Acute Kidney Injury and Chronic Kidney Disease
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
Acute kidney injury
Abrupt decline in GFR à loss of kidney function
Inability to excrete wastes and water, maintain f/e balance, hormone production, RBC production
Azotemia – nitrogenous wastes in the blood
Uremia – urea in the blood
Most common causes are ischemia and exposure to nephrotoxins
Major surgery, sepsis and severe pneumonia
AKA:
Renal dysfunction
Renal insufficiency
Acute renal failure
Associated with a significant increase in morbidity and mortality, LOS, complications and cost
Affects nearly 20% of patients admitted to the hospital
Azotemia
nitrogenous wastes in the blood
Uremia
urea in the blood
Causes of AKI
Prerenal - 55% of cases
Intrarenal - 40% of cases
Postrenal - 5% of cases
Causes of AKI - prerenal
55% of cases
hypoperfusion
Causes of AKI - Intrarenal
40% of cases
Direct damage to the kidney
Causes of AKI - postrenal
5% of cases
Obstruction
Prerenal image - patho note
about 60%
Decreased renal function
ex. renal stenosis, hypotension
Intrarenal image - patho note
about 35%
direct kidney damage - tubular, glomerular, vascular, interstitial
ex. acute tubular necrosis, glomerulonephritis, hemolytic uremic syndrome, tubulointerstitial nephritis
Postrenal image - patho note
about 5%
obstruction to urinary flow
ex. stone, tumor
Causes of AKI - Prerenal
Anything that decreases vascular volume, cardiac output, systemic vascular resistance
Decreases renal blood flow & perfusion
Dehydration, hemorrhage, hypovolemia, renal artery stenosis/occlusion, hypotension, sepsis
Decreased perfusion (Cardiac Output) leads to decreased GFR
Kidney needs 20-25% of cardiac output to maintain GFR
Prerenal AKI can reverse rapidly if blood flow is restored quickly
Unresolved ischemia leads to nephron damage
Causes of AKI - Intrarenal
Direct damage to the kidneys
Nephrotoxins: due to medications injuring kidney tissue
Aminoglycoside Antibiotics: gentamycin, vancomycin, neomycin, tobramycin
Contrast dye*
Acute, high dose exposure to NSAIDS: acetylsalicylic acid (aspirin), ibuprofen, naproxen (causes decreased perfusion)
Acute Glomerulonephritis: due to severe inflammation reducing renal blood flow or prolonged ischemia
Rhabdomyolysis - rapid muscle breakdown - athletes, statins, working out hard, seizures, crushing injuries
Acute pyelonephritis
Acute tubular necrosis (ATN)
severe consequence of prolonged exposure to any of the above
How to know its rhabdomyolysis:
dark urine
creatinine kinase high
myoglobin high (damages the kidneys)
Causes of AKI - intrarenal - nephrotoxins
due to medications injuring kidney tissue
Aminoglycoside Antibiotics: gentamycin, vancomycin, neomycin, tobramycin
Contrast dye* - (nephrotoxic, monitor kidney function - give fluids to flush kidneys, give meds such as steroids to protect the kidneys)
Acute, high dose exposure to NSAIDS: acetylsalicylic acid (aspirin), ibuprofen, naproxen (causes decreased perfusion)
Causes of AKI - intrarenal - nephrotoxins - when to draw a trough
(the low point)
30-60 minutes before
Causes of AKI - intrarenal - nephrotoxins - when to draw a peak
(highest point)
30-60 minutes after COMPLETED administration, get it at its peak in the body (IV)
Causes of AKI - intrarenal - how to protect pts
peak and trough!!
Causes of AKI - postrenal
Obstruction in the urinary tract – Postrenal
Ureteral obstructions – renal calculi, tumors, fibrosis
Bladder neck obstructions – BPH, CA prostate
Urethral obstruction – strictures, tumor
Spinal cord injury – inability to empty bladder
Acute kidney injury - urine volumes
Anuria - less than 100 ml/24 hrs
Oliguria - 100-400 ml/24 hrs
Polyuria - excessive amount of urine in 24 hrs
Phases of acute kidney injury
Initiation phase - from insult to vein
Maintenance phase - Unstable period, severe drop in GFR, metabolic acidosis, neurological: confusion, agitation, lethargy, seizures/coma
Recovery phase - Process of tubular cell repair and regeneration and return of GFR to normal - renal function improves quickly in the first several weeks of this phase and continues up to 1 year
Phases of acute kidney injury - Initiation phase
From insult to injury (hours to days)
Begins with initiating event and ends with tubular injury
If intervene now, can reverse
Often asymptomatic
Phases of acute kidney injury - Maintenance phase
Unstable period, severe drop in GFR
Urine output – usually less than normal
Oliguria – ischemic damage – 66% mortality
Non-oliguria– 25% mortality
Salt/water retention cause
Edema
Hyperkalemia: Impaired potassium secretion (cardiac, neuromuscular function, nausea, diarrhea)
Metabolic acidosis
Anemia
Decreased production of erythropoietin
Neuro: confusion, agitation, lethargy, seizures/coma
Phases of acute kidney injury - Recovery phase
Process of tubular cell repair and regeneration and return of GFR to normal
Diuresis:
Initially, abnormally large amounts of urine excreted as nephrons recover
Tubular function begins to recover
Increased urea and creatinine in the tubules, but not able to concentrate urine yet
This increased diuresis may cause low BP, low fluid volume: Closely monitor!
Renal function improves quickly in the first several weeks of this phase and continues up to 1 year
Detecting AKI
YOU may be the first to recognize the development of AKI!
Recognize risk factors and subtle changes
Healthcare provider will determine type of AKI (pre, intra, post)
heart failure, dehydration, calculi, tumor, use of antibiotics?
Acute Kidney Injury - AKI
Prevention is the goal!
Assess history and risk factors
exposure to toxins, ischemia, meds, surgery, trauma
UTI
Assessment
serum creatinine, BUN, urinary output, BP, pulse strength, edema, crackles, daily weight
Acute Kidney Injury - collaborative care
Maintain adequate hydration and electrolyte balance
Monitor aminoglycoside drug levels
Identify clients at risk and initiate prompt treatment!
Elevated BUN with normal Cr = dehydration
Relieve post-renal obstructions
Correct pre-renal hypovolemia
Increase CO when inadequate
Restore renal perfusion
Renal dose dopamine
AKI treatment:
Fluid/electrolyte balance
Fluid Restrictions?
Treat elevated electrolyte levels!
Careful diuresis (furosemide or other loop diuretic)
Newest recommendation is to limit use
Fluid challenge?
Hyperkalemia Treatment
K-cocktail (D50 and insulin-R IV), sodium polystyrene sulfonate, sodium bicarbonate
Decreases potassium levels in blood
Binds to extra potassium in GI tract so it cannot be absorbed into the blood
Calcium gluconate
Stabilizes cardiac cell membranes

Hyperkalemia Treatment - early symptoms
Peaked T waves

Hyperkalemia Treatment - late symptoms
Prolonged PR, loss of PR, wide QRS, bradycardia, vfib or asystole
AKI treatment cont.
Maintain glycemic control
Elevated BG increases risk for infection, Multisystem Organ Dysfunction (MODS)
Hyperglycemic nephropathy
Dialysis or CRRT? (Continuous Renal Replacement Therapy)
Ongoing monitoring
Nephrologist
Skin care
Daily weight
Dietary restrictions
Chronic kidney disease (CKD)
Progressive reduction of functioning nephrons
A chronic problem!
Irreversible
Destroyed nephrons replaced by scar tissue
Results in uremia and azotemia
CKD causes:
Diabetes: leading cause of ESRD
Hypertension: closely follows diabetes
Chronic glomerulonephritis
Chronic pyelonephritis
Polycystic kidney disease
Systemic lupus erythematosus
CKD patho
deterioration of nephrons
GFR falls
BUN/ creatinine rises
Urine creatinine clearance decreases
Increased glomerular capillary pressure damages capillaries which leads to sclerosis
CKD stages - stage 1
GFR normal
GFR - > 90 mL/min
BUN and Cr still normal
Asymptomatic
Normal kidney function as long as no stressors
CKD stages - stage 2
GFR mildly decreased
GFR – 60-89 mL/min
Mild hypertension
CKD stages - stage 3 (when its noticed usually)
GFR 30-59 mL/min
Moderate decrease in GFR
HTN, anemia & fatigue, mild edema
BUN and serum creatinine elevated
CKD stages - stage 4
GFR 15-29 mL/min
Severely decreased GFR
Kidneys can no longer maintain homeostasis
HTN, anemia & fatigue, malnutrition, edema, metabolic acidosis
BUN and serum creatinine continue to elevate
CKD stages - stage 5
GFR <15 mL/min
ESRD
Altered fluid/electrolyte balance
Accumulated metabolic waste affects every system of body
If left untreated, will die
Fluid/electrolyte problems
Cardiac arrhythmias, pulmonary edema, cerebral edema, death
Need dialysis or transplant
CKD S&S:
Affects all body systems!
Fluid/Electrolyte/Acid-Base Balance
Cardiovascular Effects
Hematologic Effects
Immune System Effects
Gastrointestinal Effects
Neurologic Effects
Musculoskeletal Effects
Endocrine and Metabolic Effects
Dermatologic Effects
CKD - collaborative care
***Preserve renal function, delay need for dialysis and decrease risk of cardiovascular death!
Control underlying disease
CKD - collaborative care - BP control
Utilization of ACE and/or ARB
ACE has kidney protective qualities and decreases proteinuria
CKD - collaborative care - Diabetic clients
Keep HbA1C < 7
CKD - collaborative care - SGLT2 inhibitors
empagliflozin, dapagliflozin
Blocks reabsorption of glucose and sodium to increase glucose excretion and reduce preload and afterload
Reduces risk of heart attack and stroke in CKD
Slows CKD progression
CKD - collaborative care - Mineralocorticoid receptor (MR) antagonist:
finerenone
Slows CKD progression with DM II, decreases risk of cardiac death
Potent like spironolactone without risk of hyperkalemia
CKD - collaborative care - GLP1 receptor agonists:
semaglutide, tirzepatide
Improve blood sugar control, reduce renal inflammation, slow disease, reduce risk for MI and stroke
CKD - collaborative care - symptom control
Accumulation of nitrogenous waste/Fluid Excess
Monitor cardiac & respiratory systems
Diet – low protein, low sodium, low potassium, low phosphorous
Avoid nephrotoxins
Fluid restriction?
Strict I&O
Daily weight
Continue active lifestyle as long as possible
Walking, swimming, stretching
CKD additional meds:
Diuretics
Phosphate binders: sevelamer
Supplemental vit D
Vitamins and minerals
Sodium bicarb
Erythropoietin (epoetin alpha)
CKD additional meds - diuretics:
Fluid volume excess prior to dialysis dependence
*Selection and safety based on electrolyte levels
CKD additional meds - Phosphate binders:
sevelamer
Bind to and excrete phosphate
CKD additional meds - Supplemental Vitamin D
Prevent osteodystrophy
CKD additional meds - vitamins and minerals
nephrocaps-water soluble vitamins for renal disease
CKD additional meds - sodium bicarbonate
tablets or infusions
correct metabolic acidosis
CKD additional meds - erythropoietin
(epoetin alpha)
Decreased production by kidneys
Stimulate bone marrow production of RBC
CKD - Hemodialysis
An artificial kidney designed to provide controllable transfer of solutes and water across a semi permeable membrane - (dialysis of the blood) (3-4 hrs, 3 days a week)
Uses principles of
Diffusion – movement of solutes from greater to lesser concentration
Osmosis – movement of fluid from lesser to greater concentration of solutes
Ultrafiltration – water and fluid removal across a pressure gradient
CKD - Hemodialysis - what solution is used and why
Dialysate
Varying amounts of sodium, calcium, magnesium, bicarb, chloride
Based on patient’s labs
To promote fluid and solute transfer
CKD - Hemodialysis - acute indications
•AKI refractory to treatment - (refractory = not responding)
•Hyperkalemia with AKI
•Fluid overload not responding to diuretics
•Metabolic acidosis
•Drug overdoses (lithium, ethylene glycol)
CKD - Hemodialysis - chronic indications
•CKD Stage 5- End-Stage Renal Disease
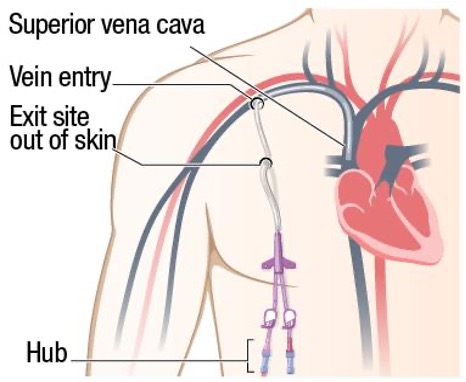
CKD - dialysis catheter - vascular access
temporary!!!
Subclavian, IJ or femoral vein
Typically, short-term
AKI - CKD if waiting for fistula/graft to mature!!
Dual lumen
Waiting for fistula or graft to mature
Ineligible for AV fistula/graft
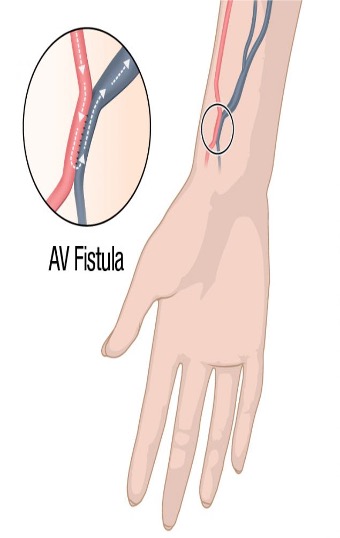
CKD - arteriovenous fistula - vascular access
Artificial connection between the vein and the artery
Takes about 4 weeks to mature
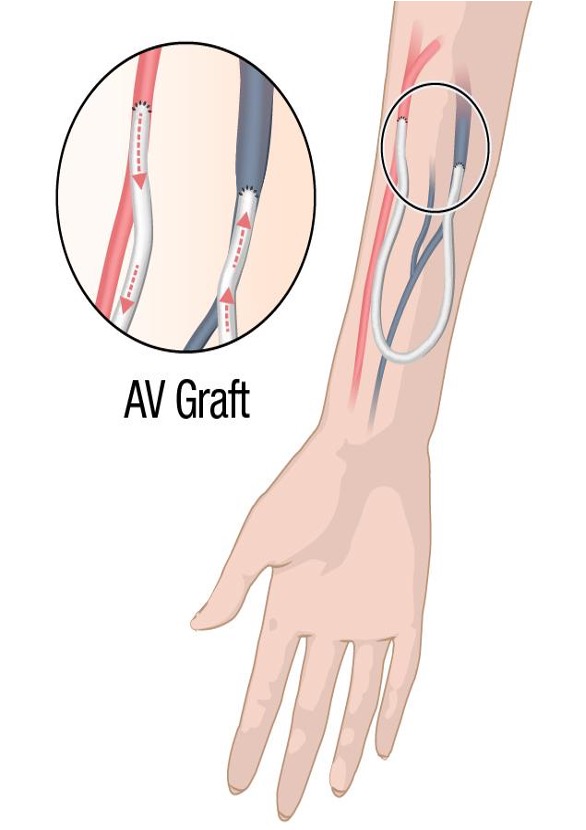
CKD - arteriovenous graft - vascular access
surgical procedure
Access created by putting a tube in to connect the artery and the vein
Higher risk for infection
Can use in about 2 weeks
CKD - vascular access complications
Loss of vascular access
Infection
Inadequate blood flow
Bleeding
CKD - venous access nursing care - grafts and fistulas
Assess for thrill and bruit
No BP or venipuncture in limb with device
CKD - grafts and fistulas - what is a thrill
is a palpable, vibratory sensation felt with the hands
feel the thrill!!!
CKD - grafts and fistulas - what is a bruit
is an audible, whooshing sound heard through the bell of a stethoscope
do you hear the brat!!
CKD - venous access nursing care - Early identification of thrombus
Embolectomy
Angioplasty
Thrombolysis
CKD - venous access nursing care - education
No constrictive clothing
Do not sleep on arm
CKD - peritoneal dialysis
utilizes the peritoneum rather than the pts blood
not as efficient
Uses peritoneal membrane as the dialyzer
Catheter is placed into peritoneal cavity
Dialysate instilled via catheter
Dialysate is then drained by gravity in to “collection” bag
CKD - peritoneal dialysis - dwell time
waste and electrolytes move into dialysate from highly vascular peritoneum
CKD - peritoneal dialysis - what often happens?
Hypotension!! - removal of fluids! - always have more fluid going out rather than going in!!
air embolism - air through peritoneal catheter possible
CKD - peritoneal dialysis - problems
Not as efficient
Inability to correct fluid or electrolyte problems quickly
Respiratory difficulty
Infection
Peritonitis
Occlusion of catheter from fibrin deposits
Hypotension
Air embolism
Hemorrhage
CKD - peritoneal dialysis - care and assessment
Catheter site
Drained dialysate (COCA)
CKD - peritoneal dialysis - advantages
Can be done at home
More "normalcy"
CKD - dialysis complications
hypotension!!! - number one!!
bleeding
infection
dysrhythmias - shifting fluid and electrolytes in a short time span
CKD - what to think about for a pt getting dialysis that day
Hold BP meds - beta blockers, ACE - worried about hypotension as is - don’t want it to be dialyzed out
Hold antibiotics - will be dialyzed out
Hold anti seizure meds - will also be dialyzed out
CKD - Continous renal replacement therapy - CRRT
Similar to intermittent hemodialysis but done constantly
Useful in AKI and patients who are hemodynamically unstable
Continuously and slowly removes fluid and solutes
Usually short term use (AKI)
Process of ultrafiltration
very slow removal of blood, fluid and solutes
nurses manage machine and monitor effluent removal
CKD - renal transplant
high success rates
original kidney left in place
lifelong immunosuppressants
new kidney placed in iliac space
donors - live or deceased
(donating is more dangerous than receiving) (wait time is over 5 yrs in OH)