LAB 14 - Glucose
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
The use of jelly beans for glucose tolerance tests is used for?
Research showed jellybeans are just as effective at raising blood glucose levels as the standard glucose drink given to pregnant women getting tested for gestational diabetes mellitus. It reduced side effects, such as nausea, and made calculations easier.
Jelly bean calculation
Simple because a jelly bean consists only of simple carbohydrates and flavoring. Since each bean equals 4 calories for 1 gram and a carbohydrate equals 4 calories for one gram, then 80g = 80 beans
What is the GTT? How did we do it in class?
GTT is a diagnostic tool used to measure the body’s ability to regulate high loads of glucose over time. In class the procedure began with measuring a “fasting” blood glucose (T0). Participants then ate 80 grams of sugar, administered as 80 jelly beans to be consumed within 5 minutes. Blood glucose levels where then measured every 30 minutes for up to three hours.
How are blood glucose levels controlled?
BG levels are homeostatically regulated variables controlled by antagonistic actions between insulin and glucagon, produced by the Islets of Langerhans. BG levels are kept within the “set point,” the narrow and normal range between 70-99mg/dL fasting blood glucose
What is insulin? What is it secreted by and what increases/decreases its secretions?
Insulin is the hormone of abundance, secreted by the beta cells of the Islets of Langerhans. An increase in plasma glucose levels and parasympathetic activity increases the secretion of insulin, while sympathetic activity decreases.
What is glucagon? What is it secreted by, and what increases/decreases its secretions?
Glucagon dominates during fasting, it is secreted by the alpha cells of the Islets of Langerhans. A decrease in plasma glucose levels and an increase in sympathetic activity, increases the secretion of glucagon.
Target tissues of insulin and physiological response
Insulin targets the liver, skeletal muscle, and adipose. Insulin does NOT target the brain, kidney, or intestines.
Physiological responses it increases
glycolysis (glucose oxidation): phosphorylating glucose to make ATP
glycogenesis: generation of glycogen in muscle and liver
lipogenesis: formation of triglycerides using cellular respiration
protein synthesis: excess of energy to make protein
Target tissues of glucagon and physiological response
Glucagon only targets the liver because its where glycogen is stored and available because skeletal muscle always needs a fast source of glucose.
Physiological responses:
Increases glycogenolysis
Increase gluconeogenesis
glucogenic amino acids, glycerol, pyruvate, lactat
What is the normal response in GTT?
Start (T0): Fasting BG will be below 100mg/dL
Peak: BG peaks at about 30-60 minutes, typically 30
End: BG declines and returns to normal before the three hour mark (x<100)
What is a prediabetic response in GTT?
Start: fasting BG begins between 100-125/6mg/dL
Peak: BG peaks between 30 to 90 minutes, typically 60 minutes
End: BG declines slowly and will not return to fasting conditions
What is a diabetic response in GTT?
Start: Fasting BG starts at 126 mg/dL
Peak: BG peaks at 90 minutes or later
End: BG remains high and stays high as it has a very slow return
Fasting BG Diagnosis: 69mg/dL and below is? What are the causes and symptoms?
hypoglycemia “low glucose in the blood”
Hypoglycemia is not very common, it’s mainly caused because a diabetic patient over injected themselves with insulin. The second cause, which is uncommon is when a person has to little glucagon. The symptoms of hypoglycemia is dizziness and fainting because the brain only runs on glucose
Fasting BG Diagnosis: 70-99mg/dL
normal fasting blood glucose levels
Fasting BG Diagnosis: 100 -125 mg/dL
Prediabetic, originally called “impaired glucose tolerance” was renamed to warn people that they are on the path to develop diabetes
Fasting BG Diagnosis: 126 mg/dL and above
Diabetes mellitus
What are the causes of diabetes mellitus?
1) is the inability of beta cells to produce insulin
2) insensitivity of insulin receptors on the cell. In this case insulin is produced but the cells cannot respond
What are the symptoms of diabetes mellitus?
hyperglycemia, glucosuria, polyuria, polydipsea, dehydration, polyphagia, and increase in lipid and protein metabolism
DM: Hyperglycemia
“High glucose in the blood”
DM: Glucosuria
“glucose in urine”
Occurs when glucose carriers in the proximal convoluted tubule of the nephron are saturated and reach their transport maximum
Nephron
afferent
glomerulus
efferent
fenestrations → filtrate journey
afferent arteriole brings blood to the glomerulus under BP
glomerulus: capillary with fenestrations
efferent arteriole takes blood away from the glomerulus
Anything that fits through the fenestrations is filtered into the glomerular capsule as filtrate which continues into the PCT → descending + ascending limbs of the Loop of Henle → DCT → collecting duct
DM: Glucosuria, what happens in the proximal convoluted tubule?
Anything that fits through the fenestrations of the glomerulus will enter the glomerular capsule as filtrate, and the composition will be the same as the plasma in the blood. In the PCT is where we mostly have reabsorption and the ONLY place where glucose is reabsorbed as its where the simple cuboidal epithelial cells for glucose are located.
In a person with normal blood glucose levels, the normal amount of carriers will move glucose back into the blood. Since carriers are used in which glucose has to bind, they are subjected to three things: specificity, competition, and saturation. If there is too much glucose in the blood the transport maximum will be reached and glucose will begin to spill into the loop of Henle → DCT → and into the collecting duct as urine.
Secondary Active Transport: Na+ - glucose transporter
moving glucose from the filtrate into the blood, you go against the CG by using secondary AT
Na+ has a concentration gradient because primary active transport maintains it by pumping out Na+ out of the cell. Causing the high concentration outside and low inside
1) glucose in the lumen is low, Na+ is high We use the concentration gradient of Na+ to rush into the cell and glucose “piggy backs.”
this is secondary active transport through a symporter protein
2) glucose is now inside the cell here it can diffuse from high to low into the blood through carrier mediated diffusion
3) Na+ is also inside the cell. Is removed by ATPase, 3 Na+ out and 2 K+ in, to maintain the concentrations
primary active transport
K+ leaking channels restore K+ levels
DM: Polyuria
“many pee”
Water follows solutes. Urine volume increases as glucose pulls water with it as it spills out of the PCT
Polyuria is one of the first signs of diabetes especially in children due to the excessive need to pee.
DM: Polydipsea
“many thirst”
increase in thirst as the person is experiencing polyuria
DM: Dehydration
increases the blood viscosity, as plasma decreases but the formed elements stay the same, leading to poor circulation
DM: Polyphagia
“many eat”
As there is no insulin signaling to cells to uptake glucose in the blood, the cells begin to starve for energy. Because the cells are starving they signal to you to eat more even though there is high levels of glucose in the blood
DM: Lipid and Protein Metabolism
Increase in lipid and protein metabolism increase the production of keto acids which can lead to ketoacidosis, an acidic blood pH which can lead to the denaturing of proteins
What types of diabetes mellitus did we discuss?
Type I, Type II, Gestational, and Emerging diabetes
Type I diabetes
“Juvenile onset”
an autoimmune disease in which the immune system recognizes beta cells as foreign and destroys them, leading to a complete lack of insulin production. It accounts for 10% if US diabetics and is treated with synthetic insulin
Type II diabetes
“Adult onset”
Accounts for 90% of US diabetes due to cells reduction in sensitivity to insulin, and decreased production of insulin by beta cells
Type II diabetes decrease in insulin production and down regulation of cells
Eating sugary snacks (simple sugars) spikes glucose levels as they are absorbed faster. When BG spikes so does the production of Insulin, signaling to cells to uptake glucose. When these pathways are overstimulated cells downregulate, desensitizing themselves so BG levels will not be brought down as fast
DM: Type II causes and treatment
Causes are excessive visceral fat, advancing in age, and some may be more genetically predisposed to Type II. Treatments are simple but not easy: exercise and dietary changes. Additional treatments can be bariatric surgery (stapling the stomach) and Metformin, a drug that inhibits glucose output by blocking gluconeogenesis.
Gestational diabetes: How it it diagnosed? Why does it develop?
“pregnancy onset”
Gestational diabetes affects 1 to 5% of pregnancies and is often diagnosed by the GTT. why it develops is due to placental hormones increasing blood sugar levels by decreasing insulin sensitivity for the growing fetus. Secondly due to the mothers increased body weight cells also increase in size, but still have the same number of receptors, a greater surface area and a smaller receptor density, decreasing the cells sensitivity to insulin.
Gestational diabetes: What are the effects? What may happen after pregnancy?
Due to gestational diabetes there is more sugar and calories, resulting in a larger fetus. Increase in fetus size, above normal, increases morbidity (increase in probability of disease in newborns) and mortality. Additionally there is a link that the baby may develop Type II diabetes later in life.
Gestational diabetes: What may happen after pregnancy?
After pregnancy gestational diabetes may go away but not always. There is a correlation with the development of gestational diabetes and increased risk in developing Type II diabetes (20-50%), but researchers are unsure which causes which. Whether is be the mother was predisposed to Type II before or if gestational diabetes causes the risk.
What is emerging diabetes?
various types of diabetic forms not seen before such as an increase in diabetes in children and young adults
Comparisons between Type I, Type II, and Gestational Diabetes
Elevated BG
Insulin dysfunction
Shared symptoms
Long-term risks
1) all three types are forms of diabetes mellitus, characterized by hyperglycemia
2) each type involves a failure in the insulin pathway, whether it is a total lack of hormone or a decreased response to it
3) When unregulated all types can lead to symptoms such as glucosuria, polyuria, and polydipsia
4) Gestational and type II diabetes are linked, as women who have gestational diabetes have an increased risk (20-50%) of developing type II diabetes later in life
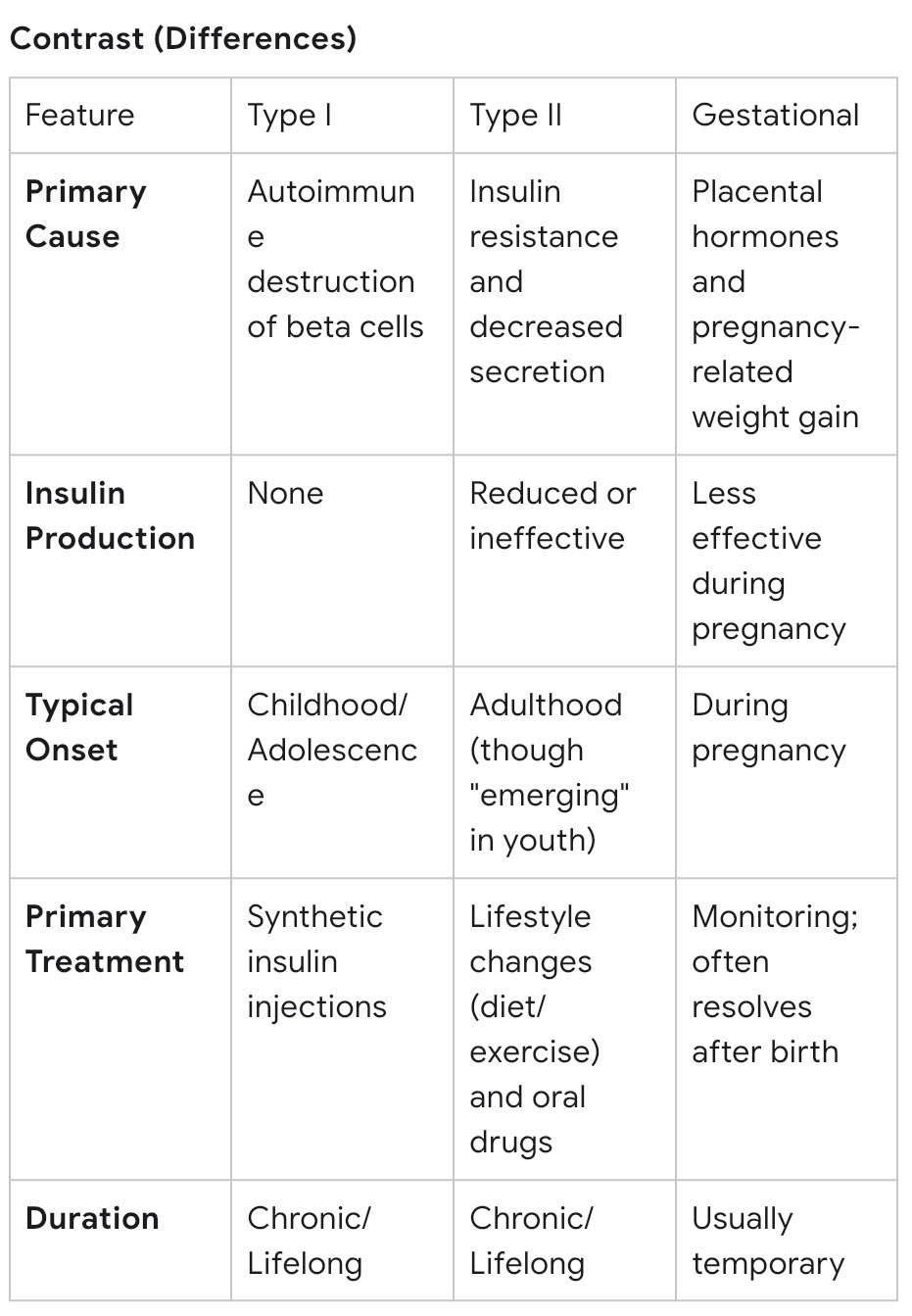
Contrasts between Type I, Type II, and Gestational Diabetes
primary cause
insulin production
typical onset
primary treatment
duration