OB 3 pt 1
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Dystocia
Abnormal or difficult labor
Abnormal progression of labor
Early admissions
Sedentary, early epidural, decreases labor progression
Encourage natural upright position
Requires medical or surgical deliver
Leading cause of cesarean deliveries
Dystocia causes
Problems with powers
Expulsive force
Problems with passageway
Pelvis/birth canal
Problems with passenger
Position/fetus
Problems with psyche
Maternal stress
problems with powers: Hypotonic uterine dysfunction
Causes: Oxytocin, fetal malpresentation
Never relaxes between contractions
More contractions to compensate for ineffective contractions
Ineffective contractions, low placental perfusion
Longer latent phase, exhausted mother
0-6cm dilated
During active labor
Weak contractions, softer fundus with contraction
Risk factors
Overstretching of uterus
Multiple fetus
One large fetus
Lots of fluid
Bowle or bladder distention
Excessive analgesia
Risk of hemorrhage
problems with powers:precipitate labor
Abnormally rapid
Less than 3 hours
Manifestations
Genetically Soft/stretchy tissues
Abnormally strong contractions
A lot of Braxton hicks
Complications
Maternal anxiety, injury, bleeding
Fetal hypoxic injury, trauma
problems with passenger
Vertex but not flexed (face), OP
Breech
Usually stuck by 35-36 wks
Risk for prolapsed cord, difficult birth
undo with External cephalic version
problem with passenger: shoulder dystocia
Obstruction of fetal decent of shoulder after head is delivered
Obstetric emergency
Occurs due to large fetus
Fetal injury
Asphyxia, brachial plexus injury, fractures from purposefully broken ckavicle
Maternal injury
Hemorrhage dt uterine atony, rupture, lacerations
Nursing care
Call for help
Assist with McRoberts maneuver or suprapubic pressure
No fundal pressure! Call NICU team!
problems with passageway
Pelvis
Pelvic inlet
Pelvic outlet
Pelvic shape
Best gynecoid, anthropoid ok
Cephalopelvic disproportion (CPD)
Can all lead to dystocia
problems with psyche
Negative emotions
Anxiety
Fear
Helplessness
Impact on dystocia
Uterine dysfunction
Uncoordinated contractions
Pain
Surgical birth
dystocia nursing assessment and management
Nursing assessment
Hx of risk factors
VS (infection)
Uterine contractions
FHR, positioning (Leopolds)
Check to see if baby in good position and see where fhr can be assesed htrough leopolds
Nursing management
Promoting labor progress
Active phase: 1cm/ hr
Bowel/bladder distention
Keep empty
Pitocin (oxytocin) augmentation
For protracted contractions
Providing physical and emotional comfort
preterm labor
• Regular uterine contractions with cervical effacement and dilation before 37 weeks’ gestation
• Preventative progesterone for high risk @16 weeks
• Always had preterm
preterm risk factors
Infection is huge! (dental, UTI)
Uterine anomalies
Multiple gestations/ ART
Polyhydramnios
Genetics
Prenatal care
ETOH/Drugs
Extreme age
Ethnicity
Obesity
preterm fetal risk
Neurodevelopment
Respiratory Distress Syndrome (RDS), surfactant deficiency, stay in house
Infections
Thermoregulation issues, not enough fat
Brain bleeds, micro premies 23-28 wks
Jaundice, immature liver, pathologic jaundice
High risk of developmental delays/disabilities
Feeding issues
Hypoglycemia
preterm Tx
Bedrest-??
With bathroom privleages
Prevent dvt
Tocolytic medications (Drug Guide 21.1)
Breaks down contraction
Won't stop preterm labor only delays it
For preterm labor up to 34 weeks
Dilation of >2cm, 80% for nulliparous mom
Purpose: Delay not Prevent!
reduce severity of RDS and other complications, delay delivery until corticosteroids can be given
Contraindications
Abruption
Detaching from uterus
Fetal distress
Pre/Eclampsia
Dilation> 6cm
Too late
Active labor
Maternal instability
preterm medical tx
magnesium sulfate ( smooth muscle relaxer)
indomethacin (prostaglandin inhibitor) NSAID
nifedipine/ Procardia (Ca+ channel blocker inhibits muscle Contrax)
betamimetics (Terbutaline)
corticosteroids (betamethasone)
all tocolytics except for steroid
its-indomethacin
not-nifedipine
my-magnesium
time-terbutaline
preterm labor nursing assessment
History/Assessments Risk factors
Subjective:
Change in Discharge or spotting, ROM
Pelvic pressure, backache, cramps, GI
Heaviness or aching in the thighs
Uterine contractions with or without pain
More than six contractions per hour
Objective:
Contractions
Effacement/Dilation
Fetal descent/station
Laboratory:
CBC, Urinalysis
Amniotic fluid analysis
Fetal fibronectin:
Glycoprotein from chorion
Glue that helps hold structure of membranes
Stuck between chorion and embrion
Good for triaging/admitting
Shouldn’t be present after 23 weeks
If present: delivery w/in 14 days
If absent: predictor of no delivery
Good sign
Diagnostic testing:
Cervical length measurement (U/S)
Good predictor after 16 weeks
If cervical length >30mm = no delivery soon
preterm support
Multifactorial
Working
Assessment
Education
Stress reduction
Nonworking
Full family support
Nicu
preterm prevention
Avoid traveling long distances
Avoid lifting heavy objects
Avoid performing hard, physical work
Mild to moderate levels of exercise
Appropriate weight and nutrition.
Wait 18 months between pregnancies.
Visit a dentist in early pregnancy
Avoid sexual activity preterm labor
Avoid cannabis, cocaine, tob, heroine
Use stress management techniques
Seek help with IPV
Teaching of Symptoms:
Contraction pattern frequency
Backache
GI issues
Pelvic pressure
Leaking
postterm labor
Pregnancy >42 weeks’ gestation
Incorrect dates
Unknown etiology
Pregnancy issues: uteroplacental insufficiency, Fluid levels
post term labor assessment and management
Nursing assessment:
Estimated date of delivery
Daily fetal movement counts,
NST, BPP, AFI twice weekly
Weekly cervical examinations
Client needs: education, anxiety, and coping ability
Nursing management:
Fetal surveillance
Decision for labor induction
Support; education
Intrapartum care; pain management!
postterm labor maternal and fetal risks
Maternal risks: Exhaustion!
C/S
Dystocia/ birth trauma
Postpartum hemorrhage
Infection
Fetal risks: problems with big babies, FGR
TX
induction and augmentation
Induction
stimulating contractions via medical or surgical means
augmentation
enhancing ineffective contractions after labor has begun
labor induction and augmentation
All-time high!
Fetal distress, C/S , instrumental delivery, epidurals, infections, NICU
Recommendations:
After CPD is ruled out , clear medical indication
Close monitoring
Contraindications:
Previa, abruption, prolapsed cord, classical incision, Abn FHR
Reasons:
PPROM, HTN, infection, dystocia, IUFD, Diabetes
Many interventions required:
IV
Bed rest
Continuous FHR monitoring
PAIN!
Prolonged stay
labor induction and augmentation: assessment
Maternal & Fetal status
Cervical Assessment for Ripeness
Ripe cervix: 1st step in before effacement/dilation
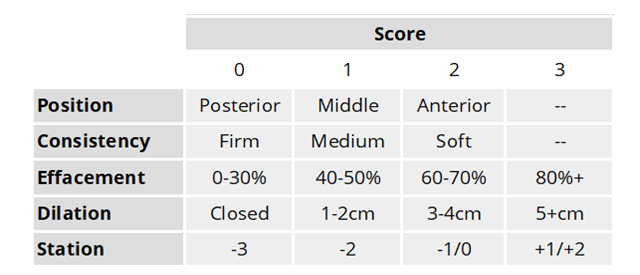
Bishop Score
likely successful induction
Short, centered, soft, partially dilated is good!
Good score:
8-10 good
6-7 give some time, middle rnage
0-5 give meds to rippen
labor induction and augmentation: therapeutic management
NonPharm:
Herbal agents
Castor oil, hot baths, enemas
Sexual intercourse with breast stimulation
Mechanical methods
Foley
Dilators (laminaria)
Rolled up Seaweed
Surgical methods
Stripping of membranes
Amniotomy
labor induction and management: pharmacological management
Bishop score of 5 or less
Prostaglandins- promotes cervical ripening and contractions
Dinoprostone (Cervidil, etc.)
Directly softens cervix
Cervical insert
Oxytocin (Pitocin)
Uterotonic Agent- very popular!
IV:POTENT
No placental crossing
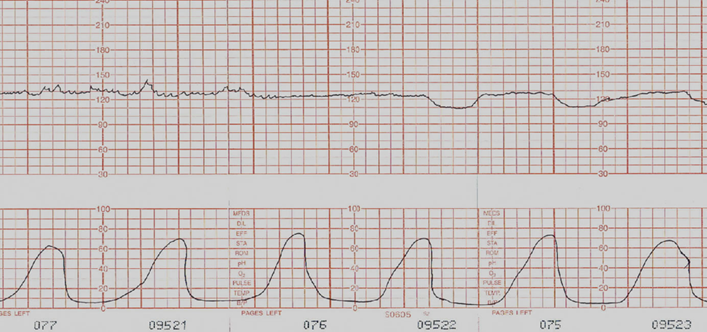
Watch out for uterine hyperstimulation = FHR!!
Tachysystole more than 6 contraction in 10 min period not enough resting tone for good placental perfusion, maternal exhaustion.
Stop Pitocin
10 units/1 L of isotonic solution, titrated to achieve stable contractions every 2 to 3 minutes lasting 40 to 60 seconds
1cm/hr dilation progress is good!
Misoprostel (Cytotec)
Prostaglandin and Uterotonic
Not as potent as oxytocin
Ripens cervix
Oral, vaginal, rectal
Can also cause uterine overstimulation
tocolytics
Magnesium Sulfate (smooth muscle relaxer)
IV
Assessment: RR, DTR, renal fx, FHR, infant RR,
Also treats preeclampsia
Indomethacin (prostaglandin inhibitor)
NSAID
Oral/Rectal
Risk: oligohydramnios
Assessment: Urine output, mat temp, AFI
Nifedipine/Procardia (Ca+ Channel blocker that inhibits muscle contractions
Better effectiveness
Oral or sublingual
Assessment: Cardiac SSX (hypotension, tachycardia, HA, N/V, flushing)
Betamimetics ( Terbutaline) Not in book
Derived from epinephrine
Assessment: racing HR! Fetal arrythmias
uterotonics
Dinoprostone (Cervidil, etc.)
Directly softens cervix
Cervical insert
Oxytocin (Pitocin)
Uterotonic Agent- very popular!
IV:POTENT
No placental crossing
Watch out for uterine hyperstimulation = FHR!!
10 units/1 L of isotonic solution, titrated to achieve stable contractions every 2 to 3 minutes lasting 40 to 60 seconds
1cm dilation progress is good!
Misoprostel (Cytotec)
Ripens cervix
Oral, vaginal, rectal
Can also cause uterine overstimulation
corticosteroids
Corticosteroids (Betamethasone) before 34 weeks
IM; 2 doses 12 hours apart
Helps Increase production of surfactant earlier and faster
obstetrical emergencies
umbilical cord prolapse
placental previa
placental abruption
uterine rupture
amniotic fluid embolism
umbilkical cord prolapse
Obstetric emergency!!
Partial or total occlusion of cord with rapid fetal deterioration
Nursing assessment
Prevention- Knowing Risk factors
Malpresentation
IUGR, Prematurity
Rom with high station
Polyhydramnios
Continuous assessment of client and fetus
Nursing management
Prompt recognition- sudden bradycardia
Measures to relieve compression
Manual
Position – Trendelenburg, knee to chest, Sims
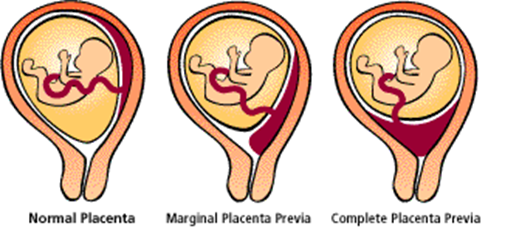
placental previa
Diagnosed with ultrasound
Placental implantation in the lower uterine segment over or near internal os of cervix
1st thought with painless bleeding
Causes:
Direct cause with # of C/S
Risks:
Separation, bleeding or hemorrhage
Barrier
2nd or 3rd trimester of pregnancy
No Vaginal Exam!! For fear of abruption
C/S
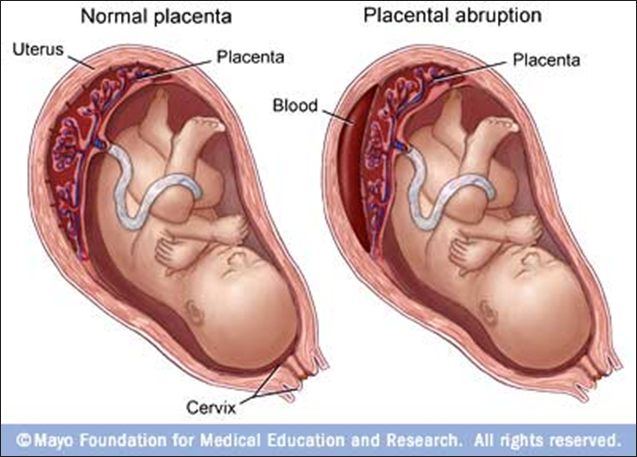
placental abruption
Obstetric emergency involving premature separation of placenta
At risk for no perfusion needs circulation
Risk factors
Illicit drugs (cocaine)
Trauma
IPV, CAR ACCIDENT
HTN
Smoking
Management dependent on gestational age, extent of hemorrhage, and maternal–fetal oxygenation perfusion
Less than 20 wks SAB
Maintenance of maternal cardiovascular status
Prompt delivery of fetus
Cesarean birth if fetus still alive; vaginal birth if fetal demise
S/S:
Vaginal bleeding (but also may not see any)
Hypertonic contractions
Maternal hypovolemia (shock, oliguria, anuria)
Coagulopathy
Pain mild to severe – usually localized over one region, but could be diffuse and feel like a board
“Silent Abruption” – may not have any pain or tenderness
Still see other signs
Maternal risk: hemostasis related
Perinatal mortality/Neonatal mortality and morbidity is 15-30% - because of:
Hypoxia, preterm birth, SGA
Risk of neuro defects is increased
uterine rupture
Obstetric emergency; onset marked by sudden fetal bradycardia
Nursing assessment
Risk factors: previous uterine surgery, hyper stimulation
Onset of sudden fetal distress
Nursing management
Preparation for urgent cesarean birth
Continuous maternal and fetal monitoring
amniotic fluid embolism
Obstetric emergency- 20% mortality and 50% survivors have neurologic injury
Sudden onset of hypotension, hypoxia, and coagulopathy d/t amniotic fluid (or particles) enter maternal circulation
Nursing assessment:
difficulty breathing,
cardiac arrest
Nursing management:
hemodynamic function
critical care monitoring
external cephalic version
36-38 weeks
Rotation of fetus done manually In patient, with ultrasound and FHR
monitoring
cesarian birt
Reasons?
Classic or low transverse incision
Incisions:
Low transverse
Classical/Vertical
Blood loss
Skin closures:
Sutures/Surgical
Glue
Sutures/staples
Nursing management
Preoperative care
Blood work
Prepare surgical site
IV
Foley
Meds
Postoperative care
Frequent VS
Fundal/Lochia Assessments
Dressing/wound assessment
Perineal Care/hygiene
Pain management
IS/Movement/GI
Help with baby
vaginal birth after cesarean VBAC
Controversy related to risk of uterine rupture and hemorrhage
Contraindications
Prior classical incision
Other uterine surgery
Emergent birth
Special areas of focus: consent, documentation, surveillance, and readiness for emergency
instrumental deliveries
Application of traction to fetal head
Forceps: similar to tongs
“Guided pushing”
Indications:
nonreassuring FHR pattern, presumed fetal jeopardy or fetal distress
Risk of tissue trauma to mother and newborn
Prevention as key
terms
“Failure to Progress”
Protracted Disorders (slower)
Hydration, reassurance, position changes
Arrest Disorders (cessation)
perinatal loss
Perinatal loss- pregnancy loss/neonatal death up
to 1 month of age
• Numerous causes, some unknown
• Post-term
• Substance abuse
• Infection, HTN, diabetes, obesity
• Congenital anomalies
• Cord, Uterine Rupture, AMA
• Trauma
• Social determinants of health
• Devastating effects on family and staff
• Nursing assessment/management
• Inability to obtain fetal heart sounds
• Ultrasound to confirm absence of fetal
activity
• Labor induction
• Assistance with grieving process/seeing
baby
• Referrals
Multiple Gestations
Increased incident
People having babies later, IVF puts multiple embryos into patient
Increased mortality, morbidity
Vaginal delivery is twins are vertex/vertex
No vaginal delivery > twins
Vaginal delivery done in OR
Must monitor both fetus'
Maternal risks: Uterine rupture, hemorrhage d/t uterine atony
Fetal risk: Prematurity, IUGR intrauterine growth restrictions, C/S
Excessive fetal size
Macrosomia (LGA) > 4000g
Risk for dystocia
Increased use of instrument delivery
May be scheduled C/S to avoid
Dystocia
Maternal hemorrhage
Maternal laceration injury