cardiovascular function
1/214
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
215 Terms
normal endothelium
smooth
very tight junctions in between individual cells
how can endothelium be damaged
smoking
mechanical stress caused by HTN
elevated LDL
mechanisms of the immune system
where do athlerosclerotic lesions form
where vessels branch or in areas of turbulent blood flow
what is the meaning of turbulent blood flow contributing to atherosclerosis
suggests that hemodynamic factors play a role in endothelial injury
when endothelium is damaged or LDL is high
monocytes become stick
attach themselves to the endothelium in response to adhesion molecules
result of monocytes sticking to endothelium
endothelium loses some of its ability to produce antithrombotic and vasodilating cytokines
monocyte emigration
an early response to endothelial injury
the movement of monocytes into the intimal layer of the endothelium squeezing through cell junctions
after monocyte emigrates to intimal layer
continue emigration into subendothelial space
monocytes are transformed into macrophages
free radicals released
what do the monocytes turn into
macrophages
what do macrophage do in atherosclerosis
consume the oxidized LDL and form foam cells
foam cells
release growth factors, inflammatory cytokines that worsen endothelial injury and further the process of atherogenesis
LDL oxidation
LDL make their way through the intact endothelium and are quickly oxidized into proinflammatory lipids
oxidized LDLs act as an attractant to monocytes in the endothelium causing further migration
smooth muscle proliferation
when the platelets in the blood are exposed to the subendothelium, they adhere to the site of injury
followed by proliferation of smooth muscle
causing endothelial layer to pouch out making the lumen of the vessel smaller
formation of fatty streak
Think, flat, yellowing discolourations that enlarge over time occluding the vessel lumen
what is the fatty streak made from
macrophages and smooth muscle cells that are distended with no lipid to form foam cells
formation of lipid core
Lipids accumulate beneath the endothelial layer and form a hard lipid core
The atherosclerotic plaque becomes vulnerable to rupture as enzymes eat away at the protective fibrous cap
plaque hemorrhage
Prothrombogenic mediators are released as the plaque begins to fissure or rupture
Platelets floating by adhere to the lesion with the help of procoagulant factors and a thrombus is formed
Blood flow to the coronary artery and myocardium can be compromised leading to infarction
steps/sequence of atherosclerosis
endothelial cell injury
monocyte emigration
LDL oxidation
smooth muscle proliferation
formation of fatty streak
formation of lipid core
plaque hemorrhage
more causes of endothelial injury
HTN
smoking
hyperlipidemia
hyperhomocysteinemia
hemodynamic factors
toxins
immune reactions
myocardial ischemia
restriction of blood supply that results from an imbalance between myocardial oxygen supply and demand
factors in oxygen supply and demand from the heart
coronary vessel patency
ventricular wall compression
diastolic filling time (heart rate)
myocardial contractility
heart rate
wall stress (preload, afterload)
diastole
the portion of the cardiac cycle when the ventricle is in a relaxed state, stretching as it fills with blood from the atrium
what is oxygen supply regulated by
the patency or size of the lumen of the coronary vessel
The ability of the ventricular wall to compress
The amount of time the ventricle spends in diastole
what is oxygen demand dependent on
Myocardial contractility
Heart rate
Vascular wall stress
preload and afterload
what if preload or afterload is too high or low?
added stress to the heart → higher oxygen demand
in normal heart how is increased demand of oxygen met?
increasing supply of oxygen
*may not occur in non healthy heart
supply ischemia
an abrupt or acute reduction in blood flow to the myocardium caused by thrombus, coronary vasospasm or platelet aggregation
demand ischemia
an increase in need for oxygen and nutrients due to exercise or stress
what happens in coronary artery disease with oxygen supply and demand
With coronary artery disease increased demand causes an imbalance
potential outcomes of cell injury
reversible injury, cell recovery, and return to normal function
apoptosis and programmed cell removal
cell death and necrosis
common causes of ischemia
Blockage or coronary artery, thrombus
Spasm of coronary artery
Coronary artery obstruction (formation of plaque)
cellular effects of ischemia
inadequate supply of oxygen and nutrients
accumulation of waste
inadequate
how long does it take for myocardial cells to become ischemic and decrease contractility
within 10 seconds of blood flow being interrupted adn contractility is depresses within minutes
how long for ischemia to progress into necrosis
20 minutes if blood flow is not resolved
what happens when oxygen not available
shift to anaerobic processes
only 2 ATP molecules and lots of pyruvic and lactic acids which are toxic to our cells
why is it bad to have anaerobic metabolism
without ATP our NaK pump becomes inefficient and electrical impulses in the heart and nervous system become uncoordinated, which can lead to dysrhythmias
what happens in accumulation of waste
Inflammatory mediators are released
Granulocyte activation
Free radical accumulation
what is the result of inadequate supply and accumulation of waste
Alteration of cell membrane
Cell edema
Arrhythmias
Cell death
Failure of contraction
hemodynamic effects of ischemia
reduced contractility
abnormal wall motion and changes in compliance
decreased cardiac output
reduced ventricles emptying
compensatory stimulation of the SNS
why is there reduced contractility with ischemia
the larger the area of ischemia, injury or infarct, the less ventricular muscle available to contract
abnormal wall motion and changes in compliance in ischemia
hypokinesis or akinesis
leads to ventricular walls losing their elasticity so they can no longer stretch to accomodate incoming volume
hypokinesis
poor contraction of the heart
akinesis
full loss of ability of heart to contract
what is decreased cardiac output in ischemia a result of
low stroke volume
when is there reduced ventricle emptying in ischemia
at the end of systole
how are compensatory stimulation of the SNS happen when there is ischemia
senses a drop in cardiac output
initiates increased HR and BP to compensate
what is acute coronary syndrome
Spectrum of ischemia diseases
A continuum that begins with plaque rupture within a coronary artery and results in infarction of myocardial tissue if perfusion is not restored
3 phases of acute coronary syndrome
unstable angina
NSTEMI
STEMI
process of acute coronary syndrome
normal artery and vessel wall
asymptomatic
stable angina
unstable angina
thrombus
acute STEMI
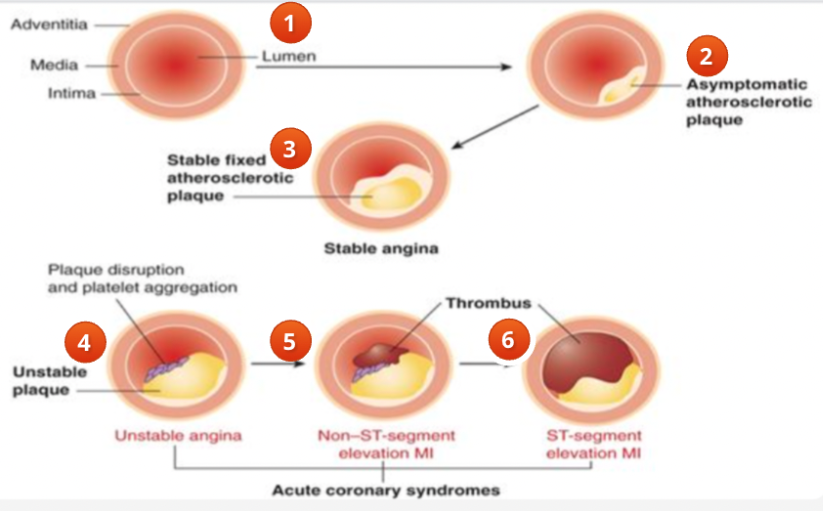
what happens in a normal artery and vessel wall
blood flows easily through the vessel
asymptomatic acute coronary syndrome
some development of atherosclerosis
because the lumen in not significantly narrowed the blood flows through providing enough oxygenated blood to prevent symptoms
stable angina
lumen has significant amount of narrowing from plaque
patient will have some symptoms when demand for oxygenated blood increases
unstable angina
atherosclerotic plaque has been disrupted and platelets travelling by begin to stick to it
the plaque is unstable or vulnerable
patient develops symptoms without warning and is not able to control symptoms with medications and rest
thrombus/NSTEMI
plaque has ruptured with hemorrhage
the lumen becomes even more occluded with clot and the patient suffers some infarction to a part of the myocardium
because the damage does not involve the full thickness of the ventricle the patient has suffered a “non ST elevated MI” or NSTEMI
acute STEMI
the clot continues to build and the entire lumen is occluded
the myocardium suffers significant infarct and changes on ECG are notes
normal ECG deflections
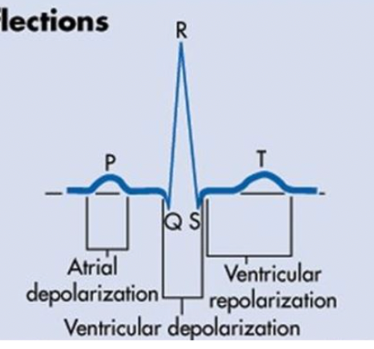
what is the relationship of the ST wave
between S and T wave
what does ST segment represent
end of ventricular depolarization and beginning or repolarization
how should ST segment look
flat on ECG
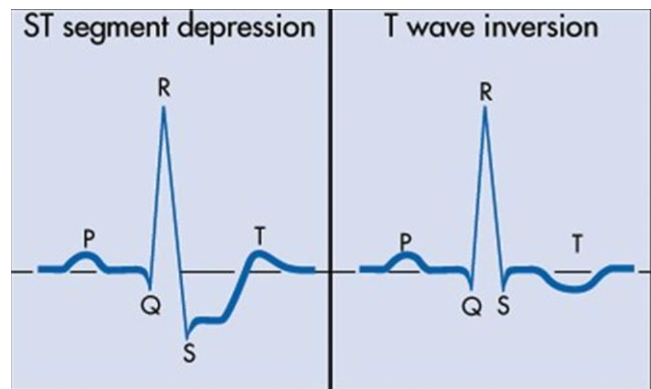
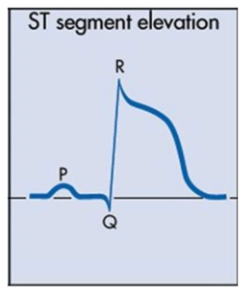
what finding is concerning of ST segment
elevation or depression of 1 mm or more
unstable angina
Atherosclerotic plaque disruption exposing injured endothelium to platelets and coagulant factors leading to clot formation
Leads the transient episodes of vessel occlusion at the site of plaque disruption
Thrombus is labile and vulnerable but perfusion is restored before necrosis can occur
Can occur at rest
Pain is persistent and severe
Difficult to relieve
what are common findings for the ST segment during unstable angina
ST segment depression
T wave inversion
when are the ST changes in unstable angina found
during pain
labs in unstable angina
cardiac enzymes:
creatinine kinase
lactic dehydrogenase
troponin
all negative
contractility during unstable angina
may be abnormal
what is an NSTEMI
Necrosis of myocardial tissue occurs but does not involve full thickness of the ventricular wall (inner ½-⅓ of ventricular wall)
Necrosis is limited to subendocardial area
NSTEMI ECG changes
ST-segment depression
T-wave inversion
NSTEMI patient experience
severe abrupt pain and no relief
NSTEMI diagnosis
history
pain
biomarkers
increased myocardial enzymes creatinine kinase and troponin
what is creatinine kinase
enzyme found in heart, brain, and muscle adn is released when the cells are damaged
creatinine kinase isoenzymes
CK-BB
CK-MB (myocardial muscle)
CK-MB levels of infarction
levels rise 3-6 hours post infarction
peak in 12-24 hr
return to normal after 12-48 hours
CK-MB normal value
0-4% of total CK
troponin
protein found in skeletal and cardiac muscle
troponin levels in MI
with MI troponin-T and troponin-I levels rise very quickly
rise in 6-10 hours
peak at 18-24 hours
falls at 5-6 days
downfalls of troponin
prolonged period for diagnosis
preferred biomarker for MI diagnosis
troponin, specifically Troponin I because it is the most specific
what is occuring in a STEMI
arterial occlusion is complete resulting in necrosis of full thickness of the ventricle altering electrical condition
symptoms of STEMI
pain is abrupt with no relief
ECG changes in STEMI
ST elevation
cardiac biomarkers for STEMI
elevated
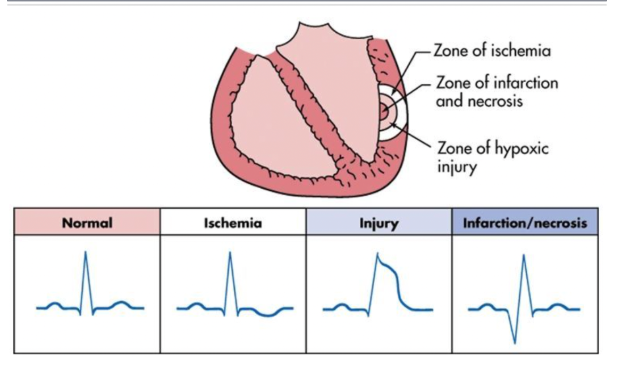
zones of tissue damage during infarction
zone of infarction (inner most)
zone of injury
zone of ischemia (outer most)
zone of infarction
Cell death and necrosis had occurred
Seen as pathological Q waves on ECG
Cells replaced with scar tissue
zone of injury
Blood flow is interrupted causing injury but potential viable tissue surrounding area of infarct
Seen as ST segment elevation on ECG
zone of ischemia
Perfusion to area decreased but no damage occurs as long as blood flow is restored
Outer region of infarcted area
Cells still viable
Manifest as T wave inversion on ECG
worst care scenario of impaired muscle perfusion
myocardial infarction
what happens to overcome ischemia
new blood vessels form through angiogenesis to form a detour around the blockage
these are to bypass the occlusion restoring blood flow to tissue (collateral circulation)
some people with collateral circulation never know they have significant heart disease
what happens if reperfusion is not obtained
necrosis of full ventricle can occur
necrotic cells can never participate in contraction so the ventricle is either hypokinetic or akinetic- some ventricular function si then lost
pathological process of myocardial infarction
once an infarct has occurred the area becomes bruised and cyanotic and cardiac enzymes are released from the damaged cells
infiltrates by neutrophils and cytokines and complement and coagulation cascades begins
inflammation and angiogenesis occur
ventricular remodelling due to inflammation and angiogenesis
inflammation → recruitment of stem cells which differentiate into endothelium leading to regeneration of myocardial tissue
catecholamines are released
coronary vasoconstriction occurs in the area of the infarct along with embolization of thrombi
location of infarct depends on vessels involved
purpose of catecholamine release
neurotransmitters increase blood glucose for energy
purpose of coronary vasoconstriction
death of myocytes may stimulate production of toxic free radicals that further plug coronary capillaries decreasing blood flow
possible locations of MI
right coronary artery
left anterior descending artery
left circumflex artery
*knowing helps to determine what clinical manifestations we might see
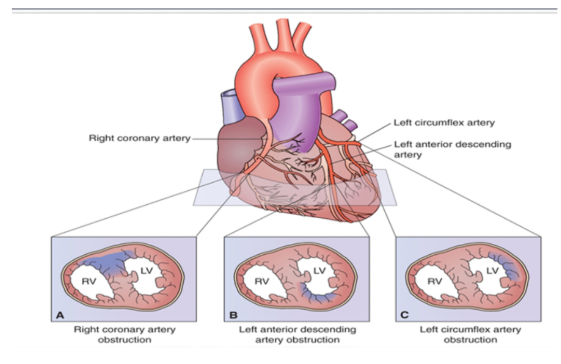
right coronary artery MI
supplies right ventricle
occlusion of this artery causes right ventricular infarct
left anterior descending artery MI
supplies anterior portion of the left ventricle
left circumflex artery MI
supplies the lateral part of the left ventricle
ECG changes at the zones of MI
Ischemia and non stemi: flipped or inverted T wave
Transmural MI: elevated ST segment
Infarction: pathological Q wave
how do some people find out they had an infarction
symptomatic is a possibility
accidentally discover at routine checkup
pathological Q wave persists forever on ECG
clinical presentation of symptomatic MI/CAD
pain (may radiate)
pallor, dyspnea, anxiety, diaphoresis
dysrhythmias
nausea and vomiting
denial of infarct
cause of pain
from lactic acid during ischemic episode or by myocardial stretching irritating nerve fibres
cause of pallor, dyspnea, anxiety, diaphoresis
From catecholamines diverting blood flow to priority areas