3017 Patho Exam 3 (Renal System, Endocrine System)
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
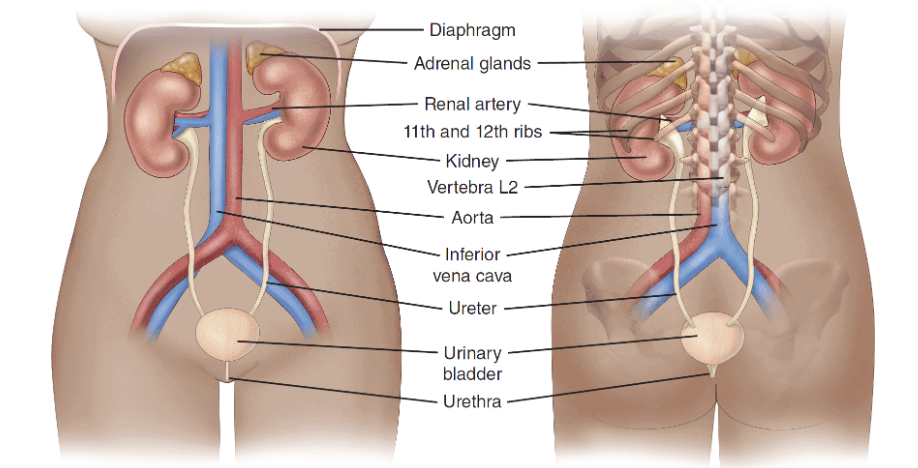
Renal and Urinary Systems Anatomy Review
Structures:
■ Kidneys
■ Ureters
■ Bladder
■ Urethra
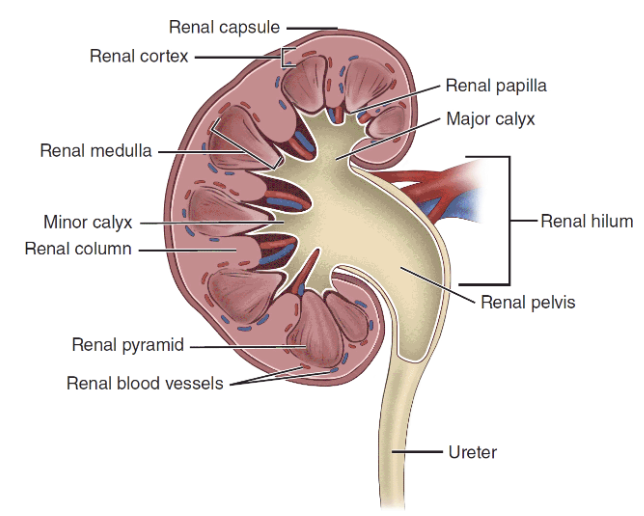
Internal Structure of Kidney and Blood Supply
Renal Capsule: outermost layer of kidney → protect kidney
Renal Cortex: directly beneath renal capsule
Medulla: innermost layer kidney, composed of multiple pyramids
Pyramid : separated by renal columns
Papillae: narrow tips of renal pyramids → empty urine to calyx
Calyx: larger collection sac → empty urine into renal pelvis
Renal Pelvis: store small amount of urine → empty urine to ureter → bladder
Functions of the Kidney
1) urine formation and excretion of wastes
2) regulation of fluid and electrolyte balance and acid–base balance
3) hormonal functions: regulate blood pressure, regulate RBC production, activation of vitamin D, production and release of bradykinin and prostaglandins (PGs).
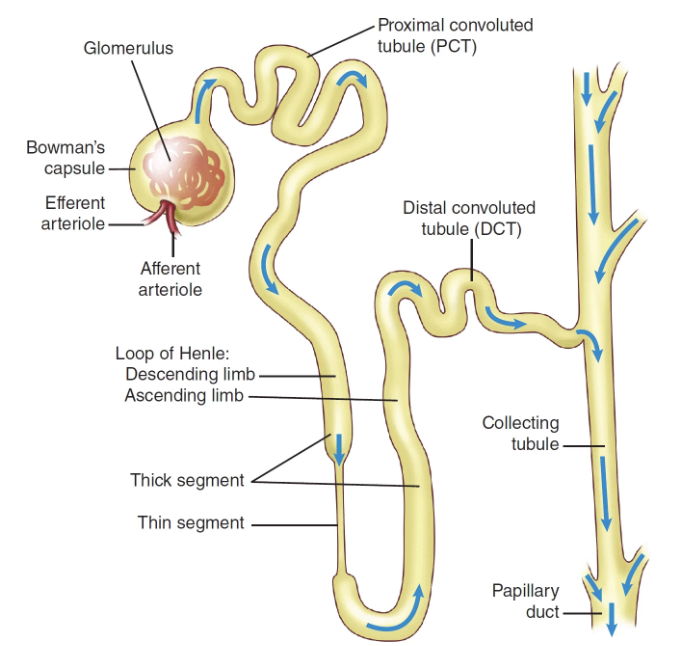
Anatomy of a Nephron
Nephron: filter blood to remove wastes and produce urine
Each nephron has:
Glomerulus: collection of capillaries → filter blood
Bowman’s capsule: structure surrounding each glomerulus
Tubular system include:
→ Proximal convoluted tubule (PCT)
→ Loop of Henle: reabsorb different substances in urine formation
→ Distal convoluted tubules (DCTs)
→ Collecting tubule
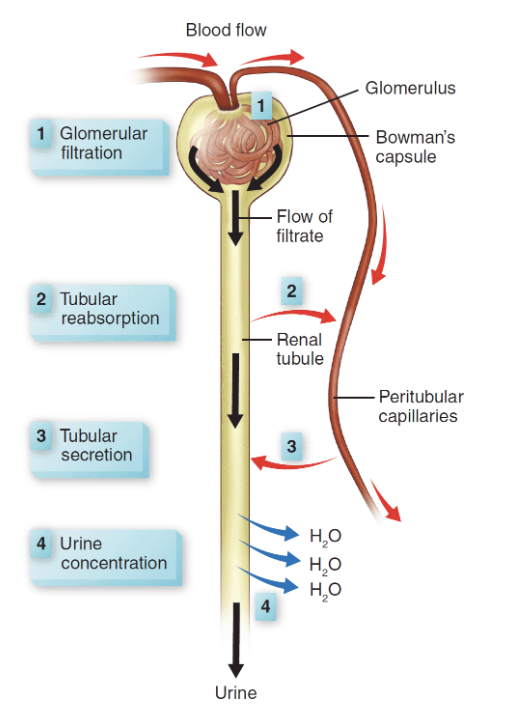
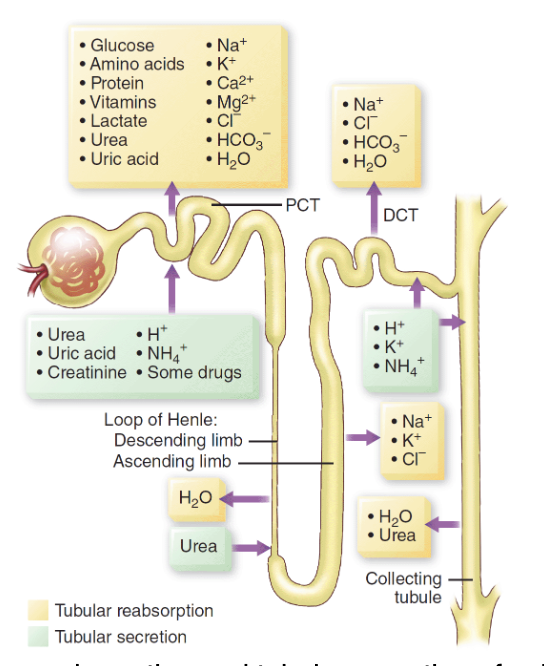
Urine Formation
Urine is formed through the continuous processes of:
Filtration (Glomerulus filter blood = don’t allow RBC and protein to pass through membrane) → force electrolytes, glucose, water across membrane into Bowman’s capsule → then into PCT
Reabsorption (PCT & DCT reabsorb water and solutes back into blood; ADH and aldosterone control permeability of the DCT membrane)
Secretion (solutes move from blood to filtrate)
Concentration (Loop of Henle reabsorbs additional water to concentrate urine)
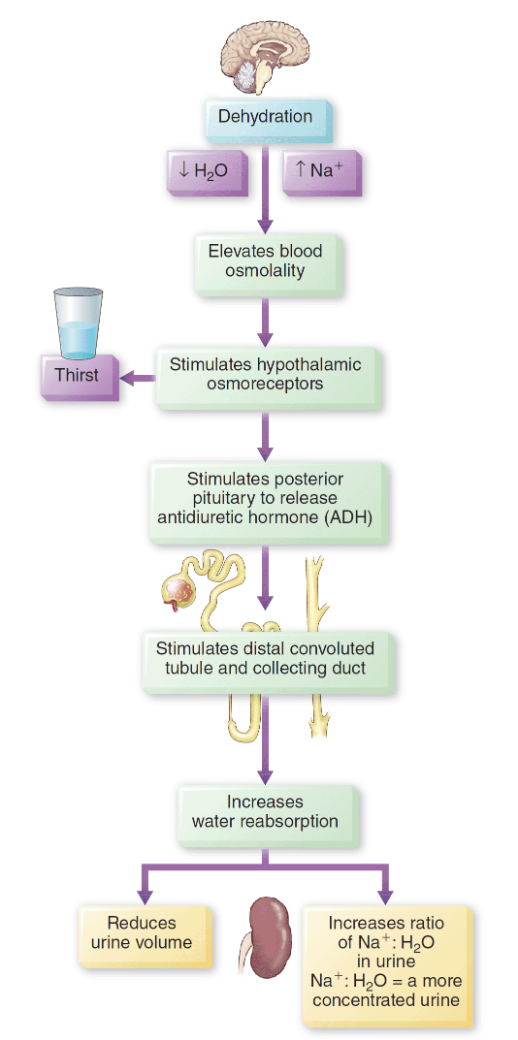
Action of antidiuretic hormone (ADH)
Purpose: Water Balance
Excess water is taken into body → ADH is suppressed → kidneys produce more dilute urine to rid body of excess water
Dehydration → ADH stimulated → kidney increase water reabsorption → reduce urine volume
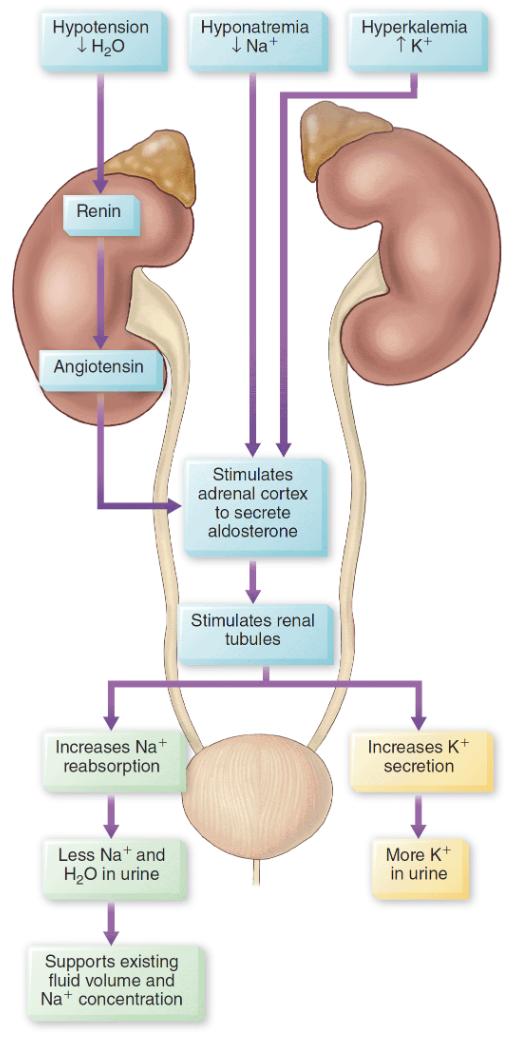
Action of aldosterone secretion
Purpose: Electrolyte Balance
Sodium decreases (hyponatremia) → Aldosterone released → increase reabsorption of sodium in distal tubule → increase serum sodium level
Elevated potassium (hyperkalemia) → aldosterone secreted → increase excretion of K+ in renal tubules → more K+ in urine
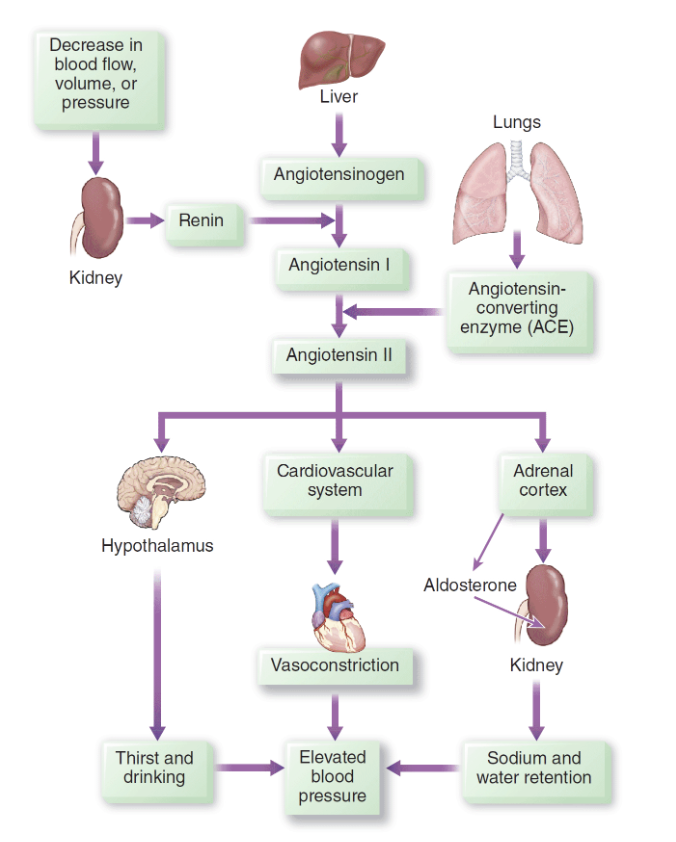
Renin-angiotensin-aldosterone system (RAAS)
Purpose: Acid-Base Balance → keep blood pH between 7.35 - 7.45
With acidosis, kidney tubules excrete H+ and reabsorb bicarbonate ions (HCO3–) to increase serum pH to a normal level
With alkalosis, kidney tubules reabsorb H+ and excrete HCO3– to decrease pH to a normal level.
Hormonal Function of Kidney
Kidney produces hormones renin, erythropoietin, activated vitamin D, bradykinin, prostaglandins
Decrease in blood pressure → Renin released + angiotensinogen released → produce angiotensin I + ACE → form angiotensin II → constricts blood vessels → increase blood pressure
Decreased renal blood flow and hypoxia → Erythropoietin released → stimulates bone marrow to produce RBCs
Prostaglandins trigger vasodilation → resulting in increased blood flow to kidneys
Bradykinin increases permeability of capillary membrane to certain solutes
Terms
Anuria: < 100-ml urine output/24 hr
Oliguria: < 400-mL urine output/24 hr
Polyuria: > 2,000-mL urine output/24 hr
Dysuria: Pain with urination
Enuresis: Involuntary urination at night
Frequency: Increase in voiding
Hematuria: Blood in urine
Hesitancy: Difficulty starting the flow of urine
Incontinence: Inability to control urinating
Nocturia: Frequent urination at night
Retention: Unable to empty bladder
Urgency: Urge to void immediately
Diagnostic Studies
Blood Tests
Serum creatinine: waste product, normal 0.5 - 1.2 mg/dL, increase in serum creatinine → renal dysfunction
BUN: waste product, normal 8 - 21 mg/dL, increased BUN → renal dysfunction
Electrolytes:
→ Sodium: normal 135 - 145 mEq/L
→ Potassium: normal 3.5 - 5.3 mEq/L
→ Phosphorus (PO4): normal 2.5 - 4.5 mEq/L
→ Calcium: 8.2 to 10.2 mg/dL
Urinalysis
Color/Turbidity/Odor
pH (changes in renal function)
Protein (normally not in urine but presence → infection, inflammation)
Glucose (diabetes)
Ketones (diabetic ketoacidosis, high-protein diet)
Bilirubin (liver disease)
RBC/WBC
Bacteria (UTI )
Gerontological considerations
Older adults susceptible to kidney injury r/t decreased blood flow, decreased GFR, altered tubal function and acid-base balance
Incomplete emptying of bladder
Decreased drug clearance
Risk factors for renal disorders
Age -> Incomplete emptying of bladder → UTI
Benign prostatic hyperplasia → Obstruction of urine flow
Diabetes/Hypertension → Chronic kidney disease
Gout/hyperparathyroidism/Crohn’s disease → Kidney stone formation
Immobilization → Kidney stone formation
Sclerosis/Tumors/Parkinson Disease → Incontinence
Terms
Acute Kidney Injury: rapid loss of renal function
Chronic Kidney Disease: kidney damage or decrease in GFR > 3 months
Acute Nephritic Syndrome: kidney disease with glomerular inflammation
Acute Tubular Necrosis: kidney injury r/t damage of kidney tubules
End-stage Kidney Disease: final stage of chronic kidney disease → retention of waste products → need for renal placement
Glomerulonephritis: inflammation of glomerular capillaries
DIABETES
Glossary terms
Diabetes: defects in insulin secretion → hyperglycemia
Diabetic ketoacidosis (DKA): Type 1 diabetes → deficiency of insulin → liver breaks down fatty acids → highly acidic ketone formed → acidocis
Fasting plasma glucose: blood glucose from fasting for 8 hours
Gestational diabetes: diabetes during pregnancy
Glycated hemoglobin (HgbA1C): glucose molecule attach to hemoglobin for the life of of red blood cell (120 days)
Hyperglycemia: elevated blood glucose level
Hyperglycemic hyperosmolar syndrome (HHS): Type 2 diabetes → insulin deficiency by an illness that raise demand for insulin
Hypoglycemia: low blood sugar level
Impaired fasting glucose (IFG) or Impaired glucose tolerance (IGT): prediabetes
Insulin: hormone secreted by beta cells of pancreas → metabolism of carbohydrates, proteins, fats
Insulin pump: continuous subcutaneous insulin infusion device delivers insulin on 24-hours basis
Ketone: highly acidic, formed when liver breaks down free fatty acid in the absence of insulin
Latent autoimmune diabetes of adults (LADA): subtype of diabetes
Nepthropathy: damage of kidney
Neuropathy: damage of nerve
Retinopathy: damage of small blood vessels that nourish retina in eye
Type 1 diabetes: absence of insulin production and secretion from genetic, immunologic, environmental factors that destroy beta cells in pancreas
Type 2 diabetes: deficiency of insulin production
Risk factors of Type 1 vs Type 2 Diabetes
Type 1
Early-onset (younger population)
Genetic/Familial
Viral or toxins factors
Type 2
Age (older population)
Obesity
Prediabetic
HTN > 140/90 mmHg
HDL < 35 mg/dL
Triglycerides >250 mg/dL
History of gestational diabetes or babies born weighing over 9 lbs
Insulin
Hormone secreted by beta cells in islets of Langerhans in pancreas
Insulin is anabolic, storage hormone
Transports, metabolizes glucose for energy
Stimulates → storage of glucose in liver, muscle (as glycogen) → storage of dietary fat in adipose tissue → transport of amino acids into cells
Inhibits breakdown of stored glucose, protein, fat
During Fasting Periods
Pancreas continuously releases a small amount of insulin (basal insulin)
When blood glucose levels decrease → Pancreas releases glucagon (secreted by alpha cells) → breaks down glycogen to make glucose (glycogenolysis)
→ breaks down amino acids to make glucose (gluconeogenesis)
Type 1/Type 2/Gestational Diabetes
Type 1 diabetes: absence of insulin production and secretion from genetic, immunologic, environmental factors that destroy beta cells in pancreas
Type 2 diabetes: deficiency of insulin production
Gestational diabetes: diabetes during pregnancy due to secretion of placental hormones → causes insulin resistance
Clinical manifestations of Diabetes
Polyuria
Polydipsia
Polyphagia
Fatigue
Vision changes
Tingling or numbness in hands or feet
Dry skin, skin lesions or wounds that are slow to heal
Recurrent infections
Type 1 may have sudden weight loss
Diagnostic findings
Fasting plasma glucose
HbA1c
→ A normal A1C level is below 5.7%
→ 5.7% - 6.4% indicates prediabetes
→ 6.5% or higher indicates diabetes
Criteria for Diagnosis of Diabetes