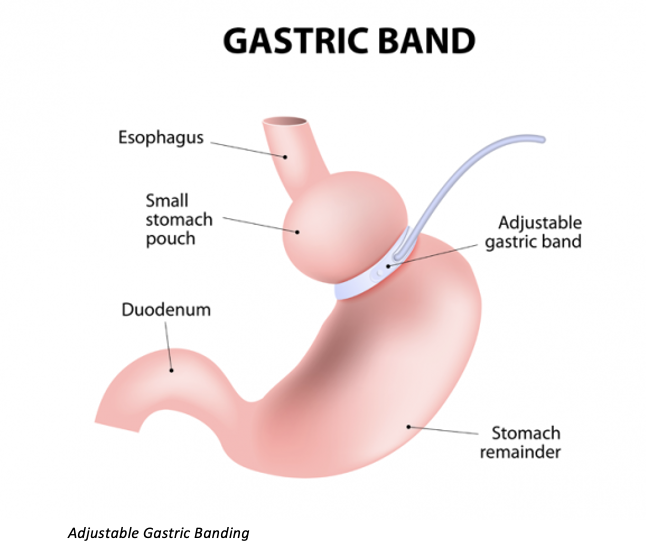
What is a Adjustable Gastric Banding: Gastric Restriction?
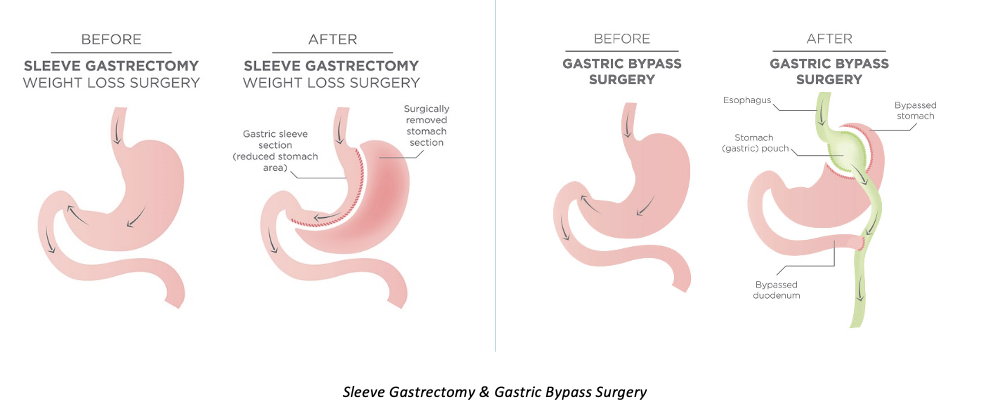
What are the Anatomical Changes Post-Bariatric Surgery?
What are the Operative (10%) Complications of Surgery?
Thromboembolism
Bleeding
Pneumonia
Stenosis
Ulcers
Infection
Hernia
Peritonitis
Death (1-2%)
What are the Long Term (20-30%) Complications of Surgery?
Iron Deficiency
Calcium & vitamin D deficiency
Vitamin B-12 deficiency
Vitamin B-1 deficiency
Protein deficiency
Gallstones
Weight Regain
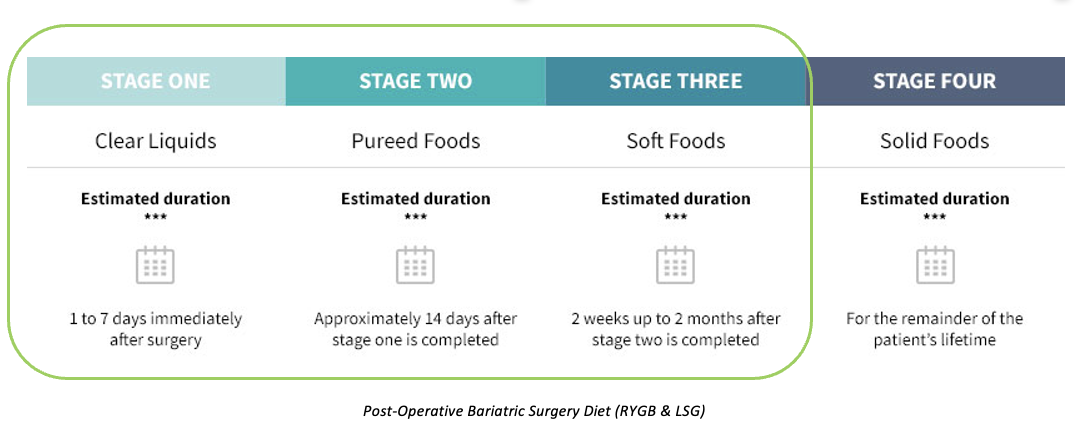
What is the Post-Bariatric Surgery Diet?
What factors affect PK in Obesity?
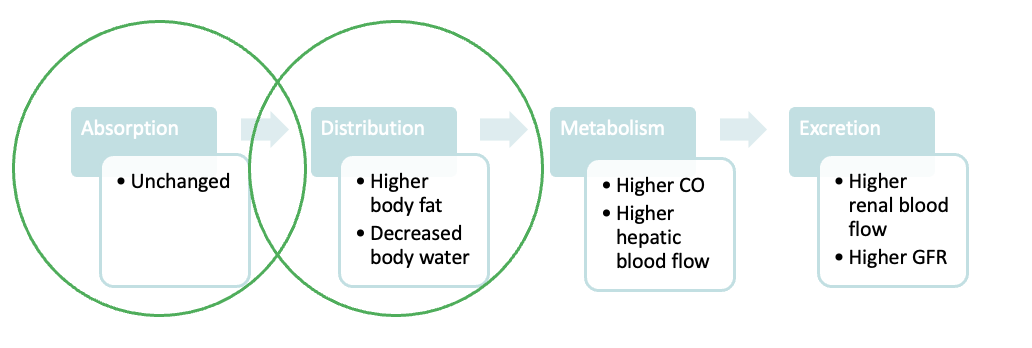
What is the Effect of Bariatric Surgery on Drug Absorption?
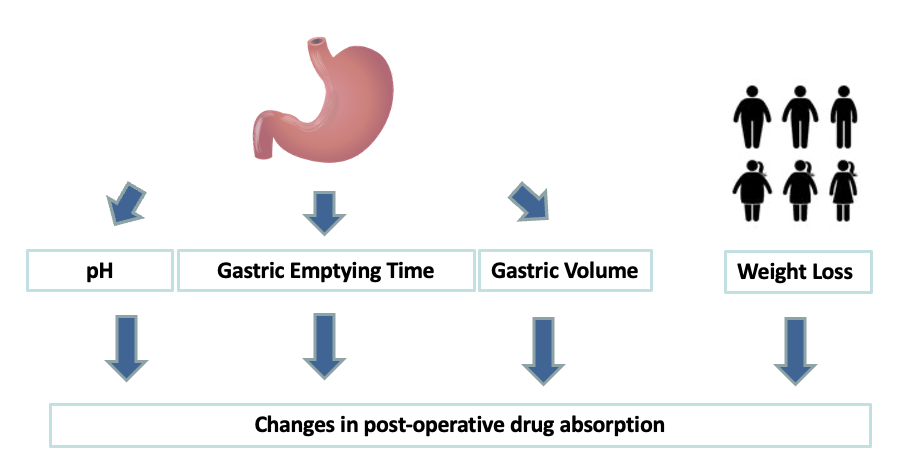
What effect does bariatric surgery have on stomach pH?
Partitioning of stomach results in decreased production of HCL
May affect bioavailability of drugs/formulations whose absorption is pH-dependent (E.g. Iron and calcium)
May be possible to use alternative salt forms or to artificially alter gastric pH
Example: Calcium carbonate depends on acid for its absorption; calcium citrate does not.
One study comparing the bioavailability of both products in achlorhydric patients found the bioavailability of calcium carbonate and calcium citrate to be 4% and 45%, respectively.
Co-administer ascorbic acid with iron supplements to convert iron to absorbable ferrous form
A drug must have a sufficient residence time at its absorption site for absorption to be…
optimal
If movement through the GI tract is too fast, the drug will…
pass through the system without being absorbed
If movement through the GI tract is too slow, the onset of…
pharmacological effect will be retarded, the drug may be degraded or the epithelium may be irritated
Do bariatric surgeries lead to a reduction in gastric volume?
All procedures result in reduced available surface area of stomach
Only limited number of drugs are absorbed through the stomach wall
Disintegration and dissolution occur in stomach
Drugs in aqueous solution more rapidly absorbed than those in oily solutions, suspensions, or solid forms
Time for complete disintegration and dissolution affect absorption and resultant bioavailability
Particular caution with drugs with narrow therapeutic index and sustained/modified release preparations
What post op considerations for Reduction in Gastric Volume post bariatric surgery?
Stomach volume reduced to ~30ml
Post-op oedema may further reduce stomach volume and opening into stomach
Solid oral medicines may get stuck
Avoid effervescent formulations (use orodispersible or allow bubbles to disperse)
Increased potential of damage to gastric mucosa e.g. Bisphosphonates, NSAIDs (avoid NSAIDS/aspirin unless definite indication e.g. MI, RA)
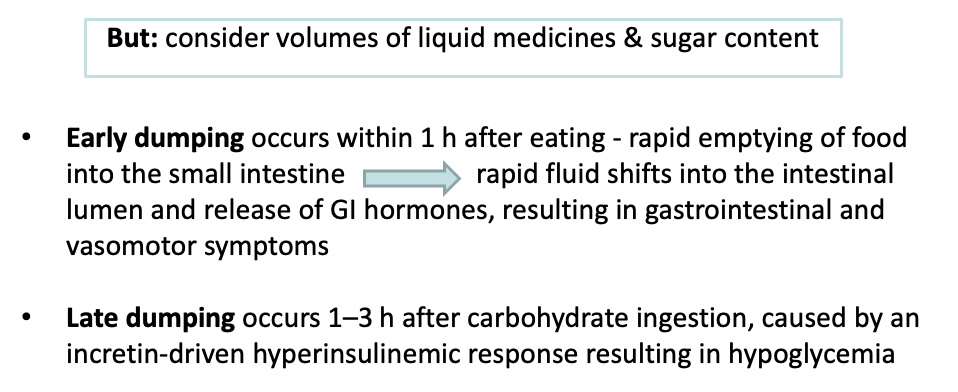
What is Reduction in Gastric Volume: Dumping Syndrome?
Describe the issues with Bypass of Absorptive Areas in bariatric surgery.
Gastric bypass procedures create a malabsorptive state for food and oral drugs
Main absorptive site for drugs: duodenum
Absorptive sites for some drugs totally bypassed
For drugs absorbed throughout GIT: surface area reduced, reduced time for absorption and enterohepaticcirculation disrupted = unpredictable reductions in bioavailability
Drugs with long absorptive phases that remain in the intestine for extended periods are likely to exhibit decreased bioavailability
Products with prolonged dissolution times, such as extended-release formulations and enteric-coated tablets, should be avoided in this population
?Compensatory absorption by other sites
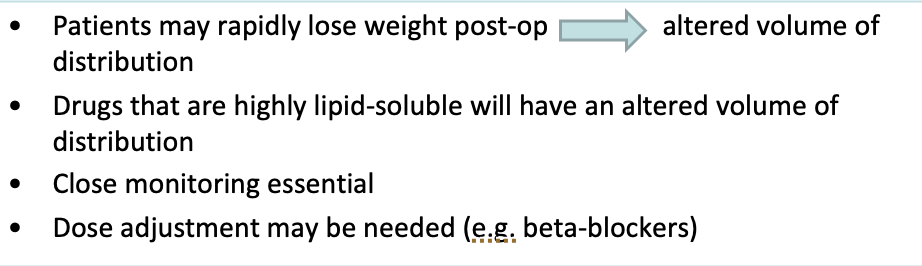
What are the changes in Volume of Distribution post bariatric surgery?
What are the key Pre-op considerations?
Often complex polypharmacy due to co-morbidities
Advise on appropriate peri-operative medicines management
VTE prophylaxis
Initiate formulation/drug changes proactively
What are the key Post-op considerations?
Close monitoring for efficacy of orally administered drug therapy
If lack of efficacy then suspect poor absorption
Consider change of formulation or route
Review drugs with GI side effects e.g. NSAIDs
Consider PPI prophylaxis
Vitamin B12 deficiency common due to reduction in functioning parietal cells and HCL in stomach.
3-Monthly B12 injections effective
Bypass patients prone to deficiencies in fat-soluble vitamins, calcium and iron: supplementation
Deficiencies less common in banding patients
Modern leech therapy is used in areas such as…
microsurgery, plastic and reconstructive surgery, cardiovascular disease and dermatology
Describe the uses of leeches in reconstructive surgery.
Following tissue transfer or reattachment, the blood supply to that area may become thick and congested; this can cause loss of part, or all the reconstructed area
A leech or leeches may be placed in the area and by draining away small amounts of blood it is possible they can relieve the congestion, keeping the blood flow going
The leech’s saliva contains numerous active ingredients such as…
anticoagulants, platelet aggregation inhibitors and proteinase inhibitors
Describe and explain use of leeches (Hirudo medicinalis) in anticoagulation therapy.
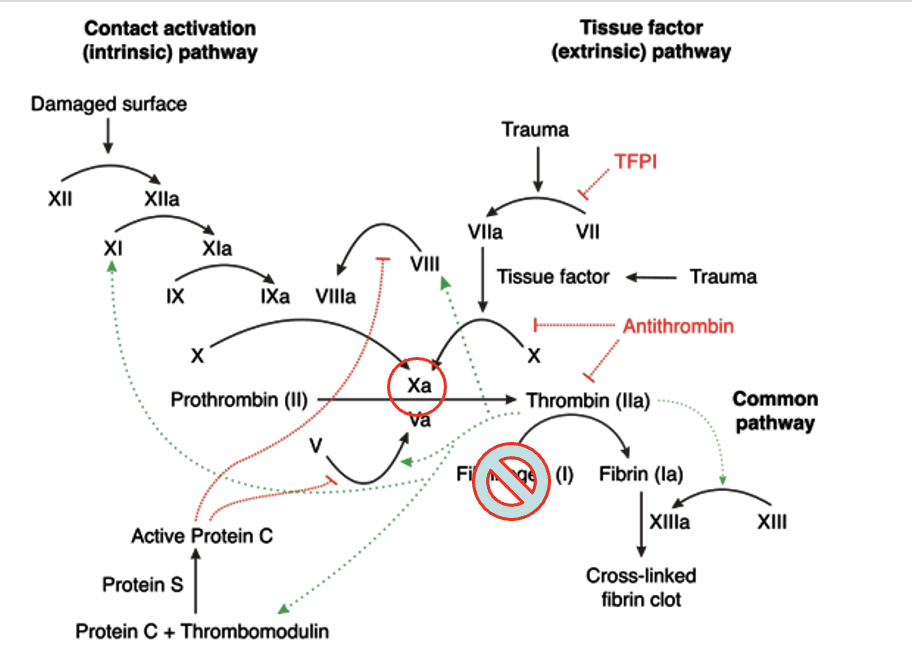
In 1884, Haycraft identify in leeches’ salivary glands an anticoagulant substance he named hirudin. As a powerful anticoagulant, it inactivates thrombin by taking the place of fibrinogen, and it also affects the Xa factor that catalyzes the conversion of prothrombin into thrombin
Hirudin maintains blood flow as the leech feeds, and immediately after the leech has finished feeding
Leech saliva contains platelet function inhibitors (e.g., calin) accounting for the persistence of bleeding following biting
Leech saliva also contains proteinase inhibitors which decrease the viscosity of the interstitial liquid and improve the depth-wise penetration of the other substances
Leech saliva also possesses a histamine-like vasodilator substance and a powerful anesthetising substance rendering the bite painless.
The bite mark can still bleed a little for up to 72 hours after the leech has detached, due to the anticoagulants in the saliva which act only locally
Describe and explain the Practical Application & Complications of leech therapy.
A piece of gauze is cut in the centre to make a hole for the desired area
The number of leeches used is decided by the surgeon
Leeches should never be detached forcibly and should be left to feed for 30-60 minutes or until they detach on their own. If still attached after an hour use table salt/alcohol swab
A new leech can be applied every 2 hours and can be tapered down to every 4 hours according to patient response and consultant review
Local infection around the wound site: Ciprofloxacin 500mg PO BD for duration of contact
Ciprofloxacin selected as excellent bioavailability; reaches site of leech bite and covers gram-negative bacteria typically transmitted during procedure
Prolonged bleeding
Allergy
What is Larval Therapy?
Maggot therapy involves the use of maggots of the green-bottle fly, which are introduced into a wound to remove necrotic, sloughy and/or infected tissue. Maggots can also be used to maintain a clean wound after debridement if a particular wound is considered prone to re-sloughing
The technique, which has been used for centuries, has been reintroduced into modern medicine by doctors and tissue viability specialists who have found that maggots are able to cleanse wounds much more rapidly than conventional dressings
While maggots should not be regarded as a cure for all types of wounds, by removing dead tissue and any associated bacteria, in most instances they will improve the condition of a wound and allow the process of healing to begin
What is BioBag: Larval Therapy?
BioBag dressing: The maggots are sealed within a dressing which is a finely woven net pouch containing a small piece, or pieces of foam, which aid the growth of the maggot and manage exudate. The BioBag dressings come in varying sizes and are applied according to the nature and size of the wound being treated. The maggots remain sealed within the dressing throughout the treatment.
What is Free Range: Larval Therapy?
The maggots are applied directly onto the wound and retained within a special dressing system. The exact nature of this is determined by the size and location of the area to be treated.
Describe the mechanism of action of Larval Therapy.
Larvae secretion of proteolytic enzymes which liquefy the necrotic tissue
Actual ingestion of the tissue by the larvae
Physical presence of the larvae increasing the exudate from the host which washes out the bacteria
Secretions from the larvae changing the wound pH
Bacteria on the wound being destroyed in the larval alimentary tract due to antibacterial substances
Larval secretions promoting healing
The crawling action of the larvae stimulating granulation tissue
What is the duration of Larval Therapy?
BioBag dressings can be left in place for up to four days—it is possible for the dressing to be removed daily to allow inspection of the wound site
‘Free range’ maggots are generally left in place for up to three days before being removed from the wound site
With both application methods, it is impossible to predict how long a course of treatment will take. Sometimes a wound is completely cleansed by a single application of larvae but other wounds may require two or more treatments to achieve the desired effect.
What are the potential outcomes for Larval Therapy?
The wound may become a little wetter than usual or show the presence of a dark red or pink discharge. This is due to the action of the maggot breaking down the dead tissue
Sometimes a wound that contains a lot of dead tissue will develop a characteristic smell during treatment
Most patients are unaware of the maggots presence, although a small number of patients claim that they can feel the larvae moving but only describe this as a tickling sensation
Some patients, particularly those with poor circulation report that their wounds become more painful during larval therapy but this can generally be controlled with medication.
Some patients have found that the pain associated with infected wounds is reduced following maggot therapy.